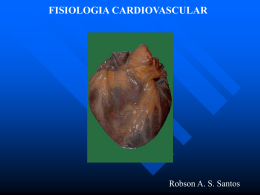
www.arquivosonline.com.br Sociedade Brasileira de Cardiologia • ISSN-0066-782X • Volume 105, Nº 2, August 2015 Right Kidney Left Kidney Figure 1 – Renal Denervation Procedure. Selective angiography performed with a 7-F Renal Double Curve guide catheter in the left anterior oblique 10° projection. Note that a single renal artery supplies each kidney and that the caliber and length of the main renal artery prior to bifurcation is ideally suited to denervation. Page 203 Editorial Role Of MMP-2 and MMP-9 in Resistance to Drug Therapy in Patients Editorial Considerations on the New Clinical and Surgical Perspectives with Resistant Hypertension of Brazilian Cardiology Reduced Progression of Cardiac Allograft Vasculopathy with Routine Special Article Use of Induction Therapy with Basiliximab Executive Summary – Guideline on Telecardiology in the Care of Brief Communication Patients with Acute Coronary Syndrome and Other Cardiac Diseases Original Articles Myocardial Scintigraphy in the Evaluation of Cardiac Events in Patients without Typical Symptoms New Exercise-Dipyridamole Combined Test for Nuclear Cardiology in Insufficient Effort: Appropriate Diagnostic Sensitivity Keeping Diastolic Function in Paced Children with Cardiac Defects: Septum vs Apex Review Article Nobel Prizes: Contributions to Cardiology Viewpoint Sudden Death in Brazil: Epilepsy Should be in Horizon Exercise Prognosis Clinicoradiological Session Cardiac Surgery Costs According to the Preoperative Risk in the Pulmonary Valve Lesion after Double Valvotomy in Childhood Brazilian Public Health System Case 6 / 2015 – A 27-Year-Old Male Patient with Double Aortic and Case Report Screening for Fabry Disease in Left Ventricular Hypertrophy: Profound Sustained Hypotension Following Renal Denervation: Documentation of a Novel Mutation A Dramatic Success? Heart Failure with Preserved Left Ventricular Ejection Fraction in Image Patients with Acute Myocardial Infarction Giant Right Atrial Mass Following Surgical AorticValve Replacement Tramadol Alleviates Myocardial Injury Induced by Acute Hindlimb Letter to the Editor Ischemia Reperfusion in Rats Subclinical Ventricular Dysfunction Detected by Speckle-Tracking Two Effects of One Resistance Exercise Session on Vascular Smooth Muscle of Hypertensive Rats Years after Use of Anthracycline Erratum A JOURNAL OF SOCIEDADE BRASILEIRA DE CARDIOLOGIA - Published since 1948 Contents Editorial Editorial Considerations on the New Clinical and Surgical Perspectives of Brazilian Cardiology Paulo Roberto B. Evora and Alfredo J. Rodrigues .....................................................................................................................................................................page 103 Special Article Executive Summary – Guideline on Telecardiology in the Care of Patients with Acute Coronary Syndrome and Other Cardiac Diseases Mucio Tavares de Oliveira Jr., Leonardo Jorge de Paula, Milena Soriano Marcolino, Manoel Fernandes Canesin .....................................................................................................................................................................page 105 Original Articles Nuclear Cardiology and PET Myocardial Scintigraphy in the Evaluation of Cardiac Events in Patients without Typical Symptoms Paola Emanuela Poggio Smanio, Juliana Horie Silva, João Vitor Holtz, Leandro Ueda, Marilia Abreu, Carlindo Marques, Leonardo Machado .....................................................................................................................................................................page 112 New Exercise-Dipyridamole Combined Test for Nuclear Cardiology in Insufficient Effort: Appropriate Diagnostic Sensitivity Keeping Exercise Prognosis Inés Vidal Cortinas, Mario Beretta, Omar Alonso, Fernando Mut .....................................................................................................................................................................page 123 Cardiac Surgery - Adults Cardiac Surgery Costs According to the Preoperative Risk in the Brazilian Public Health System David Provenzale Titinger, Luiz Augusto Ferreira Lisboa, Bruna La Regina Matrangolo, Luis Roberto Palma Dallan, Luis Alberto Oliveira Dallan, Evelinda Marramon Trindade, Ivone Eckl, Roberto Kalil Filho, Omar Asdrúbal Vilca Mejía, Fabio Biscegli Jatene .....................................................................................................................................................................page 130 Epidemiology Screening for Fabry Disease in Left Ventricular Hypertrophy: Documentation of a Novel Mutation Ana Baptista, Pedro Magalhães, Sílvia Leão, Sofia Carvalho, Pedro Mateus, Ilídio Moreira .....................................................................................................................................................................page 139 Arquivos Brasileiros de Cardiologia - Volume 105, Nº 2, August 2015 Ischemia/Myocardial Infarction Heart Failure with Preserved Left Ventricular Ejection Fraction in Patients with Acute Myocardial Infarction Lucas Antonelli, Marcelo Katz, Fernando Bacal, Marcia Regina Pinho Makdisse, Alessandra Graça Correa, Carolina Pereira, Marcelo Franken, Anderson Nunes Fava, Carlos Vicente Serrano Junior, Antonio Eduardo Pereira Pesaro .....................................................................................................................................................................page 145 Tramadol Alleviates Myocardial Injury Induced by Acute Hindlimb Ischemia Reperfusion in Rats Hamed Ashrafzadeh Takhtfooladi, Adel Haghighi Khiabanian Asl, Mehran Shahzamani, Mohammad Ashrafzadeh Takhtfooladi, Amin Allahverdi, Mohammadreza Khansari .....................................................................................................................................................................page 151 Exercising Effects of One Resistance Exercise Session on Vascular Smooth Muscle of Hypertensive Rats Tharciano Luiz Teixeira Braga da Silva, Marcelo Mendonça Mota, Milene Tavares Fontes, João Eliakim dos Santos Araújo, Vitor Oliveira Carvalho, Leonardo Rigoldi Bonjardim, Márcio Roberto Viana Santos .....................................................................................................................................................................page 160 Hypertension Role Of MMP-2 and MMP-9 in Resistance to Drug Therapy in Patients with Resistant Hypertension Leandro Lacerda, Ana Paula de Faria, Vanessa Fontana, Heitor Moreno, Valéria Sandrim .....................................................................................................................................................................page 168 Heart Transplantation - Clinical Reduced Progression of Cardiac Allograft Vasculopathy with Routine Use of Induction Therapy with Basiliximab Ricardo Wang, Lidia Ana Zytynski Moura, Sergio Veiga Lopes, Francisco Diniz Affonso da Costa, Newton Fernando Stadler Souza Filho, Tiago Luiz Fernandes, Natália Boing Salvatti, José Rocha Faria-Neto .....................................................................................................................................................................page 176 Brief Communication Diastolic Function in Paced Children with Cardiac Defects: Septum vs Apex Michel Cabrera Ortega, Adel Eladio Gonzalez Morejon, Giselle Ricardo Serrano, Dunia Barbara Benitez Ramos .....................................................................................................................................................................page 184 Review Article Nobel Prizes: Contributions to Cardiology Evandro Tinoco Mesquita, Luana de Decco Marchese, Danielle Warol Dias, Andressa Brasil Barbeito, Jonathan Costa Gomes, Maria Clara Soares Muradas, Pedro Gemal Lanzieri, Ronaldo Altenburg Gismondi .....................................................................................................................................................................page 188 Viewpoint Sudden Death in Brazil: Epilepsy Should be in Horizon Fulvio Scorza and Paulo José Ferreira Tucci .....................................................................................................................................................................page 197 Arquivos Brasileiros de Cardiologia - Volume 105, Nº 2, August 2015 Clinicoradiological Session Case 6 / 2015 – A 27-Year-Old Male Patient with Double Aortic and Pulmonary Valve Lesion after Double Valvotomy in Childhood Edmar Atik .....................................................................................................................................................................page 199 Case Report Profound Sustained Hypotension Following Renal Denervation: A Dramatic Success? Ganiga Srinivasaiah Sridhar, Timothy Watson, Chee Kok Han, Wan Azman Wan Ahmad .....................................................................................................................................................................page 202 Image Giant Right Atrial Mass Following Surgical AorticValve Replacement Teresa Bastante and Fernando Alfonso .....................................................................................................................................................................page 205 Letter to the Editor Subclinical Ventricular Dysfunction Detected by Speckle-Tracking Two Years after Use of Anthracycline Aguinaldo Figueiredo Freitas Jr., Raquel Oliveira Santos, Salvador Rassi .....................................................................................................................................................................page 206 Erratum .....................................................................................................................................................................page 208 Arquivos Brasileiros de Cardiologia - Volume 105, Nº 2, August 2015 www.arquivosonline.com.br A JOURNAL OF SOCIEDADE BRASILEIRA DE CARDIOLOGIA - Published since 1948 Scientific Director Maria da Consolação Vieira Moreira Interventionist Cardiology Pedro A. Lemos Chief Editor Luiz Felipe P. Moreira Pediatric/Congenital Cardiology Antonio Augusto Lopes Associated Editors Arrhythmias/Pacemaker Mauricio Scanavacca Clinical Cardiology José Augusto Barreto-Filho Non-Invasive Diagnostic Methods Carlos E. Rochitte Surgical Cardiology Paulo Roberto B. Evora Basic or Experimental Research Leonardo A. M. Zornoff Epidemiology/Statistics Lucia Campos Pellanda Arterial Hypertension Paulo Cesar B. V. Jardim Ergometrics, Exercise and Cardiac Rehabilitation Ricardo Stein First Editor (1948-1953) † Jairo Ramos Editorial Board Brazil Aguinaldo Figueiredo de Freitas Junior (GO) Alfredo José Mansur (SP) Aloir Queiroz de Araújo Sobrinho (ES) Amanda G. M. R. Sousa (SP) Ana Clara Tude Rodrigues (SP) André Labrunie (PR) Andrei Sposito (SP) Angelo A. V. de Paola (SP) Antonio Augusto Barbosa Lopes (SP) Antonio Carlos C. Carvalho (SP) Antônio Carlos Palandri Chagas (SP) Antonio Carlos Pereira Barretto (SP) Antonio Cláudio L. Nóbrega (RJ) Antonio de Padua Mansur (SP) Ari Timerman (SP) Armênio Costa Guimarães (BA) Ayrton Pires Brandão (RJ) Beatriz Matsubara (SP) Brivaldo Markman Filho (PE) Bruno Caramelli (SP) Carisi A. Polanczyk (RS) Carlos Eduardo Rochitte (SP) Carlos Eduardo Suaide Silva (SP) Carlos Vicente Serrano Júnior (SP) Celso Amodeo (SP) Charles Mady (SP) Claudio Gil Soares de Araujo (RJ) Cláudio Tinoco Mesquita (RJ) Cleonice Carvalho C. Mota (MG) Clerio Francisco de Azevedo Filho (RJ) Dalton Bertolim Précoma (PR) Dário C. Sobral Filho (PE) Décio Mion Junior (SP) Denilson Campos de Albuquerque (RJ) Djair Brindeiro Filho (PE) Domingo M. Braile (SP) Edmar Atik (SP) Emilio Hideyuki Moriguchi (RS) Enio Buffolo (SP) Eulógio E. Martinez Filho (SP) Evandro Tinoco Mesquita (RJ) Expedito E. Ribeiro da Silva (SP) Fábio Vilas-Boas (BA) Fernando Bacal (SP) Flávio D. Fuchs (RS) Francisco Antonio Helfenstein Fonseca (SP) Gilson Soares Feitosa (BA) Glaucia Maria M. de Oliveira (RJ) Hans Fernando R. Dohmann (RJ) Humberto Villacorta Junior (RJ) Ínes Lessa (BA) Iran Castro (RS) Jarbas Jakson Dinkhuysen (SP) João Pimenta (SP) Jorge Ilha Guimarães (RS) José Antonio Franchini Ramires (SP) José Augusto Soares Barreto Filho (SE) José Carlos Nicolau (SP) José Lázaro de Andrade (SP) José Péricles Esteves (BA) Leonardo A. M. Zornoff (SP) Leopoldo Soares Piegas (SP) Lucia Campos Pellanda (RS) Luís Eduardo Rohde (RS) Luís Cláudio Lemos Correia (BA) Luiz A. Machado César (SP) Luiz Alberto Piva e Mattos (SP) Marcia Melo Barbosa (MG) Maria da Consolação Moreira (MG) Mario S. S. de Azeredo Coutinho (SC) Maurício I. Scanavacca (SP) Max Grinberg (SP) Michel Batlouni (SP) Murilo Foppa (RS) Nadine O. Clausell (RS) Orlando Campos Filho (SP) Otávio Rizzi Coelho (SP) Otoni Moreira Gomes (MG) Paulo Andrade Lotufo (SP) Paulo Cesar B. V. Jardim (GO) Paulo J. F. Tucci (SP) Paulo R. A. Caramori (RS) Paulo Roberto B. Évora (SP) Paulo Roberto S. Brofman (PR) Pedro A. Lemos (SP) Protásio Lemos da Luz (SP) Reinaldo B. Bestetti (SP) Renato A. K. Kalil (RS) Ricardo Stein (RS) Salvador Rassi (GO) Sandra da Silva Mattos (PE) Sandra Fuchs (RS) Sergio Timerman (SP) Silvio Henrique Barberato (PR) Tales de Carvalho (SC) Vera D. Aiello (SP) Walter José Gomes (SP) Weimar K. S. B. de Souza (GO) William Azem Chalela (SP) Wilson Mathias Junior (SP) Exterior Adelino F. Leite-Moreira (Portugal) Alan Maisel (USA) Aldo P. Maggioni (Italy) Cândida Fonseca (Portugal) Fausto Pinto (Portugal) Hugo Grancelli (Argentina) James de Lemos (USA) João A. Lima (USA) John G. F. Cleland (England) Maria Pilar Tornos (Spain) Pedro Brugada (Belgium) Peter A. McCullough (USA) Peter Libby (USA) Piero Anversa (Italy) Sociedade Brasileira de Cardiologia President Angelo Amato V. de Paola Special Advisor to the Presidency Fábio Sândoli de Brito SBC/MG - Odilon Gariglio Alvarenga de Freitas Vice-President Sergio Tavares Montenegro Adjunct Coordination SBC/MS - Mércule Pedro Paulista Cavalcante SBC Newsletter Editor Nabil Ghorayeb e Fernando Antonio Lucchese SBC/MT - Julio César De Oliveira Continuing Education Coordination Estêvão Lanna Figueiredo SBC/NNE - Jose Itamar Abreu Costa President-Elect Marcus Vinícius Bolívar Malachias Financial Director Jacob Atié Scientific Director Maria da Consolação Vieira Moreira Administrative Director Emilio Cesar Zilli Assistance Quality Director Pedro Ferreira de Albuquerque Communication Director Maurício Batista Nunes Norms and Guidelines Coordination Luiz Carlos Bodanese Governmental Integration Coordination Edna Maria Marques de Oliveira Regional Integration Coordination José Luis Aziz Presidents of State and Regional Brazilian Societies of Cardiology SBC/AL - Carlos Alberto Ramos Macias Information Technology Director José Carlos Moura Jorge SBC/AM - Simão Gonçalves Maduro Government Liaison Director Luiz César Nazário Scala SBC/BA - Mario de Seixas Rocha Director of State and Regional Affairs Abrahão Afiune Neto SBC/CE - Ana Lucia de Sá Leitão Ramos Cardiovascular Health Promotion Director - SBC/Funcor Carlos Costa Magalhães Department Director Especializados - Jorge Eduardo Assef Research Director Fernanda Marciano Consolim Colombo Chief Editor of the Brazilian Archives of Cardiology Luiz Felipe P. Moreira SBC/CO - Frederico Somaio Neto SBC/PA - Luiz Alberto Rolla Maneschy SBC/PB - Helman Campos Martins SBC/PE - Catarina Vasconcelos Cavalcanti SBC/PI - João Francisco de Sousa SBC/PR - Osni Moreira Filho SBC/RJ - Olga Ferreira de Souza SBC/RN - Rui Alberto de Faria Filho SBC/RS - Carisi Anne Polanczyk SBC/DF - Wagner Pires de Oliveira Junior SBC/SC - Marcos Venício Garcia Joaquim SBC/ES - Marcio Augusto Silva SBC/SE - Fabio Serra Silveira SBC/GO - Thiago de Souza Veiga Jardim SBC/SP - Francisco Antonio Helfenstein Fonseca SBC/MA - Nilton Santana de Oliveira SBC/TO - Hueverson Junqueira Neves Presidents of the Specialized Departaments and Study Groups SBC/DA - José Rocha Faria Neto SBCCV - Marcelo Matos Cascado GECC - Mauricio Wanjgarten SBC/DECAGE - Josmar de Castro Alves SBHCI - Helio Roque Figueira GEPREC - Glaucia Maria Moraes de Oliveira SBC/DCC - José Carlos Nicolau SBC/DEIC - Dirceu Rodrigues Almeida SBC/DCM - Maria Alayde Mendonça da Silva Grupo de Estudos de Cardiologia Hospitalar Evandro Tinoco Mesquita GERTC - Clerio Francisco de Azevedo Filho SBC/DCC/CP - Isabel Cristina Britto Guimarães SBC/DIC - Arnaldo Rabischoffsky SBC/DERC - Nabil Ghorayeb GAPO - Danielle Menosi Gualandro GEECG - Joel Alves Pinho Filho Grupo de Estudos de Cardio-Oncologia Roberto Kalil Filho GEEC - Cláudio José Fuganti GECIP - Gisela Martina Bohns Meyer SBC/DFCVR - Ricardo Adala Benfati GEECABE - Mario Sergio S. de Azeredo Coutinho SBC/DHA - Luiz Aparecido Bortolotto GECETI - Gilson Soares Feitosa Filho GECN - Ronaldo de Souza Leão Lima SOBRAC - Luiz Pereira de Magalhães GEMCA - Alvaro Avezum Junior GERCPM - Artur Haddad Herdy GECESP - Ricardo Stein Arquivos Brasileiros de Cardiologia Volume 105, Nº 2, August 2015 Indexing: ISI (Thomson Scientific), Cumulated Index Medicus (NLM), SCOPUS, MEDLINE, EMBASE, LILACS, SciELO, PubMed Address: Av. Marechal Câmara, 160 - 3º andar - Sala 330 20020-907 • Centro • Rio de Janeiro, RJ • Brasil Phone.: (21) 3478-2700 E-mail: [email protected] www.arquivosonline.com.br SciELO: www.scielo.br Commercial Department Phone: (11) 3411-5500 Graphic Design and Diagramming SBC - Internal Design Department E-mail: [email protected] Print IMOS Editora e Gráfica Editorial Production Circulation 1.500 copies SBC - Internal Publication Department Affiliated at the Brazilian Medical Association The ads showed in this issue are of the sole responsibility of advertisers, as well as the concepts expressed in signed articles are of the sole responsibility of their authors and do not necessarily reflect the views of SBC. This material is for exclusive distribution to the medical profession. The Brazilian Archives of Cardiology are not responsible for unauthorized access to its contents and that is not in agreement with the determination in compliance with the Collegiate Board Resolution (DRC) N. 96/08 of the National Sanitary Surveillance Agency (ANVISA), which updates the technical regulation on Drug Publicity, Advertising, Promotion and Information. According to Article 27 of the insignia, "the advertisement or publicity of prescription drugs should be restricted solely and exclusively to health professionals qualified to prescribe or dispense such products (...)". To ensure universal access, the scientific content of the journal is still available for full and free access to all interested parties at: www.arquivosonline.com.br. SUPPORT Back to the Cover Editorial Editorial Considerations on the New Clinical and Surgical Perspectives of Brazilian Cardiology Paulo Roberto B. Evora and Alfredo J. Rodrigues Departamento de Cirurgia e Anatomia da Faculdade de Medicina de Ribeirão Preto, Ribeirão Preto, SP – Brazil The Arquivos Brasileiros de Cardiologia (ABC) has been the official publication of the Brazilian Society of Cardiology for more than 60 years, and has proved to be one of the most prestigious scientific journals in Latin America, approaching all aspects of cardiology, including the surgical ones. In August 1986, the Revista Brasileira de Cirurgia Cardiovascular (RBCCV), specifically directed to the surgical aspects of heart diseases, began to be published. Thus, the editorial policy of the ABC has progressively privileged publications focused on the clinical treatment of cardiovascular diseases over surgical publications of common interest to cardiologists and cardiac surgeons1. Despite the substantial changes in the treatment of heart diseases, deriving from the appearance of new drugs and percutaneous devices, cardiac surgeries are still the treatment of choice to a substantial number of heart diseases, mainly the congenital, valvular and even coronary ones, whose onus of surgery indication is invariably on cardiologists. Thus, those specialists should be aware of several aspects of cardiac surgery, mainly those concerning their risks and results, so that they can base their indications on evidence. The great majority of cardiologists might know that the use of bilateral internal thoracic arteries (BITA) for coronary artery bypass grafting improves survival as compared to the use of only one single internal thoracic artery (ITA)2. Thus, the optimization of arterial grafts has been widespread with the use of the radial artery (RA) and composite grafts. However, only few professionals are aware of the controversies involving risky situations, possible limitations to the use of BITA3, the patency index of RA grafts and their influencing factors. The RA was the second arterial graft introduced in the clinical practice for coronary artery bypass grafting, and has drawn the interest of Brazilian surgeons since the 1990s4. Skeletonization of the left ITA (LITA) can favorably change the flow capacity of the graft, leading to the assumption that the behavior of the RA, as a coronary graft, is similar to that of the skeletonized LITA. Considering the potential role of the RA as a second option of coronary grafting and the concept of complete coronary artery bypass grafting with the exclusive use of arterial grafts, Keywords Cardiology/trends; Case-Control Studies; Cardiovascular Surgical Procedures/trends; Evidence Based Practice/trends. Mailing Address: Paulo Roberto B. Evora • Faculdade de Medicina de Ribeirão Preto – USP. Rua Rui Barbosa 367/15, Centro. Postal Code 14015-120, Ribeirão Preto, SP – Brazil E-mail: [email protected]; [email protected] Manuscript received July 06, 2015; revised manuscript July 08, 2015; accepted July 08, 2015. DOI: 10.5935/abc.20150094 103 Bonini et al5 have carried out a prospective randomized study comparing 40 patients distributed into two groups. In group I, skeletonized RA was used in 20 patients, and, in group II, RA with adjacent tissues was used in 20 patients. After the surgical procedure, flow velocity was measured. The results showed that the morphological and pathological characteristics, as well as the hemodynamic performance of the free RA grafts, regardless of being skeletonized or having adjacent tissues, were similar. However, a larger number of non-obstructive lesions was observed in the group with the RA graft preserving the adjacent tissues5. In addition, small is the number of cardiologists aware of the models to calculate the perioperative risk for morbidity and mortality available and popular among cardiac surgeons6, as well as of their limitations, mainly regarding the most recent options of percutaneous therapies6,7. The applicability of risk scores to cardiac surgery is another relevant international matter, but not well defined in centers outside North America and Europe. Garoffalo et al8 have assessed the ability of the Parsonnet-Bernstein 2000 score and EuroSCORE to predict the in-hospital mortality of patients undergoing cardiac surgery at a reference hospital in Brazil, and have identified risk predictors. The use of those scores has underestimated in-hospital mortality, suggesting inadequate preoperative assessment of the patients undergoing cardiac surgery. That study has stressed the need to develop local scores based on the reality of the populations to better assess the risk of cardiac surgery3. Considering the controversies about the ideal method of coronary artery bypass grafting for patients on dialysis, Herzog et al9, in the United States, have compared long-term survival of patients on dialysis after angioplasty, coronary stenting and coronary artery bypass grafting. That retrospective study has reported better long-term survival of patients on dialysis after coronary artery bypass grafting than after percutaneous coronary intervention and coronary stenting, emphasizing the relatively poorer results of patients with diabetes. That study has supported the need to develop large clinical registries and prospective studies on coronary revascularization procedures for patients on dialysis9. Miranda et al10 have approached that important question, analyzing retrospectively 50 consecutive and non-selected patients on dialysis, undergoing coronary artery bypass grafting at a tertiary university-affiliated hospital between 2007 and 2012. Those authors have shown that coronary artery bypass grafting is feasible in patients on dialysis, although followed by high morbidity and in-hospital mortality. In addition, they have emphasized the frequent exclusion of that group of patients from large cardiac studies. That detail might even contribute to the difficulty in selecting a better approach and to the still modest surgical results as compared to those of patients with preserved kidney function10. Evora & Rodrigues Brazilian clinical and surgical perspectives Editorial It is therefore evident that, although the ABC prioritizes articles on clinical therapies and their guidelines, the restriction upon articles with a surgical bias can deprive cardiologists from essential information to support their clinical decision-making, especially regarding the case- to-case analysis in daily practice. It is worth noting the publication in the ABC of several articles of common interest to both cardiac surgeons and cardiologists in recent years, therefore providing a relevant service to cardiology and cardiovascular surgery. References 1. Evora PR. Cardiac surgery, the Brazilian Archives of Cardiology and the Brazilian Journal of Cardiovascular Surgery. Rev Bras Cir Cardiovasc. 2012;27(4):VIII-XI. 2. Lytle BW, Blackstone EH, Sabik JF, Houghtaling P, Loop FD, Cosgrove DM. The effect of bilateral internal thoracic artery grafting on survival during 20 postoperative years. Ann Thorac Surg. 2004;78(6):2005-12; discussion 2012-4. 3. Gatti G, Dell’Angela L, Benussi B, Dreas L, Forti G, Gabrielli M, et al. Bilateral internal thoracic artery grafting in octogenarians: where are the benefits? Heart Vessels. 2015. [Epub ahead of print] 4. Dallan LA, Oliveira SA, Jatene FB, Corso R, Iglesias JCR, Prates N, et al. Radial artery for a wider arterial myocardial revascularization: microscopical anatomy and surgical technique. Rev Bras Cir Cardiovasc. 1996; 11(2): 75-81. 5. Bonini RC, Staico R, Issa M, Arnoni AS, Chaccur P, Abdulmassih Neto C,et al. Effects of skeletonized versus pedicled radial artery on postoperative graft patency and flow. Arq Bras Cardiol. 2014;102(5):441-8. 6. Head SJI, Osnabrugge RL, Howell NJ, Freemantle N, Bridgewater B, Pagano D, et al. A systematic review of risk prediction in adult cardiac surgery: considerations for future model development. Eur J Cardiothorac Surg. 2013;43(5):e121-9 7. Thalji NM, Suri RM, Greason KL, Schaff HV. Risk assessment methods for cardiac surgery and intervention. Nat Rev Cardiol. 2014;11(12):704-14. 8. Garofallo SB, Machado DP, Rodrigues CG, Bordim O Jr, Kalil RA, Portal VL. Applicability of two international risk scores in cardiac surgery in a reference center in Brazil. Arq Bras Cardiol. 2014;102(6):539-48. 9. Herzog CA, Ma JZ, Collins AJ. Comparative survival of dialysis patients in the United States after coronary angioplasty, coronary artery stenting, and coronary artery bypass surgery and impact of diabetes. Circulation. 2002;106(17):2207-11. 10. Miranda M, Hossne NA Jr, Rodrigues Branco JN, Vargas GF, Almeida Palma da Fonseca JH, Medina de Abreu Pestana JO, et al. Myocardial revascularization in dyalitic patients: in-hospital period evaluation. Arq Bras Cardiol. 2014;102(2):128-33. Arq Bras Cardiol. 2015; 105(2):103-104 104 Back to the Cover Special Article Executive Summary – Guideline on Telecardiology in the Care of Patients with Acute Coronary Syndrome and Other Cardiac Diseases Mucio Tavares de Oliveira Jr.1, Leonardo Jorge Cordeiro de Paula1, Milena Soriano Marcolino2, Manoel Fernandes Canesin3 Instituto do Coração, HCFMUSP1, São Paulo, SP; Universidade Federal de Minas Gerais2, Belo Horizonte, MG; Universidade Estadual de Londrina3, Londrina, PR – Brazil Cardiology is a very promising field in telemedicine. The transmission of electrocardiograms (ECG) from remote health services or ambulances to a central for analysis is already routine in the approach to acute coronary syndromes (ACS). This approach allows the obtention of expert guidance and referral to appropriate health units, with the potential of saving lives. This impact may be seen in acute myocardial infarction (MI), in which telemedicine has reduced intra-hospital mortality rates from 12.3% to 7.1%1-4. Basic concepts In a health system geographically distributed like the Brazilian system, in which Basic Health Units (Unidades Básicas de Saúde, UBSs), Emergency Care Units (Unidades de Pronto Atendimento, UPAs), secondary hospitals, and ambulances are scattered throughout the country (often in remote locations), and specialized centers are located in advanced care units in large cities (such as tertiary hospitals), telemedicine offers the opportunity to improve the treatment of emergencies. The clinical ability of specialists in tertiary hospitals may be used to improve the care in Remote Care Units (Unidades Remotas de Atendimento, URAs), offering support for early diagnosis and therapy guidance for non‑specialist medical practitioners providing medical care to patients in URAs5,6. Communication channels in telemedicine include telephone lines for voice communication and connection to the internet, and for transmission of test results, ECG tracings, and images. Optionally, a video link may be used for visualization of the patient. Telemedicine in the approach to ACS7,8 Situation A: A patient goes by himself to the nearest URA, or calls the prehospital care service and is taken to the URA in a standard ambulance without an electrocardiograph. Keywords Heart Failure / mortality; Myocardial Infarction / mortality; Telemedicine / utilization; Electrocardiography; Mobile Health Units. Mailing Address: Mucio Tavares de Oliveira Jr. • Av. Dr. Eneas de Carvalho Aguiar, 44 - Unidade de Emergência. Postal Code 05403-900, São Paulo, SP – Brazil E-mail [email protected] Manuscript received July 10, 2015; revised manuscript July 10, 2015; accepted July 10, 2015. DOI: 10.5935/abc.20150104 105 Arq Bras Cardiol. 2015; [online].ahead print, PP.0-0 The professionals at the URA take the clinical history, examine, and obtain serial ECGs from the patient. The ECG tracings are transmitted along with the clinical history to the telecardiology hub where they are interpreted by cardiologists who quickly prepare and send a report, and guide the professionals at the URA on the appropriate therapy. Situation B: A patient connects with the prehospital care service and an ambulance with an electrocardiograph and without a physician answers the call. Based on the patient's history and interpretation of the ECG, if the cardiologist at the telecardiology hub diagnoses the patient as having an ST‑segment elevation MI (STEMI), he guides the medical team to administer the standard therapy (for example, aspirin and other medications) and transport the patient to a hospital that offers percutaneous coronary intervention (PCI) or to administer fibrinolytic treatment. Even if the diagnosis of STEMI is excluded, the ambulance team is oriented to follow the cardiologist’s instructions about the path to be followed for that patient. Situation C: A patient calls the prehospital care service, an ambulance with a physician and an electrocardiograph answers the call, and the team obtains an ECG that is transmitted to the telecardiology hub. Based on the clinical history and interpretation of the ECG, if the cardiologist at the telecardiology hub determines that the patient has STEMI, he guides the physician to administer treatment for STEMI, such as antiplatelet and anticoagulant agents, and to follow one of these options: • If the STEMI patient can be transported to a hospital with PCI capability and the PCI can be performed within 120 minutes, or if the patient has contraindication to fibrinolytic treatment, the patient must be transported to the hospital with PCI. The ambulance physician also alerts the hospital to prepare the catheterization laboratory to treat a STEMI patient with primary PCI. • If the PCI cannot be performed within 120 minutes, the ambulance physician is instructed to first administer fibrinolytic agents, preferably within 30 minutes, and then transport the patient to the nearest hospital equipped with a catheterization laboratory to continue the therapy. • If the cardiologist in the telecardiology hub confirms that STEMI is not the diagnosis and the ambulance physician determines that the patient has ACS, after receiving the initial therapy the patient should be transferred preferably to a hospital equipped with a catheterization laboratory. If that is not possible, the patient should be transferred to the nearest hospital equipped with an intensive cardiac care unit. If the cardiologist determines Oliveira Jr. et al Guideline on Telecardiology in ACS and Other Cardiopathies Special Article that the chest pain protocol should be initiated for the patient, he or she may direct the ambulance team to transport the patient to the nearest hospital, even if the hospital is not equipped with a catheterization laboratory, for monitoring of clinical parameters, ECG, and markers of myocardial necrosis (Figure 1). • Third "D": if the ECG does not show signs of ischemia, assess the probability of the patient having coronary artery disease (CAD) based on the presence of risk factors: age (above 45 years in men and 55 years in women), smoking, diabetes, hypertension, and family history of early CAD (below the age of 55 years in men and 65 years in women). To ensure that the transmitted information has good quality and the interaction is valuable, the patient with chest pain should receive a systematic approach, which can be achieved with several methodologies. One of these methodologies takes into account the "4D" for systematization of the diagnosis of ACS (Figure 2)9: • Fourth "D": the diagnosis of ACS must be confirmed or excluded, or the chest pain protocol should be initiated. Requirements in telemedicine for adequate diagnosis and treatment of ACS and other acute cardiac diseases (Figure 3)10. • First "D": classify the chest pain (discomfort) into types A (definitely anginal), B (probably anginal), C (probably not anginal), or D (definitely not anginal). Financial requirements, procedures, and clinical and team protocols for deployment of telemedicine for adequate diagnosis and treatment of ACS and other acute cardiac diseases (Figure 4)10. • Second "D": define whether an ST-segment elevation is present or not in the ECG. Medical equipment, information technology, and services (Figures 5 and 6)10. Figure 1 – Schematic representation of telemedicine for acute emergency therapy. Treatment strategies using telemedicine are shown for acute coronary syndrome (ACS). ECG: surface electrocardiogram. Arq Bras Cardiol. 2015; 105(2):105-111 106 Oliveira Jr. et al Guideline on Telecardiology in ACS and Other Cardiopathies Special Article Chest pain (Discomfort): screen the patient and classify the pain into types A, B, C, or D Define the ECG: presence of ST-segment elevation or signs of ischemia CAD: low, intermediate, or high probability Diagnosis: confirm/exclude ACS or initiate the chest pain protocol Figure 2 – Care systematization for the establishment of the diagnosis in patients with chest pain. ECG: electrocardiogram; CAD: coronary artery disease; ACS: acute coronary syndrome. Investigation of the patient, including the type of pain and the likelihood of coronary artery disease, and acquisition of an electrocardiogram for detection of ST-segment elevation myocardial infarction and coronary syndrome without ST-segment elevation in patients with suspected acute coronary syndrome treated in mobile and fixed emergency units before the teleconsultation. Distant specialized support for electrocardiogram interpretation for detection of ST-segment elevation myocardial infarction and coronary syndrome without ST-segment elevation in patients treated in mobile and fixed emergency units. Distant specialized support for guidance on the management of patients with suspected acute coronary syndrome treated in mobile and fixed emergency units. Acquisition of a prehospital electrocardiogram to refine the management and reduce the time to reperfusion in patients presenting with ST-segment elevation myocardial infarction. Acquisition of a prehospital electrocardiogram for the diagnosis of STsegment elevation myocardial infarction and acute coronary syndrome without ST-segment elevation to reduce mortality in these patients. Recommendation Grade Level of Evidence I A Recommendation Grade Level of Evidence I B Recommendation Grade Level of Evidence IIa A Recommendation Grade Level of Evidence I B Recommendation Grade Level of Evidence I B Figure 3 – Recommendation grades and levels of evidence of the procedures for management of patients with ACS. Telecardiology in remote routine diagnosis One of the most common applications of telecardiology in remote areas is in the analysis of diagnostic tests, such as ECG, Holter, ambulatory monitoring of blood pressure (AMBP), and echocardiography. Other applications include synchronous or asynchronous teleconsulting systems or second opinions, teleauscultation, remote monitoring of blood pressure, vital signs and implantable electronic devices, and educational activities. In addition, telecardiology 107 Arq Bras Cardiol. 