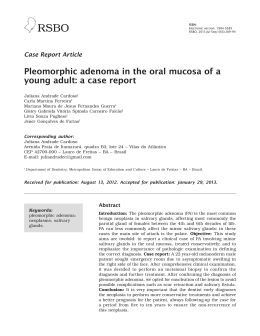
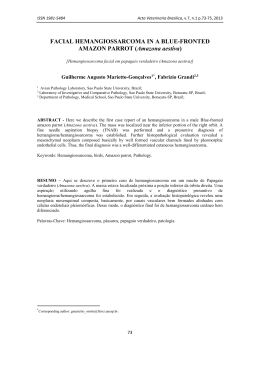
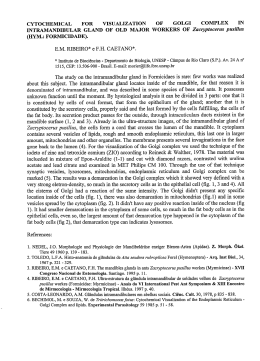
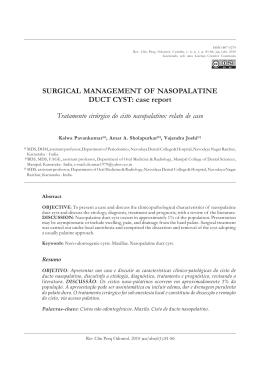
Dentistry / Odontologia Synchronous pleomorphic adenoma and periapical cyst: clinical case report Adenoma pleomorfo e cisto periapical sincrônicos: relato de caso clínico Cláudio Maranhão Pereira1, Danilo Santos Carneiro1, Patrícia Freire Gasparetto1, Tessa de Lucena Botelho1 1 Dental School, University Paulista, Goiânia-GO, Brasil. Abstract The pleomorphic adenoma or mixed benign tumor is the most common benign neoplasia of the salivary gland in human beings. It preferentially occurs in the superficial lobe of the parotid gland. In the oral cavity, associated with the minor salivary glands, it has a greater predilection for the palate region, with slight predisposition in women between the 3rd and 4th decades of life. The radicular cyst is an odontogenic inflammatory cyst resulting from pulp lesions caused by traumas or caries. In spite of being relatively common, there are no reports of association with salivary gland tumors. The aim of this work is to report a case of a 36-year-old woman patient, who presented with synchronous development of a pleomorphic adenoma and periapical cyst within the same region. The option taken was to perform enucleation of both lesions, followed by local curettage. The patient has been followed-up clinically and radiographically for around 18 months without signs of recurrence. Descriptors: Adenoma, plesmorphic; Odontogenic cysts; Odontogenic tumours; Salivary gland, minor Resumo O adenoma pleomórfico ou tumor misto benigno é a neoplasia benigna mais comum primária de glândula salivar. Ocorre preferencialmente no lobo superficial da glândula parótida. Na cavidade oral, associado com as glândulas salivares menores, tem uma maior predileção para a região do palato, com ligeira predisposição em mulheres entre a 3 ª e 4 ª décadas de vida. O cisto radicular é um cisto odontogênico inflamatório decorrente de lesões causadas por traumas ou cárie. Apesar de ser relativamente comum, não há relatos de cistos periapicais associados com tumores de glândula salivar. O objetivo deste artigo é relatar um caso de uma paciente de 36 anos de idade com desenvolvimento sincrônico de adenoma pleomorfo e cisto periapical em uma mesma região. A opção tomada foi a de realizar a enucleação de ambas as lesões, seguido de curetagem local. A paciente está sendo acompanhada clínica e radiograficamente por cerca de 18 meses sem sinais de recidiva. Descriptors: Adenoma pleomorfo; Cistos odontogênicos; Tumores odontogênicos; Glândulas salivares menores Introduction the mouth”. During anamnesis, no datum from the previous medical and family history made any contribution. On extraoral physical exam no asymmetry was found in the right maxillary region. The oral exam revealed the presence of an increase in volume in the shape of a cupola in the right maxillary posterior palatal region, covered with whole mucosa, with a firm consistency on palpation, and measuring about 2.0 cm in its largest diameter. After analyzing the imaging exam, a radiolucent, unilocular, circumscribed, well defined lesion with a radiopaque halo was observed, associated with the roots of tooth 16, compatible with a periapical cyst (Figure 1). Puncture and aspiration were performed, in which a yellow, viscous liquid was obtained. Immediately afterwards, an excisional biopsy of the lesion was performed, associated with extraction of tooth 16. After cystic enucleation, it was possible to visualize a mass with a firm consistency on palpation, well delimited and in continuity with the extraction site (Figure 2). In the trans-operative period it was necessary to increase the envelope type incision to the maxillary tuber region, in addition to performing a relief incision with three angles to increase the surgical exposure area, the maxillary sinus floor, major palatal artery as the nerve endings were preserved (Figure 3). After detachment of the mucoperiosteal