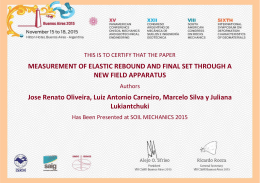
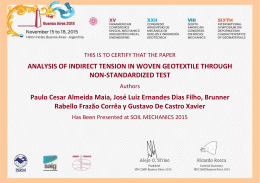
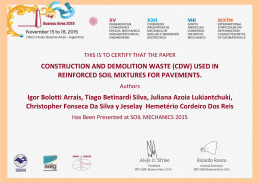
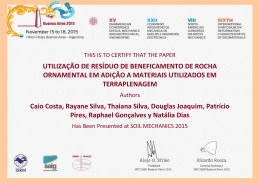
Original Article Control of Arterial Pressure in Patients undergoing Anti-Hypertensive Treatment in Brazil - Controlar Brazil Fernando Nobre1, Artur Beltrame Ribeiro2, Décio Mion Jr.3 Hospital das Clínicas da Faculdade de Medicina da USP1, Ribeirão Preto; Escola Paulista de Medicina - Hospital do Rim e Hipertensão2; Hospital das Clínicas da Faculdade de Medicina da USP3, São Paulo, SP - Brazil Abstract Background: Blood pressure (BP) control is crucial in arterial hypertension (AH). Objective: To determine the percentage of patients requiring specific BP control goals treated in medical offices throughout Brazil. Methods: Each researcher, from a total number of 291, had to evaluate, through conventional BP measurement performed during five consecutive days, the two first patients treated on that day. We determined the number of hypertensive patients treated for at least four weeks who presented BP control, according to the goals established for the risk group they belonged to. Results: A total of 2,810 patients were assessed in 291 centers. The individuals were divided in groups as follows: A (AH stages 1 and 2, low and moderate additional risk) = 1,054 (37.51%); B (AH and borderline BP, high additional risk ) = 689 (24.52%); C (AH and borderline BP, very high additional risk, including diabetic patients) = 758 (26.98%) and D (AH with nephropathy and proteinuria > 1 g/l) = 309 (11%). The BP means in the population were: 138.9 ± 17.1 and 83.1 ± 10.7 mmHg. Factors associated with a worse BP control were: age, abdominal circumference, diabetes, smoking and coronary disease. The BP control percentages in each of the groups were, respectively: 61.7; 42.5; 41.8 and 32.4%. Conclusion: The low BP control according to the predefined goals, as demonstrated in the results, reinforces the necessity to establish measures to promote better control rates. (Arq Bras Cardiol 2007;88(6):624-628) Key words: Blood pressure/drug effects; antihypertensive agents/therapeutic use. Introduction Arterial hypertension (AH) is a disease directly or indirectly responsible for the high rates of morbidity and mortality caused by cardiovascular diseases (CVD)1. This is a common worldwide scenario. The risk of cardiovascular events due to AH increases from BP means of 115 x 75 mmHg. For each 20 mmHg added to the systolic arterial pressure (SAP) or 10 mmHg added to the diastolic arterial pressure (DAP), there is a 2-fold risk increase, for both the occurrence of coronary artery disease (CAD) and cerebrovascular accident (CVA)2. Therefore, the classifications of the BP behavior have become more stringent, considering values < 140 x 90 mmHg as necessary for certain groups of patients. Table 1 shows the BP levels for each group, according to the V Brazilian Hypertension Guidelines (V DBH)3, considering their degree of risk. Mailing address: Fernando Nobre • Av. Independência, 3767 - Jd. Califórnia - 14026-150 - Ribeirão Preto, SP Brazil E-mail: [email protected], [email protected] Manuscript received April 08, 2009; revised manuscript received November 05, 2009; accepted November 18, 2009. 623 It is unquestionable that the BP control is directly related to the decrease in AH complications4. Thus, it is of utmost importance that patients with high BP be treated, so that they can benefit from the anti-hypertensive treatment5. Nevertheless, in spite of the evidence demonstrating the risk of arterial hypertension, as well as the benefits of its treatment, the number of diagnosed patients receiving anti-hypertensive therapy that presents BP control is still small worldwide6,1,6. Studies have demonstrated that the benefits of AH treatment are more significant when the control is more stringent7. In this context, guidelines that establish the therapy for hypertensive patients indicate BP goals to be attained with the treatment in specific groups with arterial hypertension8 (Table 1). This concern has been seen worldwide and can be observed in recently published studies9. In Brazil, there are no data regarding the prevalence of arterial hypertension in the general population, as well as on the control levels of patients undergoing therapy, under the same conditions of the studied population. Similarly, there are no data that express BP control in specific subgroups. The present study was designed to evaluate the percentage of patients undergoing anti-hypertensive treatment that have Nobre et al Controlar Brazil Original Article Table 1 - BP goals to be attained with treatment for arterial hypertension, according to the V DBH (V Brazilian