2015; 105(2):105-111 has important applications in the penitentiary system, in pediatrics, and in fetal cardiology. Cardiac arrhythmias and syncope11-13 Since several types of cardiac arrhythmia occur in short and unexpected episodes, its diagnosis depends on an ECG recorded during the paroxysmal episode. A standard 10-second surface ECG may not be able to detect the abnormality in the heart rhythm. In this case, long-term Oliveira Jr. et al Guideline on Telecardiology in ACS and Other Cardiopathies Special Article Adequate support from financial resources to establish the infrastructure of the telecardiology hub and assembly of the organizational structure for operation of the telecardiology service. In the telecardiology hub and in the Remote Care Unit, the clinical protocols for diagnosis and treatment must be written in easy language and have simple application. The processes and work pace for each step must be documented and communicated to the team. The team of cardiologists at the telecardiology hub for emergency consultations, such as interpretation of electrocardiograms, conference calls, web conferences, videoconferences, or telephone calls, must be adequate to the number of calls and the number of units connected to the hub. Technical support and management professionals must be part of the team, and everyone should be trained, including users of the system at the mobile and fixed Remote Care Units. Recommendation Grade Level of Evidence I C Recommendation Grade Level of Evidence I C Recommendation Grade Level of Evidence I C Recommendation Grade Level of Evidence I C Figure 4 – Recommendation grades and levels of evidence for the financial requirements, procedures, and clinical and team protocols in telemedicine for adequate diagnosis and treatment of ACS and other acute cardiac diseases. monitoring is recommended, such as 24-hour Holter monitoring or event recording for 2 to 4 weeks. For selected, more difficult cases, an implantable monitoring device named loop recorder may be used to record the ECG patterns during occasional but significant symptoms like syncope. patient and offer specialized treatment to HF patients, has been shown to reduce the mortality and hospitalizations due to HF, improve quality of life, reduce the cost of treatment of prescriptions based on evidence, and improve the patients’ knowledge and their knowledge about self-treatment. The system may be useful in several situations, among others: • Detection of asymptomatic episodes of atrial fibrillation, which may require anticoagulation therapy to reduce the risk of stroke. • Quick recognition of electrode lead failure, allowing fast intervention and avoiding inappropriate shocks. • Reduction in the number of outpatient visits during long-term follow-up of patients with a pacemaker or implanted defibrillator. Heart failure (HF)14,15 Distant monitoring, or telemonitoring, is a promising strategy to improve the outcomes of HF treatment, allowing remote monitoring of patients so physicians can intervene early when evidence of clinical deterioration is present. The approaches vary from computerized systems for decision support to programs managed by nurses or physicians. A dedicated hardware or a smartphone may be used to transmit the patient's data (for example, symptoms, weight, blood pressure, and heart rate). A structured phone support, which can better guide the Author contributions Conception and design of the research, Acquisition of data, Writing of the manuscript and Critical revision of the manuscript for intellectual content: Oliveira Jr. MT, Paula LJC, Marcolino MS, Canesin MF; Analysis and interpretation of the data and Obtaining financing: Oliveira Jr. MT. Potential Conflict of Interest No potential conflict of interest relevant to this article was reported. Sources of Funding This study was partially funded by Philips Healthcare. Study Association This study is not associated with any thesis or dissertation work. Arq Bras Cardiol. 2015; 105(2):105-111 108 Oliveira Jr. et al Guideline on Telecardiology in ACS and Other Cardiopathies Special Article In the Remote Care Unit, all patients with chest pain must have a 12‑lead electrocardiogram performed, which should be interpreted in less than 10 minutes from the first medical contact (FMC). Availability of a 12-lead electrocardiograph with a capability to transmit the tracing to the telecardiology hub, preferably with an option to print the tracing. Use of photographic reproduction or low-quality scanning to transmit the electrocardiogram to the telecardiology hub for preparation of the report. Use of software for electrocardiogram interpretation validated for emergency situations. In remote locations in which the results of the markers are not available within 60 minutes, the local availability of point-of-care equipment should be evaluated. Wait for the results of myocardial necrosis markers to start therapy in patients with a diagnosis of ST-segment elevation myocardial infarction. Availability of cardiac markers assessment by a point-of-care methodology in remote fixed areas where a central laboratory is not available. Recommendation Grade Level of Evidence I A Recommendation Grade Level of Evidence I C Recommendation Grade Level of Evidence III C Recommendation Grade Level of Evidence IIb C Recommendation Grade Level of Evidence I A Recommendation Grade Level of Evidence III A Recommendation Grade Level of Evidence IIa B Figure 5 – Recommendation grades and levels of evidence for the medical equipment in telemedicine for adequate diagnosis and treatment of ACS and other acute cardiac diseases. 109 Arq Bras Cardiol. 2015; 105(2):105-111 Oliveira Jr. et al Guideline on Telecardiology in ACS and Other Cardiopathies Special Article Internet availability for wired or wireless transmission of patients’ data, electrocardiogram, and other tests. Presence of equipment for patient monitoring in the Remote Care Unit and in the mobile unit for all patients with suspected acute coronary syndrome. Presence of telephone equipment for routine transmissions or to allow communication during network downtime, or failure in the equipment or transmission system. Presence of internet connection with adequate bandwidth in the Remote Care Unit and in the telecardiology hub adapted for transmission of electrocardiograms and other additional resources, such as data and image. Presence of wired or wireless hardware for work and communication, suitable for the demand of both the telecardiology hub and Remote Care Unit. In services that choose to transmit videos, or still or dynamic images, the wired or wireless hardware for work and communication should be suitable for this purpose. Presence of a protection system, security of local data and data to be transmitted, as well as an up-to-date anti-virus program in the telecardiology hub and Remote Care Unit. Recording of all the communication involving orientation or exchange of information between the telecardiology hub and the Remote Care Unit. Presence in the Remote Care Unit of electrocardiogram equipment compatible with the system used in the telecardiology hub and technical stock in sufficient amount to replace and maintain the system operative. Recommendation Grade Level of Evidence I C Recommendation Grade Level of Evidence I A Recommendation Grade Level of Evidence I C Recommendation Grade Level of Evidence I C Recommendation Grade Level of Evidence I B Recommendation Grade Level of Evidence I A Recommendation Grade Level of Evidence I C Recommendation Grade Level of Evidence I C Recommendation Grade Level of Evidence I C Figure 6 – Recommendation grades and levels of evidence for the information technology equipment and services in telemedicine for adequate diagnosis and treatment of ACS and other acute cardiac diseases. Arq Bras Cardiol. 2015; 105(2):105-111 110 Oliveira Jr. et al Guideline on Telecardiology in ACS and Other Cardiopathies Special Article References 1. Moraes E, Barros LP, Rodrigues AE, Pagliara AT, Carvalho AC. Pre hospital electrocardiography: prevalence of clinically important ECG findings of a public health system in a developing country. In: 2nd International Conference on Global Tele Health. 26 to 28 November, 2012. Australian Tele Health Society. Sydney; 2012. 2. Diercks DB, Kontos MC, Chen AY, Pollack CV Jr, Wiviott SD, Rumsfeld JS, et al. Utilization and impact of pre-hospital electrocardiograms for patients with acute ST-segment elevation myocardial infarction: data from the NCDR (National Cardiovascular Data Registry) ACTION (Acute Coronary Treatment and Intervention Outcomes Network) Registry. J Am Coll Cardiol. 2009;53(2):161-6. 3. Terkelsen CJ, Lassen JF, Norgaard BL, Gerdes JC, Poulsen SH, Bendix K, et al. Reduction of treatment delay in patients with ST-elevation myocardial infarction: impact of pre-hospital diagnosis and direct referral to primary percutanous coronary intervention. Eur Heart J. 2005;26(8):770-7. Sociedade Brasileira de Cardiologia. [IV Guidelines of Sociedade Brasileira de Cardiologia for treatment of acute myocardial infarction with ST- segment elevation]. Arq Bras Cardiol. 2009;93(6 Suppl 2): e179-264. 9. Oliveira Jr MT, Canesin MF, Nazima WI, Gualandro DM, Barretto AC, Soeiro AM, et al. Suporte avançado de vida em insuficiência coronariana – SAVICO. Barueri (SP): Manole; 2014. 10. Brunetti ND, De Gennaro L, Dellegrottaglie G, Amoruso D, Antonelli G, Di Biase M. A regional prehospital electrocardiogram network with a single telecardiology “hub” for public emergency medical service: technical requirements, logistics, manpower, and preliminary results. Telemed J E Health. 2011;17(9):727-33. 11. Scalvini S, Piepoli M, Zanelli E, Volterrani M, Giordano A, Glisenti F. Incidence of atrial fibrillation in an Italian population followed by their GPs through a telecardiology service. Int J Cardiol. 2005;98(2):215-20. 4. Marcolino MS, Brant LC, Araujo JG, Nascimento BR, Castro LR, Martins P, et al. Implementation of the myocardial infarction system of care in city of Belo Horizonte, Brazil. Arq Bras Cardiol.2013;100(4):307-14. Erratum in: Arq Bras Cardiol. 2013;100(4):313. 12. Kirtava Z, Gegenava T, Gegenava M, Matoshvili Z, Kasradze S, Kasradze P. Mobile telemonitoring for arrhythmias in outpatients in the Republic of Georgia: a brief report of a pilot study. Telemed J E Health. 2012;18(7):570-1. 5. 13 Brunetti ND, De Gennaro L, Pellegrino PL, Dellegrottaglie G, Antonelli G, Di Biase M. Atrial fibrillation with symptoms other than palpitations: incremental diagnostic sensitivity with at-home tele-cardiology assessment for emergency medical service. Eur J Prev Cardiol. 2012;19(3):306-13. Paim J, Travassos C, Almeida C, Bahia L, Macinko J. The Brazilian health system: history, advances, and challenges. Lancet. 2011;377(9779):1778-97. 6. Andrade MV, Maia AC, Cardoso CS, Alkmim MB, Ribeiro AL. Cost-benefit of the telecardiology service in the state of Minas Gerais: Minas Telecardio Project. Arq Bras Cardiol. 2011;97(4):307-16. 7. Alkmim MB, Figueira RM, Marcolino MS, Cardoso CS, Pena de Abreu M, Cunha LR, et al. Improving patient access to specialized health care: the Tele health Network of Minas Gerais, Brazil. Bull World Health Organ. 2012;90(5):373-8. 111 8. Arq Bras Cardiol. 2015; 105(2):105-111 14. Morguet AJ, Kuhnelt P, Kallel A, Rauch U, Schultheiss HP. Utilization of telemedicine by heart disease patients following hospitalization. J Telemed Telecare. 2008;14(4):178-81. 15. Anker SD, Koehler F, Abraham WT. Telemedicine and remote management of patients with heart failure. Lancet. 2011;378(9792):731-9. Back to the Cover Original Article Myocardial Scintigraphy in the Evaluation of Cardiac Events in Patients without Typical Symptoms Paola Emanuela Poggio Smanio, Juliana Horie Silva, João Vitor Holtz, Leandro Ueda, Marilia Abreu, Carlindo Marques, Leonardo Machado Instituto Dante Pazzanese de Cardiologia, São Paulo, SP – Brazil Abstract Background: Cardiovascular disease is a leading cause of death in the world and in Brazil. Myocardial scintigraphy is an important noninvasive method for detecting ischemia in symptomatic patients, but its use in asymptomatic ones or those with atypical symptoms is yet to be defined. Objective: To verify the presence of major cardiac events in asymptomatic patients or those with atypical symptoms (atypical chest pain or dyspnea) that underwent myocardial scintigraphy (MS), over a period of 8 years. Secondary objectives were to identify cardiac risk factors associated with myocardial scintigraphy abnormalities and possible predictors for major cardiac events in this group. Methods: This was a retrospective, observational study using the medical records of 892 patients that underwent myocardial scintigraphy between 2005 and 2011 and who were followed until 2013 for assessment of major cardiac events and risk factors associated with myocardial scintigraphy abnormalities. Statistical analysis was performed by Fisher’s exact test, logistic regression and Kaplan-Meyer survival curves, with statistical significance being set at p ≤ 0.05. Results: Of the total sample, 52.1% were men, 86.9% were hypertensive, 72.4% had hyperlipidemia, 33.6% were diabetic, and 12.2% were smokers; 44.5% had known coronary artery disease; and 70% had high Framingham score, 21.8% had moderate and 8% had low risk. Of the myocardial scintigraphies, 58.6% were normal, 26.1% suggestive of fibrosis and 15.3% suggestive of ischemia. At evolution, 13 patients (1.5%) had non-fatal myocardial infarction and six individuals (0.7%) died. The group with normal myocardial scintigraphy showed longer period of time free of major cardiac events, non-fatal myocardial infarction (p = 0.036) and death. Fibrosis in the myocardial scintigraphy determined a 2.4-fold increased risk of non-fatal myocardial infarction and five-fold higher risk of death (odds ratio: 2.4 and 5.7, respectively; p = 0.043). Conclusion: The occurrence of major cardiac events in 8 years was small. Patients with fibrosis at MS had more major events, whereas patients with normal MS result had fewer major cardiac events, with higher survival. (Arq Bras Cardiol. 2015; [online].ahead print, PP.0-0) Keywords: Myocardial Scintigraphy; Ischemia; Atypical Symptoms; Hard events. Introduction Cardiovascular diseases are the leading cause of death worldwide, with ischemic heart disease and cerebrovascular accident (CVA) being the most frequent1. The incidence of coronary artery disease (CAD) is increasing worldwide, being the second leading cause of death in Brazil, with a mean of 80,000 deaths per year. Its prevalence in the adult population is estimated at 5-8%2. According to the Department Informatics of the Brazilian Unified Health System (DATASUS), in 2010, ischemic heart disease accounted for 210,046 hospital admissions in Brazil and 29% of deaths Mailing Address: Paola Emanuela Poggio Smanio • João Lourenço,763 Vila Nova Conceição. Postal Code 045080-31. São Paulo, SP – Brazil. E-mail: [email protected] Manuscript received February 18, 2014; revised manuscript December 08, 2014; accepted December 08, 2014. DOI: 10.5935/abc.20150074 112 (99,408 deaths or 55.11 deaths/100,000 inhabitants)3,4, corresponding to a burden of R$ $ 1.9 billion, or 19% of the total cost with hospitalizations5. Due to the epidemiological importance of CAD, appropriate risk stratification strategies are needed to establish better cost-effectiveness and safety of preventive treatments, as well as request for additional tests. The clinical manifestation of coronary heart disease is the result of the imbalance between myocardial oxygen supply and consumption. The subjective description of angina may make symptom interpretation difficult and, therefore, the clinical diagnosis. Thus, objective ischemia tests can confirm the diagnostic hypothesis and assess CAD severity6. Myocardial scintigraphy (MS) is a cornerstone in the evaluation of patients with suspected CAD due to its high diagnostic accuracy, as well as being able to define the extent, severity and location of myocardial perfusion abnormalities, greatly assisting in clinical management7. The technique uses electromagnetic gamma radiation to obtain images. Radioactive isotopes are injected into the Smanio et al. Myocardial perfusion without typical symptoms events Original Article patient and, due to affinity for the myocardium, they bring perfusion and/or metabolic information. After the radiotracer injection, it is possible to indirectly assess blood flow and myocardial flow reserve in a non-invasive manner8,9. patient had creatinine clearance < 90 mL/min; LVEF was determined by Doppler echocardiogram performed at most three months before the MS with no procedures between the methods. Currently, there is strong evidence for using MS in the diagnosis, follow-up, risk stratification and prognosis of symptomatic patients with known or suspected CAD. However, MS indication in asymptomatic patients or patients with atypical symptoms, even with known CAD, is yet to be defined, since in addition to the fact that benefits in this population are not fully established, the examination involves the inherent risks of physical or pharmacological stress, as well as exposure to ionizing radiation10,11. MS was performed using 99mTc-sestamibi as the radiotracer and according to the standard protocol of 1 or 2 days, with the stress test (exercise or pharmacological test) being the basal stage, being performed on the same day or on subsequent days. The objective of this study was to identify, in asymptomatic patients or patients with atypical symptoms submitted to MS, the occurrence of events such as death and acute myocardial infarction (AMI), occurring in up to 8 years. Secondary objectives were to define the time free of events such as death and AMI after normal MS in asymptomatic patients or patients with atypical symptoms; to identify risk factors associated with alterations in myocardial perfusion scintigraphy; to identify risk factors that are independent predictors of death and nonfatal AMI in this group of patients. Methods Retrospective, observational study carried out by the data analysis of medical records in a group of asymptomatic patients with cardiovascular symptoms or those considered to be atypical, with previously known CAD or not. All patients underwent MS at Instituto Dante Pazzanese de Cardiologia from December 2005 to June 2011. Patients were followed for the period from the date of the examination until July 2013, to verify the occurrence of nonfatal myocardial infarction or death. All patients were analyzed for the presence of systemic arterial hypertension (SAH), dyslipidemia, smoking status, occlusive peripheral arterial disease (OPAD) and / or carotid disease, diabetes mellitus, chronic renal failure (CRF), ischemic cerebrovascular accident (iCVA), previously known CAD, Left Ventricular Ejection Fraction (LVEF) < 50%, family history of coronary heart disease, type of stress used at the MS (exercise stress or pharmacological stress test with dipyridamole), and presence of alteration suggestive of ischemia in the exercise test performed prior to the MS. Patients were also classified as having high, intermediate and low cardiovascular risk, according to the Framingham score. A patient was considered hypertensive if he/she required the use of one or more antihypertensive drugs and through the criteria used in the VI Brazilian Guidelines on Hypertension of the Brazilian Society of Cardiology11; and was considered dyslipidemic according to the criteria of the IV Brazilian Guidelines on Dyslipidemia and Atherosclerosis Prevention of the Department of Atherosclerosis of the Brazilian Society of Cardiology 12. A patient was considered diabetic when he or she required the use of one or more oral hypoglycemic agents and/or insulin and no patients with metabolic syndrome were included. The presence of CRF was defined if the Inclusion criteria were patients submitted to MS that did not show any cardiac symptom from the date of the examination request by the requesting clinician to the date when the MS was performed; and those with symptoms considered atypical by the clinician that requested the examination, as they did not meet the classic characteristics described, such as angina (retrosternal pain, triggered by exertional or emotional stress, with relief at rest or nitrate) or that had symptoms suggestive of ischemic equivalent (dyspnea). Most of the patients had other cardiac symptoms that were poorly characterized and uncharacteristic for ischemic heart disease. Exclusion criteria were patients with chest pain suggestive of ischemic heart disease, dyspnea or symptoms suggestive of ischemic equivalent, or electrocardiogram suggestive of ischemia from the date of the MS request until its performance; and patients with incomplete data during the review of medical records. The MS were analyzed by two specialists in nuclear medicine and a third expert was called in to analyze the images, when there was disagreement. The images were analyzed qualitatively only by the presence or absence of low radiotracer uptake in the myocardium in the 17 analyzed segments. The equipment used for image acquisition was the Millennium VG gamma camera (GE Medical Systems, Milwaukee, United States), with two scintillation detectors, angled at 90°, with parallel hole collimators, high resolution and low energy. Information acquired was processed in a Xeleris workstation. MS was performed associated with physical exertion with exercise testing or pharmacological stimulation through dipyridamole infusion, according to clinical indication. Bruce and modified Bruce protocols were used at the exercise testing, with anti-ischemic medications being withdrawn according to standardized recommendations from the nuclear medicine department. The clinicians of the institution were aware of the drug withdrawal for the test and, when they did not wish the medication to be withdrawn they requested that the evaluation should be performed while on medication, in the medical request form. The following were considered as ischemic myocardial response criteria to the physical stress test, as standardized in the literature: the presence of ST‑segment depression ≥ 1.5 mm during or after exercise, when compared to baseline, with slow ascending morphologies (analyzed at point Y), horizontal (analyzed at point J) or descending (analyzed at point J), or the presence of clinical signs/symptoms suggestive of ischemia, according to the known classical and standardized criteria13. Arq Bras Cardiol. 2015; 105(2):112-122 113 Smanio et al. Myocardial perfusion without typical symptoms events Original Article For the pharmacological test, dipyridamole was infused at a dose of 0.56 mg /kg/ min during a total time of 4 minutes. A dose of 20 mCi or 740 MBq of 99mTc-MIBI was administered in the second minute after the dipyridamole infusion was finished, considered as the moment of maximum hyperemia. As interpretation criteria of electrocardiographic response to dipyridamole, used for the characterization of the ischemic response, the presence of horizontal depression, slowly ascending or descending ST segment ≥ 1.0 mm (or intensification of depression = 1.0 mm) was considered suggestive of ischemia, measured at the J point in the horizontal and descending morphologies, and at the Y point, in the slow ascending morphology. Typical chest pain and/or other clinical manifestations suggestive of coronary heart disease were also considered suggestive of ischemia, according to known classical and standardized criteria13. being set at p < 0.05. Moreover, logistic regression analysis of the clinical and epidemiological characteristics and risk factors was performed and the event-free survival Kaplan‑Meier curve was constructed. The present study only analyzed the presence or absence of alterations in the functional tests that were suggestive of ischemia and prognostic scores were not calculated. Of patients without known CAD (483 patients), 449 patients were completely asymptomatic since the consultation when MS was requested and 34 patients had symptoms considered atypical for CAD. Of the patients with known CAD (388 patients), 368 were totally asymptomatic since the consultation when MS was requested and 20 had atypical symptoms (p = 0.059). The images were processed using the dedicated software QGS, also known as Cedars-Sinai software, obtaining tomographic cuts in the vertical plane, according to the smallest cardiac axis, in the vertical plane, according to the greatest axis and in the horizontal plane, according to the greatest axis. The cuts of the two phases were paired to allow a cut-to-cut comparison of the radioactive concentration at stress and at baseline. Image processing synchronized with the ECG provided the reproduction of cardiac wall contractions, in addition to indices of systolic and diastolic volumes and LVEF; it was possible to visualize the heart dynamics in both views, as well as of a three-dimensional representation of the left ventricle. According to the department routine, the criteria for the analysis of myocardial perfusion images were visual and qualitative evaluations of the radiotracer concentration in the different myocardial segments (17 segments), comparing cut‑by-cut the images of the stress phase with the corresponding baseline ones. The following factors were considered in the qualitative analysis of myocardial perfusion: homogeneity or heterogeneity of the radiotracer concentration in myocardial segments; extension of radiotracer concentration defects in the myocardial segments; and intensity of the relative low uptake of the radiotracer in the myocardial segments. However, for this study, we took into account only the presence or absence of perfusion abnormalities. MS was considered normal if the radiotracer concentration was homogeneous in both phases (basal and stress); suggestive of ischemia, if the low uptake was reversible after stress; suggestive of fibrosis, if the low uptake was fixed after the stress phase in relation to baseline; and suggestive of ischemia and fibrosis, if there was fixed and reversible low uptake of the radiotracer in one or more myocardial segments at the baseline and stress phases. Statistical analysis was performed using the Statistical Package for Social Sciences (SPSS), and Pearson’s chi-square test and Fisher’s test were used, with statistical significance 114 Arq Bras Cardiol. 2015; 105(2):112-122 This study was submitted to the Research Ethics Committee, with Certificate Presentation for Ethics Appreciation (CAAE: 20702313500005462). Results A total of 892 patients were analyzed, characterized as asymptomatic or with atypical cardiac symptoms, who were submitted to MS from December 2005 to June 2011. Twenty-one patients were excluded due to inconclusive information in medical records or loss to follow-up during the study period, thus totaling 871 patients. After statistical analysis of the collected data, it was observed equivalence between the genders, with a prevalence of 454 (52.1%) male patients. The Framingham score was applied to all assessed patients, with 611 (70.1%) being classified as having high cardiovascular risk, 190 (21.8%) as intermediate risk and 70 (8%) as low risk. The prevalence of all analyzed variables with their respective percentages is shown in Table 1, depicting a large number of hypertensive (86.9%) and dyslipidemic (72.4%) patients. When evaluating the MS characteristics, it was observed that of the examinations performed, 385 (44.2%) were submitted to physical stress through exercise test and 486 (55.8%) Table 1 – Prevalence of cardiovascular risk factors Variables Yes n (%) Systemic arterial hypertension 757 (86.9) Dyslipidemia 631 (72.4) Smoking 106 (12.2) OPAD/ carotid disease Diabetes mellitus 58 (6.7) 293 (33.6) CRF 37 (4.2) iCVA 48 (5.5) Previous CAD 388 (44.5) LVEF < 50% 86 (9.9) Family history of CAD 101 (11.6) OPAD: Occlusive peripheral arterial disease; CRF: Chronic renal failure; iCVA: Ischemic cerebrovascular accident; CAD: Coronary artery disease; LVEF: Left ventricular ejection fraction. Smanio et al. Myocardial perfusion without typical symptoms events Original Article were performed with pharmacological stimulation, through dipyridamole administration. At the ischemia-inducing tests for the MS, of the 871 tests analyzed, 189 (21.7%) showed abnormalities suggestive of ischemia due to the presence of ECG alterations and / or symptoms suggestive of ischemia. The prevalence of normal MS, fixed low uptake suggestive of fibrosis and reversible low uptake suggestive of ischemia in the assessed patients was 511 individuals (58.6%), 227 (26.1%) and 133 (15.3%), respectively. Table 2 shows the prevalence of the results obtained by scintigraphy, including the ischemia-inducing test. Statistical analysis of the association between the clinical and epidemiological variables and the result of the MS was performed, which were described as normal, with fixed or reversible low uptake. The results are shown in Tables 3 to 5. Patients with CRF, ischemic CVA, previous known CAD and LVEF < 50% showed a greater association with MS suggestive of fibrosis, with statistical significance (Table 4). Table 2 – Analysis of the results of altered ischemia-inducing tests and results of myocardial scintigraphy (MS) Yes n (%) Result Altered ischemia-inducing test 189 (21.7) Normal MS 511 (58.6) Fixed low uptake 227 (26.1) Reversible low uptake 133 (15.3) Altered ischemia-inducing test: suggestive of ischemia. When assessing the primary endpoint, patients with fixed low uptake had an increased chance of developing AMI during the analyzed period that was 2.4-fold higher than patients with normal MS, but without statistical significance. When evaluating the occurrence of death, of the six recorded deaths, four had MS with fixed low uptake, with a more than 5-fold higher chance of having this outcome, with statistical significance (odds ratio - OR: 5.958; 95% confidence interval - 95%CI: 1.047 to 31.651; p = 0.043) (Table 4). In the group of patients that had MS with reversible low uptake suggestive of ischemia, the analysis of the variables showed that diabetes mellitus, previous known CAD and altered ischemia-inducing test (suggestive of ischemia) were associated with the development of reversible low uptake, which was statistically significant, with p < 0.05. The incidence of death and AMI was not statistically significant for this group of patients (Table 5). In the independent analysis of variables, for the occurrence of death and AMI it was observed that CRF and LVEF < 50% were predictors for the occurrence of death was statistically significant, with p = 0.001 and 0.031, respectively. The presence of factors such as smoking and LVEF < 50% was an independent predictor for the occurrence of AMI, with p = 0.037 and 0.039, respectively. Figure 1 shows the Kaplan-Meier curve for the presence of CRF and LVEF < 50% for the outcome of death. Figure 2 shows the Kaplan-Meier curve for the presence of smoking and LVEF < 50% for the occurrence of AMI. During the study period, 13 cases of AMI were obtained, of which four (30.8%) in the normal MS group, six (46.2%) in the MS group with fixed low uptake and three (23.1%) in MS group with reversible low uptake. Table 3 – Analysis on the association between clinical variables, risk factors, functional test results, events at the follow-up and normal myocardial scintigraphy (MS) Variables Normal MS n (%) p value OR 95%CI Systemic arterial hypertension 463 (86.5) 0.757 0.919 0.611-1.381 Dyslipidemia 377 (70.5) 0.102 0.770 0.565-1.051 Smoking 61 (11.4) 0.396 0.832 0.551-1.256 35 (6.5) 0.889 0.953 0.553-1.642 173 (32.3) 0.338 0.860 0.649-1.147 0.238-0.899 OPAD/ carotid disease Diabetes mellitus CRF 16 (3) 0.250 0.462 iCVA 13 (2.4) < 0.0001 0.214 0.112-0.411 147 (27.5) < 0.0001 0.149 0.110-0.202 LVEF < 50% 15 (2.8) < 0.0001 0.108 0.061-0.192 Family history of CAD 74 (13.9) 0.009 1.841 1.158-2.927 Altered ischemia-inducing test Previous CAD 102 (19.1) 0.018 0.674 0.487-0.934 AMI 4 (0.7) 0.04 0.274 0.840-0.896 Death 1 (0.2) 0.034 0.124 0.014-1.066 OR: Odds ratio; 95% CI: 95% confidence interval; OPAD: Occlusive peripheral arterial disease; CRF: Chronic renal failure; iCVA: Ischemic cerebrovascular accident; CAD: Coronary artery disease; LVEF: Left ventricular ejection fraction; AMI: Acute myocardial infarction. Arq Bras Cardiol. 2015; 105(2):112-122 115 Smanio et al. Myocardial perfusion without typical symptoms events Original Article Table 4 – Analysis of association between clinical variables, risk factors, functional test result, events at the follow-up and myocardial scintigraphy (MS) with fixed low uptake suggestive of fibrosis Variables Systemic arterial hypertension MS fibrosis n (%) p value OR 95%CI 194 (85.5) 0.492 0.846 0.547-1.309 Dyslipidemia 168 (74) 0.604 1.113 0.790-1.568 Smoking 30 (13.2) 0.557 1.138 0.724-1.790 OPAD/ carotid disease 20 (8.8) 0.162 1.541 0.877-2.208 Diabetes mellitus 75 (33) 0.870 0.964 0.699-1.329 CRF 17 (7.5) 0.007 2.526 1.299-4.912 iCVA 29 (12.8) < 0.001 4.818 2.644-8.786 Previous CAD 181 (79.7) < 0.001 8.307 5.776-11.947 LVEF < 50% 60 (26.4) < 0.001 8.540 5.227-13.952 Family history of CAD 17 (7.5) 0.0290 0.539 0.312-0.929 Altered ischemia-inducing test 40 (17.6) 0.092 0.771 0.482-1.047 AMI 6 (2.6) 0.113 2.471 0.821-7.430 Death 4 (1.8) 0.043 5.758 1.047-31.651 OR: Odds ratio; 95% CI: 95% confidence interval; OPAD: Occlusive peripheral arterial disease; CRF: Chronic renal failure; iCVA: Ischemic cerebrovascular accident; CAD: Coronary artery disease; LVEF: Left ventricular ejection fraction; AMI: Acute myocardial infarction. Table 5 – Analysis of the association between clinical variables, risk factors, functional test result, events in the follow-up and myocardial scintigraphy (MS) with reversible low uptake suggestive of ischemia Ischemia MS n (%) p value OR 95%CI Systemic arterial hypertension 122 (91.7) 0.093 1.799 0.938-3.450 Dyslipidemia 103 (77.4) 0.172 1.366 0.882-2.114 Smoking 16 (12) 1.000 0.985 0.558-1.736 OPAD/ carotid disease 7 (5.3) 0.574 0.748 0.332-1.686 55 (41.4) 0.046 1.481 1.015-2.162 7 (5.3) 0.487 1.311 0.564-3.050 Variables Diabetes mellitus CRF iCVA 9 (6.8) 0.534 1.303 0.615-2.2753 Previous CAD 84 (63.2) < 0.001 2.447 1.671-3.584 LVEF < 50% 18 (13.5) 0.153 1.542 0.885-2.689 Family history of CAD 13 (9.8) 0.557 0.799 0.432-1.476 Altered ischemia-inducing test 51 (38.3) < 0.001 2.704 1.821-4.016 AMI 3 (2.3) 0.432 1.680 0.456-6.187 Death 1 (0.8) 1.000 1.111 0.124-9.582 OR: Odds ratio; 95% CI: 95% confidence interval; OPAD: Occlusive peripheral arterial disease; CRF: Chronic renal failure; iCVA: Ischemic cerebrovascular accident; CAD: Coronary artery disease; LVEF: Left ventricular ejection fraction; AMI: Acute myocardial infarction. Six deaths were recorded, of which three were of cardiac origin. Of these three, two (33.3%) belonged to the fixed low uptake and one (16.7%) to the reversible low uptake group. The other three deaths were of noncardiac origin, with two (33.3%) in the fixed low uptake group and one (16.7%) in the normal scintigraphy group. 116 Arq Bras Cardiol. 2015; 105(2):112-122 During the mean follow-up of nearly 8 years, patients with normal MS showed better survival rates free of events such as death and AMI, when compared to that of patients with altered MS, with statistical significance, as demonstrated by the Kaplan-Meier curves (Figure 3). Smanio et al. Myocardial perfusion without typical symptoms events Original Article Event-free survival curve 1.0 0 No CRF 1 CRF 0.8 p = 0.001 0.6 0.4 0.2 0.0 0 500 1000 1500 2000 2500 3000 Cumulative survival x time Event-free survival curve 1.0 0 LVEF > 50% 1 LVEF < 50% 0.8 p = 0.031 0.6 0.4 0.2 0.0 0 500 1000 1500 2000 2500 3000 Cumulative survival x time Figure 1 – Kaplan-Meier curves for the occurrence of death vs. chronic renal failure (CRF) and vs. left ventricular ejection fraction (LVEF) < 50%. Discussion Recent publications have sought to identify subgroups of asymptomatic patients that could benefit from the MS for the detection of ischemia, such as those with early CAD family history and patients with anginal equivalent, OPAD, erectile dysfunction, chronic renal failure and type 2 diabetes. However, the evidence for MS indication in these subgroups is still scarce10. The American Society of Nuclear Cardiology (ASCN)9 recommends the performance of MS when screening for coronary disease in the following asymptomatic patient subgroups: those with high cardiovascular risk by the ATP III Arq Bras Cardiol. 2015; 105(2):112-122 117 Smanio et al. Myocardial perfusion without typical symptoms events Original Article Event-free survival curve 1.00 0 No SMK 1 SMK 0.98 p = 0.037 0.96 0.94 0.92 0.90 0 500 1000 1500 2000 2500 3000 Cumulative survival x time Event-free survival curve 1.00 0 LVEF > 50% 1 FEVE < 50% 0.95 p = 0.039 0.90 0.85 0.80 0 500 1000 1500 2000 2500 3000 Cumulative survival x time Figure 2 – Kaplan-Meier curves for the occurrence of acute myocardial infarction (AMI) and vs. smoking (SMK) vs. left ventricular ejection fraction (LVEF) <50%. criteria; those with Agatston calcium score > 400; diabetics; patients with CRF; patients with incomplete myocardial revascularization; and as follow-up in patients with myocardial revascularization, 5 years after the surgery. The results obtained in our study showed that MS should be performed in patients with high pretest probability, even without symptoms considered typical of ischemia, whether 118 Arq Bras Cardiol. 2015; 105(2):112-122 they have known coronary disease or not, as their outcome, when normal, is associated with low prevalence of major events in the follow-up. The safety period after the performance of MS with normal result was well evaluated in a meta-analysis that included 17 studies with 8,008 patients, which showed that a normal MS result had a high negative predictive value for cardiac events for 3 years14. Smanio et al. Myocardial perfusion without typical symptoms events Original Article Event-free survival curve 1.00 0 Abnormal MS 1 Normal MS 0.8 0.6 p = 0.036 0.4 0.2 0.0 0 500 1000 1500 2000 2500 3000 Cumulative survival x time Event-free survival curve 1.00 0 Abnormal MS 1 Normal MS 0.98 0.96 p = 0.019 0.94 0.92 0.90 0 500 1000 1500 2000 2500 3000 Cumulative survival x time Figure 3 – Event curves (acute myocardial infarction and death) in patients with normal or abnormal myocardial scintigraphy (MS). A study published by Ottenhouf et al. 15 evaluated 261 patients with known CAD and normal myocardial perfusion scintigraphy, who were followed for a mean period of 12 years, assessing as primary endpoint of death from all causes, cardiac death and AMI and / or cardiac death. They also analyzed independent predictors for the occurrence of events during this period. The results showed 94 (36%) deaths, 26 (10%) due to cardiac causes and 15 (6%) due to AMI; of the risk factors, age and diabetes were predictors for the event death from all causes, with statistical significance Arq Bras Cardiol. 