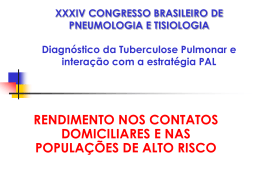
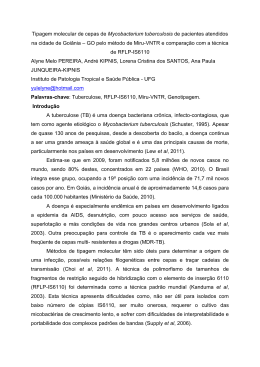
Miliary tuberculosis in a young child – a case report Liliana Pinho1, Sara Oliveira1, Josefina Serino2, Teresa Febra3, Sandra Ramos1, Conceição Silva1, Maria José Dinis1 1Paediatrics, 3Centro Centro Hospitalar Póvoa de Varzim/Vila do Conde; 2Ophthalmology, Hospital Pedro Hispano, Matosinhos; de Diagnóstico Pneumológico, Póvoa de Varzim/Vila do Conde – Portugal INTRODUCTION Tuberculosis represents a public health problem. During 2011, a total of 41 cases of tuberculosis in children were notified in Portugal, with 17 of them less than 5 years old. Young age and HIV infection are the most important risk factors for severe or disseminated disease. CASE REPORT Previously healthy 3-year-old girl Normal physical examination Normal WBC ↑CRP (22mg/dL) Urinalysis: leucocytes+bacteria Oral cefuroxime (40 mg/kg/day) Normal physical examination and urinalysis Symptomatic treatment Urine culture: Escherichia coli Oral amoxicillinclavulanate (sub-therapeutic dose) Antibiotic intolerance Pale skin, high fever (40⁰C), hepatomegaly Laboratory findings: mild anemia, ↑CRP (21mg/dL),↑transaminases (AST 245U/L, ALT 143U/L), nitrites and bacteria in urinalysis… Intravenous cefuroxime Urine culture confirmed UTI by E. coli Laboratory reevaluation: Normal WBC, CRP 13 mg/dL, ESR 16 mm/hr, AST 132U/L, ALT 93U/L Chest X-ray (figure 1) Diarrhea Anorexia Dysuria Abdominal pain Fever Day 1 Day 2 Day 4 Day 13 Emergency Service Emergency Service Emergency Service Day 19 Day 23 Hospital admisson Negative tuberculin skin test Isolation of Mycobacterium tuberculosis in gastric aspirate, cerebrospinal fluid and urine Persistent fever and anorexia, despite antibiotic treatment for UTI Hepatomegaly with hepatitis (streptomycin-resistant) (negative viral serology) Pulmonary infiltrate with a miliary pattern Miliary tuberculosis? • Normal cerebral MRI • Ophthalmological examination: tuberculous posterior Figure 1. Chest X-ray uveitis (figure 2) Therapy with rifampicin, isoniazid and pyrazinamide associated with prednisolone Significant clinical improvement after two weeks of treatment Total treatment consisted of prednisolone (1 month), rifampicin, isoniazid and pyrazinamide (2 months), followed by rifampicin and isoniazid (10 months) HIV infection and main primary immunodeficiencies were excluded Figure 2. Choroidal tuberculomas COMMENTS Even in the era of advanced medical technology, tuberculosis is still a diagnostic challenge, especially when the presentation is atypical and extra-pulmonary. Beyond that, in this case, superinfection by other bacteria somewhat delayed recognition of the underlying tuberculosis. A high index of suspicion by the physician is required as prompt institution of adequate treatment is decisive for final outcome. BIBLIOGRAPHY: 1. Sandgren A, Hollo V, Quinten C, Manissero D. Childhood tuberculosis in the European Union/ European Economic Area, 2000 to 2009. Euro Surveill. 2011; 16 (12): pii=19825. 2. W Haas. High time to tackle childhood tuberculosis. Euro Surveill. 2011; 16 (12): pii=19827. 3. Direção-Geral da Saúde. Programa Nacional de Luta Contra a Tuberculose. Ponto da Situação Epidemiológica e de Desempenho – Relatório para o Dia Mundial da Tuberculose, Março 2012. 4. Moreno-Pérez D, et al. Diagnóstico de la tuberculosis en la edad pediátrica. An Pediatr (Barc). 2010. doi:10.1016/ j.anpedi.2010.01.002. 5. Grupo de Trabajo de Tuberculosis de la Sociedad Española de Infectología Pediátrica (SEIP). An Pediatr (Barc). 2008;69(3):271-8. 6. Oberhelman RA, Soto-Castellares G, Gilman RH et al. Diagnostic Approaches for Paediatric Tuberculosis by Use of Different Specimen Types, Culture Methods and PCR – a Prospective Case-control Study. Lancet Infect Dis, 2010; 10 (9): 612-620. 7. Rodrigo C, Atukorala I. Delay in diagnosis of generalized miliary tuberculosis with osseo-articular involvement: a case report. Journal of Medical Case Reports, 2011; 5: 512. 8. Marais BJ, Schaaf HS. Childhood tuberculosis: an emerging and previously neglected problem. Infect Dis Clin N Am, 2010; 24: 727-749. 9. Swaminathan S, Rekka B. Pediatric Tuberculosis: global overview and challenges. Clinical Infectious Diseases, 2010; 50 (S3): S184-S194. 10. Pereira L, Marques L, Castro C, Guedez Vaz L. Diagnóstico e tratamento da tuberculose em pediatria – recomendações das Secções de Pneumologia e Infecciologia Pediátrica da Sociedade Portuguesa de Pediatria. Rev Port Clin Geral, 2003; 19: 643-646. 11. Fernandes SRC, Homa MNO, Igarashi A et al. Miliary tuberculosis with positive acid-fast bacilli in a pediatric patient. São Paulo Med J, 2003; 121 (3): 125-127. 12. Nelson Textbook of Pediatrics, 18th edition, 2007.
Baixar