Hypertension Guidelines)3 Categories Minimum BP goal* A - AH stage 1 and 2 Low and moderate risk < 140 x 90 mmHg B - AH and borderline BP High risk < 130 x85 mmHg C - AH and borderline BP Very high risk** < 130 x 80 mmHg D - AH with nephropathy and proteinuria > 1g/l < 120 x 75 mmHg 3. Frequency of the associated clinical conditions in the assessed patients; 4. Patients undergoing monotherapy; 5. Patients undergoing treatment with an association of anti-hypertensive drugs. Inclusion and exclusion criteria Inclusion criteria - Age ≥ 21 and < 80 years of either sex; *If the patient can tolerate it, BP values that are even lower than those indicated are recommended as treatment, and, if possible, the attainment of optimal BP values (≤ 120 x 80 mmHg). ** including diabetes mmellitus. AH - arterial hypertensiona; BP - ablood pressure. attained the goals established for their specific condition, having been assigned to four pre-defined categories in medical offices and clinics throughout Brazil. Methods The data collection and assessment were carried out between February and June 2008, after the Ethics Committee in Research of HC-FMRP-USP approved the study, to be carried out in multiple centers as proposed in the presented protocol. A total of 2,810 individuals were assessed by 291 medical research physicians, general practitioners, cardiologists or nephrologists, in medical offices, outpatient clinics or services of arterial hypertension, distributed throughout the four macroregions of Brazil as follows: North-Northeast region: 13.5%; Midwest region: 6.5%; Southeast region: 68% and South region, 12%. The protocol determined that each researcher should evaluate, during five consecutive days, the two first patients treated at the office or clinic that met the study inclusion criteria. Patients with medical insurance, including the Brazilian Public Health System (SUS) were assessed, as well as those who were treated at private medical offices, with or without free access to medication. Study characteristic The present was an observational study and the data were obtained from patients treated in medical offices and outpatient clinics throughout Brazil. The protocol did not foresee therapeutic intervention, aiming solely at observing, among others, the following aspects: 1. Relative number of patients undergoing treatment with SAP and DAP < 140 x 90 mmHg , respectively, menteregardless of their clinical condition; 2. Relative number of hypertensive patients who had presented, for at least four weeks, the control of systolic and diastolic arterial pressure, according to their individual goals, as established in Table 1; - Confirmed clinical diagnosis of hypertension and to be currently undergoing treatment with anti-hypertensive drug (monotherapy, fixed combination or open combination of drugs), according to the clinical history; - Regular use of anti-hypertensive medication for at least four weeks; - To be one of the two first patients assessed on the day; - To accept participating in the study, after being informed on the study procedures, risks, benefits and rights and reading and signing the free and informed consent form. Exclusion criteria - Secondary arterial hypertension; - Poor general health due to end-stage diseases; - Pregnant or breastfeeding women and those who had given birth less than two months before; - Regular use of corticósteroies, chemotherapy agenes or immunosuppressive drugs; - Chronic use of alcohol (daily or large amounts) or neuroleptic drugs; - Participation in another observational study sooner than three months after their possible inclusion in the present study. Criteris for data collections The demographic data were collected by the researchers and included age (in full years); height (in meters); weight (in kg); body mass index (BMI = kg/m2), sex, current smoking status (smoker or nonsmoker); diabetic nephropathy (present or not); left ventricular hypertrophy, detected by the electrocardiogram (present or not); coronary and/ or peripheral artery disease (present or not); heart failure (present or not); previous history of myocardial infarction and/ or cerebrovascular accident, based on patients’ files or their evaluation during the consultation. Information on the use of monotherapy or an association of drugs (fixed or open), as well as the medications being used for the treatment was also obtained by the researcher during patient evaluation. Blood pressure measurement The BP measurements were obtained according to the criteria established by the V DBH3.musing an automatic Microlife sphygmomanometer, model 3 BT0A validated by the British Hypertension Society, AA qualification, with three Arq Bras Cardiol 2010;94(5):623-630 624 