2015; 105(2):112-122 119 Smanio et al. Myocardial perfusion without typical symptoms events Original Article (OR: 1.05; 95% CI: 1.03 to 1.07; p < 0.05; and OR: 2.13; 95%CI: 1.23 to 3.71; p < 0.05, respectively). Age and male gender were predictors for cardiac death, also with statistical significance (OR: 1.05; 95% CI: 1.01-1.10; p < 0.05; and OR: 2.45; 95% CI: 1.07 to 5.64; p < 0.05, respectively). Diabetes was associated with the occurrence of cardiac death and / or AMI, also with statistical significance (OR: 2.34; 95% CI: 1.03 to 5.30; p < 0.05). In the same study, the normal MS was associated with a lower probability of death from all causes, cardiac death and AMI and/or cardiac death, with annual event rates of 3.2, 0.9 and 1.2%, respectively. Schinkel et al. 16, in another recent study, evaluated 233 patients with suspected or known CAD who underwent MS with 99m Tc-setamibi and had normal myocardial perfusion. They were followed for a mean of 15.5 years for the occurrence of death from all causes, cardiac death, AMI, and major cardiac events, defined as the occurrence of cardiac death, myocardial infarction and need for myocardial revascularization. Among the 233 patients, there were 41 (18%) deaths from all causes, of which 13 were cardiac deaths; 18 (8%) had AMI; and 47 (20%) required myocardial revascularization, of which 7% were submitted to cardiac surgery and 13% to PCI. The event annual rates for death from all causes, cardiac death and / or AMI and the presence of major cardiac events were 1.1, 0.3, 0.7 and 1.8%, respectively. Factors such as age, male gender and diabetes were independent predictors for the occurrence of death from all causes, with statistical significance (OR: 1.06; 95% CI: 1.04‑1.09; p < 0.001; OR; 2.70; 95% CI: 1.45 to 5.03; p = 0.002; and OR: 3.06; 95% CI, 1.22 to 7.65; p = 0.02, respectively). Factors such as male gender and diabetes were also independent predictors for the occurrence of major cardiac events with statistical significance (OR: 2.61; 95% CI: 1.11 to 6.14; p = 0.03; and OR: 6.93; 95% CI: 2.18 to 22.04, p = 0.01, respectively). It was concluded that patients with known or suspected CAD showed a favorable outcome during the analyzed period, especially during the first 5 years. In comparison, this study showed normal MS in 511 patients (58.6%); 388 (44.5%) of them had known CAD, 293 (33.6%) patients had diabetes mellitus and 611 (70%) were classified as high risk by the Framingham score. Nevertheless, the group with normal MS showed lower probability of events such as death (p = 0.019) and AMI (p = 0.036) during the analyzed period with statistical significance, suggesting that patients with normal MS, even though they are at high cardiovascular risk, are less likely to have major events in the follow-up over a mean period up to 8 years. In this study, when analyzing which variables were independent predictors of events such as death and AMI, it was verified that the presence of CRF and LVEF < 50% were risk factors associated with death, with statistical significance, with p = 0.001 and p = 0.031, respectively. For the occurrence of AMI, risk factors such as smoking and LVEF < 50% were associated with higher probability of this event, also with statistical significance, with p = 0.037 and 0.039, respectively. 120 Arq Bras Cardiol. 2015; 105(2):112-122 It was also observed that patients with fixed low uptake in the MS showed higher probability of death outcome, with p = 0.043. Risk factors such as CRF, previous CVA, known CAD and LVEF < 50%, were, in turn, associated with the occurrence of fixed low uptake, suggestive of fibrosis. Study limitations In this group of patients that was totally asymptomatic or without typical symptoms of ischemia since the medical consultation when the scintigraphy was requested, 44.5% had known coronary disease. In fact, the aim of this study was to evaluate events in patients without typical symptoms, and not in individuals without typical symptoms and without known CAD; therefore, the group with known CAD was not excluded. The idea for this study appeared when we discovered that, unlike what is recommended by the appropriate use criteria, many patients in our institution undergo scintigraphy even when they are asymptomatic and we tried to retrospectively determine whether the method discriminated events in asymptomatic patients, with most of them being considered as high risk according to the Framingham score. We observed that the method is of great value to discriminate major events in the follow-up. Scintigraphy was analyzed qualitatively and magnitude (intensity and extent of perfusion findings) was not evaluated. The exercise test was interpreted as suggestive of ischemia due to the presence of suggestive clinical signs and symptoms and the presence of ECG alterations, whereas prognostic scores, such as the Duke score, was not analyzed. Conclusion The results obtained suggest that in the group of patients without typical symptoms (asymptomatic or with atypical symptoms), submitted to myocardial scintigraphy, the occurrence of major cardiac events such as death and acute myocardial infarction was small. The event-free period after normal myocardial scintigraphy in this group was 7.5 years. The presence of perfusion alterations suggestive of fibrosis in the myocardial scintigraphy was associated with an increased number of deaths at follow-up and might, therefore, be considered an adjunctive risk factor for more detailed patient assessment and monitoring. The occurrence of acute nonfatal myocardial infarction showed no statistically significant difference between the groups of patients with normal perfusion, suggestive of fibrosis or ischemia. Risk factors associated with perfusion abnormalities suggestive of fibrosis in the assessed group were chronic renal failure, ischemic stroke, known prior coronary artery disease and left ventricular ejection fraction < 50%. Diabetes, previous coronary artery disease and ischemic test (exercise or dipyridamole test) showed to be associated with myocardial scintigraphy suggestive of ischemia, but patients with this alteration in the myocardial scintigraphy showed no statistical significance for death or acute myocardial infarction, probably because they were submitted to therapeutic optimization and/or some type of therapeutic intervention. Smanio et al. Myocardial perfusion without typical symptoms events Original Article Risk factors considered to be independent predictors of death were chronic renal failure and left ventricular ejection fraction < 50%. Smoking and left ventricular ejection fraction < 50% were independent predictors of nonfatal acute myocardial infarction, regardless of the myocardial scintigraphy result. Author contributions Conception and design of the research:Smanio PEP. Acquisition of data:Smanio PEP, Silva JH, Holtz JV, Ueda L, Abreu M, Marques C. Analysis and interpretation of the data: Silva JH, Holtz JV, Machado L. Writing of the manuscript:Smanio PEP. Critical revision of the manuscript for intellectual content: Smanio PEP. Potential Conflict of Interest No potential conflict of interest relevant to this article was reported. Sources of Funding There were no external funding sources for this study. Study Association This study is not associated with any thesis or dissertation work. References 1. Bonow RO, Smaha LA, Smith SC Jr, Mensah GA, Lenfant C. World Heart Day 2002: the international burden of cardiovascular disease: responding to the emerging global epidemic. Circulation. 2002;106(13):1602-5. 2. Lessa I. Medical care and deaths due to coronary artery disease in Brazil, 1980-1999. Arq Bras Cardiol. 2003;81(4):336-42, 329-35. 3. Piegas LS, Avezum A, Guimarães HP, Muniz AJ, Reis HJ, Santos ES, et al. Comportamento da síndrome coronariana aguda: resultados de um registro brasileiro. Arq Bras Cardiol. 2013;100(6):502-10. 4. Ministério da Saúde. Datasus. [internet]. Sistema de informações de mortalidade: óbitos por residência por ano do óbito segundo capítulo CID10. Dados preliminares de mortalidade 2010. [Acesso em 2012 fev 03]. Disponível em: http://www.datatsus.gov.br. 5. Ministério da Saúde. Datasus. [internet]. Sistema de informações hospitalares. Intervençoes e valor total de internações segundo capítulo CID-10. [Acesso em 2011 fev 14]. Disponível em: htpp//www.datasus.gov.br. 6. Armaganijan LV, Armaganijan D, Sampaio MF. Insuficiência coronária crônica: apresentações clinicas. In: Timerman A, Bertolami MC, Ferreira FM. Manual de cardiologia. São Paulo: Atheneu; 2012. p. 199-201. 7. Smanio PE, Buchpiguel CA. Medicina Nuclear: Princípios gerais, indicações e interpretação. In: Timerman A, Bertolami MC, Ferreira FM. Manual de cardiologia. São Paulo: Atheneu; 2012. p. 781-9. 8. Robilotta CC. Noções de processamento de imagens. In: Thom AF, Smanio PEP. (eds.). Medicina nuclear em cardiologia: da metodologia à clínica. São Paulo: Atheneu; 2007. p. 37-44. 9. Hendel RC, Abbott BG, Bateman TM, Blankstein R, Calnon DA, Leppo JA, et al; American Society of Nuclear Cardiology. The role of radionuclide myocardial perfusion imaging for asymptomatic individuals. J Nucl Cardiol. 2011;18(1):3-15. 10. Hendel RC, Berman DS, Di Carli MF, Heidenreich PA, Henkin RE, Pellikka PA, et al; American College of Cardiology Foundation Appropriate Use Criteria Task Force; American Society of Nuclear Cardiology; American College of Radiology; American Heart Association; American Society of Echocardiology; Society of Cardiovascular Computed Tomography; Society for Cardiovascular Magnetic Resonance; Society of Nuclear Medicine. ACCF/ASNC/ACR/AHA/ASE/SCCT/SCMR/SNM 2009 Appropriate Use Criteria for Cardiac Radionuclide Imaging: a Report of the American College of Cardiology Foundation Appropriate Use Criteria Task Force, the American Society of Nuclear Cardiology, the American College of Radiology, the American Heart Association, the American Society of Echocardiography, the Society of Cardiovascular Computed Tomography, the Society for Cardiovascular Magnetic Resonance, and the Society of Nuclear Medicine. J Am Coll Cardiol. 2009;53(23):2201-29. 11. Sociedade Brasileira de Cardiologia; Sociedade Brasileira de Hipertensão; Sociedade Brasileira de Nefrologia. VI Diretrizes brasileiras de hipertensão. Arq Bras Cardiol. 2010;95(1 supl. 1):1-51. 12. Sposito AC, Caramelli B, Fonseca FA, Bertolami MC, Afiune Neto A, Souza AD, et al.; Sociedade Brasileira de Cardiologia. IV Diretriz brasileira sobre dislipidemias e prevenção da aterosclerose. Arq Bras Cardiol. 2007;88(supl 1):1-18. 13. Fletcher GF, Ades PA, Kligfield P, Arena R, Balady GJ, Bittner VA, et al; American Heart Association Exercise, Cardiac Rehabilitation, and Prevention Committee of the Council on Clinical Cardiology, Council on Nutrition, Physical Activity and Metabolism, Council on Cardiovascular and Stroke Nursing, and Council on Epidemiology and Prevention. Exercise standards for testing and training: a scientific statement from the American Heart Association. Circulation. 2013;128(8):873-934. 14. Metz LD, Beattie M, Hom R, Redberg RF, Grady D, Fleischmann KE. The prognostic value of normal exercise myocardial perfusion imaging and exercise echocardiography: a meta-analysis. J Am Coll Cardiol. 2007;49(2):227-37. 15. Ottenhof MJ, Wai MC, Boiten HJ, Korbee RS, Valkema R, van Domburg RT, et al. 12-Year outcome after normal myocardial perfusion SPECT in patients with known coronary artery disease. J Nucl Cardiol. 2013;20(5):748-54. 16. Schinkel AF, Boiten HJ, van der Sijde JN, Ruitinga PR, Sijbrands EJ, Valkema R, et al. 15-Year outcome after normal exercise 99mTc-sestamibi myocardial perfusion imaging: what is the duration of low risk after a normal scan? J Nucl Cardiol. 2012;19(5):901-6. Arq Bras Cardiol. 2015; 105(2):112-122 121 Smanio et al. Myocardial perfusion without typical symptoms events Original Article 122 Arq Bras Cardiol. 2015; 105(2):112-122 Back to the Cover Original Article New Exercise-Dipyridamole Combined Test for Nuclear Cardiology in Insufficient Effort: Appropriate Diagnostic Sensitivity Keeping Exercise Prognosis Inés Vidal Cortinas, Mario Beretta, Omar Alonso, Fernando Mut Departamento de Medicina Nuclear do Hospital ‘Asociación Española’, Br. Artigas 1515, Montevideo – Uruguay Abstract Background: Myocardial perfusion scintigraphy (MPS) in patients not reaching 85% of the maximum predicted heart rate (MPHR) has reduced sensitivity. Objectives: In an attempt to maintain diagnostic sensitivity without losing functional exercise data, a new exercise and dipyridamole combined protocol (EDCP) was developed. Our aim was to evaluate the feasibility and safety of this protocol and to compare its diagnostic sensitivity against standard exercise and dipyridamole protocols. Methods: In patients not reaching a sufficient exercise (SE) test and with no contraindications, 0.56 mg/kg of dipyridamole were IV administered over 1 minute simultaneously with exercise, followed by 99mTc-MIBI injection. Results: Of 155 patients, 41 had MPS with EDCP, 47 had a SE test (≥ 85% MPHR) and 67 underwent the dipyridamole alone test (DIP). They all underwent coronary angiography within 3 months. The three stress methods for diagnosis of coronary lesions had their sensitivity compared. For stenosis ≥ 70%, EDCP yielded 97% sensitivity, SE 90% and DIP 95% (p = 0.43). For lesions ≥ 50%, the sensitivities were 94%, 88% and 95%, respectively (p = 0.35). Side effects of EDCP were present in only 12% of the patients, significantly less than with DIP (p < 0.001). Conclusions: The proposed combined protocol is a valid and safe method that yields adequate diagnostic sensitivity, keeping exercise prognostic information in patients unable to reach target heart rate, with fewer side effects than the DIP. (Arq Bras Cardiol. 2015; 105(2):123-129) Keywords: Coronary Artery Disease; Exercise Test; Myocardial Perfusion Imaging/methods; Dipyridamole/diagnostic use. Introduction The reduced diagnostic sensitivity of myocardial perfusion scintigraphy (MPS) in patients not achieving a sufficient exercise (SE) test is well recognized 1-4 . Many laboratories, in the absence of contraindications, usually perform a vasodilator test in these patients, either on the same session or on a separate one. However, this procedure is time consuming and cost-inefficient, since the stress laboratory personnel needs to perform and monitor a full second stress test. Knowing the functional capacity is important for prognosis in patients evaluated for coronary artery disease (CAD) 5-9 . The same can be said of the chronotropic response to exercise and the speed of heart rate recovery10,11. Therefore, in order to improve diagnostic sensitivity without losing functional ergometric data, patients with insufficient exercise tests could benefit from a combined protocol that uses vasodilators in addition to physical stress. Another advantage would be the fact that patients would not be transferred from the treadmill or bicycle to a stretcher, where they would wait for recovery before receiving the pharmacologic stimulus. Adequate diagnostic sensitivity has been reported in patients with insufficient exercise tests and limited exercise capacity by using a combined protocol of exercise and dipyridamole12. Also, the side effects of dipyridamole are less serious in patients who exercise at the same time13‑16. Further consideration must be given to the improved diagnostic quality of the scintigraphic images achieved with the simultaneous injection of the vasodilator. This is due to a diminished hepatic and intestinal uptake of the radiotracer, which is usually high after dipyridamole13-16. The objectives of our investigation were: Mailing Address: Inés Vidal Cortinas • Presidente Giró, 2540, La Blanqueada. Postal Code 11600, Montevideo – Uruguay E-mail: [email protected], [email protected] Manuscript received June 06,2014; revised manuscript January 01,2015; accepted January 01,2015. DOI: 10.5935/abc.20150051 123 1) To establish the safety and sensitivity for CAD diagnosis of a new protocol combining exercise and dipyridamole given over the course of 1 minute; 2)To validate that protocol use for patients performing insufficient exercise test by comparing its diagnostic sensitivity with those of conventional tests: SE test and dipyridamole alone test (DIP). Vidal et al. Combined Diagnostic Test in Insufficient Exercise Original Article Methods Since March 2004, every patient submitted to stress MPS, who performed an insufficient exercise test [who did not reach at least 85% of the maximum predicted heart rate (MPHR) for their age, calculated as 220 - age in years] and had no contraindication for vasodilators, was injected with 0.56 mg/kg of dipyridamole over 1 minute while maintaining the physical stress. One minute after the completion of dipyridamole infusion, 99mTc-methoxy-isobutyl-isonitrile (99mTc-MIBI) was intravenously (IV) administered at the dose of 14 MBq/kg. If the patient was unable to keep exercising at the maximum effort achieved, the workload was lowered during the dipyridamole infusion. This allowed all patients to keep at least some level of exercise until test completion. One minute after the tracer injection, 240 mg of aminophylline were IV administered, and upon completion, exercise was stopped (Figure 1). Due to the incorporation of this protocol, all patients were instructed to fast for at least 2 hours prior to the test and to abstain from caffeine and other xanthines for at least 24 hours. Informed consent was obtained in all cases. Exercise was performed on a cycle-ergometer placed vertically, adding weights of 150 or 300 kgm/min at each stage. The protocol included the acquisition of a post-stress gated SPECT scan, approximately 30‑45 minutes after the injection of the radiotracer, and of a rest gated SPECT on a separate day. Studies were obtained using a dual-head camera equipped with high-resolution collimators, 180° rotation, 32 projections, 40 s/projection, 8 frames/cycle, no arrhythmia rejection and a 64×64 matrix with 1.5 zoom. These studies were reconstructed using iterative algorithm (OSEM) without attenuation or scatter correction, and realigned along the heart axis. Image interpretation was performed by one or more members of our medical staff. Diagnostic criteria were based on the presence of reversible perfusion defects (considered as ischemia), fixed perfusion defects (considered as infarction), or partially reversible defects (considered as infarction plus ischemia). No quantitative analysis was used, but rather the visual analysis of experienced observers. We included patients studied with MPS using our exercise-dipyridamole combined protocol (EDCP), patients having SE tests, and patients undergoing conventional DIP (0.56 mg/kg over 4 minutes). All patients included in this investigation were studied during the first half of 2012, and the selection criterion was that they should have a coronary angiography performed no later than 3 months after the MPS. Side effects of the new protocol were recorded and compared with those of the conventional DIP. The diagnostic sensitivity of the proposed protocol for severe coronary lesions (stenosis of ≥ 70%, and ≥ 50% in case of left main coronary artery involvement) as well as for moderate ones (stenosis of ≥ 50%) was determined. Sensitivity was calculated with the 95% confidence interval (95% CI). The Student’s t Test was used for the comparison of sample means, and the Chi‑square Test was used for categorical data comparison among different subsamples. Group differences were considered significant at p < 0.05, and calculations were performed using GraphPad Prism software, version 6.00 for Windows (GraphPad Software, La Jolla, California, USA). Results Of 155 patients recruited, the EDCP was followed in 41 [73% male, mean age 62.26 (SD = 9.4) years]. Forty-seven patients [72% male, mean age 59.8 (SD = 9.2) years] underwent a SE test, while the DIP was performed in 67 patients [51% male, mean age 64 (SD = 9.2) years]. There were no significant Exercise/dipyridamole protocol Dipyridamole 0.56 mg/kg 99 mTc-MIBI 25 mCi Aminophylline 240 mg Exercise Vital signs supervsion Figure 1 – Schematic representation of the proposed combined protocol. Arq Bras Cardiol. 2015; 105(2):123-129 124 Vidal et al. Combined Diagnostic Test in Insufficient Exercise Original Article differences in the mean age of the three groups of patients. Risk factors resulted similar among groups, except for overweight, which was less prevalent in the SE group (Table 1). There were no significant differences regarding the presence of previous myocardial infarction: 15 patients in the EDCP group; 14 patients in the SE group; and 22 patients in the DIP group (p = 0.79). groups (p < 0.001). Dizziness was present in 5 patients (12%) of the EDCP and in 4 patients of the DIP group (6%) (p = 0.25). A mean drop of 26 (SD = 13.6) mm Hg in systolic blood pressure was found in patients who did not experience symptoms, while the decrease was 37 (SD = 15) mm Hg in patients with dizziness (p = 0.14). Patients undergoing SE test reached a higher mean heart rate and developed a higher metabolic output than those following the combined protocol: 87% vs. 70% of MPHR, and 5.8 (SD = 1.56) vs. 5.1 (SD = 1.57) METs, respectively, each with p = 0.03. In patients undergoing EDCP, mean systolic blood pressure was 180 (SD = 27) mm Hg at maximum effort and decreased to 152 (SD = 24) mm Hg after dipyridamole injection (p < 0.001), while mean diastolic blood pressure values were 103 (SD = 13) mm Hg and 88 (SD = 13) mm Hg, respectively (p < 0.001). No change in the PR interval was found with either the DIP protocol or the EDCP. There were no significant differences in CAD prevalence among the three groups of patients, either regarding the severity of the lesions or the number of affected vessels (Table 2). In 83% of the patients, severe coronary lesions were found (76% of those following the EDCP, 83% with SE, and 87% with DIP). In 42%, one vessel was affected, in 24%, two vessels, and in 17%, three vessels or its equivalent (left main and right coronary artery). The combined protocol had 97% diagnostic sensitivity for severe coronary lesions (95% CI: 83.2% to 99.5%), while the SE test showed 90% (95% CI: 75.8% to 97.1%) and the DIP protocol, 95% (95% CI: 85.8% to 98.9%), with no significant difference among them (p = 0.43) (Figure 2). At least moderate coronary lesions were present in 88% of the total population (85% of patients following the EDCP, 87% of those with SE test, and 91% of those with DIP). The EDCP showed 94% sensitivity for moderate coronary lesions (95% CI: 80.8% to 99.1%); the ES test showed 88% (95% CI: 73.8% to 95.9%), and the DIP protocol, 95% (95% CI: 86.3% to 98.9%). These differences in sensitivity between the different types of protocols showed no statistical significance (p = 0.35) (Figure 2). Regarding side effects, 49 patients in the DIP group (73%) showed one or more. Headache was present in 40% of the patients, flushing in 30%, weakness in 22%, gastric discomfort in 10%, and dizziness in 6%. Conversely, dizziness was the only side effect present with the EDCP (5 patients), usually in connection to a drop in blood pressure. These results establish a difference of statistical significance between both Discussion The idea of combining an insufficient exercise test with a dipyridamole stimulus in order to reach adequate diagnostic sensitivity without losing functional capacity data seems to be theoretically correct and to have achieved positive practical results. Candell-Riera et al.12 have shown that the diagnostic sensitivity for 50% coronary stenosis of their combined protocol (89%) was significantly higher than that of the insufficient effort test (71%) and comparable to that of the SE test (93%). We achieved similar results: the difference between the diagnostic sensitivity of our combined protocol and that of the SE for coronary lesions ≥ 50% was not significant. We also compared it to the DIP protocol alone and found no diagnostic difference either. However, we made no comparison with the diagnostic sensitivity of the insufficient exercise test alone. As a rule, no insufficient effort scintigraphy is performed in our laboratory except when it is specifically required by the attending physician. Before the EDCP was adopted, any patient who failed to reach at least 85% of the MPHR was laid in a stretcher and, after 10-15 minutes, underwent conventional dipyridamole test. With EDCP, adequate diagnostic sensitivity is achieved without losing information from the exercise test about functional capacity and chronotropic response. Furthermore, the total time required for completion of the full procedure is shortened. Candell-Riera et al.12 have administered IV 0.56 mg/kg of dipyridamole over 4 minutes during the exercise test. The major differences with our protocol are that we give the dose in only 1 minute and that it is used in all patients not reaching sufficient effort, not only those achieving less than 5 METs. We chose to shorten the infusion time because most patients with insufficient exercise tests showed difficulties in maintaining the effort further. Unlike the investigation by the abovementioned authors, heart rate alone was taken Table 1 – Risk factors in the three groups of patients Risk factor EDCP (n = 41) SE (n = 47) DIP (n = 67) p value Diabetes 13 (32%) 9 (19%) 19 (28%) 0.36 Hypertension 27 (66%) 31 (66%) 52 (78%) 0.28 Dyslipidemia 26 (63%) 27 (57%) 35 (52%) 0.52 Smoking 12 (29%) 9 (19%) 17 (25%) 0.53 BMI ≥ 25 25 (61%) 16 (34%) 40 (60%) 0.01 Family history 15 (37%) 24 (51%) 34 (51%) 0.29 EDCP: Exercise-dipyridamole combined protocol; SE: Sufficient exercise test; DIP: Dipyridamole only; BMI: Body mass index. 125 Arq Bras Cardiol. 2015; 105(2):123-129 Vidal et al. Combined Diagnostic Test in Insufficient Exercise Original Article Table 2 – Prevalence of CAD among the three groups Angiography EDCP (n = 41) SE (n = 47) DIP (n = 67) Total (n = 155) p value Lesions ≥ 70% 31(76%) 39(83%) 58(87%) 128(83%) 0.45 3V 8(20%) 6(15%) 12(18%) 26(17%) 0.66 2V 8(20%) 10(21%) 19(28%) 37(24%) 0.51 1V 15(37%) 23(49%) 27(40%) 65(42%) 0.47 Lesions ≥ 50% 35(85%) 41(87%) 61(91%) 137(88%) 0.19 3V 12(29%) 11(23%) 15(22%) 38(25%) 0.71 2V 9(22%) 8(17%) 18(27%) 35(23%) 0.46 14(34%) 22(47%) 28(42%) 64(41%) 0.48 1V EDCP: Exercise-Dipyridamole Combined Protocol; SE: Sufficient exercise test; DIP: Dipyridamole only; V: Vessel. Diagnostic sensitivity 100 97 94 90 95 90 95 88 80 70 60 50 40 30 20 10 0 EDCP (n = 41) SE (n = 47) Stenosis ≥ 70% DIP (n = 67) Stenosis ≥ 50% Figure 2 – Comparison of diagnostic sensitivity of the three protocols for coronary stenosis ≥ 70% and ≥ 50%. EDCP: Exercise-Dipyridamole Combined Protocol; SE: Sufficient exercise test; DIP: Dipyridamole only. into account and not METs; whenever 85% of MPHR was not reached – and no contraindications were present – dipyridamole was always administered. Our results seem to validate the followed criteria, since the diagnostic sensitivity of the EDCP was not significantly different from that of the SE test, even though some patients with a mean metabolic output higher than 5 METs (5.1, SD = 1.57) were included. It could be argued that full vasodilation effect of dipyridamole might not have been reached in every case at the time of the radiotracer injection due to the short time allowed for the pharmacologic action. However, no difference in sensitivity was demonstrated compared to conventional protocols. This fact permits the assumption that vasodilation was adequate enough for diagnostic purposes. Furthermore, even if pharmacologic vasodilation was not optimal, it should be taken into account that some vasodilation was already present with exercise, and that myocardial extraction of the radiotracer is not linear with flow, especially at high values17, so a marginal increase with time might not be reflected in imaging. We also confirmed the previously demonstrated fact that the combination of exercise with dipyridamole produces fewer side effects than the use of dipyridamole alone. Patients studied with the new combined protocol only presented dizziness in 12%, which can be associated with a decrease in blood pressure. This decline (rapidly compensated laying the patient down) could be explained by the vasodilatation effect of dipyridamole, as well as by the physiologic decrease resulting from exercise cessation or reduction. In fact, patients presenting dizziness underwent Arq Bras Cardiol. 2015; 105(2):123-129 126 Vidal et al. Combined Diagnostic Test in Insufficient Exercise Original Article a more pronounced yet non-significant decrease in systolic blood pressure. Conversely, most patients (73%) studied with the DIP protocol experienced some kind of discomfort, mostly headache. The usual supine position during conventional pharmacologic stress allows better tolerance to hypotension than the upright position. Nevertheless, we did not find a statistical significant difference regarding the presence of dizziness for both groups. At the beginning of the implementation of the combined protocol, we usually asked the patient to stop exercising after MIBI injection. Afterwards, aminophylline administration was started. We frequently observed a sudden drop in blood pressure, caused by the vasodilatation effect of dipyridamole added to the abrupt cessation of the physical effort. This was resolved by quickly positioning the patient in the decubitus position. In consequence, we decided thereafter to ask the patients to keep pedaling at a lower level until the aminophylline infusion was completed. As a result, the prevalence of dizziness as a side effect was reduced significantly, as described in the study. The association of exercise with dipyridamole has also proved to increase image quality13-16. Even though image characteristics in the various protocols considered in our investigation were not specifically evaluated, all the images were adequate for diagnostic purposes according to standard criteria of interpretation. To our knowledge, with the exception of our protocol and of that described by Candell-Riera et al.12, all others combining exercise with dipyridamole start first with the vasodilator drug, being then complemented with exercise, either at a low‑level or limited by symptoms13,16,18. However, this sequence does not allow clinical monitoring, which is more relevant in patients with exercise-related symptoms, or proper evaluation of functional capacity. Ahlberg et al.18 reported that almost one third of patients referred for MPS reached 85% of their MPHR. If this had been known in advance, the stimulation with dipyridamole before the exercise would have been unnecessary. These authors proved the prognostic value of their protocol combining dipyridamole with symptom-limited exercise, but they recognized limitations by not comparing with a similar group of patients reaching suboptimal effort or using dipyridamole alone. An editorial 19 written about their work mentions the need of a control group, such as dipyridamole with low-level exercise, dipyridamole alone, or exercise alone. In addition, the lack of coronary angiography to evaluate the sensitivity and specificity of the test is highlighted. Therefore, it is not known whether the dipyridamole/exercise test limited by symptoms improves the diagnostic sensitivity for CAD when compared to other protocols. The same conclusions could be drawn from the analysis of adenosine/exercise protocols. An approach similar to ours has been possible with regadenoson, a vasodilating drug , which specifically stimulates the A2a receptors. In recent works by Parker et al.20 and Ross et al.21, regadenoson was administered at peak exercise in bolus injection if the patient had not reached 85% of the MPHR. However, the subjects studied were submitted 127 Arq Bras Cardiol. 2015; 105(2):123-129 to a pharmacologic stress and agreed to undergo an exercise test as an additional procedure. They were not patients directly assigned to an exercise MPS who did not reach the target heart rate. Parker et al.20 reported that 50% of their patients were able to reach 85% of the target heart rate, while this was the case in 62.5% of the patients in the series by Ross et al.21. Hence, at least half of their patients did not formally require the administration of a vasodilator stimulus since the exercise was adequate. This highlights a frequently mistaken medical perception of the patient’s exercise capacity when perfusion tests are indicated. It also supports the design of a protocol geared towards complementing an insufficient exercise test while at the same time saving the prognostic functional data of physical stress. Therefore, every patient referred to our department for an exercise MPS is instructed to abstain from xanthines for 24 hours previous to the test, just in case dipyridamole has to be administered in a combined protocol. In regard to this, we share the idea of administering a vasodilator when necessary22. Both Parker et al.20 and Ross et al.21 have demonstrated that their respective protocols are feasible and safe, and are associated with fewer side effects compared to the administration of regadenoson only. However, their patients underwent no coronary angiography, so the diagnostic sensitivity was not determined. The current work proves that our EDCP is feasible, safe, and, more importantly, has a diagnostic sensitivity at least similar to that provided by a SE test or a DIP test alone. Together with the evaluation of exercise-induced symptoms, ECG changes, functional capacity and chronotropic response, we could say that, paraphrasing Hendel and Frost22, with our combined protocol, we work off-label, on target and with diagnostic accuracy. Limitations The coronary anatomy of only a few dozens of the hundreds of patients undergoing the EDCP was established, because the indication of a coronary angiography depended mainly on a positive nuclear test result, producing a strong referral bias that explains the high prevalence of CAD. This was an obvious obstacle to evaluate specificity, accuracy, as well as positive and negative predictive values of the technique. Conclusions We demonstrated that our combined protocol for MPS is well tolerated and yields at least similar diagnostic sensitivity as compared to a SE test or a DIP test alone. It preserves prognostic information from the exercise even when the test is insufficient. Additionally, it can be safely completed in a shorter time than other proposed combined protocols with dipyridamole, and close to that using regadenoson. Author contributions Conception and design of the research: Vidal I. Acquisition of data:Vidal I, Beretta M. Analysis and interpretation of the data: Vidal I, Mut F. Statistical analysis: Alonso O. Writing of the manuscript:Vidal I, Mut F. Critical Vidal et al. Combined Diagnostic Test in Insufficient Exercise Original Article revision of the manuscript for intellectual content: Mut F. Supervision / as the major investigador:Vidal I. Potential Conflict of Interest No potential conflict of interest relevant to this article was reported. Sources of Funding There were no external funding sources for this study. Study Association This study is not associated with any thesis or dissertation work. References 1. Iskandrian AS, Heo J, Kong B, Lyons E. Effect of the exercise level on the ability of thallium-201 tomographic imaging in detecting coronary artery disease: analysis of 461 patients. J Am Coll Cardiol 1989;14(6):1477-86. 2. Verzijlbergen JF, Vermeersch PH, Laarman GJ, Ascoop CA. Inadequate exercise leads to suboptimal imaging. Thallium-201 myocardial perfusion imaging after dypiridamole combined with low-level exercise unmasks ischemia in symptomatic patients with non-diagnostic thallium-201 scans who exercise submaximally. J Nucl Med. 1991;32(11):2071-8. 3. Heller GV, Ahmed I, Tilkemeier PL, Barbour MM, Garber CE. Influence of exercise intensity on the presence, distribution, and size of thallium-201 defects. Am Heart J. 1992;123(4 Pt 1):909-16. 4. Santana-Boado C, Candell-Riera J, Castell-Conesa J, Olona M, PaletBalart J, Aguadé-Bruix S, et al. Influence of ergometric parameters on the results of myocardial perfusion tomographic scintigraphy. Med Clin (Barc). 1997;109(11):406-9. 5. Snader CE, Marwick TH, Pashkow FJ, Harvey SA, Thomas JD, Lauer MS. Importance of estimated functional capacity as a predictor of all-cause mortality among patients referred for exercise thallium single-photon emission computed tomography: report of 3,400 patients from a single center. J Am Coll Cardiol. 1997;30(3):641-8. 6. Lauer MS. Exercise electrocardiogram testing and prognosis: novel markers and predictive instruments. Cardiol Clin. 2001;19(3):401-14. 7. Myers J, Prakash M, Froelicher V, Do D, Partington S, Atwood JE. Exercise capacity and mortality among men referred for exercise testing. N Engl J Med. 2002;346(11):793-801. 8. Gulati M, Pandey DK, Arnsdorf MF, Lauderdale DS, Thisted RA, Wicklund RH, et al. Exercise capacity and the risk of death in women: the St James Women Take Heart Project. Circulation. 2003;108(13):1554-9. 9. Miller TD. Exercise treadmill test: estimating cardiovascular prognosis. Cleve Clin J Med. 2008;75(6):424-30. 10. Myers J, Tan SY, Abella J, Aleti V, Froelicher VF. Comparison of the chronotropic response to exercise and heart rate recovery in predicting cardiovascular mortality. Eur J Cardiovasc Prev Rehabil. 2007;14(2):215-21. 11. Gulati M, Shaw LJ, Thisted RA, Black HR, Bairey Merz CN, Arnsdorf MF. Heart rate response to exercise stress testing in asymptomatic women: the St. James women take heart project. Circulation. 2010;122(2):130-7. 