flap, the tumoral mass was visualized, in which enucleation and vigorous curettage was performed. Both lesions were fixed in 10% formol and sent to the Pathologic Anatomy Service. The two tissues were microscopically analyzed, making it possible to confirm the diagnosis of pleomorphic adenoma, in which the epithelial cells formed solid sheets or a double layer of ductiform structures, containing eosinophilic inclusions within them. The stroma of the lesion generally presented eosinophilic hyaline material (Figure 4). In the other tissue, the histologic characteristics confirmed the diagnosis of periapical cyst, which was shown to be lined with stratified squamous epithelium associated with cholesterol crystals with multinucleated giant cells, hemocytes and areas of hemosiderin pigmentation, typical of the radicular cyst. Salivary gland tumors constitute one of the most important groups of lesions affecting the head and neck region. The pleomorphic adenoma or mixed benign tumor is the most frequently occurring one of the salivary gland tumors, affecting both the minor and major salivary glands. Among all the salivary glands, the parotid is the site of major predilection1-4. When it occurs in minor salivary glands, the hard palate region presents the greatest predilection, followed by the upper lip, tongue, floor of the mouth and retromolar region. In the hard palate it may perforate the bone and extend into the maxillary sinus1-2. Patients between the ages of 30 and 40 years are the most affected, but it may develop at any age, even in newborn children2. Clinically, these tumors present as solitary oval lesions with well delimited margins. The lesion is mobile, except when it occurs in the palate, presenting slow growth and is asymptomatic. It may vary from a few to several centimeters in size1-3. The recommended treatment protocol is surgical excision, recurrence being frequent and variable according to the location of the lesion and surgical technique used4-5. Fewer than 5% of these tumors undergo malignant transformation, this being more common in cases of multiple recurrences, and when this occurs it is denominated carcinoma ex pleomorphic adenoma5-6. There are reports of simultaneous development of pleomorphic adenoma with some types of adenocarcinomas7-10. However few cases in the literature describe associations or development of cysts in regions of gnathic bone4. The aim of this case report was to describe the case of a patient with a pleomorphic adenoma associated with a periapical cyst in the same region. Case report The patient, a 36-year-old woman, presented to the Oral Diagnostic Service at the University Paulista, complaining of a “lump in J Health Sci Inst. 2011;29(1):34-6 34 Figure 1. Radiographic aspect – a radiolucent, unilocular lesion was observed associated with the roots of tooth 16 Figure 4. It is possible to note the epithelial cells formed solid sheets or a double layer of ductiform structures, containing eosinophilic inclusions within them The post-operative period developed satisfactorily; the sutures were removed after seven days, and fourteen days later the surgical area was found to be completely healed. The patient has been clinically and radiographically followed up for 18 months and no recurrence of the lesion has been observed. Discussion Both the pleomorphic adenoma and the periapical cyst present a very typical clinical pattern. Analyzing the pleomorphic adenoma, in the case of palatal lesions, conventional radiographs are not of much help in diagnosis, as the lesion is located in an area of many superimpositions, and in general, the palatal bone is not compromised3-4,8. Nevertheless, in this case, the option was taken to perform an orthopantomograph that proved there was no bone compromise. The treatment most used for pleomorphic adenoma consists of surgical excision with a safety margin4-6,9, as recurrence could occur due to remaining residues of the capsule or of the lesion itself. In the present case, conventional surgical removal was performed