Nobre et al Controlar Brazil Original Article different cuff models, according to the patient’s condition: adult, thin adult and obese adult. The BP was measured in the sitting position after 5 minutes of rest and two measurements were obtained consecutively, with a one-minute interval between them, with the objective of obtaining the actual BP value through the mean of these measurements. A third measurement was obtained, equally one minute after the second measurement, when the difference between the two first ones was > 5 mmHg. Statistical analysis Demographic data, as well as data on physical examination, associated clinical conditions and current antihypertensive treatments were descriptively summarized. The classificatory variables were described through the distribution of frequencies and percentages. Means, standard deviations, minimum and maximum values were used to describe continuous variables. Exact confidence intervals for the binomial distribution, with a 95% confidence interval (95%CI) were established for the proportion of patients that had achieved their goals for BP control, when considering the total number or the subgroups of patients. Factors that were predictive of BP control were explored by adjusting a logistic linear model. The factors predictive of non-control were also assessed using the same model. The SAS system (Statistical Analysis System), release 9.1.3 was used to perform all statistical analyses. Results Table 2 - Characteristics of the patients included in the study Characteristic Data obtained Age (years) 60.4 ± 12.4 Height (meters) 1.63 ± 0.9 Gender Male 1,095 (37.7%) Female 1,810 (62.3%) Weight (kg) 75.9 ± 15.4 Abdominal circumference (cm) 96.9 ± 12.5 Body mass index (kg/m ) 28.49 ± 4.9 Waist: hip ratio 0.94 ± 0.09 Smoking (number and percentage) 242 (8.4%) 2 Arterial pressure (mmHg) 138.8 ± 17.1 x 83.1 ± 10.7 Diabetes mellitus 563 (20.77%) Diabetic nephropathy 52 (1.92%) Obesity 1,049 (38.71%) Dyslipidemia 1,736 (64.06%) LV hypertrophy (through ECG) 461 (17.01%) Coronary artery disease 376 (13.87%) Peripheral artery disease 135 (4.98%) Congestive heart failure 67 (2.47%) Previous history of myocardial infarction 153 (5.65%) Previous history of cerebrovascular accident 78 (2.88%) No comorbidity 366 (13.51%) Other comorbidities 255 (9.41%) Characteristics of the studied individuals A total of 2,810 patients from 291 centers were assessed. The data on the individuals included in the study, as well as the prevalence of the clinical conditions and the associated risk factors are shown in Table 2. As for the risk stratification used to define the four groups, the distribution was as follows: Group A (hypertension 1 to 2 with low or middle risk): 1,054 (37.51%); Group B (hypertension or borderline behavior with high risk): 689 (24.52%); Group C (hypertension or borderline behavior with very high risk): 758 (26.98%) and Group D (arterial hypertension and kidney disease with protein loss > 1 g/24 h): 309 (10.99%) (Table 3). Arterial pressure control In total analysis, regardless of the individual’s condition, 1,497 (53.3%) of them presented BP < 140 x 90 mmHg. Considering the specific control targets desired for each of the groups, we obtained the following number of patients with systolic and diastolic arterial pressure control: Group A: 650 (61.7%); Group B: 293 (42.5%); Group C: 317 (41.8%) and Group D: 100 (32.4%). These data are shown in Table 4. Associated clinical conditions The numbers and percentages of the clinical conditions 625 Arq Bras Cardiol 2010;94(5):623-630 Table 3 - Distribution of the individuals according to the risk stratification (as established in the V DBH3) Risk stratification Number (%) Group A 1,054 (37.51) Group B 689 (24.52) Group C 758 (26.98) Group D 309 (10.99) Table 4 - Numbers and percentages of assessed individuals that presented control of the systolic and diastolic pressure, according to the goals defined by the DBH V3 Desired level Number (%) assessed Number (%) controlled A <140 x 90 mmHg 1,054 (37.51) 650 (61.7) B <130 x 85 mmHg 689 (24.52) 293 (42.5) C <130 x 80 mmHg 758 (26.98) 317 (41.8) D <120 x 75 mmHg 309 (10.99) 100 (32.4) 2,810 (100) 1,360 (46.5) Group Total Nobre et al Controlar Brazil Original Article associated with arterial hypertension in the studied group can be seen in Table 2. goals established for each one of the four risk classes they were allocated in. Treatment with monotherapy or with an association of drugs Impact of associated factors and blood pressure control Using a model of logistic regression, it was possible to establish that for each year of life added to the studied individual, the probability of BP control was 2% lower. A similar observation was