12. Candell-Riera J, Santana-Boado C, Castell-Conesa J, Aguadé-Bruix S, Olona M, Palet J, et al. Simultaneous dipyridamole/maximal subjective exercise with 99mTc-MIBI SPECT: improved diagnostic yield in coronary artery disease. J Am Coll Cardiol. 1997;29(3):531-6. 13. Casale PN, Guiney TE, Strauss HW, Boucher CA. Simultaneous low level treadmill exercise and intravenous dipyridamole stress thallium imaging. Am J Cardiol. 1988;62(10 Pt 1):799-802. 14. Stern S, Greenberg ID, Corne RA. Qualification of walking exercise required for improvement of dipyridamole thallium-201 image quality. J Nucl Med. 1992;33(12):2061-6. 15. Brown KA. Exercise-dipyridamole myocardial perfusion imaging: the circle is now complete. J Nucl Med. 1993;34(12):2061-3. 16. Vitola JV, Brambatti JC, Caligaris F, Lesse CR, Nogueira PR, Joaquim AI, et al. Exercise supplementation to dypiridamole prevents hypotension, improves electrocardiogram sensitivity, and increases heart-to-liver activity ratio on Tc-99m sestamibi imaging. J Nucl Cardiol. 2001;8(6):652-9. 17. Berman DS, Kiat H, Maddahi J. The new 99mTc myocardial perfusion imaging agents: 99m-Tc-sestamibi and 99m.Tc-teboroxime. Circulation. 1991;84(3 Suppl):17-21. 18. Ahlberg AW, Baghdasarian SB, Athar H, Thompsen JP, Katten DM, Noble GL, et al. Symptom-limited exercise combined with dipyridamole stress: prognostic value in assessment of known or suspected coronary artery disease by use of gated SPECT imaging . J Nucl Cardiol. 2008;15(1):42-56. 19. Bybee KA, Bateman TM. Symptom-limited exercise during vasodilator stress: best of both worlds?. J Nucl Cardiol. 2008;15(1):3-6. 20. Parker MW, Morales DC, Slim HB, Ahlberg AW, Katten DM, Cyr G, et al. A strategy of symptom-limited exercises with regadenoson-as-needed for stress myocardial perfusion imaging: a randomized controlled trial. J Nucl Cardiol. 2013;20(2):185-96. 21. Ross MI, Wu E, Wilkins JT, Gupta D, Shen S, Aulwes D, et al. Safety and feasibility of adjunctive regadenoson injection at peak exercise during exercise myocardial perfusion imaging: the Both Exercise and Regadenoson Stress Test (BERST) trial. J Nucl Cardiol. 2013;20(2):197-204. 22. Hendel RC, Frost L. Off-label, but on target: use of regadenoson with exercise (editorial). J Nucl Cardiol. 2013;20(2):179-81. Arq Bras Cardiol. 2015; 105(2):123-129 128 Vidal et al. Combined Diagnostic Test in Insufficient Exercise Original Article 129 Arq Bras Cardiol. 2015; 105(2):123-129 Back to the Cover Original Article Cardiac Surgery Costs According to the Preoperative Risk in the Brazilian Public Health System David Provenzale Titinger, Luiz Augusto Ferreira Lisboa, Bruna La Regina Matrangolo, Luis Roberto Palma Dallan, Luis Alberto Oliveira Dallan, Evelinda Marramon Trindade, Ivone Eckl, Roberto Kalil Filho, Omar Asdrúbal Vilca Mejía, Fabio Biscegli Jatene Instituto do Coração do Hospital das Clínicas da Faculdade de Medicina da Universidade de São Paulo, São Paulo, SP – Brazil Abstract Background: Heart surgery has developed with increasing patient complexity. Objective: To assess the use of resources and real costs stratified by risk factors of patients submitted to surgical cardiac procedures and to compare them with the values reimbursed by the Brazilian Unified Health System (SUS). Method: All cardiac surgery procedures performed between January and July 2013 in a tertiary referral center were analyzed. Demographic and clinical data allowed the calculation of the value reimbursed by the Brazilian SUS. Patients were stratified as low, intermediate and high-risk categories according to the EuroSCORE. Clinical outcomes, use of resources and costs (real costs versus SUS) were compared between established risk groups. Results: Postoperative mortality rates of low, intermediate and high-risk EuroSCORE risk strata showed a significant linear positive correlation (EuroSCORE: 3.8%, 10%, and 25%; p < 0.0001), as well as occurrence of any postoperative complication (EuroSCORE: 13.7%, 20.7%, and 30.8%, respectively; p = 0.006). Accordingly, length-of-stay increased from 20.9 days to 24.8 and 29.2 days (p < 0.001). The real cost was parallel to increased resource use according to EuroSCORE risk strata (R$ 27.116,00 ± R$ 13.928,00 versus R$ 34.854,00 ± R$ 27.814,00 versus R$ 43.234,00 ± R$ 26.009,00, respectively; p < 0.001). SUS reimbursement also increased (R$ 14.306,00 ± R$ 4.571,00 versus R$ 16.217,00 ± R$ 7.298,00 versus R$ 19.548,00 ± R$935,00; p < 0.001). However, as the EuroSCORE increased, there was significant difference (p < 0.0001) between the real cost increasing slope and the SUS reimbursement elevation per EuroSCORE risk strata. Conclusion: Higher EuroSCORE was related to higher postoperative mortality, complications, length of stay, and costs. Although SUS reimbursement increased according to risk, it was not proportional to real costs. (Arq Bras Cardiol. 2015; 105(2):130-138) Keywords: Cardiac Surgical Procedures/economics; Hospital Costs; Unified Health System; Risk Groups; Preoperative Care; Hospital Mortality; Morbidity. Introduction During the last four decades, cardiac surgery has developed with the increase in complex procedures in progressively critically‑ill patients 1. Evidence shows that this scenario proportionally increases with morbimortality and hospital costs2,3. In Brazil, most of the highly complex procedures are performed with funding from the Unified Health System (SUS). This system is responsible for 80% of CABG surgeries performed in the country4. The reimbursement for hospitals that belong to SUS uses SUS own price list for the hospitalization authorization (AIH). The payment of this value is little yielding in its composition and may not reflect correct Mailing Address: Omar Asdrúbal Vilca Mejía • Instituto do Coração, Segundo Bloco, Segundo Andar, Sala 11. Avenida Doutor Enéas de Carvalho Aguiar, 44 – Cerqueira César. Postal Code 05403-900, São Paulo, SP – Brazil. E-mail: [email protected] Manuscript received October 30, 2014; revised manuscript March 23, 2015; accepted March 24, 2015. DOI: 10.5935/abc.20150068 130 fund allocation that correspond to the actual cost (AC) of the procedure5. Thus, the AIH paid by SUS for the procedure may have no direct association with patient severity. An unequal association between the AC of these procedures and SUS reimbursement may discourage hospital care provided to high-risk surgical patients, which are the cases that would benefit the most from these procedures6. On the other hand, international guidelines advise about the use of risk scores to identify patients at higher risk of morbimortality7. In Brazil, the EuroSCORE is the most used model and the only one that has been validated in significant samples8. The objective of this study was to evaluate the use of resources by risk group, comparing the AC of cardiovascular procedures with SUS reimbursement in a hospital. Methods Sample A prospective observational study carried out at the Cardiovascular Surgery Division and SUS Billing Unit of Instituto do Coração do Hospital das Clínicas da Faculdade de Titinger et al. Cardiac surgery costs according to the risk Original Article Medicina da Universidade de São Paulo (InCor-HC/FMUSP) (Heart Institute of the Faculty of Medicine, University of São Paulo (InCor-HC / USP)). Data from consecutive patients were obtained from the institution’s database (SI3). All demographic data that could identify patients were removed. Clinical data and use of resources were exported to an Excel spreadsheet for analysis. By cross-checking patients’ data with the registry of the participating units, it was verified that there were no errors and no patients loss due to lack of data. Inclusion and exclusion criteria The inclusion criteria were: adult patients consecutively operated between January and July 2013, in the elective, urgent or emergency mode, at the Cardiovascular Surgery Division of InCor-HC/FMUSP. Patients not hospitalized by SUS were excluded from the study. Data collection, definition and organization Data were collected prospectively in the electronic medical file system of InCor-HC/FMUSP (SI3). After exporting data to a single worksheet in Excel and removal of demographic data that could identify patients, this worksheet was adapted to take into account all the variables described in the first EuroSCORE model (additive version)9. All definitions assigned to variables by EuroSCORE were accomplished, together with their values, according to their relevance to the death event. Therefore, after calculating the value of the variables in each patient, the patients were classified according to the risk groups established by the model. In addition to the clinical and laboratory variables included in the EuroSCORE, the economic variables were considered. The total value of AC included fixed and variable costs per patient. The AC was calculated by analysis of variable costs accounted by the micro-costing methodology10 and by the full costing method for the fixed costs. The mean unit cost of each material item and medications was estimated from the purchases of these items during this period, being considered, in each category, the individual units costs. The mean unit cost of each diagnostic service, daily hospital stay costs or therapy was estimated by total inclusion of fixed costs (pro-rata of general consumption fixed costs – water, electricity and telephone, auxiliary services – maintenance contracts, cleaning services, air conditioning, etc., and administrative services) from the cost centers, divided by unit of produced outcome. Thus, we considered the quantitative variables ICU length of stay (days), hospitalization length of stay (days) and time of orotracheal intubation (hours). Similarly, it was considered the total value of SUS reimbursement, adding hospital service, professional service, ICU and compatible materials. The primary outcomes were in-hospital mortality and morbidity (cerebrovascular accident, Renal Replacement Therapy - RRT, pneumonia, atrial fibrillation, mediastinitis/ osteomyelitis and reoperation for bleeding). The definitions of the study variables outside the EuroSCORE were taken from the glossary of the American Heart Association11. All patients were followed until hospital discharge. Statistical analysis Continuous variables were expressed as mean ± standard deviation or median, and categorical variables as percentages. Logistic regression analysis for the hospital morbidity and mortality outcome was performed by using the value provided by EuroSCORE for each patient. Patients were subdivided by the EuroSCORE as low (1-4), intermediate (5-7), and high (≥ 8) risk. The three categories were analyzed to highlight the differences related to the morbimortality, resource use, AC and SUS reimbursement. Variable distribution was tested for normality using the Kolmogorov-Smirnov test. Variables with normal distribution were compared between the risk categories using analysis of variance. Paired comparisons were corrected using the Bonferroni-Dunn test. Student’s t test was used for parametric distributions, and the Mann-Whitney and Kruskal-Wallis tests were used for non-parametric distributions. Categorical variables were compared using Pearson’s chi-square test. The null hypothesis was rejected when p < 5% (p < 0.05). This study made a comparison, in the “real world”, between the mean costs of the risk categories, reducing the possibility of bias in patient selection12. The analysis was performed using the Statistical Package for the Social Sciences (SPSS) software, version 20.0.0 (Chicago, IL). Ethics and Consent Form This study was approved by the Ethics Committee for Analysis of Research Projects (CAPPesq) HC/FMUSP, under number 1575, being exempt from the need to use the Free and Informed Consent form, due to the use of analysis of non-identified data only. Results Sample The characteristics of patients in the different risk groups are shown in Table 1. The low-risk group consisted of 131 (34%) patients, the intermediate risk group, of 150 (39%) and the high-risk group of 104 (27%) patients. There were significant differences in EuroSCORE means according to the risk group: 2.91 ± 1.03, 5.89 ± 0.84 and 10.32 ± 2.6 in the lower, intermediate and high-risk categories, respectively. The mean age was 61 ± 12.29 years. Clinical outcomes and resource use The clinical outcomes and resource use are shown in Table 2. The EuroSCORE was associated with death (p < 0.0001) and showed good calibration (p = 0.9744) in the Hosmer‑Lemeshow test. Nevertheless, this model was associated with morbimortality (p < 0.0001) and also showed good calibration (p = 0.2221) in the Hosmer‑Lemeshow test. Mortality, morbidity and morbimortality of 11.26, 21.41 and 27.15% were observed, respectively. There was 3.82% of mortality in low risk, 10% in intermediate risk and 25% in high risk (Figure 1). The low-risk group had Arq Bras Cardiol. 2015; 105(2):130-138 131 Titinger et al. Cardiac surgery costs according to the risk Original Article Table 1 – Patient characteristics Characteristics Sample (n = 385) Low Risk (n = 131) Intermediate Risk (n = 150) High Risk (n = 104) p Age 61 ± 12.3 56.1 ± 10.3 61.2 ± 12.5 65.3 ± 12.5 < 0.001* Female gender 160 (41.6) 48 (36.6) 69 (46) 43 (41.3) 0.28 EuroSCORE 6.1 ± 3.3 2.9 ± 1 5.9 ± 0.8 10.3 ± 2.6 < 0.001* Creatinine > 2mg/dL 39 (10.1) 2 (1.5) 11 (7.3) 26 (25) < 0.001‡ Ejection fraction < 30% 32 (8.3) 7 (5.3) 16 (10.7) 9 (8.7) 0.27 Recent Infarction 42 (10.9) 7 (5.3) 18 (12) 17 (16.3) 0.012† Reoperation 68 (17.7) 5 (3.8) 25 (16.7) 38 (36.5) < 0.001* CABG 188 (48.8) 78 (59.5) 78 (52) 32 (30.8) < 0.001‡ HVS 173 (44.9) 50 (38.2) 63 (42) 60 (57.7) 0.002‡ CABG + HVS 21 (5.5) 3 (2.3) 7 (4.7) 11 (10.6) 0.007‡ Others (Not CABG + HVS) 3 (0.8) 0 1 (0.7) 2 (1.9) 0.28 Urgency / Emergency 17 (4.4) 2 (1.5) 6 (4) 9 (8.7) 0.014‡ Events 38 (9.9) 0 4 (2.7) 34 (32.7) < 0.001‡ The item “events” includes at least one of the following situations prior to surgery: intra-aortic balloon, cardiogenic shock, ventricular tachycardia or fibrillation, orotracheal intubation, acute renal failure, use of inotropic drugs and cardiac massage. * Significant difference between all risk groups; † Significant difference between the low/intermediate risk groups and the high-risk group; ‡ Significant difference between the low-risk group and the intermediate/high risk group. CABG: Coronary‑artery bypass grafting; HVS: Heart valve surgery. Table 2 – Clinical outcomes and resource utilization Variable Sample (n = 385) Low risk (n = 131) Intermediate risk (n = 150) High risk (n = 104) p Mortality 56 (14.5) 5 (3.8) 15 (10) 26 (25) < 0.001* Morbidity 81 (21) 18 (13.7) 31 (20.7) 32 (30.8) 0.004* CVA 1 (0.3) 1 (0.8) 0 0 0.61 Atrial fibrillation 30 (7.8) 6 (4.6) 15 (10) 9 (8.7) 0.22 RRT 15 (3.9) 4 (3.1) 2 (1.3) 9 (8.7) 0.003* Pneumonia 12 (3.1) 4 (3.1) 3 (2) 5 (4.8) 0.46 Reoperation x Bleeding 17 (4.4) 5(3.8) 4 (2.7) 8 (7.7) 0.15 OTI > 24h Time of ICU Hospital length of stay 22 (5.7) 3 (2.3) 9 (6) 10 (9.6) 0.055 8.3 ± 10.1 days 5.6 ± 5.9 days 8.1 ± 10.4 days 11.9 ± 12.6 days < 0.001‡ 25 ± 17days 21 ± 13.2days 25 ± 13.25 days 29 ± 16.3days < 0.001† * Significant difference between low / intermediate risk and high risk groups. †Significant difference between the low risk and intermediate / high risk groups. ‡ Significant difference between all risk groups. CVA: Cerebrovascular accident; RRT: Renal replacement therapy; OTI: Orotracheal intubation; ICU: Intensive care unit. the lowest percentage of deaths, which increased with the risk increase (p < 0.0001). There was 13.74% of morbidity in low risk, 20.67% in intermediate risk and 30.77% in the high risk. The low-risk group had a lower percentage of complications, which increased with the risk increase (p = 0.0063). There was 3.1% of RST in the low-risk, 1.3% in intermediate‑risk and 8.7% in the high-risk group. The low‑risk and intermediate‑risk groups had the lowest percentage of RST, and the high-risk group had the highest percentage (p = 0.003). While one can observe that, regarding the length of stay, the high-risk group showed no 132 Arq Bras Cardiol. 2015; 105(2):130-138 significant difference compared to the intermediate risk, the low-risk group had a significantly lower value than the groups at high and intermediate risk. In the analysis of ICU length of stay, we observed that the low‑risk group had significantly lower value than the groups with intermediate and high risk, and the group with intermediate risk had a significantly lower value than the high-risk group. SUS reimbursement and actual cost Risk groups differed in relation to the total value of the SUS reimbursement (low risk: R$ 14.306,00 ± R$ 4.571,00; Titinger et al. Cardiac surgery costs according to the risk Original Article 40 35 30 p = 0.002 p < 0.001 p < 0.001 p = 0.155 25 % p = 0.052 Low 20 15 p < 0.001 p = 0.111 Moderate High p = 0.003 10 p = 0.457 5 0 Mortality Morbidity RRT Figure 1 – In-hospital outcomes of morbidity, mortality and renal replacement therapy (RRT) by risk groups, according to the EuroSCORE. intermediate risk: R$ 16.115,00 ± R$ 7.381,00, and high risk: R$ 19.548,00 ± R$ 9.355,00, p < 0.001), being higher in higher risk categories. Still, regarding the AC, the low risk group (R$ 27.116,00 ± R$ 13.928,00) showed a significantly lower value than the other groups, and the intermediate risk group had a significantly lower value than the high group risk (R$ 34,854.00 ± R$ 27,814.00 & R$ 43.234,00 ± R$ 26.009,00 ± R) (Figure 2). However, when we analyze the risk groups for specific values of SUS reimbursement, we found some discrepancies not demonstrated in the total sample (Figure 3). In reimbursement for hospital services, even if the high-risk group had significantly higher value than the low and intermediate‑risk groups, the low‑risk group showed no significant difference in relation to the intermediate risk group. Similarly, in relation to reimbursement for professional services, the low-risk group showed no significant difference in relation to the intermediate-risk group, although there was a lower significant difference in relation to the high-risk group. In this item, the intermediate and high-risk groups were not significantly different. Similarly, on the reimbursement for the cost of materials, even if the high-risk group had significantly higher value than the low and intermediate-risk groups, the low risk group showed no significant difference in relation to the intermediate risk. Only in the reimbursement assessment for the ICU costs, the low-risk group had significantly lower value than the groups with intermediate and high risk, and the group with intermediate risk had a significantly lower value than the high-risk group. However, when we discriminately analyze the items established for the AC calculation (Figure 4), we can observe a significant difference as the risk increases by EuroSCORE. To confirm this, a logistic regression model was created for the SUS reimbursement value versus EuroSCORE (p < 0.0001): 11371 + 839.14*EuroSCORE It was also a model for the AC value versus EuroSCORE (p < 0.0001): 18831 + 2577.69*EuroSCORE Thus, with the estimates obtained from EuroSCORE (Table 3), the greater the patient risk, the greater the difference between the AC and the SUS reimbursement value. Discussion Being a reference only in simple procedures should not give credit to an institution that does not make any effort to treat critically-ill patients that need complex surgeries. With an aging population and increasing life expectancy13, a larger population of frail patients is referred for cardiovascular procedures and improved quality of life. Evidence shows that critical patients are those that benefit the most from cardiovascular procedures, even if they have higher cost and morbimortality risk14. This would explain why surgeons and hospitals that accept to operate more severe patients can have higher costs and greater morbimortality15,16. The use of risk scores allows the correction of the results according to patient severity for a more stringent cost-effectiveness analysis17. In Brazil, the most widely used risk model in cardiovascular surgery for outcome adjustment is the EuroSCORE18-22. Our study confirmed the direct association of the EuroSCORE with increased mortality and morbimortality. Arq Bras Cardiol. 2015; 105(2):130-138 133 Titinger et al. Cardiac surgery costs according to the risk Original Article 90000 p < 0.05 p < 0.05 80000 p < 0.05 70000 60000 p < 0.05 Low R$ 50000 p < 0.05 40000 p < 0.05 30000 Moderate High 20000 10000 0 Actual Cost SUS Reimbursement Figure 2 – Total value of actual costs and the Unified Health System (SUS) reimbursement for risk groups, according to EuroSCORE. p < 0.05 25.000,00 p < 0.05 20.000,00 19.548,19 16.217,49 13.305,69 15.000,00 R$ 3.463,34 3.415,11 2.518,95 2.278,78 10.000,00 p < 0.05 4.679,40 6.543,72 4.064,69 4.205,75 4.378,11 4.498,87 4.813,39 5.211,25 Low (n = 131) Moderate (n = 150) High (n = 104) 5.000,00 Materials ICU costs Prof Serv Hosp Serv Risk Figure 3 – Detailed values of the of the Unified Health System (SUS) reimbursement for cardiovascular procedures by risk groups, according to EuroSCORE. Materials: reimbursement for cost of materials (excluding drugs); ICU costs: reimbursement for the intensive care unit services; Prof Serv: reimbursement for professional services; Hosp Serv: reimbursement for hospital services. 134 Arq Bras Cardiol. 2015; 105(2):130-138 Titinger et al. Cardiac surgery costs according to the risk Original Article p < 0.05 60.000,00 p < 0.05 50.000,00 p < 0.05 43.234,33 R$ 40.000,00 30.000,00 20.000,00 10.000,00 34.854,16 23.819,97 27.115,63 19.065,86 Items Surgery Fees 13.944,62 3.386,62 3.441,44 ICU Daily Fee 9.370,58 Floor Daily Fee 3.244,73 4.403,53 6.418,15 5.522,75 6.002,94 6.602,34 Low (n = 131) Moderate (n = 150) High (n = 104) Risk Figure 4 – Detailed values of the actual costs for cardiovascular procedures by risk groups, according to the EuroSCORE. Items: Includes the actual value of the materials and drugs; ICU: Intensive care unit. Table 3 – Estimates obtained from the regression models for reimbursement by the Unified Health System (SUS) and the actual cost (AC), according to the EuroSCORE value. EuroSCORE SUS (R$) AC (R$) Difference (R$) 0 11371,00 18831,00 -7460,00 2 13049,28 23986,38 -10937,10 4 14727,56 29141,76 -14414,20 6 16405,84 34297,14 -17891,30 8 18084,12 39452,52 -21368,40 10 19762,40 44607,90 -24845,50 12 21440,68 49763,28 -28322,60 14 23118,96 54918,66 -31799,70 16 24797,24 60074,04 -35276,80 26475,52 65229,42 -38753,90 18 (R$) Values in Brazilian reais. SUS performs the majority of cardiovascular surgeries in Brazil, treating primarily patients with more unfavorable socioeconomic conditions. At InCor-HC/FMUSP, the number of cardiovascular surgeries by SUS corresponds to approximately 80% of the total. It is important to mention that the government allocates to the public health in Brazil a total of US$ 157.00 per inhabitant/year (I/Y). This is in sharp contrast with public health spending in Germany (US$ 3.521,00 I/Y), Canada (US$ 2.823,00 I/Y), United States (US$ 2.725,00 I/Y), Portugal (US$ 1,850,00 I/Y), Chile (US$ 720,00 I/Y), Argentina (US$ 380,00 I/Y) and Costa Rica (US$ 378,00 I/Y) 6. We know that the value of public spending in the US is an emblematic example of a system segmented for the poor (Medicaid), elderly (Medicare) and war veterans (about 66 million of inhabitants), while Brazil is the source of funding for approximately 160 million of inhabitants23. A publication on patients undergoing aortic valve replacement in the United States showed a direct correlation between the risk increase of patients and increased morbimortality and costs14. In Brazil, a study published by Instituto Dante Pazzanese de Cardiologia5 (Dante Pazzanese Institute of Cardiology) showed that the cost of coronary artery bypass surgery (primary, isolated and elective) is lower than Arq Bras Cardiol. 2015; 105(2):130-138 135 Titinger et al. Cardiac surgery costs according to the risk Original Article Study limitations the reimbursement supplied by SUS, showing that the mean cost of surgery was R$ 6.990,00 and the amount paid was R$ 5.551.41. These values are different from those found in our analysis, upon which the variety of procedures performed, including emergency care, the progressive worsening of the patients over time, and the current adjustment of costs and SUS reimbursement may have influenced. There are several limitations in this study. First, no follow‑up was performed for long-term analysis, although a recent study showed that, in a follow-up of five years after aortic valve replacement, there was a higher cost for high-risk patients24. Second, a multicenter analysis could have found differences related to specific patterns of SUS reimbursement between hospital categories. Third, the sample size may have influenced some analyses, especially among the categories of intermediate and high risk. Fourth, some risk factors, such as frailty, were excluded from the study. However, this could increase differences in the highrisk patient group25. This cost discrepancy has made university and philanthropic hospitals, and even private hospitals with social security-funded care suspend medical care due to accumulated debt. All this can worsen considering the global trend of increased high-risk patients referred to undergo cardiovascular procedures. In this study, it was shown that AC increases progressively when the preoperative risk of the patient increases. Although the SUS reimbursement also increases with the patient’s risk, it is disproportionate to the AC, and this increases as the patient’s risk increases. This scenario could influence the selection of patients operated in SUS-funded hospitals. Unquestionably, the ideal would be that SUS-funded hospitals be reimbursed by an amount equivalent to the AC. However, the minimum to be done is a reimbursement proportional to the AC. In the current context and for the same budget, that would be to pay less for low-risk surgeries and more for higher-risk surgeries, according to what we call risk adjusted reimbursement (Figure 5). Therefore, for each EuroSCORE unit increase, there will be a fairer amount to be reimbursed by SUS. In short, high-risk patients referred for cardiovascular surgery, in addition to the fact that they have higher cost, also show higher risk of morbimortality. Analyses in larger samples are needed to justify the cost-effectiveness of the procedures, to support SUS sustainability and funding, and improve the quality of outcomes and safety for patients. Conclusions Although the SUS reimbursement increases with the increase in patient risk, it is disproportionate to the real cost. Future directions in SUS reimbursement should be adopted so that care of an increasing number of high-risk surgical patients is not discouraged. Risk adjusted reimbursement 160000 140000 120000 R$ 100000 80000 y = 2538x + 18449 60000 40000 20000 0 y = 831.31x + 11246 0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 EuroSCORE SUS reimbursement Actual cost SUS Actual cost Risk adjusted reimbursement Figure 5 – Unified Health System (SUS) reimbursement increase, actual cost (AC) and risk adjusted reimbursement, according to the EuroSCORE value. 136 Arq Bras Cardiol. 2015; 105(2):130-138 Titinger et al. Cardiac surgery costs according to the risk Original Article Acknowledgments To FAFESP, for the limitless support in carrying out the present study. Lisboa LAF, Dallan LAO, Trindade EM, Kalil Filho R, Mejia OAV, Jatene FB. Potential Conflict of Interest Author contributions Conception and design of the research:Titinger DP, Trindade EM, Mejia OAV, Jatene FB. Acquisition of data:Titinger DP, Matrangolo BR, Eckl I, Mejia OAV. Analysis and interpretation of the data:Titinger DP, Lisboa LAF, Dallan LAO, Trindade EM, Mejia OAV. Statistical analysis: Titinger DP, Trindade EM, Mejia OAV, Jatene FB. Writing of the manuscript:Titinger DP, Lisboa LAF, Matrangolo BR, Dallan LRP, Dallan LAO, Mejia OAV. Critical revision of the manuscript for intellectual content: No potential conflict of interest relevant to this article was reported. Sources of Funding There were no external funding sources for this study. Study Association This study is not associated with any thesis or dissertation work. References 1. Pettersson GB, Martino D, Blackstone EH, Nowicki ER, Houghtaling PL, Sabik JF 3rd, et al. Advising complex patients who require complex heart operations. J Thorac Cardiovasc Surg. 2013;145(5):1159-69.e3. 14. Osnabrugge RL, Speir AM, Head SJ, Fonner CE, Fonner E Jr, Ailawadi G, et al. Costs for surgical aortic valve replacement according to preoperative risk categories. Ann Thorac Surg. 2013;96(2):500-6. 2. Engoren M, Arslanian-Engoren C, Steckel D, Neihardt J, Fenn-Buderer N. Cost, outcome, and functional status in octogenarians and septuagenarians after cardiac surgery. Chest. 2002;122(4):1309-15. 15. Clark MA, Duhay FG, Thompson AK, Keyes MJ, Svensson LG, Bonow RO, et al. Clinical and economic outcomes after surgical aortic valve replacement in Medicare patients. Risk Manag Healthc Policy. 2012;5:117–26. 3. Scott BH, Seifert FC, Grimson R, Glass PS. Octogenarians undergoing coronary artery bypass graft surgery: resource utilization, postoperative mortality, and morbidity. J Cardiothorac Vasc Anesth. 2005;19(5):583-8. 16. Bhamidipati CM, LaPar DJ, Fonner E Jr, Kern JA, Kron IL, Ailawadi G. Outcomes and cost of cardiac surgery in octogenarians is related to type of operation: a multiinstitutional analysis. Ann Thorac Surg. 2011;91(2):499-505. 4. 17. Smith CR, Leon MB, Mack MJ, Miller DC, Moses JW, Svensson LG, et al; PARTNER Trial Investigators. Transcatheter versus surgical aortic-valve replacement in high-risk patients. N Engl J Med. 2011;364(23):2187-98. Piegas LS, Bittar OJ, Haddad N. Myocardial revascularization surgery (MRS): results from national health system (SUS). Arq Bras Cardiol. 2009;93(5):555-60. 5. Haddad N, Bittar E, Marchi AF, Kantorowitz CS, Ayoub AC, Fonseca ML, et al. Hospital costs of coronary artery bypass grafting on elective coronary patients. Arq Bras Cardiol. 2007;88(94):418-23. 6. Gomes WJ, Mendonça JT, Braile DM. Cardiovascular surgery outcomes opportunity to rediscuss medical and cardiological care in the Brazilian public health system. Rev Bras Cir Cardiovasc. 2007;22(4):III-VI. 7. Kolh P, Wijns W. Essential messages from the ESC/EACTS guidelines on myocardial revascularization. Eur J Cardiothorac Surg. 2012;41(5):983-5. 18. Moraes F, Duarte C, Cardoso E, Tenório E, Pereira V, Lampreia D, et al. Assessment of the Euroscore as a predictor for mortality in myocardial revascularization surgery at the Heart Institute of Pernambuco. Rev Bras Cir Cardiovasc. 2006;21(1):29-34. 19. Sá MP, Soares EF, Santos CA, Figueredo OJ, Lima RO, Escobar RR, et al. EuroSCORE and mortality in coronary artery bypass graft surgery at Pernambuco Cardiologic Emergency Medical Services. Rev Bras Cir Cardiovasc. 2010;25(4):474-82. Mejía OA, Lisboa LA, Dallan LA, Pomerantzeff PM, Moreira LF, Jatene FB, et al. Validation of the 2000 Bernstein-Parsonnet and EuroSCORE at the Heart Institute – USP. Rev Bras Cir Cardiovasc. 2012;27(2):187-94. 20. Carvalho MRM, Silva NASe, Klein CH, Oliveira GMM. Aplicação do EuroSCORE na cirurgia de revascularização miocárdica em hospitais públicos do Rio de Janeiro. Rev Bras Cir Cardiovasc. 2010;25(2):209-17. 9. Nashef SA, Roques F, Michel P, Gauducheau E, Lemeshow S, Salamon R. European system for cardiac operative risk evaluation (EuroSCORE). Eur J Cardiothorac Surg. 1999;16(1):9-13. 21. Mejía OA, Lisboa LA, Puig LB, Dias RR, Dallan LA, Pomerantzeff PM, et al. The 2000 Bernstein-Parsonnet score and EuroSCORE are similar in predicting mortality at the Heart Institute, USP. Rev Bras Cir Cardiovasc. 2011;26(1):1-6. 8. 10. Smith MW, Barnett PG, Phibbs CS, Wagner TH. Microcost methods of determining VA healthcare costs. Menlo Park, CA: Health Economics Resource Center; 2010. 11. Weintraub WS, Karlsberg RP, Tcheng JE, Boris JR, Buxton AE, Dove JT, et al; American College of Cardiology Foundation; American Heart Association Task Force on Clinical Data Standards. ACCF/AHA 2011 key data elements and definitions of a base cardiovascular vocabulary for electronic health records: a report of the American College of Cardiology Foundation/ American Heart Association Task Force on Clinical Data Standards. Circulation. 2011;124(1):103-23. 12. Polsky D, Glick H. Costing and cost analysis in randomized controlled trials: caveat emptor. Pharmacoeconomics. 2009;27(3):179-88. 13. Global Population Estimates by Age, 1950-2050. [Access in 2014 Dec 24]. Available from: http://www.pewglobal.org/2014/01/30/global-population. 22. Lisboa LAF, Mejia OA, Moreira LF, Dallan LAO, Pomerantzeff PM, Dallan LR, et al. EuroSCORE II e a importância de um modelo local, InsCor e o futuro SP-SCORE. Rev Bras Cir Cardiovasc. 2014;29(1):1-8. 23. Mendes, EV. 25 anos do Sistema Único de Saúde: resultados e desafios. Estudos Avançados. 2013; 27(78): 27-34 24. Clark MA, Duhay FG, Thompson AK, Keyes MJ, Svensson LG, Bonow RO, et al. Clinical and economic outcomes after surgical aortic valve replacement in medicare patients. Risk Manag Healthc Policy. 2012;5:117-26. 25. Kappetein AP, Head SJ, Genereux P, Piazza N, van Mieghem NM, Blackstone EH, et al; Valve Academic Research Consortium (VARC)-2. Updated standardized endpoint definitions for transcatheter aortic valve implantation: the Valve Academic Research Consortium-2 consensus document (VARC-2). Eur J Cardiothorac Surg. 2012;42(5):S45-60. Arq Bras Cardiol. 2015; 105(2):130-138 137 Titinger et al. Cardiac surgery costs according to the risk Original Article 138 Arq Bras Cardiol. 2015; 105(2):130-138 Back to the Cover Original Article Screening for Fabry Disease in Left Ventricular Hypertrophy: Documentation of a Novel Mutation Ana Baptista, Pedro Magalhães, Sílvia Leão, Sofia Carvalho, Pedro Mateus, Ilídio Moreira Centro Hospitalar de Trás-os-Montes e Alto Douro, Unidade de Vila Real – Portugal Abstract Background: Fabry disease is a lysosomal storage disease caused by enzyme α-galactosidase A deficiency as a result of mutations in the GLA gene. Cardiac involvement is characterized by progressive left ventricular hypertrophy. Objective: To estimate the prevalence of Fabry disease in a population with left ventricular hypertrophy. Methods: The patients were assessed for the presence of left ventricular hypertrophy defined as a left ventricular mass index ≥ 96 g/m2 for women or ≥ 116 g/m2 for men. Severe aortic stenosis and arterial hypertension with mild left ventricular hypertrophy were exclusion criteria. All patients included were assessed for enzyme α-galactosidase A activity using dry spot testing. Genetic study was performed whenever the enzyme activity was decreased. Results: A total of 47 patients with a mean left ventricular mass index of 141.1 g/m2 (± 28.5; 99.2 to 228.5 g/m2] were included. Most of the patients were females (51.1%). Nine (19.1%) showed decreased α-galactosidase A activity, but only one positive genetic test − [GLA] c.785G>T; p.W262L (exon 5), a mutation not previously described in the literature. This clinical investigation was able to establish the association between the mutation and the clinical presentation. Conclusion: In a population of patients with left ventricular hypertrophy, we documented a Fabry disease prevalence of 2.1%. This novel case was defined in the sequence of a mutation of unknown meaning in the GLA gene with further pathogenicity study. Thus, this study permitted the definition of a novel causal mutation for Fabry disease – [GLA] c.785G>T; p.W262L (exon 5). (Arq Bras Cardiol. 