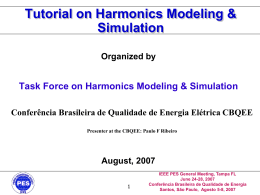
Nutrigenomics and Familial Hypercholesterolemia Andréa Simões 1, Cláudia Azoia 1, Dulce Rodrigues 1, Tatiana Cunha 1, Célia A. Gomes 2 Edição 02/14 1 Dezembro 2014 (1) – Alunos do 3º ano da Licenciatura de Dietética e Nutrição da Escola Superior de Tecnologia da Saúde de Coimbra (2) – Docente de Genética da Escola Superior de Tecnologia da Saúde de Coimbra 1. Introduction Familial Hypercholesterolemia (FH) is an hereditary disease 45Y C:318 2 3 64Y C:241 60Y C:233 20 000 individuals with FH 56Y C:335 AMHA:52Y from a genetic alteration, which causes an increase in cholesterol levels, specifically LDL Cholesterol (LDL-C)1,2. This is considered as a risk factor for the premature development of cardiovascular disease (CVD)1,2. It is an autosomal dominant disease, 40Y C:375 2 3 37Y C:199 33Y C:188 Legend 29Y C:303 35Y C:421 Y – Age in years which their genotype may be heterozygous or, more rarely, homozygous, with the C – Cholesterol with respective values AMHA – Acute Myocardial Heart Attack latter more severe phenotype and Total Cholesterol (TC) levels higher than in the heterozygous form1,2. 7A C:502 4A C:164 Fig.1- Family tree of FH carrier family. Our main goal is to demonstrate the relationship between bioactive compounds (in particularly, polyphenols) and the expression of some genes that are "altered" in the individual with FH. 2. Familial Hypercholesterolemia 4. Nutrigenomics and FH The FH is considered a "silent disease" since usually has no symptoms3. Diagnosis TC > 290 mg/dl ou c-LDL >190mg/dl Tendon Xanthomas Table 2: Dietary polyphenols with target protein and molecular signature9 Molecular Signature Dietary Polyphenols Target Protein Procyanidin B2, Procyanidin C1, Cinnamtannin A2, Resveratrol, Catechin, Epicatechin, Quercetin, Gallic acid, Tangeretin, Taxifolin APOA-I, APOB, APOB100 Increase expression and secretion Catechin, Naringenin, Hesperetin, Gossypin, Eriocitrin, Red grape juice polyphenols LDLR Increase expression TC - Total Cholesterol Mutations in LDLR, APOB or PCSK9 genes This disease can be caused by a mutation in the receptor gene of low density lipoproteins (LDLR) or apolipoprotein B gene (APOB) or the proprotein convertase subtilisin / kexina type 9 gene (PCSK9)2,5. 3. Genetics of FH 5. Nutritional and pharmacological care of FH Table 1: Genetic causes that cause HF 2,5-8 LDLR gene Chromosome Chromosome 19p13.1-p13.3 ApoB gene Chromosome 2p23-p24 PCSK9 gene Chromosome 1p32-p34 Encodes Mutations Class 1 Class 2 Class 3 Class 4 Class 5 LDL receptor - cell surface glycoprotein (LDLR) ApoB100 protein (LDL binds to its receptor through apoB100) (+ frequent in Europe) Serine protease (decreased LDLR in hepatocytes) Increased activity (increased levels of cLDL) p.R3531C p.R3527Y p.R3527Q Individuals suffering from FH should adopt a healthier life style combined with a balanced diet2 : Rich in plant foods, fruits, whole grains and fiber, (preferably soluble since it helps to decrease the concentrations of TC and cLDL5 Low in saturated and trans fat, preferring the unsaturated (mono and polyunsaturated), in particular the olive oil, to reduce the c-LDL from the diet5 Drug therapy is almost inevitable, and is a therapy that involves the medication with statins, fibrates, nicotinic acid and cholestyramine1,2. 5. Final Remarks Early diagnosis enables that CVD risk behaviours (like physical inactivity, smoking, alcohol) be reduced by implementing physical activity and healthy eating habits (such as diet low in saturated fats and quickly absorption sugars) and / or pharmacological treatment, thus modifying the levels of mortality and morbidity. 6. References 1.Bourbon M, Rato Q. Portuguese Familial Hypercholesterolemia Study: presentation of the study and preliminary results. Rev. Port. Cardiol. 2006;25(11):999-1013. 6.http://vega.sanger.ac.uk/Homo_sapiens/Location/Chromosome?chr=19;r=19:1-58617616, consultado a 18/11/2014 2.Ana Isabel da Costa Freitas Caracterização Bioquímica e Molecular da Hipercolesterolemia Familiar na Região Norte e Centro de Portugal. 2010 7.http://vega.sanger.ac.uk/Homo_sapiens/Location/Chromosome?r=2%3A1-1000, consutado a 18/11/2014 3.http://fhportugal.pt/o-que-e-a-fh/, consultado a 18/11/2014 4.Gaspar I. Hipertecolesterolemia familiar . Do diagnóstico à prevenção cardiovascular . A propósito de um estudo holândes 8.http://vega.sanger.ac.uk/Homo_sapiens/Location/Chromosome?r=1%3A1-1000, consultado a 18/11/2014 5.Brasileira S. I Diretriz Brasileira de Hipercolesterolemia Familiar (HF). Arq. Bras. Cardiol. 2012;99(2):1-28 Brasileira S. I Diretriz Brasileira de Hipercolesterolemia Familiar 9.Rahman M, Rahman F, Fatima N, et al. SPECTRA OF ALTERNATIVE THERAPIES OF HYPERCHOLESTEROLEMIA BY DIETARY BIOACTIVES : EMPHASIS ON (HF). Arq. Bras. Cardiol. 2012;99(2):1-28 NUTRIGENOMICS OF POLYPHENOLS. 2013;1(1):1-7.
Baixar