verified regarding the abdominal circumference, by verifying that for each centimeter added to this parameter, the chance of BP control was also 2% lower. In the four groups with different risk levels, 913 of them (32.5%) used monotherapy, whereas the other 1,897 (67.5%) used more than one anti-hypertensive drug. The distribution of therapeutic classes being used during the study is shown in Table 5. Figure 1 shows the percentage of patients that met the As for the smoking status, the presence or not of diabetes mellitus and the presence or not of coronary artery disease, these chances of control were, respectively, 29%, 59% and 17% lower (Figure 2). Table 5 - Percentage distribution of patients treated with monotherapy and by classes used in the treatment and number of associated drugs Type of treatment Discussion Number (%) of individuals Monotherapy 913 (32.5) ARB II 369 (40.5) ACEI 210 (23) CCA The evaluation of arterial hypertension prevalence, awareness, treatment and control has been the object of global study, due to the importance of the topic104,10,11-12. The knowledge of BP control in specific groups according to their risk stratification, however, has not been established in private medical offices and outpatient clinics (private medical care system) in Brazil. 210 (23) Beta-blocker 150 (16.5) Diuretics Isolated data obtained from assessed health units (secondary and tertiary public medical centers and healthcare facilities) have demonstrated wide-ranging BP control levels. 103 (11.3) Association 1,897 (67.5) 2 drugs 1,210 (63.8) 3 drugs 502 (26.5) More than 3 drugs 184 (9.7) Among the population of the town of Tubarão, state of Santa Catarina, Brazil, the percentages of BP prevalence, awareness, treatment and control were, respectively: 40.5%; 55.6%; 46.8% and 21.6%11. ARB II - angiotensin II receptor blocker; ACEI - angiotensin-converting enzyme inhibitors; CCA - calcium channel antagonists. Mion et al12 assessed the BP control in patients treated at 67.6 61.7 58.2 57.5 42.5 38.3 41.8 Controlled 32.4 Noncontrolled Figure 1 - Percentages of controlled patients in accordance with the goals established for each one of the four risk classes they were allocated in, according to their stratification. Arq Bras Cardiol 2010;94(5):623-630 626 Nobre et al Controlar Brazil Original Article Age - 0.989* (p=0.0012) AC - 0.983** (p<0.001) Smoker - 0.71*** (p<0.0192) Diabetes - 0.41*** (p<0.0001) CAD - 0.83*** (p=0.1247) 0.5 1 Figure 2 - Factors related to a lower BP control in all studied groups. AC - abdominal circumference; CAD - coronary artery disease. Maximal verisimilitude method determination of the logistic regression model - 95%CI. *Chance of BP control decreases 2% with each added year of life. **Chance of BP control decreases 2% with each cm added to the AC. ***Yes x no. 10 hypertension leagues (São Luis, Maceió, Salvador, Goiania, Rio de Janeiro, three in São Paulo, Porto Alegre and Sorocaba) and found that in a total of 1,998 individuals, 56% of them presented BP < 140 x 90 mmHg12. Among patients treated at the Hypertension Outpatient Clinic of HC FMRP USP, in Ribeirao Preto, followed during the year of 1995, 33.3% of them presented BP <140 x 90 mmHg13. Mancia et al14 observed that even in large clinical trials, usually very stringently monitored, the level of BP control did not show the desired results. When these assessments favor groups in which the control goals are necessarily lower, these values tend to be even lower9. The main results of the present study indicate a control rate of systolic and diastolic arterial pressure in the global analysis of 53.3%, regardless of which subgroup they refer to. Considering the specific subgroups of patients from medical offices and outpatient clinics from the different regions of the country, 61.7% in Group A (AH stages 1 and 2 with low and moderate risk); 42.5% in Group B (AH and borderline BP with high risk); 41.8% in Group C (AH and borderline BP with very high risk, including diabetics) and 32.4% in Group D (AH with nephropathy and proteinuria > 1 g/l) had achieved the desired BP goals. It is worth mentioning that, in the present study, which focused on a population who had or did not have free access to medication, these control percentages, apparently high in comparison to what is observed in the general population, are still below the expected ones. Ma and Randall15 evaluated the BP treatment and control in medical offices in the United States between 2003 and 2004. The mean BP observed by the authors was 141 x 81 mmHg in patients without comorbidities and 143 x 79 mmHg 627 Arq Bras Cardiol 2010;94(5):623-630 in those who presented associated diabetes or nephropathy. In the present population, the