2015; 105(2):139-144) Keywords: Fabry disease/complications; Hypertrophy, left ventricular; Alpha-Galactosidase/genetics. Introduction Establishing the cause of left ventricular hypertrophy (LVH) is a common challenge in clinical practice, given its high prevalence and the variety of diseases with which it may be associated. This is particularly relevant from the clinical standpoint because of the therapeutic implications regarding the different differential diagnoses. Fabry disease (FD) is a rare X-linked disease caused by enzyme α-Galactosidase A (Gal A) deficiency as a result of GLA gene mutations. Most families present with a “private” mutation found only in that family and, thus, hundreds of causal mutations are currently known. This multiplicity of mutations may contribute to variations in the residual enzyme activity and the different clinical presentations. Enzyme Gal-A deficiency leads to a progressive tissue accumulation of glycosphingolipids, especially of globotriaosylceramide (Gb3), resulting in organ failure. Mailing Address: Ana Baptista • CHTMAD. Avenida da Noruega, Vila Real. Postal Code 5000, Vila Real – Portugal E-mail: [email protected] Manuscript received November 17, 2014; revised manuscript March 27, 2015; accepted April 17, 2015. DOI: 10.5935/abc.20150090 139 The organs more frequently involved are the kidneys, heart, skin, central and autonomic nervous systems, eyes and auditory system. As regards the cardiac manifestations, Gb3 accumulation leads to LVH, whose etiology is difficult to distinguish from others using the common cardiac imaging methods, especially echocardiography. Currently, suspecting lysosomal storage diseases, namely FD, is key given the availability of enzyme replacement therapy, which brings an impact on disease progression. Thus, innumerable studies have been conducted to assess the prevalence of FD in risk populations. The objective of this study was to evaluate the prevalence of FD in a population of patients with LVH. Methods The study was conducted between October 2010 and February 2011 in a hospital center in the region of Tras‑os‑Montes and Alto Douro, northern Portugal, after approval of the Institutional Ethics Committee. All patients with age > 18 years referred for transthoracic echocardiography (TTE) were considered eligible for the FD screening program. They were included if there was evidence of LVH, defined as a left ventricular (LV) mass / body surface area (BSA) ≥ 96 g/m2, for women, and ≥ 116 g/m2, for men. LV mass was calculated using the formula: Baptista et al. Fabry disease – description of a novel mutation Original Article LV mass = 0.8 x (1.04 [(LV internal diameter + posterior wall + septum)3 – (LV internal diameter)3]) + 0.6 Linear measurements during diastole obtained from two‑dimensional echocardiography were used for the calculation. The exclusion criteria were presence of severe aortic stenosis and arterial hypertension when associated with mild LVH – LV mass/BSA < 109 g/m2 (women) and < 132 g/m2 (men), regardless of the hypertension stage. All patients enrolled gave written informed consent prior to undergoing clinical assessment, investigation of multiorgan involvement, and determination of enzyme Gal-A activity. Clinical assessment After the inclusion criteria were defined, brief history taking focused on the investigation of symptoms suggestive of FD and multiorgan involvement, especially cardiac, was performed. Thus, the questionnaire included the assessment of history of bouts of pain in extremities; gastrointestinal transit or sweating abnormalities; history of stroke; and presence of shortness of breath/orthopnea or chest pain. Next, blood pressure (BP), height and weight measurements were taken, and angiokeratomas were investigated. Clinical assessment did not include family history for cardiovascular or renal diseases. Investigation of multiorgan involvement The cardiac investigation was complemented by electrocardiogram (ECG) – assessment of rhythm, heart rate (HR), PR interval, conduction disturbances, and voltage criteria for LHV (Sokolow-Lyon criteria). For the investigation of renal involvement, BUN and serum creatinine levels were determined, with further estimate of the glomerular filtration rate (GFR) using the MDRD formula (Modification of Diet in Renal Disease). Random urine specimens were also collected to rule out albuminuria, using the microalbuminuria/urine creatinine ratio. Enzyme Gal-A activity determination Screening for FD was based on the dried blood spot (DBS) test, with four blood spots placed in a filter paper and allowed to dry at room temperature. Enzyme Gal-A activity was determined in an outside laboratory (laboratory of metabolism, Hamburg University Medical Center). Values between 200 and 2000 pmol/spot*20 h were considered normal. Genetic screening Whenever enzyme Gal-A activity was reduced, genetic screening was performed using 10 mL of blood collected in an EDTA tube with further GLA gene sequencing in the Center of Medical Genetics Doctor Jacinto de Magalhaes. Data were submitted to descriptive analysis using the Statistical Package for the Social Sciences (SPSS) program, version 19.0 (SPSS Statistics IBM®), and were expressed as numbers or percentages or mean values ± standard deviation (SD). 95% confidence intervals (95% CI) were used when applicable. Results During the study period, 75 patients had inclusion criteria; of these, 28 (37.3%) were excluded for showing arterial hypertension with mild LVH (21 patients), or severe aortic stenosis (7 patients). Screening for FD was then performed in 47 patients, of whom 24 were women (51.1%). The mean age of patients was 65.6 ± 14.5 years (ranging from 25 to 90 years). As regards their ventricular mass, the mean LV mass/BSA was 141.1 ± 28.5 g/m2 (99.2 to 228.5 g/m2) and the mean septal and posterior wall thickness was 15.3 ± 3.4 mm (10 to 24 mm) and 12.9 ± 2.1 mm (9 to 20 mm), respectively. Clinical characterization of the study population Most of the study population assessed had a known history of arterial hypertension (n = 35; 74.5%), with a mean systolic BP recorded on the day of assessment of 144.2 ± 30.3 mmHg (96 to 216 mmHg). The summary review of the clinical history suggested the presence of bouts of pain in the extremities in 27.7% of patients, sweating abnormalities in 4.3%, and gastrointestinal transit abnormalities in 29.8%. No skin lesions suggestive of angiokeratoma were found in any of the patients. Eight patients (17%) had history of stroke, 66% presented with dyspnea, and 40.4% with chest pain. Of the patients assessed, three (6.4%) were on a regular dialysis program, with the population showing a mean GFR of 81.7 ± 50.2 mL/min/1.73m2 (3.9 to 232.6 mL/min/1.73m2), as estimated from mean creatinine values of 1.4 ± 2.1 mg/dL (0.4 to 14.6 mg/dL). The prevalences of microalbuminuria and proteinuria were of 25.5% and 55.4%, respectively. Electrocardiographic assessment showed normal sinus rhythm in most of the patients (63.8%), with the remaining showing atrial fibrillation (19.1%) or pacemaker rhythm (17.1%). Their mean HR was 71 ± 15 bpm (45 to 110 bpm), PR interval of 169 ± 34 miliseconds (108 to 250 miliseconds), prevalence of atrioventricular and intraventricular conduction disturbance of 8.5% and 23.4%, respectively, with 40.4% of patients with criteria for LVH. Nine patients, all females, showed reduced enzyme Gal-A activity (19.1%), and were therefore referred for genetic screening. Only one of the genetic studies was able to document a GLA gene mutation. Thus, the incidence of false positives using the enzymatic test with DBS was 88.9%. Description of the case showing GLA gene mutation The single positive genetic test showed heterozygosis for [GLA] c.785G>T; p.W262L (exon 5) mutation, which had never been previously described in the literature as the cause of FD. The patient was a 46-year-old female recently diagnosed with arterial hypertension, who had been referred for TTE because of a brain stem stroke. In the clinical assessment, she had history of frequent episodes of bouts of pain in the extremities, especially in hands, and gastrointestinal transit abnormalities, but no angiokeratoma. The ECG revealed normal sinus rhythm, HR of 76 bpm and voltage criteria for LVH with an overload pattern. The echocardiogram showed moderate concentric LVH with grade-II diastolic dysfunction. Renal assessment revealed the presence of microalbuminuria with preserved renal function (creatinine level of 0.6 mg/dL). Arq Bras Cardiol. 2015; 105(2):139-144 140 Baptista et al. Fabry disease – description of a novel mutation Original Article Although the manifestations were suggestive of FD (microalbuminuria and LVH), they could also be explained by the history of hypertension and, therefore, the pathogenicity of this novel mutation had to be documented. This process involved three key steps: genetic information, demonstration of accumulation of Gb3 deposits, and family screening. Regarding the study of the mutation, the bioinformatics tools showed that it was causal, and the hypothesis of polymorphism was ruled out when it was not found in the study of 100 individuals from the population. Another aspect corroborating causality was the fact that other causal mutations had already been described in its proximity1,2. Tissue accumulation of Gb3 was demonstrated by cutaneous biopsy, which showed rare lysosomal inclusions with characteristics typical of Gb3 deposits in smooth muscle fibers and increased blood concentrations of lysoGb3. As regards the family study (Figure 1), it was negative for all her siblings, but positive for her daughter, who, at the age of 30 years, also presented with manifestations suggestive of FD: cornea verticilatta, peripheral neuropathic pain, and slightly increased proteins in the 24-hour urine, thus confirming the association of the mutation with the manifestations suggestive of FD. The investigation also included ruling out the involvement of other organs not defined by the study algorithm (dermatological, ophthalmological, ENT and pulmonary assessments were normal) and additional characterization by MRI of cardiac involvement, which demonstrated LVH with no late enhancement, and brain involvement, which demonstrated white matter damage. Blood pressure was also documented by ambulatory BP monitoring under medication. Thus, in a study on FD screening in patients with LVH, one case of FD was documented in association with a causal mutation – [GLA] c.785G>T; p.W262L (exon 5), which had not been previously described in the literature and is associated with 80 years (?) XY (?) X– Y 40 years (Accident) X– Y Figure 1 – Family tree. 141 Arq Bras Cardiol. 2015; 105(2):139-144 Discussion In a population of patients with LVH, after exclusion of cases with severe aortic stenosis and arterial hypertension associated with mild LVH, we documented a FD prevalence of 2.1% (95%CI: 0.1-11.3%). This prevalence is similar to that found in other screening studies in high-risk populations (populations selected with LVH, stroke and patients undergoing dialysis)3, which reported prevalence rates much higher than that estimated in the general population of 0.02 to 0.09 per 10 thousand individuals4. However, the prevalence found should be carefully interpreted taking into consideration the small number of patients analyzed in this study. The importance of screening studies lies on two major factors. First, they seek to increase awareness on FD in target groups, in which there is a higher probability of detecting cases, and thus contribute for the definition of disease prevalence. Second, these studies also provide the opportunity to detect the disease at earlier stages, at which enzyme replacement therapy is more effective. The available studies on the prevalence of FD in populations with LVH used different criteria for patient inclusion, whether because of different forms of assessing LVH, or because of the cutoff values defined. Most of the studies used the maximum ventricular wall thickness threshold of 13 or 15mm4 as an inclusion criterion, unlike in the present study, in which patient selection was based on the ventricular mass index. Although the typical manifestation of the cardiac involvement in FD is concentric LVH, several cases of asymmetrical LVH have already been documented5. To corroborate this fact, there are studies demonstrating a FD incidence of approximately 1.0% 82 years (stroke) XX (?) X– Y X– X– neurological, cardiac and renal involvement. The Organizing Committee of Treatment of Lysosomal Storage Disorders approved enzyme replacement therapy for the patient. X– X– 49 years X+ X– 30 years X+ X– Baptista et al. Fabry disease – description of a novel mutation Original Article in populations diagnosed with hypertrophic cardiomyopathy6, in which asymmetrical LVH is the most frequent form of presentation. Thus, in the present study, patients with possible FD may have been excluded because increased thickness of a single ventricular wall – usually the ventricular septum, may be not associated with increased LV mass. However, this variable –left ventricular mass index, is one of the main criteria for monitoring the effectiveness of enzyme replacement therapy in the reduction of LVH7, and this is why it was used as a criterion for patient selection. In this study, enzyme Gal-A activity as assessed by DBS was the method used for FD screening, whose result may be normal in up to 40% of women with FD8. Interpretation of the enzymatic assay is more complicated in females, because the enzyme activity may be normal or at borderline lower limits because of the phenomenon of X-chromosome inactivation (i.e., the permanent epigenetical silencing of one X chromosome creating cellular mosaicism, which explains the disease presentation in women – of delayed onset and with a higher probability of a singleorgan involvement)9. This leads to a study limitation: the possibility of underestimating FD prevalence because of false negatives among women although, interestingly, the only positive result occurred in a female patient. The use of the DBS test was based on the fact that it is an easily-accessible screening method in the clinical practice and has advantages over enzyme activity assessment in leukocytes or fibroblasts. First, it requires only a few blood spots for dose determination and, second, it permits easy and quick specimen shipping to specialized laboratories, an important aspect in our study center, where there is no laboratory dedicated to lysosomal storage diseases. Thus, we were interested in analyzing the DBS behavior to determine its further inclusion in the assessment of female patients with suspected FD. In addition to the known false negatives – a reality for which clinicians are aware of, given documentation from multiple studies, as previously mentioned, this screening showed another limitation of the DBS test: a high incidence of false positives, which has been infrequently reported in studies10. Only one in nine of the patients with reduced enzyme activity (all females) had FD confirmed by genetic testing, thus resulting in 88.9% of false positives. Therefore, in the current scenario in which costs are weighted in clinical investigation, this study questions the usefulness of DBS in female patients with suspected FD (high rate of false negatives and false positives). We observed a low incidence of unspecific manifestations, namely sweating disorders; however, gastrointestinal abnormalities and bouts of pain had an incidence of approximately 30%. This is probably explained by the fact that these are common manifestations of more prevalent diseases such as musculoskeletal and digestive disorders. On the other hand, manifestations of possible multiorgan involvement such as albuminuria had a high incidence, since they are also possible manifestations of hypertensive disease – a common finding in the study population. The assessment of these clinical and laboratory factors, which are common manifestations of FD, is a distinguishing feature of this study. Its inclusion in the screening study, unlike the usual genetic study alone in risk populations, was motivated by the interest in the definition of associations of factors with a higher probability of FD. Thus, the study results could be applied to the clinical practice, such as in the integration of findings in algorithms of etiologic studies on LVH. This way, we could limit genetic studies to certain groups selected according to criteria corroborated by a clinical trial. However, this was not possible because the sample size and the low incidence of FD limited the study power to draw conclusions on the improvement of pre-test probability. These findings were ultimately useful in the assessment of the significance of de novo mutations, as explained bellow. To date, more than 600 GLA gene variants have been described and most of them is unique for each family. However, as more studies on FD screening started to be conducted, an unexpected high number of individuals with mutations of unknown significance was observed, with a prevalence rate estimated at 0.6% in high-risk populations, although only 0.12% have typical clinical manifestations or decreased enzyme activity11. Thus, the significance of these mutations is not easy to define, because many of the screening studies involve high-risk populations that express one single specific symptom – the inclusion criteria, LVH in the case of this study and, thus, the symptom may be not related to the GLA gene variant detected or may be an FD manifestation in its non-classic form. In this study on FD screening in a predominantly hypertensive population (74.5%) with LVH, this became a clear issue. We found a GLA gene mutation not previously described in the literature - [GLA] c.785G>T; p.W262L (exon 5), whose significance could not be defined based on the finding of LVH on TTE. The patient had been diagnosed with hypertension and, thus, the LVH findings along with the presence of microalbuminuria and history of stroke could be explained either by FD or by arterial hypertension with target-organ involvement, given that the manifestations can overlap in both situations. This led to a clinical investigation focused on proving the pathogenicity associated with the mutation, which involved three key steps: bioinformatics techniques, histological diagnosis, and family screening. The assessment of the occasional pathogenicity of the mutation involved the documentation of its absence in the study of 100 chromosomes of individuals from the general population, thus excluding the hypothesis of polymorphism. Then, we proceeded to a literature review in the search for mutations described in its proximity, which also increases the probability of pathogenicity, and found the p. W262C (c.786G>C) mutation documented by Schafer et al.12, and the p. W262X (c.785G>A) mutation described by Shabbeer et al.13. The use of bioinformatics tools defined the mutation as causal. We used the PolyPhen-2® (Polymorphism Phenotyping v2) program, which predicts the possible impact of the replacement of one amino acid on the structure and function of human proteins (Figure 2). Accumulation of Gb3 deposits – histological diagnosis of FD, was demonstrated by cutaneous biopsy, which showed sparse lysosomal inclusions with characteristics typical of Gb3 deposits exclusively in smooth muscle fibers thus corroborating the relationship between genotype and phenotype. The process was concluded with family screening focused on confirming the association of Arq Bras Cardiol. 2015; 105(2):139-144 142 Baptista et al. Fabry disease – description of a novel mutation Original Article PolyPhen-2 report for P06280 W262L Query Protein Acc P06280 Position 262 AA1 AA2 W L Descrição Canonical; RecName: Full=Alphagalactosidase A; EC=3.2.1.22; AltName: Full=Alpha-D-galactosidase A; AltName: Full=Alpha-Dgalactoside galactohydrolase; AltName: Full=Melibiase; AltName: INN=Agalsidase; Flags: Precursor; Length: 429 Results Prediction/Confidence PolyPhen-2 v2.2.2r398 HumDiv This mutation is predicted to be PROBABLY DAMAGING (sensitivity: 0.00; specificity: 1.00) 0.00 0.20 0.40 0.60 With a score of 1.000 0.80 1.00 HumDiv Details Multiple sequence alignment UniProt/UniRef 2011-12 (14-dez-2011) 3D Visualization PDB/DSSP Snapshot 03-Jan-2012 (78304 Structures) Figure 2 – Use of bioinformatics tools to estimate the causality of the mutation. the mutation with clinical manifestations in multiple patients. Documentation of the mutation in a normotensive first-degree relative (daughter) associated with early manifestations of FD (cornea verticillata, peripheral neuropathic pain, and increased 24-hour urine proteins) also helped to establish a causal relationship between the mutation found - [GLA] c.785G>T; p.W262L (exon 5), and FD. Conclusions In a population of patients with left ventricular hypertrophy, after exclusion of severe aortic stenosis and arterial hypertension associated with mild left ventricular hypertrophy, we documented a Fabry disease prevalence of 2.1%. This stresses the importance of including this disease among the differential diagnoses of left ventricular hypertrophy. This screening study also documented an issue regarding these research methods that is not related to Fabry disease – the occurrence of a mutation of unknown significance in GLA gene, and showed the clinical management required to define the role of the mutation on the development of the clinical presentation. Thus, this study 143 Arq Bras Cardiol. 2015; 105(2):139-144 allowed the definition of a novel causal mutation for Fabry disease – [GLA] c.785G>T; p.W262L (exon 5). Author contributions Conception and design of the research and Writing of the manuscript: Baptista A, Mateus P; Acquisition of data and Critical revision of the manuscript for intellectual content: Baptista A, Magalhães P, Leão S, Carvalho S, Mateus P; Analysis and interpretation of the data: Baptista A, Magalhães P; Statistical analysis: Baptista A, Leão S. Potential Conflict of Interest No potential conflict of interest relevant to this article was reported. Sources of Funding There were no external funding sources for this study. Study Association This study is not associated with any thesis or dissertation work. Baptista et al. Fabry disease – description of a novel mutation Original Article References 1. Schäfer E, Baron K, Widmer U, Deegan P, Neumann HP, Sunder-Plassmann G, et al. Thirty-four novel mutations of the GLA gene in 121 patients with Fabry disease. Hum Mutat. 2005;25(4):412. 2. Shabbeer J, Yasuda M, Benson SD, Desnick RJ. Fabry disease: Identification of 50 novel α-galactosidase A mutations causing the classic phenotype and three-dimensional structural analysis of 29 missense mutations. Hum Genomics. 2006;2(5):297-309. 7. Anderson LJ, Wyatt KM, Henley W, Nikolaou V, Waldek S, Hughes DA, et al. Long-term effectiveness of enzyme replacement therapy in Fabry disease: results from the NCS-LSD cohort study. J Inherit Metab Dis. 2014;37(6):969-78. 8. Linthorst GE, Vedder AC, Aerts JM, Hollak CE. Screening for Fabry disease using whole blood spots fails to identify one-third of female carriers. Clin Chim Acta. 2005;353(1-2):201-3. Linthorst GE, Bouwman MG, Wijburg FA, Aerts JM, Poorthuis BJ, Hollak CE. Screening for Fabry disease in high-risk populations: a systematic review. J Med Genet. 2010;47(4):217-22. 9. Yousef Z, Elliott PM, Cecchi F, Escoubet B, Linhart A, Monserrat L, et al. Left ventricular hypertrophy in Fabry disease: a practical approach to diagnosis. Eur Heart J. 2013;34(11):802-8. 4. Terryn W, Deschoenmakere G, Keyser JD, Meersseman W, Van Biesen W, Wuyts B, et al. Prevalence of Fabry disease in a predominantly hypertensive population with left ventricular hypertrophy. Int J Cardiol. 2013;167(6):2555-60. 10. Caudron E, Germain DP, Prognon P. [Fabry disease: enzymatic screening using dried blood spots on filter paper]. Rev Med Interne. 2010;31 Suppl2:S263-9. 3. 5. Elliott P, Baker R, Pasquale F, Quarta G, Ebrahim H, Mehta AB, et al. Prevalence of Anderson-Fabry disease in patients with hypertrophic cardiomyopathy: the European Anderson-Fabry Disease Survey. Heart. 2011;97(23):1957-60. 6. H a g è g e A A , C a u d r o n E , D a m y T, R o u d a u t R , M i l l a i r e A , Etchecopar‑Chevreuil C, et al; FOCUS study investigators. Screening patients with hypertrophic cardiomyopathy for Fabry disease using a filter‑paper test: the FOCUS study. Heart. 2011;97(2):131-6. 11. Tol LV, Smid BE, Poorthuis JH, Biegstraaten M, Deprez RH, Linthorst GE, et al. A systematic review on screening for Fabry disease: prevalence of individuals with genetic variants of unknown significance. J Med Genet. 2014;51(1):1-9. 12. Schäfer E, Baron K, Widmer U, Deegan P, Neumann HP, Sunder-Plassmann G, et al. Thirty-four novel mutations of the GLA gene in 121 patients with Fabry disease. Hum Mutat. 2005;25(4):412. 13. Shabbeer J, Yasuda M, Benson SD, Desnick RJ. Fabry disease: identification of 50 novel alpha-galactosidase A mutations causing the classic phenotype and three-dimensional structural analysis of 29 missense mutations. Hum Genomics. 2006;2(5):297-309. Arq Bras Cardiol. 2015; 105(2):139-144 144 Back to the Cover Original Article Heart Failure with Preserved Left Ventricular Ejection Fraction in Patients with Acute Myocardial Infarction Lucas Antonelli, Marcelo Katz, Fernando Bacal, Marcia Regina Pinho Makdisse, Alessandra Graça Correa, Carolina Pereira, Marcelo Franken, Anderson Nunes Fava, Carlos Vicente Serrano Junior, Antonio Eduardo Pereira Pesaro Hospital Israelita Albert Einstein (HIAE), São Paulo, SP – Brazil Abstract Background: The prevalence and clinical outcomes of heart failure with preserved left ventricular ejection fraction after acute myocardial infarction have not been well elucidated. Objective: To analyze the prevalence of heart failure with preserved left ventricular ejection fraction in acute myocardial infarction and its association with mortality. Methods: Patients with acute myocardial infarction (n = 1,474) were prospectively included. Patients without heart failure (Killip score = 1), with heart failure with preserved left ventricular ejection fraction (Killip score > 1 and left ventricle ejection fraction ≥ 50%), and with systolic dysfunction (Killip score > 1 and left ventricle ejection fraction < 50%) on admission were compared. The association between systolic dysfunction with preserved left ventricular ejection fraction and in-hospital mortality was tested in adjusted models. Results: Among the patients included, 1,256 (85.2%) were admitted without heart failure (72% men, 67 ± 15 years), 78 (5.3%) with heart failure with preserved left ventricular ejection fraction (59% men, 76 ± 14 years), and 140 (9.5%) with systolic dysfunction (69% men, 76 ± 14 years), with mortality rates of 4.3%, 17.9%, and 27.1%, respectively (p < 0.001). Logistic regression (adjusted for sex, age, troponin, diabetes, and body mass index) demonstrated that heart failure with preserved left ventricular ejection fraction (OR 2.91; 95% CI 1.35–6.27; p = 0.006) and systolic dysfunction (OR 5.38; 95% CI 3.10 to 9.32; p < 0.001) were associated with in-hospital mortality. Conclusion: One-third of patients with acute myocardial infarction admitted with heart failure had preserved left ventricular ejection fraction. Although this subgroup exhibited more favorable outcomes than those with systolic dysfunction, this condition presented a three-fold higher risk of death than the group without heart failure. Patients with acute myocardial infarction and heart failure with preserved left ventricular ejection fraction encounter elevated short-term risk and require special attention and monitoring during hospitalization. (Arq Bras Cardiol. 2015; 105(2):145-150) Keywords: Heart Failure; Myocardial Infarction; Stroke Volume; Prevalence. Introduction Diastolic heart failure (HF) is a clinical syndrome defined by the presence of signs and symptoms of HF, preserved left ventricle ejection fraction (LVEF), and abnormal diastolic function1. It is characterized by an abnormality in ventricular distensibility, relaxation, and filling, all of which can be indirectly measured by echocardiography2. In the absence of echocardiographic assessment of diastolic function, HF with LVEF ≥ 50% can be termed only “HF with preserved LVEF.” Although patients with HF with preserved LVEF generally present a more favorable prognosis than those with systolic dysfunction, there is increasing morbidity related to HF with preserved LVEF due to population aging and therapeutic limitations associated with this pathology. Mailing Address: Antonio Eduardo Pereira Pesaro • Hospital Israelita Albert Einstein. Avenida Albert Einstein, 627/701, Pavilhão Vicky e Joseph Safra, Bloco A1, 4º andar, Postal Code 05652‑901, São Paulo, SP - Brazil. E-mail: [email protected]. Manuscript received November 18, 2014; revised manuscript February 20, 2015; accepted March 4, 2015 DOI: 10.5935/abc.20150055 145 In particular, systolic dysfunction is an important marker of poor prognosis in acute myocardial infarction (AMI)3,4. Conversely, the presence of diastolic dysfunction, whether associated with systolic dysfunction, is an aggravating factor that is associated with poor prognosis in this situation5,6. Previous studies have suggested that the development of HF after AMI is related to the infarction size, coronary multivessel disease, reperfusion efficiency, and adjuvant medication use 7-9. Despite the increasing use of early myocardial revascularization8, the prevalence of post-AMI HF is still high (20%–30%), representing the leading cause of in-hospital mortality6,10. Systolic ventricular dysfunction after AMI in relation to the development of HF and increased mortality has been extensively studied. Moreover, data relating to the prevalence and prognosis of patients with post-AMI HF with preserved LVEF are still limited11. A few registries have specifically evaluated post-AMI HF with preserved LVEF; however, they generally have not simultaneously assessed AMI patients with and without ST-segment elevation (STEMI and NSTEMI, respectively) and have used heterogenous LVEF cut-off points to establish the diagnosis of HF with preserved LVEF12-14. Here we aim to evaluate the prevalence, clinical Antonelli et al. Diastolic heart failure in myocardial infarction Original Article characteristics, and clinical outcomes of patients admitted with post-AMI HF with preserved LVEF. Methods Between January 2005 and December 2012, 1,474 patients with AMI (71% men, 73 ± 14 years, 39% with STEMI) were consecutively included in a single-center registry of a tertiary hospital. Details regarding the registry design, methods, and quality control have been previously published15. AMI was defined according to the criteria set by international guidelines16. LVEF was measured throughout hospitalization at the discretion of the healthcare team. For this analysis, the worst LVEF of each patient during hospitalization was selected. Baseline clinical characteristics and in-hospital outcomes (length of stay and inhospital mortality) were compared among the three groups of patients: those without HF at admission (Killip score = 1), those with HF with preserved LVEF at admission (Killip score > 1 and LVEF ≥ 50%), and those with systolic dysfunction at admission (Killip score > 1 and LVEF < 50%). The diagnosis of AMI and all decisions regarding the treatment administered were made by the responsible medical team based on the institution’s current guidelines and routine practices. Specific nursing staff was assigned to collect all the variables included in this registry. The Research Ethics Committee of Hospital Israelita Albert Einstein approved the present study. Statistical analyses The numerical variables with normal distribution were expressed as mean ± standard deviation or as median and interquartile range when the distribution was not normal. Categorical variables were presented as absolute and relative frequencies. The comparison between numerical variables was performed using analysis of variance or the Kruskal–Wallis test, followed by the Bonferroni–Dunn multiple comparisons test, when required. The chi-squared test was used for categorical variables; Bonferroni multiple comparisons via generalized linear models with logit link function were used when the differences between the groups were significant. A logistic regression model adjusted for sex, age, troponin, diabetes mellitus, body mass index, type of AMI, and history of prior stroke/transient ischemic attack was used to test the association between HF and in-hospital mortality. A p-value < 0.05 was considered to be statistically significant. All statistical analyses were performed using STATA 11 Special Edition (Stata Corp LP, College Station, Texas, United States). Results Among the 1,474 patients included in the study, 1,256 (85.2%) did not have HF (72% men, 67 ± 15 years), 78 (5.3%) had HF with preserved LVEF (59% men, 76 ± 14 years), and 140 (9.5%) had systolic HF (69% men, 76 ± 14 years). The baseline clinical characteristics of the three groups are shown in Table 1. It was observed that HF patients with preserved LVEF and those with systolic HF were older and had higher risk for thrombolysis in myocardial infarction (TIMI) than patients without HF. Compared with patients with systolic HF, HF patients with preserved LVEF had higher LVEF and often exhibited NSTEMI. Patients without HF, with HF with preserved LVEF, and with systolic HF presented mortality rates of 4.3%, 17.9%, and 27.1%, respectively (p < 0.001), and hospital stay (standard deviation) of 6 (5), 9 (14), and 10 (12.5) days, respectively (p < 0.001). Logistic regression revealed that HF with preserved LVEF [odds ratio (OR) = 2.91, 95% confidence interval (95% CI) 1.35–6.27, p = 0.006] and systolic dysfunction (OR = 5.38, 95% CI 3.10–9.32, p < 0.001) were notably and independently associated with in-hospital mortality (Table 2). Discussion One-third of patients with AMI who had HF at admission presented preserved LVEF (≥ 50%). Nevertheless, this subgroup had an extended hospital stay and an almost three-fold higher risk of in-hospital death than those without HF. Patients admitted with systolic HF exhibited even higher mortality rates, with a five-fold greater risk of in-hospital death when compared with patients without HF. Diastolic HF is a clinical syndrome characterized by the presence of signs and symptoms of HF, preserved LVEF, and abnormal diastolic function. The pathophysiology of diastolic HF comprises ventricular relaxation deficit and intraventricular pressure increase, with a consequent increase in pulmonary capillary wedge pressure1. In general, post-AMI HF is a result of complex and unbalanced structural, hemodynamic, and neurohumoral interactions17. Ischemia and myocardial necrosis promote systolic and diastolic contractile dysfunction because ventricular diastole is an active physiological process that consumes oxygen and glucose18. Even without extensive necrosis, a stunned or hibernating myocardium also presents contractile and relaxation dysfunction, although this may be transitory19. Echocardiographic assessment of diastolic function and filling pressures requires careful data acquisition and proper interpretation by the operating technician. Decreases in the magnitude of the early to late diastolic filling ratio, increases in the deceleration time of early diastolic filling, or increases in the isovolumetric relaxation time indicate worsened ventricular relaxation19. These echocardiographic parameters can aid in diagnosis and assessment of the severity of diastolic dysfunction. A 2007 European consensus suggested that, in addition to the clinical characteristics of HF and LVEF, echocardiographic parameters such as ventricular filling time, diastolic volume, and ventricular mass should be included among the diagnostic criteria for diastolic HF20. Data on these parameters were not available in our registry; nevertheless, as in the present study, the majority of clinical studies on post-AMI diastolic dysfunction have used only clinical HF associated with preserved LVEF to establish the diagnosis12,21. In patients with acute coronary syndromes (ACS), the presence of HF is an important marker for risk of death. Stege et al. evaluated the characteristics and prognosis of post-ACS HF based on the GRACE registry13. They observed a 2.2-fold higher risk of death for patients with HF than those without HF. Notably, the GRACE registry did not differentiate according to patients the type of HF (systolic or diastolic) but classified them only based on the Killip score at admission. In addition, patients with Killip class IV AMI were excluded Arq Bras Cardiol. 2015; 105(2):145-150 146 Antonelli et al. Diastolic heart failure in myocardial infarction Original Article Table 1 – Clinical characteristics of the three groups of patients Without HF (n = 1,256) HF with preserved LVEF (n = 78) Systolic HF (n = 140) p-value Male, n (%) 910 (72) 46 (59) 96 (69) 0,028* Age (±SD) 67 ± 15**,*** 76 ± 14**** 76 ± 14**** < 0,001 BMI (kg/m²) (±SD) 27 ± 4*** 26 ± 5**** 26 ± 5**** 0,015 Diabetes, n (%) 370 (30) 30 (39) 50 (36) 0,130 SAH, n (%) 700 (58) 52 (67) 86 (63) 0,157 Stroke/TIA, n (%) Previous AMI, n (%) LVEF (±SD) TIMI risk (P25/P75) Troponin ng/mL (P25/P75) NSTEMI, n (%) 48 (4)*** 4 (5) 15 (11)**** 0,005 195 (16)*** 8 (11) 31 (23)**** 0,050 0,54 ± 0,12**,*** 0,59 ±0,07***,**** 0,34 ±0,09**,**** < 0,001 2 (1/4)**,*** 3 (2/6)**** 4 (3/6,75)**** < 0,001 3.460 (580/16.100) 3.160 (450/21.200) 3.300 (420/21.500) 0,940 790 (63)*** 47 (60)*** 60 (43)**,**** < 0.001 * It was not possible to identify the groups in which the differences occurred. ** Statistically significant differences compared with HF patients with preserved LVEF. *** Statistically significant differences compared with systolic HF patients. **** Statistically significant differences compared with patients without HF. HF: Heart failure. LVEF: Left ventricular ejection fraction. SD: Standard deviation. BMI: Body mass index. SAH: Systemic arterial hypertension. TIA: Transient ischemic attack. AMI: Acute myocardial infarction. TIMI: Thrombolysis in myocardial infarction. NSTEMI: Acute myocardial infarction without ST-segment elevation. Table 2 – Multivariate logistic regression Variable OR HF with preserved LVEF 95% CI p-value Lowest Highest 2,91 1,35 6,27 0,006 Systolic HF 5,38 3,10 9,32 < 0,001 Age (years) 1,02 1,01 1,03 0,003 BMI (kg/m²) 0,84 0,81 0,88 < 0,001 Female sex 1,44 0,87 2,41 0,160 Diabetes 0,88 0,53 1,45 0,615 Previous AMI 0,80 0,42 1,50 0,482 Previous stroke/TIA 2,02 0,91 4,48 0,085 Troponin 1,00 1,00 1,00 0,996 NSTEMI 0,66 0,40 1,07 0,092 OR: Odds ratio. 95% CI: 95% confidence interval. HF: heart failure. LVEF: Left ventricular ejection fraction. BMI: Body mass index. AMI: Acute myocardial infarction. TIA: Transient ischemic attack. NSTEMI: Acute myocardial infarction without ST-segment elevation. from the analysis, which may justify the lower mortality in these patients compared with the results of our or other registries14,22. Conversely, the data available on diastolic dysfunction in patients with ACS are highly limited. Patients with ACS and HF often have preserved LVEF; nevertheless, most clinical studies have only analyzed the outcomes of patients with systolic HF. Recently, an epidemiological study demonstrated that, despite the prevalence of post-AMI systolic HF declining over the past two decades, prevalence for HF with preserved LVEF has remained 147 Arq Bras Cardiol. 