under local anesthesia, due to the favorable characteristics the lesion presented, since it is the most indicated therapy when the lesion is situated in the minor salivary glands. The determinant factor for recurrence is not the period of development of the lesion in which the surgical treatment is performed, but the surgical technique used4-5,10. The prognosis is considered excellent when the surgery is performed in an adequate manner, with a cure rate of approximately 95%2. It is of great value to follow up cases of pleomorphic adenoma, and post-operative control should continue for five years5. Figure 2. The oral exam revealed the presence of an increase in volume in the shape of a cupola in the right maxillary posterior palatal region Conclusion In spite of these two intraoral pathologies being relatively common when compared with the other cystic and glandular alterations of the oral cavity, their development simultaneously and in the Figure 3. After cystic enucleation, it was possible to visualize a mass with a firm consistency on palpation, well delimited and in continuity with the extraction site Pereira CM, Carneiro DS, Gasparetto PF, Botelho TL. 35 J Health Sci Inst. 2011;29(1):34-6 same region has not been reported in the specialized literature. Thus, the diagnosis of neoplastic and cystic lesions continues to play an important role in the dental clinic. However, it is necessary to point out the need for following up the patient, since the episodes of recurrence of some lesions occur at a late stage, generally in periods longer than 5 years after treatment. Therefore, it is mandatory to have knowledge of the clinical and histological characteristics and treatment of lesions involving the maxillae and their adjacent structures. 6. Thakur JS, Mohindroo NK, Mohindroo S, Sharma DR, Thakur A. Pleomorphic adenoma of minor salivary gland with therapeutic misadventure: a rare case report. BMC Ear Nose Throat Disord. 2010;10:2. 7. Pistorio V, Teggi R, Bussi M. Simultaneous pleomorphic adenoma of the parapharyngeal space and contralateral submandibular gland. Case report. Acta Otorhinolaryngol Ital. 2008;28(5):257-60. 8. Coombes DM, Kaddour R, Shah N. Synchronous unilateral pleomorphic adenomas in the parotid gland: report of a case. Br J Oral Maxillofac Surg. 2009;47(2):155-6. 9. Papadogeorgakis N, Kalfarentzos EF, Vourlakou C, Malta F, Exarhos D. Simultaneous pleomorphic adenoma of the left parotid gland and adenoid cystic carcinoma of the contralateral sublingual salivary gland: a case report. Oral Maxillofac Surg. 2009;13(4):221-4. References 1. Oliveira FA, Duarte EC, Taveira CT, Máximo AA, Aquino EC, Alencar RC et al. Salivary gland tumor: a review of 599 cases in a Brazilian population. Head Neck Pathol. 2009;3(4):271-5. 10. Pires FR, Alves FA, Almeida OP, Lopes MA, Kowalski LP. Synchronous mucoepidermoid carcinoma of tongue and pleomorphic adenoma of submandibular gland. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2003;95(3):328-31. 2. McGuff HS, Perez DE, Kern TW, Jones AC. Oral and maxillofacial pathology case of the month. Pleomorphic adenoma (benign mixed tumor). Tex Dent J. 2010;127(5):508, 518-20. Corresponding author: 3. Jansisyamont P, Blanchaert RH, Ord RA. Intraoral minor salivary gland neoplasm: a single institution experience of 80 cases. Int J Oral Maxillofac Surg. 2002;31:257-61. Cláudio Maranhão Pereira Department of Oral Diagnosis Dental Scool, University Paulista SGAS Quadra 913, s/nº – Conjunto B – Asa Sul Brasília-DF, CEP 70390-130 Brazil 4. Bradley PJ. Recurrent salivary gland pleomorphic adenoma: etiology, management, and results. Curr Opin Otolaryngol Head Neck Surg. 2001;9:100-8. 5. Delbem ACB, Cunha RF, Vieira AE, Pugliesi DM. Conservative treatment of a radicular cyst in a 5-year-old child: a case report. Int J Paediatr Dent. 2003; 13(6):447-50. E-mail: [email protected]; [email protected] Received November 24, 2010 Accepted January 31, 2011 J Health Sci Inst. 2011;29(1):34-6 36 Synchronous pleomorphic adenoma and periapical cyst
Baixar