general mean of BP was 138.8 ± 17.1 x 83.1 ± 10.7 mmHg. Whereas in the United States these authors found 42% of individuals without comorbidities with BP < 140 x 90 mmHg, in the present study, among those classified as belonging to Group A (AH stages 1 and 2 with low and moderate risk), 61.7% presented BP control. Regarding the group considered by the authors as presenting the higher risk (patients with associated diabetes and/or nephropathy), this rate, considering an ideal BP level < 130 x 80 mmHg, was 20%. This rate was approximately 30% to 40% in a population with a similar profile in the present study. Interestingly, when assessing the drugs more frequently used in the United States, it was observed that diuretics were the first choice (46%), followed by ACEI (37%), beta-blockers (36%) and ARB II (24%). When assessing the medications that are generally prescribed in Brazilian medical offices, the order is different (Table 5), with ARB II being the ones most frequently prescribed. However, the use of medications in monotherapy or in association with other drugs exhibits a very similar situation when comparing the medical practice in the Unites States with that in Brazil. In that study, 58% of the patients used a combination of medications, whereas the present study shows that 67.5% of patients did the same. Another study, by McInnis et al16, observed that only 49% to 51% of the patients evaluated by them received monotherapy. This study, which was carried out in Canada, showed that 62% of the patients used ARB II, similarly to what was observed in the present study. The percentages of patients with controlled BP in the present study, according to the gols defined by the V DB H and also by other similar documents, are optimistic in comparison to other observations. It is, however, necessary to mention that for Groups A, B, C and D we have, respectively, 38.3%; 57.5%; 58.2% and 67.6% of individuals with noncontrolled BP. Nobre et al Controlar Brazil Original Article Due to their importance and impact, the associations of individual variables, which, when present, act as additional risk factors and can interfere with the desired BP control, were also assessed. In this sense, we observed that for each centimeter added to the abdominal circumference or for each year of life gained, the BP control is reduced by 2%. Similarly, the habit of smoking, the presence of diabetes mellitus and coronary artery disease were determinants of a lower chance of blood pressure control (Figure 2). New evidence has shown that the abdominal circumference is an acknowledged risk factor for cardiovascular disease caused by increased visceral fat19. The present study showed that this parameter increased the difficulty to control the BP, even for small variations such as 1 cm. The more difficult BP control presented by patients with diabetes and nephropathy, is due, among other factors, to the fact this population has lower BP goals than those presented by individuals without these diseases, with the objective of protecting target organs from vascular injury caused by hypertension20,21. A final observation is opportune and necessary. Why is the blood pressure control so seldom achieved? Perhaps that is the biggest challenge to be overcome by all professionals who work with arterial hypertension. Ogedegbe22 and Nobre et al13, among others, studied the reasons why patients do not maintain a continuing treatment and only a small percentage of them achieve BP control. The factors that contribute to the low rate of BP control are focused on variables associated with the physician and the patient and must be considered: low adherence to prescriptions, medication costs, personal beliefs on the treatment and the disease itself, low frequency of consultations, adverse effects, among others. It is, however, necessary to seek better BP control, considering the evidence regarding the benefits obtained with its control. The present study brings contributions regarding the identification of the number of individuals undergoing treatment in medical offices and clinics in Brazil, who present BP control according to the established goals and their clinical conditions. It is also useful so that actions can be taken in search of better control rates, based on the conclusions drawn by the study. Nevertheless, it has limitations. Among them, we should mention that the sample is not representative of the population of patients with arterial hypertension in Brazil, but rather of those patients treated in private clinics and medical offices (vs. those treated at the Brazilian Public Health System - SUS). For this reason, one must state that these data refer to this specific study population. Finally, it