2015; 105(2):145-150 stable, reaching a rate comparable with systolic HF23. In general, patients with HF with preserved LVEF are majorly women, the elderly, hypertensive individuals, and those with lower prevalence of diabetes mellitus compared with patients with post-ACS systolic HF12. In the present study, compared with patients without HF, patients with systolic HF or HF with preserved LVEF were older and had a higher risk of AMI, as assessed by the TIMI score. Compared with patients with systolic HF, HF patients with preserved LVEF had higher LVEF and often exhibited NSTEMI. Antonelli et al. Diastolic heart failure in myocardial infarction Original Article In relation to clinical outcomes, some studies have shown that patients with post-AMI HF and preserved LVEF had higher risk of mortality compared with patients without HF, despite not exhibiting systolic dysfunction. Bennett et al. found results similar to the present study in the CRUSADE registry, specifically in patients with NSTEMI12. In that registry, over half the patients with post‑AMI HF had preserved LVEF. However, the cut-off point used to determine preserved LVEF was 40%. Therefore, patients with mild systolic ventricular dysfunction were considered to have diastolic HF, which may have worsened the prognosis of this subset of patients. Nevertheless, in the CRUSADE registry, mortality in patients with HF with preserved LVEF was lower than that in patients with systolic dysfunction12. Similarly to the present study, this rate was more than twice the rate in patients without HF. In the same registry, this behavior was also observed in the short- and long-term sub-analysis in patients aged over 65 years 24. Notably, the CRUSADE registry did not include patients with STEMI, who represented 40% of HF patients with preserved LVEF in the study. Subsequently, Kim et al.22 assessed predictors of death including NT-proBNP in 555 patients with AMI and preserved LVEF. Age and NT-proBNP were independent predictors of cardiovascular mortality and rehospitalization for HF. Recently, in a large registry (ACTION) analyzed by Shah et al.,21 3.8% of patients with AMI admitted without HF developed HF during hospitalization. In this subgroup, 35% of patients exhibited NSTEMI and 22% of those exhibiting STEMI developed HF with LVEF ≥ 50%. Despite mortality in patients with post-AMI HF being approximately five times greater than in those without HF, they did not observe differences in mortality between patients with systolic HF and those with HF with preserved LVEF. However, the study suggested that preserved LVEF and absence of HF at admission did not guarantee that patients with AMI were free from the risk of developing HF during hospitalization. The present study had several limitations because this was a retrospective, observational, single-center study with a relatively small population sample. Data on the patients’ Killip score throughout hospitalization was not available but only that upon admission was available; therefore, this study did not include cases of HF that developed during hospitalization. Echocardiographic measurements related to diastolic function other than the LVEF score were also not available in the present registry. Finally, complete data on the medical and interventional treatment of the patients were not available, and as a result, statistical adjustments related to therapeutic aspects were not possible. Thus, although post-AMI HF with preserved LVEF is moderately prevalent and presents important prognostic implications, few studies have specifically evaluated the clinical outcomes and therapeutic needs of this subgroup of patients. Despite its limitations, the objective of this study was to describe the clinical features, prevalence, and prognosis of patients with systolic HF or HF with preserved LVEF following AMI. Conclusion One-third of patients with AMI with HF at admission presented preserved LVEF. Although outcomes for this subgroup were more favorable than those for the patients with systolic HF, the former had longer hospital stays and a three-fold higher risk of death than the patients without HF. Therefore, HF patients with preserved LVEF after AMI are a subgroup encountering a short-term risk and require special attention and monitoring during hospitalization. Acknowledgements The authors would like to thank Rogério Ruscitto Prado for his support in the statistical analyses. Author contributions Conception and design of the research:Antonelli L, Katz M, Bacal F, Makdisse MRP, Correa AG, Pereira C, Franken M, Fava AN, Serrano Junior CV, Pesaro AEP. Acquisition of data:Antonelli L, Fava AN, Pesaro AEP. Analysis and interpretation of the data: Antonelli L, Katz M, Pesaro AEP. Statistical analysis: Antonelli L, Katz M, Pesaro AEP. Writing of the manuscript:Antonelli L, Katz M, Bacal F, Makdisse MRP, Correa AG, Pereira C, Franken M, Serrano Junior CV, Pesaro AEP. Critical revision of the manuscript for intellectual content: Antonelli L, Katz M, Bacal F, Makdisse MRP, Correa AG, Pereira C, Franken M, Fava AN, Serrano Junior CV, Pesaro AEP. Potential Conflict of Interest No potential conflict of interest relevant to this article was reported. Sources of Funding There were no external funding sources for this study. Study Association This study is not associated with any thesis or dissertation work. References 1. Zile MR, Brutsaert DL. New concepts in diastolic dysfunction and diastolic heart failure: Part I: diagnosis, prognosis, and measurements of diastolic function. Circulation. 2002;105(11):1387-93. 2. Wang J, Nagueh SF. Current perspectives on cardiac function in patients with diastolic heart failure. Circulation. 2009;119(8):1146-57. 3. Pfeffer MA, Braunwald E, Moye LA, Basta L, Brown EJ Jr, Cuddy TE, et al. Effect of captopril on mortality and morbidity in patients with left ventricular dysfunction after myocardial infarction. Results of the survival and ventricular enlargement trial. The SAVE Investigators. N Engl J Med. 1992;327(10):669-77. Arq Bras Cardiol. 2015; 105(2):145-150 148 Antonelli et al. Diastolic heart failure in myocardial infarction Original Article 4. Volpi A, De Vita C, Franzosi MG, Geraci E, Maggioni AP, Mauri F, et al. Determinants of 6-month mortality in survivors of myocardial infarction after thrombolysis. Results of the GISSI-2 data base. The Ad hoc Working Group of the Gruppo Italiano per lo Studio della Sopravvivenza nell’Infarto Miocardico (GISSI)-2 Data Base. Circulation. 1993;88(2):416-29. 5. Oh JK, Ding ZP, Gersh BJ, Bailey KR, Tajik AJ. Restrictive left ventricular diastolic filling identifies patients with heart failure after acute myocardial infarction. J Am Soc Echocardiogr. 1992;5(5):497-503. 6. Nijland F, Kamp O, Karreman AJ, van Eenige MJ, Visser CA. Prognostic implications of restrictive left ventricular filling in acute myocardial infarction: a serial Doppler echocardiographic study. J Am Coll Cardiol. 1997;30(7):1618-24. 7. Sanz G, Castaner A, Betriu A, Magrina J, Roig E, Coll S, et al. Determinants of prognosis in survivors of myocardial infarction: a prospective clinical angiographic study. N Engl J Med. 1982;306(18):1065-70. 8. 9. Nicod P, Gilpin E, Dittrich H, Chappuis F, Ahnve S, Engler R, et al. Influence on prognosis and morbidity of left ventricular ejection fraction with and without signs of left ventricular failure after acute myocardial infarction. Am J Cardiol. 1988;61(15):1165-71. Spencer FA, Meyer TE, Gore JM, Goldberg RJ. Heterogeneity in the management and outcomes of patients with acute myocardial infarction complicated by heart failure: the National Registry of Myocardial Infarction. Circulation. 2002;105(22):2605-10. 10. Greenberg H, McMaster P, Dwyer EM Jr. Left ventricular dysfunction after acute myocardial infarction: results of a prospective multicenter study. J Am Coll Cardiol. 1984;4(5):867-74. 11. Poulsen SH, Jensen SE, Gotzsche O, Egstrup K. Evaluation and prognostic significance of left ventricular diastolic function assessed by Doppler echocardiography in the early phase of a first acute myocardial infarction. Eur Heart J. 1997;18(12):1882-9. 12. Bennett KM, Hernandez AF, Chen AY, Mulgund J, Newby LK, Rumsfeld JS, et al. Heart failure with preserved left ventricular systolic function among patients with non-ST-segment elevation acute coronary syndromes. Am J Cardiol. 2007;99(10):1351-6. 13. Steg PG, Dabbous OH, Feldman LJ, Cohen-Solal A, Aumont MC, Lopez-Sendon J, et al. Determinants and prognostic impact of heart failure complicating acute coronary syndromes: observations from the Global Registry of Acute Coronary Events (GRACE). Circulation. 2004;109(4):494-9. 14. Wu AH, Parsons L, Every NR, Bates ER. Hospital outcomes in patients presenting with congestive heart failure complicating acute myocardial infarction: a report 149 Arq Bras Cardiol. 2015; 105(2):145-150 from the Second National Registry of Myocardial Infarction (NRMI-2). J Am Coll Cardiol. 2002;40(8):1389-94. 15. Makdisse M, Katz M, Correa Ada G, Forlenza LM, Perin MA, de Brito Junior FS, et al. Effect of implementing an acute myocardial infarction guideline on quality indicators. Einstein. 2013;11(3):357-63. 16. Alpert JS, Thygesen K, Antman E, Bassand JP. Myocardial infarction redefined--a consensus document of The Joint European Society of Cardiology/American College of Cardiology Committee for the redefinition of myocardial infarction. J Am Coll Cardiol. 2000;36(3):959-69. 17. Velazquez EJ, Pfeffer MA. Acute heart failure complicating acute coronary syndromes: a deadly intersection. Circulation. 2004;109(4):440-2. 18. Solomon SD, Glynn RJ, Greaves S, Ajani U, Rouleau JL, Menapace F, et al. Recovery of ventricular function after myocardial infarction in the reperfusion era: the healing and early afterload reducing therapy study. Ann Intern Med. 2001;134(6):451-8. 19. Braunwald E, Kloner RA. The stunned myocardium: prolonged, postischemic ventricular dysfunction. Circulation. 1982;66(6):1146-9. 20. Paulus WJ, Tschope C, Sanderson JE, Rusconi C, Flachskampf FA, Rademakers FE, et al. How to diagnose diastolic heart failure: a consensus statement on the diagnosis of heart failure with normal left ventricular ejection fraction by the Heart Failure and Echocardiography Associations of the European Society of Cardiology. Eur Heart J. 2007;28(20):2539-50. 21. Shah RV, Holmes D, Anderson M, Wang TY, Kontos MC, Wiviott SD, et al. Risk of heart failure complication during hospitalization for acute myocardial infarction in a contemporary population: insights from the National Cardiovascular Data ACTION Registry. Circ Heart Fail. 2012;5(6):693-702. 22. Kim SA, Rhee SJ, Shim CY, Kim JS, Park S, Ko YG, et al. Prognostic value of N-terminal probrain natriuretic peptide level on admission in patients with acute myocardial infarction and preserved left ventricular ejection fraction. Coron Artery Dis. 2011;22(3):153-7. 23. Gerber Y, Weston SA, Berardi C, McNallan SM, Jiang R, Redfield MM, et al. Contemporary trends in heart failure with reduced and preserved ejection fraction after myocardial infarction: a community study. Am J Epidemiol. 2013;178(8):1272-80. 24. van Diepen S, Chen AY, Wang TY, Alexander KP, Ezekowitz JA, Peterson ED, et al. Influence of heart failure symptoms and ejection fraction on short- and long-term outcomes for older patients with non-ST-segment elevation myocardial infarction. Am Heart J. 2014;167(2):267-73. Antonelli et al. Diastolic heart failure in myocardial infarction Original Article Arq Bras Cardiol. 2015; 105(2):145-150 150 Back to the Cover Original Article Tramadol Alleviates Myocardial Injury Induced by Acute Hindlimb Ischemia Reperfusion in Rats Hamed Ashrafzadeh Takhtfooladi1, Adel Haghighi Khiabanian Asl1, Mehran Shahzamani2, Mohammad Ashrafzadeh Takhtfooladi3, Amin Allahverdi4, Mohammadreza Khansari5 Department of Pathobiology, Science and Research Branch, Islamic Azad University1, Department of Cardiovascular Surgery, Isfahan University of Medical Sciences2, Young Researchers and Elites Club, Science and Research Branch, Islamic Azad University3, Department of Surgery, Science and Research Branch, Islamic Azad University4, Department of Physiology, Science and Research Branch, Islamic Azad University5, Tehran - Iran Abstract Background: Organ injury occurs not only during periods of ischemia but also during reperfusion. It is known that ischemia reperfusion (IR) causes both remote organ and local injuries. Objective: This study evaluated the effects of tramadol on the heart as a remote organ after acute hindlimb IR. Methods: Thirty healthy mature male Wistar rats were allocated randomly into three groups: Group I (sham), Group II (IR), and Group III (IR + tramadol). Ischemia was induced in anesthetized rats by left femoral artery clamping for 3 h, followed by 3 h of reperfusion. Tramadol (20 mg/kg, intravenous) was administered immediately prior to reperfusion. At the end of the reperfusion, animals were euthanized, and hearts were harvested for histological and biochemical examination. Results: The levels of superoxide dismutase (SOD), catalase (CAT), and glutathione peroxidase (GPx) were higher in Groups I and III than those in Group II (p < 0.05). In comparison with other groups, tissue malondialdehyde (MDA) levels in Group II were significantly increased (p < 0.05), and this increase was prevented by tramadol. Histopathological changes, including microscopic bleeding, edema, neutrophil infiltration, and necrosis, were scored. The total injury score in Group III was significantly decreased (p < 0.05) compared with Group II. Conclusion: From the histological and biochemical perspectives, treatment with tramadol alleviated the myocardial injuries induced by skeletal muscle IR in this experimental model. (Arq Bras Cardiol. 2015; 105(2):151-159) Keywords: Tramadol/ therapeutic use; Heart Injuries; Heart/physiopathology; Reperfusion Injury; Rats. Introduction Restoration of blood flow after a period of ischemia causes ischemia reperfusion (IR) injury. IR injury is a serious clinical problem that occurs in many diseases and surgeries, such as limb orthopedic surgery, organ transplantation, cardiopulmonary bypass, and hypovolaemic shock1,2. During IR, tissues are subjected to destructive proinflammatory cytokines and reactive oxygen species released by inflammatory cells, leading to inflammatory injury and cell apoptosis3,4. IR also affects the secondary organs, including liver5, heart6, kidney7, lung8, and even causes multiple organ failure, which is a common cause of mortality. Therefore, antioxidative, anti-inflammatory, and antiapoptotic agents to attenuate multiple organ injury induced by IR are urgently required. Various investigators have demonstrated that the opioid pathway is involved in tissue preservation during hypoxia Mailing Address: Mohammad Ashrafzadeh Takhtfooladi • Young Researchers and Elites Club, Science and Research Branch, Islamic Azad University. Postal Code 8177613343, Tehran, Iran. E-mail: [email protected] Manuscript received January 02, 2015; revised manuscript February 27, 2015; accepted March 11, 2015. DOI: 10.5935/abc.20150059 151 or ischemia, and this protection is mediated via the delta opioid receptor9,10. It has been shown that morphine has cardioprotective effects during IR11,12. Factors, such as respiratory depression and histamine release, are disadvantages of using morphine in the postoperative period of open heart surgery13. Tramadol is a narcotic-like pain reliever drug as it has an unusual mechanism of action involving opioid, noradrenaline, and serotonin (5-hydroxytryptamine) systems of analgesia. It is certainly useful in the treatment of chronic and acute pain. Although it does not cause respiratory depression, the problems of nausea when used in clinically effective analgesic doses for severe pain and the risk of intra-operative awareness may represent significant disadvantages of tramadol14. Recent research discloses that tramadol decreases lipid peroxidation and regulates noradrenalin uptake; therefore, these therapeutic properties are used for the management of myocardial ischemia15. In the past few years, the administration of tramadol was shown to protect against IR injuries in local and remote organs15-18. However, the role of tramadol in reducing injury in the myocardium after hindlimb IR has not been addressed yet. In this study, the effect of tramadol on myocardial injury after hindlimb IR was assessed by biochemical and histological changes in rats. Takhtfooladi et al. Effects of Tramadol on Myocardial Remote Injury Original Article Methods Thirty healthy mature male Wistar rats weighing 250–300 g were purchased from the Pasteur Institute of Iran. All experimental procedures and protocols used in this investigation were reviewed and approved by the Committee of Ethics in Research with Animals at the Islamic Azad University Faculty of Veterinary Medicine. They were kept under constant room temperature of 20–22°C, relative humidity of 50%–60%, 12 h/12 h light/dark cycle, with ad libitum access to filtrated tap water and commercial food and were placed in individual plastic cages with soft bedding. Experimental groups The rats were randomly divided into three experimental groups of ten rats each (of these ten, five were used for biochemical assays and five for histological analysis): Group I (sham group) was subjected to all procedures, except arterial occlusion. The animals received 2 mL of 0.9% saline via the jugular vein. Group II (IR group) was subjected to IR. Two milliliters of 0.9% saline was administered immediately prior to the reperfusion period. Group III (IR + tramadol group) was subjected to IR. A solution of 20 mg/kg tramadol16 in 0.9% saline solution was administered, with a total volume of 2 mL. Anesthesia The rats were weighed and anesthetized using an intramuscular injection of ketamine hydrochloride 10% and xylazine hydrochloride 2% (50 mg/kg and 10 mg/kg, respectively). Surgery After induction of anesthesia, the animals were placed on a board, in a dorsal, recumbent position, with their thoracic and pelvic limbs immobilized with adhesive tape. The jugular vein was isolated and catheterized for the administration of heparin, tramadol, and normal saline. The left hindlimb was prepared for sterile surgery. A skin incision was made on medial surface of the left hindlimb and femoral artery was isolated and was clamped with a non-traumatic clamp for 3 h and followed by 3 h of reperfusion. Prior to the occlusion of the femoral artery, 250 IU heparin17 was administered via the jugular vein in order to prevent clotting. Rats were maintained in a dorsal, recumbent position and kept anesthetized (additional doses were given in case of necessity) throughout the duration of the ischemic period. Body temperature was maintained with a heating pad and monitored using a rectal thermometer. The vascular forceps was removed and the surgical site was routinely closed with 3/0 polypropylene sutures following the ischemic period. Subjects in Group I underwent a surgical procedure similar to the other groups but the femoral artery was not occluded. Specimen collection At the end of the trial, rats were euthanized with an overdose of pentobarbital injection (300 mg/kg, intraperitoneal) and the hearts were rapidly excised. Histological analysis For histological analysis, the hearts were fixed with 10% formalin and then embedded in paraffin and sectioned into 5-μm thick sections and stained with hematoxylin and eosin (H&E). The sections were examined in a semiquantitative manner, using 250× and 400× magnifications under a light microscope by a pathologist who was blinded to the experiment and data. The histological parameters, such as microscopic bleeding, edema, neutrophil infiltration, and necrosis, were scored according to the classification of Papoutsidakis et al.19 as shown in Table 1. Approximately ten fields of view were examined under each magnification. The total histological score for each specimen was determined by the sum of all the partial scores. Biochemical assays Evidence of oxidative stress was determined from heart tissue homogenates using glutathione peroxidase (GPx), catalase (CAT), and superoxide dismutase (SOD) activities and the levels of malondialdehyde (MDA). Each heart was stored separately at −80°C until analysis. The tissues were homogenized in 0.1 M phospate buffer (pH 7.4) with an Ultra Turrax homogenizer. The homogenates were centrifuged at 5000 rpm at 4°C for 10 min; the supernatants were removed and assayed for MDA, GPx, and SOD activities. Tissue GPx and SOD activities were measured with a Hitachi 917 autoanalyser using commercial kits. SOD and GPx activities were expressed as U/mg protein in tissue samples. Tissue MDA levels were determined by the thiobarbituric acid method of Okhawa et al.20 MDA levels were expressed as nmol/mg protein in tissue samples. CAT activities were determined by measuring the decrease in hydrogen peroxide concentration at 230 nm by the method of Beutler21. CAT activity was expressed U/mg protein in tissue samples. Statistical analysis Data were analyzed using SPSS statistical software package (version 18). Distribution of the groups was analyzed with one sample Kolmogorov–Smirnov test. The results were analyzed using analysis of variance for comparing multiple means (ANOVA) with post-hoc test analysis. Biochemical data were tested using the Kruskal–Wallis nonparametric test. Data are shown as the mean ± standard deviation and the significance level was 5%. Results The experimental procedure was well tolerated and no animals died during the experiment. Biochemical results SOD, CAT, GPx, and MDA levels were measured in the heart tissues after 3 h of reperfusion. The levels of SOD, CAT, and GPx were significantly lower in Group II than those in the other groups (Figures 1–3). The reductions in the levels of these molecules were reversed by intravenous injection of tramadol. In comparison with other groups, tissue MDA levels in group II were significantly increased (Figure 4) and this was prevented by tramadol. Arq Bras Cardiol. 2015; 105(2):151-159 152 Takhtfooladi et al. Effects of Tramadol on Myocardial Remote Injury Original Article Table 1 – Histological grading (Papoutsidakis et al.) 0 1 2 3 Magnification None or 1–3 dead cells in < 3 FOV ≤ 3 dead cells per FOV in at least 3 FOV or 4–6 cells in no more than 3 FOV 4–6 dead cells per FOV in at least 4 FOV or > 6 cells in no more than 3 FOV > 6 dead cells in at least 4 FOV 400× Polymorphonuclear leucocytes None or 1–3 cells in < 3 FOV ≤ 3 cells per FOV in at least 3 FOV or 4–6 cells in no more than 3 FOV 4–6 cells per FOV in at least 4 FOV or > 6 cells in no more than 3 FOV > 6 cells in at least 4 FOV 400× Eosinophils None or 1–3 cells in < 3 FOV ≤ 3 cells per FOV in at least 3 FOV or 4–6 cells in no more than 3 FOV 4–6 cells per FOV in at least 4 FOV or > 6 cells in no more than 3 FOV > 6 cells in at least 4 FOV 400× Loss of striation None or 1–5 cells in < 3 FOV ≤ 5 cells per FOV in at least 3 FOV or 5–10 cells in no more than 3 FOV 5–10 cells per FOV in at least 4 FOV or > 6 cells in no more than 3 FOV > 10 cells in at least 4 FOV 400× Edema None < 10% of FOV in at least 3 FOV or > 10% in < 3 FOV 10%–30% of FOV in at least 3 FOV or > 30% in < 3 FOV > 30% of FOV in at least 3 FOV 250× Microscopic bleeding None Present in < 10% of FOV in at least 3 FOV or > 10% in < 3 FOV Present in 10%–30% of FOV in at least 3 FOV or > 30% in < 3 FOV Present in > 30% of FOV in at least 3 FOV 250× Necrosis FOV: Fields of view Histological results Histopathological changes, including microscopic bleeding, edema, neutrophil infiltration, and coagulative necrosis, were scored. The total injury score in Group III was significantly decreased compared with Group II (Figure 5). Representative H&E-stained microscopic images of myocardial tissue from Groups II and III are presented in Figures 6 and 7, respectively. Discussion The local and remote consequences of limb IR injury continue to be a serious clinical problem for general vascular surgeons, interventional radiologists, and cardiologists. Reperfusion of the skeletal muscle causes activation and adhesion of polymorphonuclear neutrophils, with the release of proinflammatory substances and the formation of free radicals, which include nitrogen-derived reactive nitrogen species and oxygen-derived reactive oxygen species, such as superoxide, peroxide, and hydroxyl radicals22-24. In addition, the proinflammatory and injurious factors activated in large amounts after skeletal muscle IR injury circulate via both the venous and lymph systems and induce distant organ injury 25. This distant organ injury may be a component of systemic inflammatory response syndrome, acute respiratory distress syndrome, or multi‑organ dysfunction syndrome, which are initially triggered by muscle-derived inflammatory mediators26. As far as we know, there are only a few reports demonstrating remote myocardial injury following skeletal muscle IR injury.8 The results of Takhtfooladi et al.27 indicated that hindlimb IR induces severe myocardial damage and that N-acetylcysteine has protective effects on the myocardium after hindlimb IR. Their data supported the concept that temporary occlusion of the femoral artery induced myocardial injury in rats27. 153 Arq Bras Cardiol. 2015; 105(2):151-159 Previous studies have shown that the use of tramadol after IR in animals attenuated the oxidative injuries. Nagakannan et al. 28 demonstrated the neuroprotective effect of tramadol against transient forebrain ischemia in rats. Tramadol provides a cardioprotective effect against myocardial IR in isolated rat hearts 15. Wagner et al. 29 suggested that tramadol given to humans in high doses actually caused myocardial injury, with increased troponin 1 and decreased inducible nitric oxide synthases expression, possibly due to the systemic undesirable serotonergic effect on diseased coronary arteries. A recent study showed that ischemia for 2 h was sufficient to obtain a considerable degree of injury in skeletal muscles and the intravenous injection of 20 mg/kg tramadol prevented this deleterious effect16. Similarly, tramadol at a similar dose was found to be beneficial on lung injuries induced by skeletal muscle IR when femoral artery clamping was applied 17. Furthermore, tramadol (20 mg/kg) was determined to be protective against cerebral injuries caused by hindlimb IR in rats18. There is growing evidence regarding tramadol’s beneficial effects in ameliorating IR; however, its role in reducing the damage in heart tissue after skeletal muscle IR has not been addressed yet. In our study, the antioxidant potential of tramadol was investigated using MDA, GPx, CAT, and SOD contents in myocardial tissue following acute hindlimb IR. The MDA level is a marker of tissue lipid peroxidation. The amount of MDA accumulation in tissue is an index of the extent of lipid peroxidation and oxidative stress15,30. The lower levels of MDA observed in the group receiving tramadol compared with the IR group supports the hypothesis that tramadol may reduce oxidative stress by scavenging peroxyl radicals. GPx activity is known to depend on reduced levels of glutathione, glutathione transferase, and glutathione reductase. Activities of these enzymes play an essential role in the cellular defense against free radicals15,30. Data regarding Takhtfooladi et al. Effects of Tramadol on Myocardial Remote Injury Original Article 7 SOD (U/mg protein) 6 5 4 3 2 1 0 Sham IR* IR + T Figure 1 – Superoxide dismutase (SOD; U/mg protein) in heart tissue between the groups studied. IR: ischemia reperfusion; and IR + T: ischemia reperfusion + tramadol. Data were expressed as mean ± SD. *: The significant digits in all group were p < 0.001. 500 CAT (U/mg protein) 400 300 200 100 0 Sham IR* IR + T Figure 2 – Catalase (CAT; U/mg protein) in heart tissue between the groups studied. IR: ischemia reperfusion and IR + T: ischemia reperfusion + tramadol. Data were expressed as mean ± SD. *: The significant digits in all group were p < 0.001. Arq Bras Cardiol. 2015; 105(2):151-159 154 Takhtfooladi et al. Effects of Tramadol on Myocardial Remote Injury Original Article 0.05 GPX (U/mg protein) 0.04 0.03 0.02 0.01 0.00 Sham IR* IR + T Figure 3 – Glutathione peroxidase (GPX; U/mg protein) in heart tissue between the groups studied. IR: ischemia reperfusion and IR + T: ischemia reperfusion + tramadol. Data were expressed as mean ± SD. *: The significant digits in all group were p < 0.001. 6 MDA (nmol/protein) 5 4 3 2 1 0 Sham IR* IR + T Figure 4 – Malendialdehyde (MDA; nmol/mg protein) in heart tissue between the groups studied. IR: ischemia reperfusion and IR + T: ischemia reperfusion + tramadol. Data were expressed as mean ± SD. *: The significant digits in all group were p < 0.001. 155 Arq Bras Cardiol. 2015; 105(2):151-159 Takhtfooladi et al. Effects of Tramadol on Myocardial Remote Injury Original Article 5 Histological Grading 4 3 2 1 0 Sham IR* IR + T Figure 5 – Histological grading between the groups studied. IR: ischemia reperfusion and IR + T: ischemia reperfusion + tramadol. Data were expressed as mean ± SD. *: The significant digits in all group were p < 0.001. Figure 6 – Photomicrograph of myocardium in the ischemia reperfusion group showing coagulative necrosis. Muscle cells with pyknotic nuclei were stained more deeply with eosin in the area of coagulative necrosis (hematoxylin and eosin staining, bar = 100 μm). SOD support a possible antioxidant effect of tramadol. The decreased levels of MDA and elevated levels of SOD activity in tissues may be evidence of decreased lipid peroxidation and increased antioxidant capacity. The analysis of the myocardium under light microscopy revealed the presence of more edema, neutrophil infiltration, and coagulative necrosis in Group II than in Group III; this shows tramadol’s tendency to attenuate these injuries, a Arq Bras Cardiol. 2015; 105(2):151-159 156 Takhtfooladi et al. Effects of Tramadol on Myocardial Remote Injury Original Article Figure 7 – Representative photomicrograph of myocardium in the ischemia reperfusion + tramadol group showing nearly normal structure (hematoxylin and eosin staining, bar = 100 μm). trend that has statistical significance. This observation was supported by Takhtfooladi et al.27, who demonstrated that temporary occlusion of the femoral artery in rats resulted in histological changes. Conclusion The results of this study confirmed that the administration of tramadol significantly decreased myocardial injuries induced by hindlimb IR. This protective effect of tramadol is probably ascribed to anti-inflammatory activity. We underscore the necessity of human studies with tramadol that may be beneficial in preventing remote organ injury, particularly during surgical interventions. and interpretation of the data: Takhtfooladi HA, Allahverdi A. Statistical analysis: Khansari M. Obtaining financing: Takhtfooladi MA. Writing of the manuscript: Takhtfooladi MA. Critical revision of the manuscript for intellectual content: Khiabanian AH. Supervision / as the major investigador: Shahzamani M. Histological Analysis: Khiabanian AH. Help with technical procedures: Allahverdi A. Potential Conflict of Interest No potential conflict of interest relevant to this article was reported. Sources of Funding There were no external funding sources for this study. Author contributions Study Association Conception and design of the research: Takhtfooladi HA, Shahzamani M. Acquisition of data: Takhtfooladi MA. Analysis This study is not associated with any thesis or dissertation work. References 157 1. Parks DA, Granger DN. Contributions of ischemia and reperfusion to mucosal lesion formation. Am J Physiol. 1986;250(Pt1):749-53. 6. Horton JW, White DJ. Free-radical scavengers prevent intestinal ischemiareperfusion-mediated cardiac dysfunction. J Surg Res.1996;64(1):19-25. 2. Welbourn CR, Goldman G, Paterson IS, Valeri CR, Shepro D, Hechtman HB. Pathophysiology of ischaemia reperfusion injury: central role of the neutrophil. Br J Surg. 1991;78(6):651-5. 7. 3. Grace PA, Ischaemia-reperfusion injury. Br J Surg.1994;81(5):637-47. 4. Rudiger HA, Clavien PA. Tumor necrosis factor-alpha, but not Fas, mediates hepatocellular apoptosis in the murine ischemic liver. Gastroenterology. 2002;122(1):202-10. 8. Savas C, Ozguner M, Ozguner IF,Delibas N. Splenectomy attenuates intestinal ischemia-reperfusion-induced acute lung injury. J Pediatr Surg. 2003;38(10):1465-70. 5. Yamagish Y, Horie Y, Kato S, Kajiara M, Tamai H, Granger DN, et al. Ethonal modulates gut ischemia/reperfusion-induced liver injury in rats. Am J Physiol Gastrointest Liver Physiol 2002;282(4):G640-6. Arq Bras Cardiol. 2015; 105(2):151-159 LaNoue JL, Turnage RH, Kadesky KM, Guice KS, Oldham KT, Myers SI. The effect of intestinal reperfusion on renal function and perfusion. J Surg Res. 1996;64(1):19-25. 9. Chien S, Oeltgen PR, Diana JN, Salley RK, Su TP. Extension of tissue survival time in multiorgan block preparation with a delta opioid DADLE ([D-Ala2, D-Leu5]-enkephalin). J Thorac Cardiovasc Surg . 1994;107(3):964–7. Takhtfooladi et al. Effects of Tramadol on Myocardial Remote Injury Original Article 10. Mayfield KP, D’Alecy LG. Delta-1 opioid receptor dependence of acute hypoxic adaptation. J Pharmacol Exp Ther. 1994;268(1):74–7. 21. Beutler E. Red cell metabolism. 2nd ed. New York: Grune and Stratton Co., 1975.p. 261–5. 11. Groban L, Vernon JC, Butterworth J. Intrathecal morphine reduces infarct size in a rat model of ischemia-reperfusion injury. Anesth Analg. 2004;98(4):903-9. 22. Guven A, Tunc T, Topal T, Kul M, Korkmaz A, Gundogdu G, et al. ɑ-Lipoic acid and ebselen prevent ischemia/reperfusion injury in the rat intestine. Surg Today 2008;38(11):1029-35. 12. McPherson BC, Yao Z. Signal transduction of opioid-induced cardioprotection in ischemia-reperfusion. Anesthesiology. 2001;94(6):1082-8. 13. Ellmauer S, Dick W, Otto S, Muller H. Different opioids in patients at cardiovascular risk. Comparison of centrally and peripheral hemodynamic adverse effects. Anaesthesist. 1994;43(11):743-9. 14. Raffa RB, Friderichs E, Reimann W, et al, Opioid and nonopioid components independently contribute to the mechanism of action of tramadol, an ‘atypical’ opioid analgesic. J Pharmacol Exp Ther. 1992;260(1):275-85. 15. Bilir A, Erkasap N, Koken T,Gulec C, Kaggisiz Z, Tanriverdi B, et al. Effects of tramadol on myocardial ischemia-reperfusion injury. Scand Cardiovasc J. 2007;41(4):242–7. 16. Takhtfooladi HA, Takhtfooladi MA, Karimi P, Abbasian Asl H, Mousavi Nasab Mobarakeh SZ. Influence of tramadol on ischemia-reperfusion injury of rats’ skeletal muscle. Inter J Surg. 2014;12(9):963-8. 17. Takhtfooladi MA, Jahanshahi A, Sotoudeh A, Daneshi MH, Khansari M, Takhtfooladi HA. Effect of tramadol on lung injury induced by skeletal muscle ischemia-reperfusion: an experimental study. J Bras Pneumol. 2013;39(4):434-9. 18. Takhtfooladi MA, Jahanshahi A, Sotoudeh A, Daneshi MH, Aslami K, Takhtfooladi H. Neuroprotective effects of tramadol on cerebral injuries caused by hind limb ischaemia/reperfusion in rats. Comp Clin Pathol 2014;23:1141–6. 19. Papoutsidakis N, Arkadopoulos N, Smyrniotis V, Tzanatos H, Kalimeris K, Nastos K, et al. Early myocardial injury is an integral component of experimental acute liver failure–a study in two porcine models. Arch Med Sci. 2011;2(2):217-23. 20. Ohkawa H, Ohishi N, Yagi K. Assay for lipid peroxidase in animal tissues by thiobarbituric acid reaction. Anal Biochem. 1979;95(2):351–8. 23. Mallick IH, Yang W, Winslet MC, Seifalian AM. Ischemia-reperfusion injury of the intestine and protective strategies against injury. Dig Dis Sci 2004;49(9):1359-77. 24. Li C, Jackson RM. Reactive species mechanisms of cellular hypoxiareoxygenation injury. Am J Physiol Cell Physiol 2002; 282(2):C227-41. 25. Deitch EA, Forsythe R, Anjaria D, Livingston DH, Lu Q, Xu DZ, et al. The role of lymph factors in lung injury, bone marrow suppression, and endothelial cell dysfunction in a primate model of trauma-hemorrhagic shock. Shock. 2004;22(3):221-8. 26. Rotstein OD. Pathogenesis of multiple organ dysfunction syndrome: Gut origin, protection, and decontamination. Surg Infect (Larchmt). 2000;1(3):217–23. 27. Takhtfooladi MA, Jahanshahi G, Sotoudeh A, Jahanshahi A. Protective effects of N-acetylcysteine on myocardial injury induced by hind limb ischaemia reperfusion; Histological study in rat model. Comp Clin Pathol 2014; 23:1237–40. 28. Nagakannan P, Shivasharan BD, Thippeswamy BS, Veerapur VP. Effect of tramadol on behavioral alterations and lipid peroxidation after transient forebrain ischemia in rats. Toxicol Mech Methods. 2012; 22(9):674–8. 29. Wagner R, Piler P, Bedanova H, Adamek P, Grodecka L, Freiberger T. Myocardial injury is decreased by late remote ischaemic preconditioning and aggravated by tramadol in patients undergoing cardiac surgery: a randomised controlled trial, Interact. Cardiovasc. Thorac Surg . 2010;11(6):758-62. 30. Polat A, Emre MH. Effects of melatonin or acetylsalicylic acid on gastric oxidative stress after bile duct ligation in rats. J Gastroenerol. 2006;41(5):433–9. Arq Bras Cardiol. 2015; 105(2):151-159 158 Takhtfooladi et al. Effects of Tramadol on Myocardial Remote Injury Original Article 159 Arq Bras Cardiol. 2015; 105(2):151-159 Back to the Cover Original Article Effects of One Resistance Exercise Session on Vascular Smooth Muscle of Hypertensive Rats Tharciano Luiz Teixeira Braga da Silva1, Marcelo Mendonça Mota1, Milene Tavares Fontes1, João Eliakim dos Santos Araújo1, Vitor Oliveira Carvalho1, Leonardo Rigoldi Bonjardim2, Márcio Roberto Viana Santos1 Universidade Federal de Sergipe1, São Cristóvão, SE; Universidade de São Paulo2, São Paulo, SP – Brazil Abstract Background: Hypertension is a public health problem and increases the incidence of cardiovascular diseases. Objective: To evaluate the effects of a resistance exercise session on the contractile and relaxing mechanisms of vascular smooth muscle in mesenteric arteries of NG-nitro L-arginine methyl ester (L-NAME)-induced hypertensive rats. Methods: Wistar rats were divided into three groups: control (C), hypertensive (H), and exercised hypertensive (EH). Hypertension was induced by administration of 20 mg/kg of L-NAME for 7 days prior to experimental protocols. The resistance exercise protocol consisted of 10 sets of 10 repetitions and intensity of 40% of one repetition maximum. The reactivity of vascular smooth muscle was evaluated by concentration‑response curves to phenylephrine (PHEN), potassium chloride (KCl) and sodium nitroprusside (SNP). Results: Rats treated with L-NAME showed an increase (p < 0.001) in systolic blood pressure (SBP), diastolic blood pressure (DBP) and mean arterial pressure (MAP) compared to the initial period of induction. No difference in PHEN sensitivity was observed between groups H and EH. Acute resistance exercise reduced (p < 0.001) the contractile response induced by KCl at concentrations of 40 and 60 mM in group EH. Greater (p < 0.01) smooth muscle sensitivity to NPS was observed in group EH as compared to group H. Conclusion: One resistance exercise session reduces the contractile response induced by KCl in addition to increasing the sensitivity of smooth muscle to NO in mesenteric arteries of hypertensive rats. (Arq Bras Cardiol. 