is worth mentioning that the selection of the participating centers was not randomly performed, but defined by the willingness of the individuals invited to participate in the study. Researchers participating in the Controlar BRAZIL Study Abrao Luiz Jablonka, Aderito das Neves Coelho, Adil Abdul Latif Fares, Adriana Carvalho Ribeiro, Adriano Assis Mendes, Alberto Pianta Neto, Alcione Maria Simoes, Alcy Maria Pinheiro, Aldo Odilon Xavier Vitoria, Alessandro F. Chagas, Alex Gules Mello. Alexandra O. Mesquita, Alexandre E. P. C. Lucena, Alexandre Jorge Andrade Negri, Alexei A. Der Bedrossian, Alfredo Jose P. G Leitão, Alice Porfirio Oliveira, Álvaro Álvares da Silva, Amancio Valois, Ana Valéria S. G. Ramirez, Andre Luiz S. Ferreira, Angela Cristina Farias, Anibal Barros Jr., Anibal Prata Barbosa, Antônio Almeida Braga, Antonio Carlos Lopes, Antonio da Silva Junior, Antonio Edmond Ghattas, Antonio José L. Jorge, Antônio Mendes P. Neto, Antonio Ribeiro P. Neto, Ariane L.Chair, Armando C. Balbinotti, Armando M. Maranhão, Arnaldo Lemos Porto, Ary Dos Santos Mesquita, Audes D. de M. Feitosa, Augusto O. S. Coutinho, Augusto Terranova Rocha, Badir Hassan Awad, Bruno Dumas Galvão, Carlos Alberto Chicca, Carlos Alberto Oliveira, Carlos Alberto Penna Fernandes, Carlos Alberto Teles Drews, Carlos Antônio de Souza Andrade, Carlos Cesar da Silva, Carlos Delmar Ferreira, Carlos E. Dos Santos, Carlos Eduardo Ornela, Carlos Manoel R. Costa, Carlos Roberto Ito, Celia Regina Galeotti, Celso Machado Cury, Cesar Augusto de Carli, Chris Machado Paulini de Andrade, Cicero Emanuel Barros da Nóbrega, Cícero Roberto Azulay, Claudia B. B. Alcipret, Claudia Kazuya Yamada, Cláudio David La Terza, Cláudio Vieira Catharina, Cleiber Antônio dos Santos Teixeira, Cristiano Jaeger, Cristina Maria Marcolan Quitete, Cristina Pimentel Seba, Daniel Carvalho Alarcon Gonçalves, Daniel José da Silva Filho, Daniele Mattos, Daniella Rosano, Darci Alcoforado Quirino, Dario Cezar Vasconcello, Darlan Carneiro Silva, Davi Gomes, Davis Taublib, Delma Maria S. H. Gasparotti, Denise C. G. de Oliveira, Denise L. de Carvalho, Denise Maria Soares Mohr, Denize Vozniak, Dorival Moraes Ferreira, Douglas Conrado Schimidt, Dyrlei da Cunha Filho, Edgar Pessoa de Melo, Edgard Matheus da Silva, Edinaldo Jorge P. Malheiros, Edson A.Santos Jr., Eduardo Calixto Saliba, Eduardo Costa Barbosa, Eduardo de Camargo, Eduardo Rodolpho Ferber, Edvaldo do N. Barbosa, Elaine Brandão Soares, Eliane Pereira Passos, Elio Lumertz Rolim, Emerson Clayton Borges, Emerson de Morais Silva, Emerson Costa Porto, Emmanuel Pires Abreu, Eric Murasca, Ernesto Jose F.Puppi, Evandro G. de Souza, Evandro Veiler Ferrari, Fabiano de O. Martins, Fabio Viegas Pimenta, Fátima E. F. de O. Negri, Fausto Duarte Guimarães, Evandro Veiler Ferrari, Fabiano de O. Martins, Fabio Viegas Pimenta, Fátima E. F. de O. Negri, Fausto Duarte Guimarães, Fernanda Baptista Lins, Fernando Antônio Flores, Fernando Augusto Neiva, Fernando Freire Maia, Fernando Funari Vivolo, Fernando Lara Roquete, Fernando Resende, Flávio Brugnara Veloso, Flavio Ferramola Pozzuto, Flávio Roberto Salatino, Floramil Castilho, Francisco Delano Macedo, Francisco Jose Godoi, Francisco R. de P. Filho, Frederico Baumann, Germano M. P. Santos, Gerson N. Guimarães, Gilberto Gheur Ramos, Gisel Pereira de C. Junior, Gisely Martinelli Pudo, Gonzalo A.H.Gutierrez, Gustavo Cortez Vieira, Helcio F. Salmazo, Hélio Cesar Telles Primo, Helio Rubens Crialezi, Helio Soares, Henrique Miller Balieiro, Hermilo Borba Carvalho Neto, Hidemburgo de B. Carvalho Filho, Hugo Pinheiro Faria, Irineu B.Moreno, Ivan Cardoso de Sá, Ivan Sergio Baddini, Ivna Maria B. de Macedo, Izo Helber, Jaime Grynberg, Jamil Cherrem Scheneider, Jessica Myriam A. Garcia, João Alberto R. Oliveira, João Batista de S. E Silva, João Luiz Figueiredo, João Nei G Fernandes, João Nobrega A. Arq Bras Cardiol 2010;94(5):623-630 628 Nobre et al Controlar Brazil Original Article Filho, João Voino Nicolitz, Joel Albuquerque P. Júnior, Jones Moraes, Jose Alves Patricio Junior, Jose Augusto Condina, José Campos Filho, José Carlos Ferreira da Silva Filho, José Carlos Robalinho, Jose D. C. Solano Aliaga, José Eduardo D’ottaviano, Jose Ibis Coelho das Neves, José Joaquim F. Raposo Filho, José Roberto Brito, José Roberto Redini, Jose Wladimir Tambelli Pires, Karen Oliveira Reis, Keffel Antonio Pereira, Kerginaldo Paulo Torres, Keyla Alves Ferreira Abdala, Kleber Natal, Lazaro Fernandes de Miranda, Leandro Espindola Roese, Lenilza Martins, Loredana Mantovano, Lucélia B.N. C. Magalhães, Luciana Frison Spiazzi, Luciano Maia de Melo, Luciano Mauricio de Abreu Filho, Lúcio Lobo Leite Vitarelli, Ludenulfo Cruz Lacet, Ludmila Daru Rey, Luiz Artur Sutic da