2015; 105(2):160-167) Keywords: Hypertension; Exercise; Vasodilatation; Rats; Muscle, Smooth; Mesenteric, Artery. Introduction Hypertension is a public health problem worldwide, and is associated with the increasing incidence of deaths due to cardiovascular diseases1. Several hypertension models have been developed within the basic sciences to mimic the pathological effects of hypertension2,3. The experimental hypertension model in rats using inhibition of nitric oxide synthase (NOS) with NG-nitro-L-arginine-methyl-ester (L-NAME) determines arterial hypertension, kidney injury, sympathetic overactivity and endothelial dysfunction4-8. It is worth noting that the induction of hypertensive rats depends on the L-NAME dose administered, treatment duration, target organ studied, age and type of the animal used in the study. In association with that hypertension Mailing Address: Marcio Roberto Viana Santos • Universidade Federal de Sergipe. Departamento de Fisiologia, Universidade Federal de Sergipe, Av. Marechal Rondon, S/N, Rosa Elze. Postal Code 49100-000, São Cristóvão, SE – Brazil E-mail: [email protected], [email protected] Manuscript received November 16, 2014; revised manuscript March 12, 2015; accepted March 23, 2015. DOI: 10.5935/abc.20150070 160 model, studies have shown that aerobic and resistance exercises are beneficial regarding aspects related to blood pressure and vascular function in rats9,10. Nitric oxide synthase inhibition induces hypertension by increasing blood pressure via an endothelium-dependent response7. Our team has recently shown that submitting L-NAME-induced rats to resistance exercise for four weeks can reduce sensitivity to phenylephrine (PHEN) and increase sensitivity to sodium nitroprusside (SNP) of the superior mesenteric artery smooth muscle10. The study of resistance exercise in animal models mimicking hypertension provides relevant information for clinical studies aimed at disease prevention, treatment and control. Despite our team’s findings10, so far the effects of resistance exercise on the contracting and relaxing parameters related to vascular smooth muscle have not been well established. A study has recently shown that submitting spontaneously hypertensive rats (SHR) to one session of resistance exercise does not change the vascular function of the tail artery in relaxations induced by SNP, an exogenous donor of nitric oxide (NO)11. Several variables, such as disease animal model, type of artery studied, type of resistance exercise, and volume, intensity and duration of physical stimulus, can influence the benefits of resistance exercise. The present study aimed at assessing the effects Braga da Silva et al. Acute Effects of Resistance Exercise on Smooth Muscle Original Article of one resistance exercise session on the contraction and relaxation mechanisms of the mesenteric artery smooth muscle of L-NAME-induced hypertensive rats. Methods Animals Wistar rats (250-300 g) were used in all experiments. The animals were maintained under controlled temperature (22 ± 1°C) and 12-hour light-dark cycles, with water and food ad libitum. All procedures described in the present study were approved by the Ethics Committee in Research with Animals of the Universidade Federal de Sergipe, Brazil (Protocol 32/2013). The animals were divided into three groups with ten animals each: sedentary control (C); sedentary control with hypertension (H) and exercised hypertensive (EH). The animals of groups C and H were maintained inside boxes with no exposure to exercise, and only group EH animals underwent one resistance exercise session. Hypertension induction, and blood pressure and body weight measurements Before beginning the procedure of experimental hypertension induction, blood pressure was measured by using the non-invasive caudal method (LETICA, LE5002, Barcelona, Spain). After that, only animals of groups H and EH received orally L-NAME (20 mg/kg, daily), through gavage, for seven days8. By the end of the induction period, blood pressure was measured again in all groups. Animals with mean arterial pressure (MAP) greater than 130 mm Hg were categorized as hypertensive. Body weight was daily assessed to adjust the L-NAME dosage. Protocol of resistance exercise Resistance exercise was performed in a squatting apparatus according to the model by Tamaki et al.12. Initially, group EH animals were acquainted with the exercise apparatus for three days, and, then, the one repetition maximum (RM) test was performed. One RM was determined as the maximum weight lifted by each rat, using the exercise apparatus13. Two days after the RM test, the animals underwent the resistance exercise protocol adapted from Fontes et al.14. The rats underwent ten sessions of ten repetitions, with 60-second rest intervals, and intensity of 40% of the load established by using the RM test. The parameters of electrical stimulation are similar to those described by Barauna et al.15. The animals of groups C and H underwent none of those procedures. Assessing smooth muscle vascular reactivity Immediately after the resistance exercise session, all rats of all groups were sacrificed and superior mesenteric artery rings, free from connective tissue, were sectioned (1-2 mm). Endothelium‑independent relaxation was assessed by using the superior mesenteric artery rings prepared according to the description by Menezes et al.16. The presence or absence of functional endothelium was assessed by the ability, measured as percentage (%), of acetylcholine (ACh; 1 µM) to relax the pre‑contracted rings with 1 µM of PHEN. Rings whose relaxations were below 10% were considered not to have a functional endothelium and automatically selected for this study17. The changes in vascular reactivity due to the contracting and relaxing agents were assessed through concentrationresponse curves of the superior mesenteric artery rings of the rats of all groups. After the stabilization period of the isolated rings, curves for the contracting agents were performed: PHEN (10-9-10-4 M) (α-1 adrenergic agonist) and KCl (20-80 mM) (unspecific contracting agent). In addition, experiments for the relaxing agent were conducted: SNP (10-11-10-6 M), NO donor, in pre-contracted rings with PHEN (1 µM). All experimental protocols were conducted separately. Data from the concentration-response curves were assessed by using the adjustment of a logistic function: E = Rmax/ ((1+(10c/10x)n) + Φ), where E is the response; Rmax is the maximal response the agonist can produce; c is the logarithm of EC50, which is the concentration at which the agonist produces a response equal to 50% of the maximal response; x is the logarithm of the concentration of the agonist; the exponential term, n, is a parameter of adjustment of the curve that defines the inclination of the concentration-response line; and Φ is the response observed in the absence of the agonist. Non-linear regression analyses were performed to determine the parameters Rmax, EC 50 and n, with the restriction Φ = zero. The sensitivity of the superior mesenteric artery rings was assessed by determining the pD2 value of each agonist. That corresponds to the negative logarithm of the molar concentration of the agonist that determines a response equal to 50% of the maximal response (EC50), in each experiment. Drugs and reagents NG-nitro-L-arginine-methyl-ester (L-NAME), acetylcholine chloride (ACh), L-phenylephrine chloride (PHEN), sodium nitroprusside (SNP), salts and reagents used in the present study were obtained from Sigma (Sigma Chemical Co, St. Louis, MO, USA). Statistical analyses The Kolmogorov-Smirnov test was used to determine whether the probability distributions of the data were parametric or non-parametric. All data had a normal distribution. The values were expressed as mean ± standard error of the mean (SEM). Student t tests paired and analysis of variance (one-way and two-way ANOVA) followed by Bonferroni post‑test were used when necessary to assess the significance of the differences between the means. The values were considered statistically significant when p < 0.05. The GraphPad Prism program, version 3.02 (GraphPad Software, San Diego-CA, USA), was used in all procedures. Results Body weight and blood pressure in response to hypertension induction We observed that in the beginning and end of the hypertension induction period, the body weight of the rats Arq Bras Cardiol. 2015; 105(2):160-167 161 Braga da Silva et al. Acute Effects of Resistance Exercise on Smooth Muscle Original Article was similar in all groups. After seven days of induction, the rats treated with L-NAME showed an increase (p < 0.001) in the levels of MAP, systolic blood pressure (SBP) and diastolic blood pressure (DBP). When the end of the induction period between the groups was statistically assessed, L-NAME showed to induce an increase in MAP, SBP and DBP (p < 0.001) in the groups H and EH as compared to group C (Table 1). Vascular smooth muscle constriction in response to PHEN We observed that PHEN (10 -9 -10 -4 M) induced concentration-dependent contraction of the isolated rings of the superior mesenteric artery in all groups. However, the maximal contraction response did not differ between the groups (Figure 1A). L-NAME could interfere with the arterial sensitivity of PHEN‑induced contractions in hypertensive-induced rats, because pD2 changed (p < 0.05) in group H as compared to group C (Figure 1B). In addition, one resistance exercise session did not interfere with arterial sensitivity, and pD2 remained unaltered when comparing groups EH and H (Figure 1B). Vascular smooth muscle constriction in response to KCl We observed that the increase in extracellular KCl (20‑80 mM) produced contractile tension in the isolated rings of the superior mesenteric artery of the rats of all groups. However, the maximal responses induced by KCl did not differ between the groups (Figure 2). The animals induced to hypertension with L-NAME had a higher percentage contraction of vascular smooth muscle at the concentrations of 40 and 60 mM of KCl (p < 0.01; p < 0.001, respectively) (Figure 2). On the other hand, group EH animals had a lower percentage contraction of vascular smooth muscle at the concentrations of 40 and 60 mM (p < 0.001) (Figure 2). Vascular smooth muscle dilation in response to SNP We observed that SNP (10-11-10-6 M) induced endotheliumindependent relaxation in the isolated rings of the superior mesenteric artery of the rats of all groups (Figure 3A). The maximal vascular relaxation in response to SNP was similar in the three groups studied (Figure 3A). L-NAME reduced (p < 0.05) the arterial sensitivity to SNP in group H animals as compared to those in group C (Figure 3B). Inversely, we observed that resistance exercise could restore arterial sensitivity to SNP by increasing (p < 0.01) pD2 of group EH as compared to that of group H (Figure 3B). Discussion The results of this study show that one resistance exercise session in L-NAME-induced hypertensive rats caused a reduction in the KCl-induced contracting mechanisms by increasing the vasodilating sensitivity of the mesenteric artery smooth muscle. There is evidence that the reduced levels of NO play an important role in the development of hypertension4,18. The experimental model of hypertension that mimics that effect is the one induced by the inhibition of NOS with a unspecific inhibitor, L-NAME4,19. Treatment with L-NAME is associated with structural and functional changes in the kidneys, changes in autonomic modulation and in peripheral vascular resistance, and an increase in blood pressure4,6,8,20. The present study showed a blood pressure increase of the animals treated with L-NAME for seven days. The hypertensive levels obtained are similar to those previously reported for rats treated with L-NAME for seven days 6,8,20. The literature describes that the transmission of the signal originated in the plasma membrane for the receptors of the smooth muscle contractile machinery is due to pharmacomechanical and/or electromechanical stimuli 21. Those mechanisms should not be understood as completely separated systems, but understood as part of a network of signals that interact to maintain vascular physiology. In our study, the rats treated with L-NAME showed higher α-1 adrenergic sensitivity. The modulation of α-1 adrenergic receptors and the reduction in NO production play an important role in the cardiovascular changes of hypertensive rats22. It has already been shown that a reduction in NO shifts the contraction curve of PHEN to the left in the aorta of rats, but not in the tail artery, confirming that the modulation of receptors in response to NO seems to depend on the type of the artery studied23. Heijenbrok et al.24 have treated Wistar rats with L-NAME (15 mg/kg/day) for six weeks and have not observed any change related to PHEN in the vascular reactivity of the carotid and mesenteric arteries. The inconsistence about the modulation of α-1 adrenergic receptors in animals Table 1 – Body weight, mean arterial pressure (MAP), systolic blood pressure (SBP) and diastolic blood pressure (DBP) of rats at the beginning and end of systemic hypertension induction Groups C (n = 10) H (n = 10) EH (n = 10) Period Weight (g) MAP (mm Hg) SBP (mm Hg) DBP (mm Hg) INITIAL 253 ± 12.0 101.6 ± 1.8 125.0 ± 1.6 90.0 ± 2.0 FINAL 258 ± 13.7 106.3 ± 2.1 129.0 ± 1.4 95.0 ± 2.2 INITIAL 257 ± 11.6 104.3 ± 1.4 121.0 ± 1.5 96.0 ± 2.1 FINAL 263 ± 13.6 134.3 ± 2.0***.C 147.0 ± 1.8***.C 128.0 ± 1.9***.C INITIAL 252 ± 12.6 104.6 ± 1.7 128.0 ± 1.3 93.0 ± 2.3 FINAL 257 ± 14.6 131.9 ± 1.9***.C 145.0 ± 1.3***.C 124.0 ± 1.6***.C C: Control group; H: Hypertensive group; EH: Exercised hypertensive group. Data are shown as means ± SEM. The statistical differences were determined by Student t tests one-way ANOVA followed by Bonferroni post-test. ***p < 0.001 initial vs final period; Cp < 0.001 vs final period of the control group. 162 Arq Bras Cardiol. 2015; 105(2):160-167 Braga da Silva et al. Acute Effects of Resistance Exercise on Smooth Muscle Original Article 125 A C H EH 75 8 50 B 7 25 pD2 % of contraction 100 6 0 5 -25 4 9 8 7 6 - Log [PHEN] M 5 4 * C H HE Figure 1 – Concentration-response curves for phenylephrine (PHEN: 10-9-10-4 M) in isolated superior mesenteric artery rings without functional endothelium (Figure 1A) obtained from rats of the groups Control (C), Hypertensive (H) and Exercised Hypertensive (EH). Figure 1B indicates means ± standard error of the mean (SEM) of pD2 of the phenylephrine induced contractions (B). Data are expressed as means ± SEM for ten experiments in each group. The statistical differences between means were determined by using two-way ANOVA followed by the Bonferroni post-test (Figure 1A) and one-way ANOVA followed by the Bonferroni post-test (Figure 1B). *p < 0.01 vs C. pD2: negative logarithm of the molar concentration of the agonist that produces 50% of maximal response. treated with L-NAME can be associated with the administration route, the drug dose, the treatment length and the type of artery studied. α-1 adrenergic receptor level, but successive resistance exercise sessions can cause a significant reduction in the contractile sensitivity promoted by PHEN. In our study, immediately after one low-intensity resistance exercise session, there was no change in the sensitivity of α-1 adrenergic receptors of rats treated with L-NAME. In healthy rats, repeated strenuous swimming sessions, rather than only one session, reduced α-1 adrenergic sensitivity in the mesenteric artery with injured endothelium25. Our results differ from those by Faria et al.11, who, after one resistance exercise session (20 x 15, 50% intensity), have shown greater attenuation of the post-exercise responses to PHEN in the tail artery with intact endothelium11. The differences in our results can be attributed to the training protocol, the experimental hypertension model, the type of artery studied and the functional endothelium preservation to assess vascular reactivity. On the other hand, a previous study of our group has demonstrated that chronic low-intensity resistance exercise (3 x 10, 50% intensity) controlled blood pressure and reduced the α-1 adrenergic sensitivity of the mesenteric artery without functional endothelium of L-NAME-induced hypertensive rats 10. This shows that one low-intensity resistance exercise session in L-NAME-induced hypertensive rats does not seem to be sufficient to make a change at the In addition, the present study assessed another mechanism that modulates smooth muscle contraction, the contractile coupling through depolarizing KCl solutions. In general, KCl produces smooth muscle vascular contraction via membrane depolarization, causing Ca 2+ inflow via voltage-dependent Ca2+ channels26. It has been reported that depolarizing KCl concentrations mediate the increase in intracellular Ca2+ concentration27. Our results indicate that animals treated with L-NAME increased smooth muscle contraction through membrane depolarization in mesenteric artery rings. Other studies with chronically L-NAME-induced animals have shown abnormal functioning of the voltage-dependent Ca2+ channels5,28. Bank et al.28 have suggested that the L-NAME-induced hypertension model increases the vascular smooth muscle tonus, and such effect is due to the reduction in NOS availability, which can lead to an increase in Ca2+ concentration or intracellular sensitivity. These findings are in accordance with our results that the increase in smooth muscle contractility found in L-NAME-induced animals can be related to the KCl-induced contractile mechanisms. Arq Bras Cardiol. 2015; 105(2):160-167 163 Braga da Silva et al. Acute Effects of Resistance Exercise on Smooth Muscle Original Article 100 C H EH % of contraction 75 *** ** 50 25 ### 0 ### -25 20 40 60 80 KCI (mM) Figure 2 – Concentration-response curves for potassium chloride (KCl: 20-80 mM) in isolated superior mesenteric artery rings without functional endothelium obtained from rats of the groups Control (C), Hypertensive (H) and Exercised Hypertensive (EH). Data are expressed as means ± standard error of the mean (SEM) for ten experiments in each group. The statistical differences between means were determined by using two-way ANOVA followed by the Bonferroni post-test. **p < 0.01 and *** p < 0.001 vs C; ###p < 0.001 vs H. It is worth noting that, when the rats in our study underwent one resistance exercise session, they had a reduction in contraction in response to depolarizing KCl solutions (20‑80 mM). That points to the possibility that resistance exercise alters in a beneficial way the depolarization of the vascular smooth muscle cells of L-NAME-induced hypertensive animals. Similarly, Chen et al.29 have shown a reduction in the contractile response to KCl (15-60 mM) in mesenteric artery rings of healthy rats after eight weeks of running training. In addition, the aortic rings of rats trained in running (10 to 12 weeks) have shown a lower contractile response to depolarizing KCl concentrations (10‑100 mM) by the end of the protocol30. So far, the effects of resistance exercise on the contractile response of the smooth muscle to depolarizing KCl solutions have not been described. The present study is the first to show the efficacy of one resistance exercise session on the decrease of smooth muscle contractility via independent mechanisms of adrenergic receptors in hypertensive rats. These results suggest that low-intensity resistance exercise, when performed for a long period, can be an important tool to fight cardiovascular disorders originating from smooth muscle contractile mechanisms. In addition, we observed that the rats treated with L-NAME had lower vasodilating sensitivity to SNP. When submitted to one resistance exercise session, they showed increased vasodilating sensitivity to NO in the smooth muscle of mesenteric artery rings. A recent study by our group has shown that the NO pathway sensitivity was decreased in L-NAME-induced hypertensive rats for eight weeks, and that chronic low-intensity resistance 164 Arq Bras Cardiol. 2015; 105(2):160-167 exercise could reverse that effect10. Acute and chronic effects of resistance exercise on the endothelium-independent vasodilating response are beneficial to vascular function in L‑NAMEinduced hypertensive rats. It is worth noting that, the study by another group conducting one resistance exercise session in spontaneously hypertensive animals has shown no changes in the SNP-induced relaxations in the vascular bed of the tail artery25. Those differences can result from the hypertension induction model and the training protocol adopted. The present study has some limitations. The first is that the results obtained are specific to hypertensive rats. The second is not having assessed the effect of resistance exercise on other arteries because there already is functional heterogeneity among the arteries of different vascular beds. The third is the lack of a healthy group undergoing exercise, which limits data extrapolation. Another point to be noted is that the resistance exercise protocol adopted in the present study has the characteristic of high volume and low intensity. That exercise characteristic is similar to aerobic exercise protocols indicated to control blood pressure1,13. Some studies have shown that moderate-intensity resistance exercise can reduce blood pressure and improve vascular function1,11,31,32. Despite those advantages, a recent meta‑analysis has indicated that high-intensity resistance exercise is associated with increased arterial stiffness in health young individuals33. In addition, the physiological mechanisms responsible for the advantages and/or disadvantages of resistance exercise on the vascular health of animals and humans are yet to be established. Braga da Silva et al. Acute Effects of Resistance Exercise on Smooth Muscle Original Article A 0 B 9 50 ## 8 *** 75 pD2 % of relaxation 25 100 C H 11 7 6 5 EH 125 * 10 9 8 7 - Log [SNP] M 6 4 H C HE Figure 3 – Concentration-response curves for sodium nitroprusside (SNP: 10-11-10-6 M) in isolated superior mesenteric artery rings without functional endothelium and pre-contracted with phenylephrine (1 µM) (Figure 3A). The rings were obtained from rats of the groups Control (C), Hypertensive (H) and Exercised Hypertensive (EH). Figure 3B indicates means ± standard error of the mean (SEM) of pD2 of the SNP-induced relaxations. Data are expressed as means ± SEM for ten experiments in each group. The statistical differences between means were determined by using two-way ANOVA followed by the Bonferroni post-test (Figure 3A) and one-way ANOVA followed by the Bonferroni post-test (Figure 1B). *p < 0.05 vs C; ***p < 0.001 vs H; ##p < 0.01 vs H. pD2: negative logarithm of the molar concentration of the agonist that produces 50% of maximal response. Conclusion The pharmacological evidence of this study showed that one resistance exercise session caused benefits to the vascular function of L-NAME-induced hypertensive animals. Those benefits involve a reduction in the contractile responses via KCl-induced cell depolarization, independent of α-1 adrenergic receptors, and higher vasodilating sensitivity to NO of the mesenteric artery smooth muscle in L-NAME-induced hypertensive rats. The vascular smooth muscle adjustments resulting from one resistance exercise session seem beneficial to control vascular tonus in hypertension. Acknowledgements We thank the Brazilian Board of Research and Technological Development (CNPq), the Coordination for the Improvement of Higher-Level-Education Personnel (Capes) and the Foundation of Support to Research and Technological Innovation of the State of Sergipe (Fapitec-SE) for financial support. Author contributions Conception and design of the research: Silva TLTB, Mota MM, Fontes MT, Bonjardim LR, Santos MRV. Acquisition of data: Silva TLTB, Araújo JES. Analysis and interpretation of the data: Silva TLTB, Mota MM, Fontes MT, Carvalho VO. Statistical analysis: Silva TLTB, Mota MM. Obtaining financing: Santos MRV. Writing of the manuscript: Silva TLTB, Mota MM, Fontes MT, Carvalho VO. Critical revision of the manuscript for intellectual content: Silva TLTB, Mota MM, Fontes MT, Bonjardim LR, Santos MRV. Supervision / as the major investigador: Silva TLTB. Potential Conflict of Interest No potential conflict of interest relevant to this article was reported. Sources of Funding This study was funded by Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq), Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (Capes) e Fundação de Apoio à Pesquisa e à Inovação Tecnológica do Estado de Sergipe (Fapitec-SE). Study Association This article is part of the thesis of Doctoral submitted by Tharciano Luiz Teixeira Braga da Silva from Programa de Pós‑Graduação em Ciências da Saúde da Universidade Federal de Sergipe (UFS). Arq Bras Cardiol. 2015; 105(2):160-167 165 Braga da Silva et al. Acute Effects of Resistance Exercise on Smooth Muscle Original Article References 1. Pescatello LS, Franklin BA, Fagard R, Farquhar WB, Kelley GA, Ray CA; American College of Sports Medicine. American College of Sports Medicine position stand. Exercise and hypertension. Med Sci Sports Exerc. 2004;36(3):533-53. 2. Török J. Participation of nitric oxide in different models of experimental hypertension. Physiol Res. 2008;57(6):813-25. 3. Dornas WC, Silva ME. Animal models for the study of arterial hypertension. J Biosci. 2011;36(4):731-7. 4. Ribeiro MO, Antunes E, de Nucci G, Lovisolo SM, Zatz R. Chronic inhibition of nitric oxide synthesis. A new model of arterial hypertension. Hypertension. 1992;20(3):298-303. 5. Ribeiro MO, Antunes E, Muscará MN, De Nucci G, Zatz R. Nifedipine prevents renal injury in rats with chronic nitric oxide inhibition. Hypertension. 1995;26(1):150-5. 18. Holécyová A, Török J, Bernátová I, Pechánová O. Restriction of nitric oxide rather than elevated blood pressure is responsible for alterations of vascular responses in nitric oxide-deficient hypertension. Physiol Res. 1996;45(4):317-21. 19. Kopincová J, Púzserová A, Bernátová I. L-NAME in the cardiovascular system - nitric oxide synthase activator? Pharmacol Rep. 2012;64(3):511-20. 20. dos Santos FM, Martins Dias DP, da Silva CA, Fazan R Jr, Salgado HC. Sympathetic activity is not increased in L-NAME hypertensive rats. Am J Physiol Regul Integr Comp Physiol. 2010;298(1):89-95. 21. Somlyo AP, Somlyo AV. Signal transduction and regulation in smooth muscle. Nature. 1994;372(6503):231-6. 6. Souza HC, Ballejo G, Salgado MC, Da Silva VJ, Salgado HC. Cardiac sympathetic overactivity and decreased baroreflex sensitivity in L-NAME hypertensive rats. Am J Physiol Heart Circ Physiol. 2001;280(2):844-50. 22. Hong E, Larios F, Gómez-Viquez NL, Huang F, Bravo G. Role of alpha adrenoceptors and nitric oxide on cardiovascular responses in acute and chronic hypertension. J Physiol Biochem. 2011;67(3):427-35. 7. Török J, Kristek F. Functional and morphological pattern of vascular responses in two models of experimental hypertension. Exp Clin Cardiol. 2001;6(3):142-8. 23. Tabernero A, Giraldo J, Vila E. Effect of NG-nitro-L-arginina-metil-ester (L-NAME) on functional and biochemical alpha 1-adrenoceptor-mediated responses in rat blood vessels. Br J Pharmacol. 1996;117(4):757-63. 8. Biancardi VC, Bergamaschi CT, Lopes OU, Campos RR. Sympathetic activation in rats with L-NAME-induced hypertension. Braz J Med Biol Res. 2007;40(3):401-8. 24. Heijenbrok FJ, Mathy MJ, Pfaffendorf M, van Zwieten PA. The influence of chronic inhibition of nitric oxide synthesis on contractile and relaxant properties of rat carotid and mesenteric arteries. Naunyn Schmiedebergs Arch Pharmacol. 2000;362(6):504-11. 9. Kuru O, Sentürk UK, Koçer G, Ozdem S, Başkurt OK, Cetin A, et al. Effect of exercise training on resistance arteries in rats with chronic NOS inhibition. J Appl Physiol (1985). 2009;107(3):896-902. 10. Araujo AJ, Santos AC, Souza KS, Aires MB, Santana-Filho VJ, Fioretto ET, et al. Resistance training controls arterial blood pressure from L-NAME induced hypertensive rats. Arq Bras Cardiol. 2013;100(4):339-46. 11. Faria Tde O, Targueta GP, Angeli JK, Almeida EA, Stefanon I, Vassallo DV, et al. Acute resistance exercise reduces blood pressure and vascular reactivity, and increases endothelium-dependent relaxation in spontaneously hypertensive rats. Eur J Appl Physiol. 2010;110(2):359-66. 12. Tamaki T, Uchiyama S, Nakano S. A weight-lifting exercise model for inducing hypertrophy in the hindlimb muscles of rats. Med Sci Sports Exerc. 1992;24(8):881-6. 13. Pescatello LS, Arena R, Riebe DW, Thompson PD. (editors). ACSM’s guidelines for exercise testing and prescription. 9th ed. Baltimore, MD: Lippincott Williams & Wilkins; 2013. 14. Fontes MT, Silva TL, Mota MM, Barreto AS, Rossoni LV, Santos MR. Resistance exercise acutely enhances mesenteric artery insulin-induced relaxation in healthy rats. Life Sci. 2014;94(1):24-9. 15. Barauna VG, Batista ML Jr, Costa Rosa LF, Casarini DE, Krieger JE, Oliveira EM. Cardiovascular adaptations in rats submitted to a resistance-training model. Clin Exp Pharmacol Physiol. 2005;32(4):249-54. 16. Menezes IA, Moreira IJ, Carvalho AA, Antoniolli AR, Santos MR. Cardiovascular effects of the aqueous extract from Caesalpinia ferrea: involvement of ATP-sensitive potassium channels. Vascul Pharmacol. 2007;47(1):41-7. 166 17. Furchgott RF, Zawadzki JV. The obligatory role of endothelial cells in the relaxation of arterial smooth muscle by acetylcholine. Nature. 1980;288(5789):373-6. Arq Bras Cardiol. 2015; 105(2):160-167 25. Chies AB, de Oliveira AM, Pereira FC, de Andrade CR, Corrêa FM. Phenylephrine-induced vasoconstriction of the rat superior mesenteric artery is decreased after repeated swimming. J Smooth Muscle Res. 2004;40(6):249-58. 26. Braunstein TH, Inoue R, Cribbs L, Oike M, Ito Y, Holstein-Rathlou NH, et al. The role of L- and T-type calcium channels in local and remote calcium responses in rat mesenteric terminal arterioles. J Vasc Res. 2009;46(2):138-51. 27. Fellner SK, Arendshorst WJ. Complex interactions of NO/cGMP/PKG systems on Ca2+ signaling in afferent arteriolar vascular smooth muscle. Am J Physiol Heart Circ Physiol. 2010;298(1):H144-51. 28. Bank N, Aynedjian HS, Khan GA. Mechanism of vasoconstriction induced by chronic inhibition of nitric oxide in rats. Hypertension. 1994;24(3):322-8. 29. Chen SJ, Wu CC, Yen MH. Exercise training activates large-conductance calcium-activated K(+) channels and enhances nitric oxide production in rat mesenteric artery and thoracic aorta. J Biomed Sci. 2001;8(3):248-55. 30. Delp MD, McAllister RM, Laughlin MH. Exercise training alters endotheliumdependent vasoreactivity of rat abdominal aorta. J Appl Physiol (1985). 1993;75(3):1354-63. 31. Fagard RH, Cornelissen VA. Effect of exercise on blood pressure control in hypertensive patients. Eur J Cardiovasc Prev Rehabil. 2007;14(1):12-7. 32. Mota MM, da Silva TL, Fontes MT, Barreto AS, Araújo JE, de Oliveira AC, et al. Resistance exercise restores endothelial function and reduces blood pressure in type 1 diabetic rats. Arq Bras Cardiol. 2014;103(1):25-32. 33. Miyachi M. Effects of resistance training on arterial stiffness: a meta-analysis. Br J Sports Med. 2013;47(6):393-6. Braga da Silva et al. Acute Effects of Resistance Exercise on Smooth Muscle Original Article Arq Bras Cardiol. 2015; 105(2):160-167 167 Back to the Cover Original Article Role Of MMP-2 and MMP-9 in Resistance to Drug Therapy in Patients with Resistant Hypertension Leandro Lacerda1, Ana Paula de Faria2, Vanessa Fontana2, Heitor Moreno2, Valéria Sandrim1 Núcleo de Pós-Graduação e Pesquisa - Santa Casa de Belo Horizonte1, Belo Horizonte, MG; Faculdade de Ciências Médicas da UNICAMP2, Campinas, SP – Brazil Abstract Background: Despite the increased evidence of the important role of matrix metalloproteinases (MMP-9 and MMP‑2) in the pathophysiology of hypertension, the profile of these molecules in resistant hypertension (RHTN) remains unknown. Objectives: To compare the plasma levels of MMP-9 and MMP-2 and of their tissue inhibitors (TIMP-1 and TIMP-2, respectively), as well as their MMP-9/TIMP-1 and MMP-2/TIMP-2 ratios, between patients with controlled RHTN (CRHTN, n = 41) and uncontrolled RHTN (UCRHTN, n = 35). In addition, the association of those parameters with clinical characteristics, office blood pressure (BP) and arterial stiffness (determined by pulse wave velocity) was evaluate in those subgroups. Methods: This study included 76 individuals diagnosed with RHTN and submitted to physical examination, electrocardiogram, and laboratory tests to assess biochemical parameters. Results: Similar values of MMP-9, MMP-2, TIMP-1, TIMP-2, and MMP-9/TIMP-1 and MMP-2/TIMP-2 ratios were found in the UCRHTN and CRHTN subgroups (p > 0.05). A significant correlation was found between diastolic BP (DBP) and MMP-9/TIMP-1 ratio (r = 0.37; p = 0.02) and DPB and MMP-2 (r = -0.40; p = 0.02) in the UCRHTN subgroup. On the other hand, no correlation was observed in the CRHTN subgroup. Logistic regression models demonstrated that MMP-9, MMP-2, TIMP-1, TIMP-2 and their ratios were not associated with the lack of BP control. Conclusion: These findings suggest that neither MMP-2 nor MMP-9 affect BP control in RHTN subjects. (Arq Bras Cardiol. 2015; 105(2):168-175) Keywords: Matrix Metalllooproteinases; Hypertension/physiopathology; Endopeptidases; Hyperaldosteronism/physiopathology. Introduction Resistant hypertension (RHTN) is a clinical condition characterized by maintenance of blood pressure (BP) levels above goal (140/90 mm Hg), despite the concurrent use of three or more antihypertensive agents of different classes. Ideally, one of these drugs should be a diuretic, and all agents should be prescribed at optimal doses [subgroup called uncontrolled RHTN (UCRHTN)]. The subgroup of resistant hypertensive patients whose BP is controlled using four or more drugs is known as controlled RHTN (CRHTN)1. Matrix metalloproteinases (MMPs), a group of zinc- and calcium-dependent endopeptidases, and their endogenous tissue inhibitors (TIMPs) are primarily responsible for stromal matrix remodeling2. Currently, some evidence has also suggested that those molecules play a role in hypertensive processes3. Mailing Address: Leandro Heleno Guimaraes Lacerda • Universidade Federal de Minas Gerais – UFMG. Rua Santa Rita do Sapucaí, 70, Vale das Palmeiras. Postal Code 35701168, Sete Lagoas, MG – Brazil E-mail: [email protected] Manuscript received September 17, 2014; revised manuscript January 21, 2015; accepted January 22, 2015. DOI: 10.5935/abc.20150060 168 Experimental hypertension studies have reported that the intima and media thickness of conduct vessels was associated with increased expression of MMP-9 and MMP‑2, and this event could be prevented with non-selective MMP inhibitor (doxycycline) treatment4,5. Previous studies have found that MMP-2 is upregulated in response to high intra-luminal pressure6, and its increased levels have been reported in the mammary arteries of hypertensive subjects7. Evidence has suggested that MMP-2 can degrade big endothelin-1, thus promoting vasoconstrictor effect8. Matrix metalloproteinases have been shown to suppress the vasodilation induced by β-agonists in hypertensive rats9. In hypertensive patients, increased MMP-9 activity may lead to degradation of elastin, while reduced TIMP-1 activity can lead to accumulation of fibrin degradation products, resulting in misdirected deposition of collagen10. These experimental studies have stimulated further investigation of MMPs and TIMPs as potential biomarkers in hypertension. The circulating concentration of these molecules may be associated with hypertension complications and prognosis, being therefore useful in clinical practice11. In addition, MMP-2, MMP-9, TIMP-1 and TIMP-2 may be directly associated with RHTN, playing a role in BP control in those patients12. Lacerda et al. Gelatinases in resistant hypertension Original Article Although plasma MMP-9, MMP-2, TIMP-1 and TIMP‑2 levels have been measured in hypertensive subjects13, these concentrations in RHTN patients are unknown. The present study is the first to compare the plasma levels of those molecules, as well as their ratios (MMP-9/TIMP-1 and MMP‑2/TIMP-2) between CRHTN and UCRHTN patients. Methods Patient population This cross-sectional study included all 76 individuals diagnosed with RHTN on regular follow-up at the Resistant Hypertension Outpatient Clinic, University of Campinas, Campinas, Brazil. Patients were classified into two subgroups, UCRHTN (n = 35) and CRHTN (n = 41), in accordance with the guidelines established by the American Heart Association14. All patients underwent physical examination, electrocardiogram, and laboratory tests to assess biochemical parameters. Patients with secondary forms of hypertension as well as renal failure, ischemic heart, liver and peripheral vascular diseases, stroke, smoking or any other serious disease were properly identified and excluded from the study. Ambulatory BP monitoring was performed (Spacelabs 90207, Spacelabs Inc, Redmond, WA, USA) to exclude pseudo‑resistant hypertension and to characterize CRHTN and UCRHTN patients. Treatment adherence was determined by pill counting (threshold of 80% or greater of the prescribed medication). This study was approved by the Research Ethics Committee at the Medical Sciences School, University of Campinas, Campinas, Brazil, and was performed in accordance with the Declaration of Helsinki. All participants were aware of the nature of the research study and signed an informed consent before enrolling in the study. The following patients’ parameters were evaluated: office BP; pulse wave velocity (PWV); plasma concentrations of MMP-9, MMP-2, TIMP-1 and TIMP-2; plasma aldosterone concentration (PAC); and plasma renin activity (PRA). Office BP measurements Systolic and diastolic BP (SBP and DBP, respectively) levels were assessed three times, using a digital sphygmomanometer (Omron HEM-711DLX, OMRON Healthcare Inc., Bannockburn, IL, USA) on the right upper arm, in the sitting position, after a 10-minute rest. The mean of two consecutive measurements was used, with a variation lower than 5 mmHg. Pulse wave velocity assessment Pulse wave velocity was measured by using the Sphygmocor System (Atcor Medical, Sydney, Australia) with the patient in the supine position15. The PWVs of the right carotid and femoral arteries were analyzed, estimating the delay with respect to the electrocardiogram wave. Distance measurements were taken between the femoral recording site and the supra-sternal notch minus the distance from the supra-sternal notch to the carotid recording site. Carotid-femoral PWV was calculated by dividing the traveled distance by transit time [PWV = distance(m)/time(s)]. At least two measurements were performed; if they differed by more than 0.5 m/s, a third measurement was taken. Laboratory assessments Blood samples for biochemical assessment were collected at 8 AM, after an overnight fasting. PAC and PRA were measured by using radioimmunoassay, with standard techniques. Plasma levels of biomarkers MMP-9 and TIMP-1 were measured by using enzyme-linked immunosorbent assay (ELISA) (R&D System®, Minneapolis, USA). Similarly, the plasma biomarkers MMP-2 and TIMP-2 were measured by using ELISA, following the manufacturer´s instructions (RayBiotech®, Georgia, USA). Statistical analyses The Statistical Analysis System, version 3.02 (GraphPad Prism Inc., 2000), and SigmaPlot version 12.0 (Systat software, Inc.) were used for all statistical analyses of the study. All values were expressed as mean ± standard deviation. The normality of distribution was assessed by using Kolmogorov–Smirnov test. The subgroups were compared by using Student´s t test or Mann-Whitney test, according to data distribution. Chi-square test was used for categorical variables. The correlation of biomarkers with clinical parameters was evaluated by using Pearson’s or Spearman´s test. Regression models were performed to test the association of variables apart from potential confounders. The level of significance accepted was 0.05. Results Table 1 shows the clinical and laboratory data of both subgroups, and Table 2 shows the plasma levels of biomarkers. As expected, increased values of SBP, DBP and PWV were found in UCRHTN as compared to CRHTN patients. No significant differences were observed regarding age, sex, body mass index (BMI) and biochemical parameters. Similar values of MMP-9, TIMP-1, MMP-2, TIMP-2, and of MMP-9/TIMP-1 and MMP-2/TIMP-2 ratios were found in the UCRHTN and CRHTN subgroups (p > 0.05; Table 2). Regarding antihypertensive medication, UCRHTN patients were taking a significantly higher number of anti-hypertensive drugs, demonstrated by the use of calcium channel blockers, as compared to controlled subjects (Table 1). Correlation analyses for the UCRHTN subgroup indicated that DBP correlated with MMP-9/TIMP-1 ratio (r = 0.37; p = 0.02); however, DBP was inversely correlated with MMP‑2 levels (r = -0.40; p = 0.02). In that subgroup, PAC and age also correlated with MMP-9/TIMP-1 ratio (r = 0.57, p < 0.001 and r = -0.37, p = 0.02, respectively), and, only in that subgroup, MMP-2 correlated with age (r = 0.42, p = 0.01). In addition, these associations remained significant after adjusting for sex and BMI included in the linear regression model [beta coefficient = 11.5, standard error (SE) = 5.5, p = 0.04; beta coefficient = -0.08, SE = 0.04, p = 0.04, respectively]. Finally, the plasma levels of the biomarkers Arq Bras Cardiol. 