Silva Paes, Luiz Alberto Barreto, Luiz Antonio D. M. Oliveira, Luiz Benjamin Francisco, Luiz Carlos Pacheco, Luiz Claudio da Silva Félix, Luiz Claudio Mattos, Luiz Kencis Jr, Luiz Sergio Alves Silva, Manoel Estrela Obregon Jr, Mara Lia Pereira, Marcel Vezzaro ®, Marcelo Ferraz Sampaio, Marcelo Lerch Sturmer, Marcelo Rava Campos, Marcelo Russo, Marcelo Sapucaia, Marcelo Silva Seixas, Marcelo Xavier, Marcia Santos Guimarães, Marcio Amuy, Marcio Franceschi Britto, Marco Antonio de M. Alves, Marco Antonio de V. Barros, Marcos Antonio Lacerda, Marcos Boechat Lopes, Marcos Cairo Vilela, Marcos Roberto Volpi, Marcos Vinicios Andrade, Marcus Vinicius P. Matos, Marcus Vinicíus Sales, Maria Cristina Torres Cardoso, Maria da C. B. De A. F. Carvalho, Maria de Fátima M. Castro, Maria do Carmo Maia Reis, Maria do Carmo Orge Rodrigues, Maria Elizabete Silva Penido, Maria Fatima Oliveira P. Alencar, Maria Goreth P. Souza, Maria Ivone de C. Abreu, Maria Rita Veríssimo, Mario Sérgio Julio Cerci, Marlene Nakamura de Villalon, Martha Demetrio Rustum, Maurício Gonçalves Zanon, Maurício Tamura Saraiva do Brasil, Max Weyler Nery, Miraldo Pereira Matos, Miriam de Souza Protásio Mota, Nadja Sotero, Ned Maciel Oliveira, Neire Niara, Nelson Coifman Goldemberg, Newton Ferreira Rodrigues, Ney da Silva Moutinho, Nilton Leme, Olavo de Carvalho Freitas, Olympia Dias de Azevedo Bastos, Omar Sérgio Lutz, Oscar Yoshinori Ikari, Otacílio Araujo Silva, Patricia Eunice dos Santos, Paulo Eduardo Seade Serra, Paulo Miqueloti, Paulo Roberto de Souza, Paulo Rubens Moreno da Silva, Paulo Sergio de Osório Almeida, Paulo Sergio Lopes Soares, Paulo Sergio Porto, Pedro Schimidt, Pedro Vendramini Neto, Peri Sampaio Padua Neto, Plauto Jose Gouveia, Priscila Cotia Pinheiro, Rachel D. C. Paes de Aaraujo, Rafael Braga Pimenta, Raimundo Jose Vieira de Assis, Ramon Farras Lopes, Raphael Damore Zardo, Regina Celia Villela de Souza, Reinaldo Mattos Hadlich, Renan Canibal Pires, Renato Fernandes Pinheiro, Renato Schuck Saraiva, Rene Domingos Castagnino, Reynaldo A. M. da Costa Miranda, Ricardo Alvarenga, Ricardo Barcia Barbeira, Ricardo Cairo de Camargo, Ricardo Mendonça Costa, Rita de Cássia Oliveira, Robert Dancour, Roberto Estrazulas Mayer, Roberto Sandes Leal, Robson de Castro Ayala, Robson Luiz de Assis, Rodolfo Ernesto Suriano, Rodolfo Malta Alencar, Rodrigo 629 Arq Bras Cardiol 2010;94(5):623-630 Caetano Pimentel, Rogério Kraukauer, Rogério Martins Ruiz, Romário Rui de Souza, Rosana Graziane Mendes, Rosana Stella Grossman, Rute Puiatti Roman, Ruth de Almeida Medeiros, Ruy Barbosa Jr, Sadi de Carvalho Filho, Samira Kaissa Nasr, Samuel Ellovitch, Sandra Maria Figueiredo, Sandro Silva Vilella, Selem Safar T. Pinto, Sergio Baiocchi Carneiro, Sergio Fajardo Assumpção, Sergio Francisco Ruiz, Sérgio José O. de A. E Silva, Sérgio Luiz Nascimento, Sergio P. A B. de Camargo, Sergio Salim Saud, Shirley Mioto, Sidney C. Fernandes, Siegmar Starke, Silvana Purri B. Hemetério, Silvano Jorge Pessanha, Silvia Regina V. de Carvalho, Silvio Hock de Paffer Filho, Silvio Luiz Priori, Sirley da Silva Queiroz, Solange Veiga F. Faria, Soriano Furtado Neto, Suely Lourdes Pacote, Tatiana do Carmo Borges, Telemaco Luiz da Silva Jr., Telma Ferrais S. Machado, Terezinha Mara S. Steele, Théo Fernando Bub, Thiers Ribeiro Chagas, Tjioe Kok Kie, Tomas D. G. Mesquita, Valdir Pereira Aires, Victor Luiz Santos Haddad, Victor Neves da Fonseca, Vilma Cichelli Fernandes, Vilma Helena Burlamaqui, Vlademir José Lustosa, Walmir Ratier Thomaz, Walter de Assumpção, Walter Rello de Araujo Filho, Weimar Kunz Sebba Barros, Wesley Roberto Hossri, Wilson Alvear Torrano Machado, Wilson Dagone Junior, Wilson Elias Abrão, Wilson Kioshima, Wilson Koury Filho, Wladimir Magalhães de Freitas, Wladmyr de Carvalho Machado, Yanko Gonçalves Melo, Yoshio Asanuma, Zenita Portela Pavani. Acknowledgments The authors would like to thank the statistical analysis work carried out by Statistika Consulting. We also acknowledge the work of the Clinical Research Team of Sanofi-Aventis Pharmaceutical, Ltda. in carrying out this project, as well as of Dr. Maria Eliane Magalhaes (RJ), Dr. Celso Amodeo (SP), Dr. Francisco H. Fonseca (SP), Dr. Oscar Dutra (RS), Dr. Hilton Chaves Jr. (PE), Dr. Andrea A. Brandão (RJ), Dr. Paulo C. Jardim (GO), Dr. Jose Marcio Ribeiro (MG), Dr. Luis Carlos Bodanese (RS), Dr. Marco A. Mota Gomes (AL), Dr. Edgard Pessoa de Melo (PE) and Dr. Antonio Carlos Palandri Chagas (SP). Potential Conflict of Interest No potential conflict of interest relevant to this article was reported. Sources of Funding This study was funded by Sanofi-Aventis and Sociedade Brasileira de Hipertensão. Study Association This study is not associated with any post-graduation program. Nobre et al Controlar Brazil Original Article References 1. Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo JL Jr, et al. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation and Treatment of High Blood Pressure: the JNC 7 report. JAMA. 2003; 289 (19): 2560-72. 2. Lewington S, Clarke R, Chizibash N, Peto R, Collins R. Prospective Study Collaboration. Age specific relevance of usual blood pressure to vascular mortality: a meta-analysis of individual data for one million adults in 61 prospective studies Lancet. 2002; 360 (14): 1903-13. 3. Mion Jr D, Kohlmann Jr O, Machado CA, Amodeo C, Gomes MAM, et al. Sociedade Brasileira de Cardiologia / Sociedade Brasileira de Hipertensão. V Diretrizes brasileiras de hipertensão. Rev Bras Hipertens. 2006; 14 (4): 257-306. 4. Wolf-Mayer K, Cooper RS, Kramer HB, Banegas JR, Giampaoli S, Joffres MR, et al. European hypertension treatment and control in five countries, Canada and United States. Hypertension. 2004; 43 (1): 10-7. 5. Turnbull F. Blood Pressure Control Lowering Treatment Trialist’ Collaboration: Effects of different blood-pressure-lowering regimes on major cardiovascular events: results of prospectively-designed overviews of randomized trials. Lancet. 2003; 362 (9395): 1527-35. 6. Williams B. The year of hypertension. J Am Coll Cardiol. 2006; 48 (8): 1698-711. 7. Hansson L, Zanchetti A, Carruthers SG, Dahlöf B, Elmfeldt D, Julius S, et al. Effects of intensive blood pressure lowering and low-dose aspirin in patients with hypertension: principal results of the HOT (Hypertension Optimal Study) randomized trial. Lancet. 1998; 351 (9118): 1755-62. 8. Mancia G, Backer G, Dominiczak A, Cifkova R, Heagesty AM, Kjeldsen SE, et al. 2007 Guidelines for the Management of Arterial Hypertension. The Task Force for the Management of Arterial Hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). J Hypertens. 2007; 25 (6): 1105-87. 9. Borzechi AM, Wong AT, Hickey E , Berlowitz DR. Hypertension control – how well are we doing? Arch Intern Med. 2003; 163 (22): 2705-11. 10.Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo JL Jr, et al. National Heart, Lung, and Blood Institute; National High Blood Pressure Education Program Coordinating Committee. Seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. Hypertension. 2003; 42 (6): 1206-52. 11.Pereira MR, Coutinho MSSA, Freitas PF, D´Orsi E, Benardi A, Hass R. Prevalência, conhecimento, tratamento e controle de hipertensão arterial sistêmica na população adulta urbana de Tubarão, Santa Catarina, Brasil, em 2003. Cad Saúde Pública. 2007; 23 (10): 2363-74. 12.Mion Jr D. Hipertensão arterial. [Acesso em 2009 jun 23]. Disponível em: WWW.deciomion.com.br 13.Nobre F, Silva CP, Lima NKC, Santos LAC, Veiga EV, Nogueira MS, et al. Características e resultados do atendimento de pacientes na Unidade de Hipertensão do Hospital das Clínicas da Faculdade de Medicina de Ribeirão Preto da Universidade de São Paulo. Rev Bras Med. 2000; 57 (7): 694-708. 14.Mancia G, Grassi G. Systolic and diastolic blood pressure control in antihypertensive drug trials. J Hypertens. 2002; 20 (8): 1461-4. 15.Ma J, Stafford RS. Screening, treatment, and control of hypertension in US private physician offices, 2003-2004. Hypertension. 2008; 51 (5): 1275-81. 16.McInnis NH, Fodor G, Moy Lum-Kwong M, Leenen FH. Antihypertensive medication use and blood pressure control: a community-based crosssectional survey (ON-BP). Am J Hypertens. 2008; 21 (11): 1210-5. 17.Williams B, Poulter NR, Brown MJ, Davis M, McInnes GT, Potter JF, et al. The BHS guidelines working party, for the British Hypertension Society. British Hypertension Society guidelines for hypertension management 2004 (BHSIV): summary. BMJ. 2004; 328 (7440): 634-40. 18.2003 European Society of Hypertension–European Society of Cardiology guidelines for the management of arterial hypertension - Guidelines Committee. J Hypertens. 2003; 21 (6): 1011-53. 19.Yusuf S, Hawken S, Ounpuu S, Dans T, Avezum A, Lanas F, et al. on behalf of the INTERHEART Study Investigators. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): case-control study. Lancet. 2004; 364 (9438): 937-52. 20.Holman RR, Paul SK, Bethel MA, Neil HA, Matthews DR. Long-term follow-up after tight control of blood pressure in type 2 Diabetes. N Engl J Med. 2008; 359 (15): 1565-76. 21.Lazarus JM, Bourgoignie JJ, Buckalew VM, Greene T, Levey AS, Milas NC, et al. Achievement and safety of a low blood pressure goal in chronic renal disease: the Modification of Diet in Renal Disease Study Group. Hypertension. 1997; 29 (2): 641-50. 22.Ogedegbe G. Barriers to optimal hypertension control. J Clin Hypertens (Greenwich). 2008; 10 (8): 644-6. Arq Bras Cardiol 2010;94(5):623-630 630
Baixar