2015; 105(2):168-175 169 Lacerda et al. Gelatinases in resistant hypertension Original Article mentioned above did not correlate with any clinical parameter in CRHTN subjects (Table 3 and 4). Considering the entire RHTN group (n = 76), we found that (i) the MMP-9/TIMP-1 ratio was inversely associated with BMI (r = -0.25, p = 0.03), but positively with aldosterone levels (r = 0.24, p = 0.04); and (ii) MMP-2 was inversely associated with DBP (r = -0.26, p = 0.02), but positively with age (r = 0.40, p < 0.001). Finally, logistic regression models demonstrated that MMP-9 and MMP-2, their tissue inhibitors-1 and -2 and ratios were not associated with the lack of BP control (data not shown) in RHTN when adjusting for sex, age and BMI. the RHTN population. Interestingly, correlations of DBP and age with the MMP-9/TIMP-1 ratio and DBP and MMP-2 were observed only in the UCRHTN subgroup. Plasma aldosterone levels and age also correlated with the MMP‑9/TIMP-1 ratio in UCRHTN. In this context, as previously demonstrated 1,16,17 , the idea of several important differences in the pathophysiology of the RHTN subgroups should be reinforced. However, no association of the biomarkers with SBP was found, probably because DBP is a more stable variable than the systolic component. Under physiological conditions, balance between MMPs and TIMPs exists. On the other hand, in pathological processes, such as hypertension, an MMPs/TIMPs ratio imbalance contributes to the excessive degradation of extracellular matrix (ECM) proteins18, and results in pathological vascular Discussion This is the first study to analyze the association of the biomarkers MMP-2 and MMP-9 with BP levels in Table 1 – General characteristics of the resistant hypertension (RHTN) subgroups Female gender (%) UCRHTN (n = 35) CRHTN (n = 41) 63 66 Age (years)* 57 ± 11 61 ± 9 BMI (Kg/m2) 30.0 ± 4.4 30.1 ± 4.4 SBP (mm Hg)* 158 ± 20 136 ± 14 DBP (mm Hg)* 91 ± 14 80 ± 7 PWV (m/s) * 11.9 ± 1.8 10.6 ± 1.3 Total cholesterol (mg/dL) 203 ± 50 202 ± 39 LDL (mg/dL) 126 ± 38 125 ± 35 HDL (mg/dL) 44 ± 12 48 ± 14 Triglycerides (mg/dL) Urea (mg/dL) Creatinine (mg/dL) Fasting glucose (mg/dL) Uric acid (mg/dL) 160 ± 96 149 ± 66 38.1 ± 11.8 35.9 ± 7.5 1.0 ± 0.2 0.9 ± 0.2 125.4 ± 54.1 106.7 ± 34.2 5.9 ± 1.6 5.8 ± 1.5 Aldosterone (pg/mL) * 109.7 ± 82.0 101.1 ± 70.5 Renin (pg/mL) 22.4 ± 19.6 21.2 ± 18.2 4.6 ± 0.9 4.2 ± 0.9 Antihypertensive drugs Total number (daily) * Spironolactone (%) 43 37 Diuretics (%) 100 100 Beta-blockers (%) 69 68 ACEI (%) 46 29 ARB (%) 54 51 CCB (%)* 97 68 Centrally acting anti-hypertensive (%) 37 17 UCRHTN: Uncontrolled resistant hypertension; CRHTN: Controlled resistant hypertension; BMI: Body mass index; SBP: Systolic blood pressure; DBP: Diastolic blood pressure; PWV: Pulse wave velocity; LDL: Low density lipoprotein; HDL: High density lipoprotein; ACEI: Angiotensin-converting-enzyme inhibitors; ARB: Angiotensin II receptor blockers; CCB: Calcium channel blockers. Values are expressed as mean ± SD or percentage. * p < 0.05 between groups. 170 Arq Bras Cardiol. 2015; 105(2):168-175 Lacerda et al. Gelatinases in resistant hypertension Original Article Table 2 – Characteristics of biomarkers in resistant hypertension (RHTN) subgroups UCRHTN (n = 35) CRHTN (n = 41) MMP-9 (ng/mL) 253 ± 134 225 ± 121 TIMP-1 (ng/mL) 499 ± 406 407 ± 249 MMP-9/TIMP-1 Ratio 0.68 ± 0.45 0.77 ± 0.59 330 ± 71 312 ± 69 Biomarkers MMP-2 (ng/mL) TIMP-2 (ng/mL) 306 ± 132 339 ± 184 MMP-2/TIMP-2 Ratio 1.31 ± 0.79 1.24 ± 0.78 UCRHTN: Uncontrolled resistant hypertension; CRHTN: Controlled resistant hypertension; MMP-9: Matrix metalloproteinase-9; TIMP-1: Tissue inhibitor MMP-1; MMP‑2: Matrix metalloproteinase-2; TIMP-2: Tissue inhibitor MMP-2. Values are expressed as mean ± SD or percentage. * p < 0.05 between groups. Table 3 – Correlation among clinical parameters and MMP-9, TIMP-1 and MMP-9/TIMP-1 Groups CRHTN Biomarkers SBP DBP PWV MMP-9 0.23 (0.14) 0.06 (0.67) 0.06 (0.66) TIMP-1 0.03 (0.85) 0.12 (0.44) -0.06 (0.67) r (p-value) MMP-9/TIMP-1 Ratio 0.07 (0.64) -0.12 (0.42) -0.02 (0.86) MMP-9 0.04 (0.82) 0.14 (0.41) -0.03 (0.82) UCRHTN TIMP-1 -0.23 (0.17) -0.33 (0.05) -0.07 (0.68) r (p-value) MMP-9/TIMP-1 Ratio 0.15 (0.38) 0.37 (0.02*) 0.02 (0.91) Data are expressed as correlation coefficient (p-value). CRHTN: Controlled resistant hypertension; UCRHTN: Uncontrolled resistant hypertension; SBP: Systolic blood pressure; DBP: Diastolic blood pressure, PWV: Pulse wave velocity. *p < 0.05. Table 4 – Correlation among clinical parameters and MMP-2, TIMP-2 and MMP-2/TIMP-2 Groups CRHTN Biomarkers SBP DBP PWV MMP-2 -0.01 (0.93) 0.02 (0.88) -0.09 (0.54) TIMP-2 -0.14 0.25) -0.03 (0.83) 0.04 (0.77) r (p-value) MMP-2/TIMP-2 Ratio 0.23 (0.13) 0.04 (0.75) -0.24 (0.12) MMP-2 -0.21 (0.20) -0.40 (0.02*) 0.18 (0.29) UCRHTN TIMP-2 0.21 (0.21) -0.01 (0.97) 0.03 (0.85) r (p-value) MMP-2/TIMP-2 Ratio -0.26 (0.11) -0.28 (0.09) 0.06 (0.72) Data are expressed as correlation coefficient (p-value). CRHTN: Controlled resistant hypertension; UCRHTN: Uncontrolled resistant hypertension; SBP: Systolic blood pressure; DBP: Diastolic blood pressure, PWV: Pulse wave velocity. *p < 0.05. remodeling19. Therefore, the MMP-9/TIMP-1 ratio might be a better indicator of that process. Taken together, MMP-9/TIMP-1 ratio in association with DBP levels in UCRHTN could strengthen the importance of some different phenotypes in the pathophysiology of uncontrolled patients. Inconsistent results have been found about the levels of gelatinases (MMP-2 and MMP-9) in essential hypertension3. However, our study differs from this previous finding in evaluating gelatinases and their inhibitors in RHTN. It is well known that RHTN is associated with increased cardiovascular risk20, but uncontrolled hypertensive patients are probably exposed to increased cardiovascular risk, which may reflect in a worse prognosis as compared to controlled subjects. Moreover, our study found an inverse correlation between MMP-2 and DBP in the UCRHTN subgroup, suggesting no association between MMP-2 and BP control in that subgroup. Matrix metalloproteinases are zinc- dependent endopeptidases, with that ion in the active site. Likewise, the angiotensin‑ converting ‑ enzyme (ACE) is also zinc‑dependent and inhibited by ACE inhibitors, which are widely used in current antihypertensive treatment. Given this, MMP-9 may also be inhibited by ACE inhibitors by binding with zinc in the active site21; this suggests that treatment with ACE inhibitors may inhibit MMP-9 activity22. Arq Bras Cardiol. 2015; 105(2):168-175 171 Lacerda et al. Gelatinases in resistant hypertension Original Article Although high MMP-9 levels were expected in the UCRHTN subgroup, this negative finding may be explained by the fact that all RHTN individuals have the hypertensive disease for a long time and take a great number of antihypertensive drugs, which could cause the decrease in MMP-9 activity, particularly related to the use of ACE inhibitors, as evidenced by several studies21,22. For example, some studies have evaluated the relationship between MMP-9 and TIMP-1 in patients with essential hypertension, and have shown that, after antihypertensive treatment, the circulating levels of those molecules were significantly higher in subjects with hypertension than in normotensive controls. In some cases, a reduction in plasma levels of MMP-9 and consequent increased levels of TIMP-1 have occurred after antihypertensive treatment 23. Other findings are as follows: MMP changes in TIMP profile, which favor decreased ECM degradation (decreased MMP-2, MMP-9 and MMP-13 and increased TIMP-1), are associated with left ventricular hypertrophy and diastolic dysfunction; and increased TIMP-1 predicted the presence of chronic heart failure11. In addition, significantly higher TIMP-1 levels have been reported in hypertensive individuals as compared with normotensive individuals; however, TIMP-1 levels are not elevated in hypertension alone, but only in patients with diastolic dysfunction and fibrosis. This suggests that TIMP-1 synthesis and release are independent of BP and probably dependent on a variety of neurohormonal factors, being a TIMP-1 level higher than 500 ng/mL an accurate indicator of dysfunction diastolic and damage to target organs24. One hypothesis to be raised about the increase of plasma levels of TIMP-1 is to generate a response to modulate or limit collagen degradation, thus contributing to the development of arterial stiffness. Unlike MMP-9, some studies indicate an increase of TIMP-1 after antihypertensive treatment10,23,24. In contrast, some studies have reported that increased TIMP-1 levels were associated with an increased incidence of hypertension and risk of BP progression25. Other studies have shown the increase of TIMP-1 in normotensive vs. hypertensive subjects26, as well as unchanged27 or decreased TIMP-128. In addition, TIMPs play an important role in cardiovascular remodeling processes, regardless of their MMP inhibitory activity, ie, such inhibitors may play an important role in BP, irrespective of the action of MMPs23. Pulse wave velocity is widely used as an arterial elasticity and stiffness index, and the arterial wall properties, such as thickness and lumen diameter, are the factors that most influence PWV29. Pulse wave velocity is the gold standard method to measure arterial stiffness, plays an essential role in the pathophysiology of hypertension and predicts mortality in patients with hypertension30. The mechanisms involved in arterial stiffness are not completely understood; however, evidence has shown that this process is accompanied by complex mechanisms, including structural alterations of the ECM, including the participation of MMPs. In our study, the levels of gelatinases and TIMPs were not correlated with PWV values. These negative findings may be related to 172 Arq Bras Cardiol. 2015; 105(2):168-175 vascular stiffness in RHTN, as previously shown31. In addition, the stiffness of great arteries appears to be an inevitable consequence of aging, ie, this process becomes more pronounced at older ages, which, according to the authors, is the most important determinant of arterial stiffness1. In this study, the arterial stiffness process may have been completed or lost, because the individuals were in advanced age, which is directly related to the increase in PWV and pulse pressure (PP), especially in the UCRHTN group. This may be an explanation for the lack of correlation of the biomarkers studied with PWV and PP. Primary aldosteronism is the second most common cause of RHTN 32 . This condition is characterized by excessive secretion of aldosterone by the adrenal gland, the major forms being the production of adenomas and idiopathic hyperaldosteronism33,34. It is noteworthy that patients with RHTN have increased aldosterone levels, but that is not due to primary aldosteronism. Previous works have shown that UCRHTN individuals have higher PAC as compared to CRHTN individuals1. A study of 88 consecutive patients with RHTN has reported a 20% incidence of primary aldosteronism, defined by measuring two parameters: PRA and urinary aldosterone concentration35. Consistent with these findings, other medical centers have reported a 17%–22% prevalence of primary aldosteronism in RHTN patients36,37. High PAC leads to the remodeling of small and large arteries, causing collagen synthesis, which results in increased arterial stiffness and BP elevation38. Although we found a positive correlation between PAC and MMP-9/TIMP-1 ratio, hyperaldosteronism is known to be an independent risk factor in arterial hypertension and, thus, in the process of arterial stiffening32. The main limitation of this study was the small number of UCRHTN and CRHTN patients enrolled. This study’s sample size was not calculated, because all 76 subjects on regular follow-up at the Resistant Hypertension Outpatient Clinic were included. Similarly, recent studies have demonstrated important findings, including in CRHTN and UCRHTN, with such a small population16,17,39. On the other hand, the lack of association in the main findings may be attributed to low statistical power or type II error. Moreover, antihypertensive drugs can influence the levels of MMP-9, as demonstrated by Fontana et al. 13 and other studies previously cited. Multiple linear regression analyses was performed to predict biomarkers (MMP-2, MMP-9, TIMP-1, TIMP-2, and their ratios) adjusted for antihypertensive drugs. These regression models indicated that only the beta-blocker use was a predictor of TIMP-1 levels and of MMP-9/TIMP-1 ratio in all RHTN subjects. However, this potential confounding factor did not affect our findings, because both controlled and uncontrolled subgroups had a similar proportion of beta-blocker use. Because of ethical concerns, antihypertensive drugs could not be withdrawn in the RHTN subjects to exclude the influence of those medications on the plasma levels of biomarkers. Conclusion Briefly, although MMP-9/TIMP-1 ratio and MMP-2 were associated with DBP levels, aldosterone and age in the Lacerda et al. Gelatinases in resistant hypertension Original Article UCRHTN subgroup, this does not seem to influence resistance to antihypertensive therapy, because the biomarkers did not predict the lack of BP control in RHTN. Future prospective studies with a larger RHTN population should be carried out to confirm the present study’s findings. Acknowledgements This study was supported by the State of Minas Gerais Research Foundation (FAPEMIG), the State of São Paulo Research Foundation (FAPESP) and the Brazilian National Council for Scientific and Technological Development (CNPq). Author contributions Conception and design of the research:Moreno Júnior H, Sandrim VC. Acquisition of data:Lacerda LHG, Sandrim VC. Analysis and interpretation of the data: Faria AP, Moreno Júnior H, Sandrim VC. Statistical analysis: Faria AP, Sandrim VC. Obtaining financing: Moreno Júnior H, Sandrim VC. Writing of the manuscript:Lacerda LHG, Faria AP, Sandrim VC. Critical revision of the manuscript for intellectual content: Lacerda LHG, Faria AP, Fontana V, Moreno Júnior H, Sandrim VC. Potential Conflict of Interest No potential conflict of interest relevant to this article was reported. Sources of Funding This study was funded by FAPEMIG, FAPESP e CNPq. Study Association This article is part of the thesis of master submitted by Leandro Heleno Guimarães Lacerda, from Instituto de Ensino e Pesquisa da Santa Casa de Belo Horizonte. References 1. Martins LC, Figueiredo VN, Quinaglia T, Boer-Martins L, Yugar-Toledo JC, Martin JF, et al. Characteristics of resistant hypertension: ageing, body mass index, hyperaldosteronism, cardiac hypertrophy and vascular stiffness. J Hum Hypertens. 2011;25(9):532-8. 2. Nagase H, Visse R, Murphy G. Structure and function of matrix metalloproteinases and TIMPs. Cardiovasc Res..2006;69(3):562-73. 3. Fontana V, Silva PS, Gerlach RF, Tanus-Santos JE. Circulating matrix metalloproteinases and their inhibitors in hypertension. Clin Chim Acta. 2012; 413(7-8):656-62. 4. Castro MM, Rizzi E, Prado CM, Rossi MA, Tanus-Santos JE, Gerlach RF. Imbalance between matrix metalloproteinases and tissue inhibitor of metalloproteinases in hypertensive vascular remodeling. Matrix Biol. 2010;29(3):194-201. 5. Hansson J, Vasan RS, Arnlov J, Ingelsson E, Lind L, Larsson A, et al. Biomarkers of extracellular matrix metabolism (MMP-9 and TIMP-1) and risk of stroke, myocardial infarction, and cause-specific mortality: cohort study. PLoS One. 2011;6(1):e16185. 6. Lehoux S, Lemarie CA, Esposito B, Lijnen HR, Tedgui A. Pressure-induced matrix metalloproteinase-9 contributes to early hypertensive remodeling. Circulation. 2004;109(8):1041-7. 7. Chung AW, Booth AD, Rose C, Thompson CR, Levin A, van Breemen C. Increased matrix metalloproteinase 2 activity in the human internal mammary artery is associated with ageing, hypertension, diabetes and kidney dysfunction. J Vasc Res. 2008;45(4):357-62. 8. Fernandez-Patron C, Radomski MW, Davidge ST. Vascular matrix metalloproteinase -2 cleaves big endothelin-1 yielding a novel vasoconstrictor. Circ Res. 1999;85(10):906-11. 9. Chow AK, Cena J, Schulz R. Acute actions and novel targets of matrix metalloproteinases in the heart and vasculature. Br J Pharmacol. 2007;152(2):189-205. 10. Onal IK, Altun B, Onal ED, Kirkpantur A, Gul Oz S, Turgan C. Serum levels of MMP-9 and TIMP-1 in primary hypertension and effect of antihypertensive treatment. Eur J Intern Med. 2009;20(4):369-72. 11. Ahmed SH, Clark LL, Pennington WR, Webb CS, Bonnema DD, Leonardi AH, et al. Matrix metalloproteinases/tissue inhibitors of metalloproteinases: relationship between changes in proteolytic determinants of matrix composition and structural, functional, and clinical manifestations of hypertensive heart disease. Circulation. 2006;113(17):2089-96. 12. Zhou S, Feely J, Spiers JP, Mahmud A. Matrix metalloproteinase-9 polymorphism contributes to blood pressure and arterial stiffness in essential hypertension. J Hum Hypertens. 2007;21(11):861-7. 13. Fontana V, Silva PS, Belo VA, Antonio RC, Ceron CS, Biagi C, et al. Consistent alterations of circulating matrix metalloproteinases levels in untreated hypertensives and in spontaneously hypertensive rats: a relevant pharmacological target. Basic Clin Pharmacol Toxicol. 2011 Aug;109(2):130-7. 14. Calhoun DA, Jones D, Textor S, Goff DC, Murphy TP, Toto RD, et al. Resistant hypertension: diagnosis, evaluation, and treatment: a scientific statement from the American Heart Association Professional Education Committee of the Council for High Blood Pressure Research. Circulation. 2008;117(25):e510-26. 15. Laurent S, Cockcroft J, Van Bortel L, Boutouyrie P, Giannattasio C, Hayoz D, et al. Expert consensus document on arterial stiffness: methodological issues and clinical applications. Eur Heart J. 2006;27(21):2588-605. 16. Sabbatini AR, Faria AP, Barbaro NR, Gordo WM, Modolo RG, Pinho C, et al. Deregulation of adipokines related to target organ damage on resistant hypertension. J Hum Hypertens. 2014;28(6):388-92. 17. de Faria AP, Demacq C, Figueiredo VN, Moraes CH, Santos RC, Sabbatini AR, et al. Hypoadiponectinemia and aldosterone excess are associated with lack of blood pressure control in subjects with resistant hypertension. Hypertens Res. 2012;36(12):1067-72. 18. Murphy G, Nagase H. Progress in matrix metalloproteinase research. Mol Aspects Med. 2008;29(5):290-308. 19. Sluijter JP, de Kleijn DP, Pasterkamp G. Vascular remodeling and protease inhibition--bench to bedside. Cardiovasc Res. 2006;69(3):595-603. 20. Pierdomenico SD, Lapenna D, Bucci A, Di Tommaso R, Di Mascio R, Manente BM, et al. Cardiovascular outcome in treated hypertensive patients with responder, masked, false resistant, and true resistant hypertension. Am J Hypertens. 2005;18(11):1422-8. 21. Sorbi D, Fadly M, Hicks R, Alexander S, Arbeit L. Captopril inhibits the 72 kDa and 92 kDa matrix metalloproteinases. KidneyInt 1993;44(6):1266-72. Arq Bras Cardiol. 2015; 105(2):168-175 173 Lacerda et al. Gelatinases in resistant hypertension Original Article 22. Inoue N, Takai S, Jin D, Okumura K, Okamura N, Kajiura M, et al. Ef fe c t of ang io t en sin - c o nver t ing en z y m e inhibi t o r o n mat r i x met alloproteinase-9 ac tivit y in patient s with Kawasaki disease. Clin Chim Acta. 2010;411(3-4):267-9. 23. Tayebjee MH, Nadar SK, MacFadyen RJ, Lip GY. Tissue inhibitor of metalloproteinase-1 and matrix metalloproteinase-9 levels in patients with hypertension Relationship to tissue Doppler indices of diastolic relaxation. Am J Hypertens. 2004;17(9):770-4. 24. Lindsay MM, Maxwell P, Dunn FG. TIMP-1: a marker of left ventricular diastolic dysfunction and fibrosis in hypertension. Hypertension. 2002;40(2):136-41. 25. Dhingra R, Pencina MJ, Schrader P, Wang TJ, Levy D, Pencina K, et al. Relations of matrix remodeling biomarkers to blood pressure progression and incidence of hypertension in the community. Circulation. 2009;119(8):1101-7. 26. Ta n J, H u a Q , X i n g X , We n J, L i u R , Ya n g Z . I m p a c t o f t h e metalloproteinase-9/tissue inhibitor of metalloproteinase-1 system on large arterial stiffness in patients with essential hypertension. Hypertension Res. 2007;30(10):959-63. 27. Visscher DW, Hoyhtya M, Ottosen SK, Liang CM, Sarkar FH, Crissman JD, et al. Enhanced expression of tissue inhibitor of metalloproteinase-2 (TIMP‑2) in the stroma of breast carcinomas correlates with tumor recurrence. Int J Cancer. 1994;59(3):339-44. 28. Korem S, Kraiem Z, Shiloni E, Yehezkel O, Sadeh O, Resnick MB. Increased expression of matrix metalloproteinase-2: a diagnostic marker but not prognostic marker of papillary thyroid carcinoma. Isr Med Assoc J (IMAJ). 2002;4(4):247-51. 29. Safar ME, Henry O, Meaume S. Aortic pulse wave velocity: an independent marker of cardiovascular risk. Am J Geriatr Cardiol;11(5):295-8. 30. Laurent S, Boutouyrie P, Asmar R, Gautier I, Laloux B, Guize L, et al. Aortic stiffness is an independent predictor of all-cause and 174 Arq Bras Cardiol. 2015; 105(2):168-175 cardiovascular mortality in hypertensive patients. Hypertension. 2001;37(5):1236-41. 31. Figueiredo VN, Yugar-Toledo JC, Martins LC, Martins LB, de Faria AP, de Haro Moraes C, et al. Vascular stiffness and endothelial dysfunction: Correlations at different levels of blood pressure. Blood Press. 201;21(1):31-8. 32. Umpierrez GE, Cantey P, Smiley D, Palacio A, Temponi D, Luster K, et al. Primary aldosteronism in diabetic subjects with resistant hypertension. Diabetes Care. 2007;30(7):1699-703. 33. Mulatero P, Dluhy RG, Giacchetti G, Boscaro M, Veglio F, Stewart PM. Diagnosis of primary aldosteronism: from screening to subtype differentiation. Trends in endocrinology and metabolism. Trends Endocrinol Metab. 2005;16(3):114-9. 34. Mulatero P, Stowasser M, Loh KC, Fardella CE, Gordon RD, Mosso L, et al. Increased diagnosis of primary aldosteronism, including surgically correctable forms, in centers from five continents. J Clin Endocrinol Metab. 2004;89(3):1045-50. 35. Calhoun DA, Nishizaka MK, Zaman MA, Thakkar RB, Weissmann P. Hyperaldosteronism among black and white subjects with resistant hypertension. Hypertension. 2002; 40(6): 892–6. 36. Eide IK, Torjesen PA, Drolsum A, Babovic A, Lilledahl NP. Low-renin status in therapy-resistant hypertension: a clue to efficient treatment. J Hypertens. 2004; 22(11): 2217–26. 37. Strauch B, Zelinka T, Hampf M, Bernhardt R, Widimsk J Jr. Prevalence of primary hyperaldosteronism in moderate to severe hypertension in the Central Europe region. J Hum Hypertens 2003; 17(5): 349–52. 38. Duprez DA. Aldosterone and the vasculature: mechanisms mediating resistant hypertension. J Clin Hypertens (Greenwich) 2007; 9(1 Suppl 1): 13–8. 39. de Haro Moraes C, Figueiredo VN, de Faria AP, Barbaro NR, Sabbatini AR, Quinaglia T, et al. High-circulating leptin levels are associated with increased blood pressure in uncontrolled resistant hypertension. J Hum Hypertens. 2013;27(4):225-30. Lacerda et al. Gelatinases in resistant hypertension Original Article Arq Bras Cardiol. 2015; 105(2):168-175 175 Back to the Cover Original Article Reduced Progression of Cardiac Allograft Vasculopathy with Routine Use of Induction Therapy with Basiliximab Ricardo Wang1,2, Lidia Ana Zytynski Moura1,2, Sergio Veiga Lopes2, Francisco Diniz Affonso da Costa1,2, Newton Fernando Stadler Souza Filho1, Tiago Luiz Fernandes1, Natália Boing Salvatti1, José Rocha Faria-Neto2 Santa Casa de Curitiba1; Pontifícia Universidade Católica do Paraná2, Curitiba, PR - Brazil Abstract Background: Cardiac allograft vasculopathy (CAV) is a major limitation for long-term survival of patients undergoing heart transplantation (HT). Some immunosuppressants can reduce the risk of CAV. Objectives: The primary objective was to evaluate the variation in the volumetric growth of the intimal layer measured by intracoronary ultrasound (IVUS) after 1 year in patients who received basiliximab compared with that in a control group. Methods: Thirteen patients treated at a single center between 2007 and 2009 were analyzed retrospectively. Evaluations were performed with IVUS, measuring the volume of a coronary segment within the first 30 days and 1 year after HT. Vasculopathy was characterized by the volume of the intima of the vessel. Results: Thirteen patients included (7 in the basiliximab group and 6 in the control group). On IVUS assessment, the control group was found to have greater vessel volume (120–185.43 mm3 vs. 127.77–131.32 mm3; p = 0.051). Intimal layer growth (i.e., CAV) was also higher in the control group (27.30–49.15 mm3 [Δ80%] vs. 20.23–26.69 mm3 [Δ33%]; p = 0.015). Univariate regression analysis revealed that plaque volume and prior atherosclerosis of the donor were not related to intima growth (r = 0.15, p = 0.96), whereas positive remodeling was directly proportional to the volumetric growth of the intima (r = 0.85, p < 0.001). Conclusion: Routine induction therapy with basiliximab was associated with reduced growth of the intima of the vessel during the first year after HT. (Arq Bras Cardiol. 2015; 105(2):176-183) Keywords: Vascular Diseases/physiopathology; Heart Transplantation; Antibodies, Monoclonal, Murine-Derived/admininstration & dosage; Immunosuppressive Agents. Introduction With increased survival among heart transplantation (HT) patients, mainly due to improvements in immunosuppression, the incidence of late complications, including cardiac allograft vasculopathy (CAV)1, has increased. CAV is characterized by progressive obliteration of vessels due to intimal proliferation and is considered a major cause of graft dysfunction in the first year after HT and the second most common cause of long-term death2. Lymphocytes play an important role in both acute and chronic graft rejection. The immunological and non‑immunological factors implicated in the pathogenesis of CAV converge by activating T lymphocytes (TL)3, as demonstrated by Nagano et al.4. Animal models in which these cells were blocked did not develop vasculopathy5. Thus, T lymphocyte blockade has been the objective of therapies for the prevention of CAV6. Mailing Address: Ricardo Wang • Avenida Francisco Sales 1111, Santa Efigênia, Postal Code 30150-221, Belo Horizonte, MG - Brazil. E-mail: [email protected]; [email protected] Manuscript received September 29, 2014; revised manuscript January 28, 2015; accepted January 29, 2015 DOI: 10.5935/abc.20150063 176 Basiliximab is a chimeric antibody receptor antagonist of interleukin 2 (IL-2) and is indicated in induction therapy for patients at high risk of rejection after organ transplantation7. IL-2 is a potent immunomodulator that plays an important role in the activation and maintenance of the immune response and lymphocyte proliferation8; furthermore, it is a key step in the development of acute rejection9. Blockage of TL proliferation and reduced acute rejection can delay the onset of CAV10. The aim of this study was to determine whether blockage of IL-2 with basiliximab early in the transplantation process has an effect superior to placebo in decreasing the growth of the vessel intima during the first year following HT. Methods We conducted a retrospective analysis of the database from a single center, including patients who underwent HT from September 2007 through March 2009. The patients were separated in two groups according to the induction therapy: those treated with basiliximab (Simulect®; Novartis, NJ, USA) and those who received no induction therapy (control group). In our institution the use of basiliximab became routine in July 2008; therefore, a comparison was made to a series of cases before and after Wang et al. Basiliximab and graft vasculopathy Original Article this period. In this period, there was no difference regarding surgical technique, preservation, or other adjuvant medications. We included only patients who had clinical and ultrasound follow-up for at least 1 year. We excluded patients who did not comply with intravascular ultrasound (IVUS) follow-up or whose images in the database were inadequate to allow such analysis. The study was approved by local Ethics Committee (protocol 0005154/11). Endpoints The primary objective was to compare the two groups with regard to volumetric growth of the intimal layer measured by IVUS after 1 year. The secondary objective was to evaluate the remodeling of the vessel and lumen volume and donor atherosclerosis. Immunosuppression protocol Immunosuppression was performed in the basiliximab group at a dose of 20 mg IV, together with 500 mg methylprednisolone in three daily doses and 150 mg mycophenolate mofetil (MMF) in two doses on the day of transplantation; on the fifth day, another dose of 20 mg IV basiliximab was administered; on that day, therapy with cyclosporine was initiated. In the control group, immunosuppression was conducted with methylprednisolone and MMF at the same dosage; in addition, cyclosporine was initiated on the day of transplantation at the same dosage. Evaluation of vasculopathy As part of the HT protocol, patients are routinely evaluated with angiography and intracoronary ultrasound (IVUS) only at the left anterior descending (LAD) artery. This evaluation is performed 30 days after HT and then repeated annually. Coronary angiography and IUVS were performed concurrently with an endomyocardial biopsy. To perform the procedure, a 6F introducer was introduced into the femoral artery, followed by catheterization of the left coronary artery. Unfractionated heparin (100 IU/kg) was instilled intravenously together with an intracoronary dose of isosorbide mononitrate (10 mg). The ultrasound examination was performed with an Atlantis® catheter (Boston Scientific Scimed Inc., Maple Grove, Minn.) and a 4.3 Fr catheter with a 40-MHz transducer. The IVUS catheter was positioned in the distal LAD artery; automatic pullback was performed with a velocity of 1 mm/s and an acquisition rate of 30 frames/s. The images were stored on a compact disk and analyzed using ILab® software (Boston Scientific Scimed, Inc.). IVUS Analysis To provide monitoring of the same segment, a 10-mm segment was selected just after the output of the first diagonal. Segment analysis was methodologically validated in a manner similar to that previously described11,12. Analysis was performed on the first computed tomography (CT) slice after the departure of the diagonal branch, marking the beginning of the segment; then each image is evaluated every 30 cuts (1-mm interval between analyses), until 10 segment images (10 mm) are completed. The analysis consists of a manual outlining of the lumen and external elastic membrane (EEM), calculating the lumen area and EEM area. Measurements were performed as standardized by the American College of Cardiology/European Society of Cardiology13. The intimal area was calculated by subtracting the area of the lumen minus EEM. Calculation of the volume of the vessel lumen and intima was carried out using the method described by Simpson11. The volume percent was calculated according the following formula: {∑ (EEM area − lumen area)/∑ EEem area × 100. Statistical Analysis Continuous data were expressed as median plus 25th and 75 percentiles. Categorical data were expressed as absolute numbers. Nonparametric tests were used to evaluate differences in continuous data, and due to the small sample size, we used Mann–Whitney test for evaluation of the differences in IVUS findings. A simple linear regression model was used to assess the relationship between previous atherosclerosis and intimal growth as well as the relationship between intimal and vessel growth after 1 year, using Pearson correlation coefficients. For categorical data, the differences were evaluated using Fisher's exact test. A two sided p-value < 0.05 was required for statistical significance. Analyses were performed with SPSS 12.0 software (Chicago, IL, USA). th Results In the period from 2007–2009, 23 HTs were performed in our institution. Two patients died during the perioperative period, and three during the first year of follow-up. Two patients were excluded from the present study due to inadequate IVUS images, and 3 patients only underwent IVUS study beyond 13 months of follow-up. We evaluated 13 patients, of whom 7 received basiliximab (basiliximab group) and 6 did not (control group). Demographic data are listed in Table 1. The patients were predominantly male (n = 10); the median age was 55 years in the basiliximab group and 47.5 years in the control group. Three patients in the control group developed acute renal failure in the postoperative period, characterized by a serum creatinine > 0.5 mg/dL, whereas no patients in the basiliximab group developed this complication. The levels of total cholesterol, triglycerides, and angiotensin receptors were similar between the groups (p = NS), and creatinine levels were somewhat higher in the control group. The use of inhibitors and statins was higher in the basiliximab group. Only a few patients received everolimus/sirolimus during follow‑up: one in the basiliximab group and two in the control group. However, all patients received mycophenolate mofetil. No patient received a diagnosis of cytomegalovirus confirmed by serology. The number of rejection episodes was similar in both groups. Two patients in the basiliximab group and three in the control group underwent a biopsy with 2R; they required hospitalization and underwent pulse therapy with intravenous corticosteroids. Coronary angiography performed during the first year following HT did not detect the presence of significant vascular disease (e.g., CAV), based on the new classification of the International Society of Heart and Lung Transplantation (ISHLT)14. The data obtained by IVUS are presented in Table 2 Arq Bras Cardiol. 2015; 105(2):176-183 177 Wang et al. Basiliximab and graft vasculopathy Original Article Table 1 – Patient demographics Basiliximab group (n = 7) Control group (n = 6) p value Male sex (n) 4 6 N.S. * Age (years) 55 [40-65] 47.5 [40-59] N.S. Diabetes mellitus 3 2 N.S. Renal failure after transplantation 0 3 N.S. Rejection 6 6 N.S. 0R 2 1 N.S. 1R 3 2 N.S. 2R 2 3 N.S. 7 6 N.S. Biopsy (during first year after transplantation) Coronary angiography ISHLT CAV0 † Total cholesterol (mg/dL) 229 [179-243] 180 [152-249] N.S. Triglycerides (mg/dL) 223 [176-450] 150 [129.2-232] N.S. HDL (md/dL) 48 [36-52] 38 [28-44] N.S. Glucose 85 [83-98] 93 [82-105] N.S. 1.2 [1.2-1.4] 1.6 [1.4-1.6] N.S. Prednisone 6 5 N.S. MMF 7 6 N.S. Cyclosporine 6 5 N.S. Everolimus/rapamicin 1 2 N.S. Statin 4 1 N.S. Angiotensin converting enzyme inhibitor 6 4 N.S. Insulin 0 1 N.S. Creatinine Imunossupressor: N.S. Other medications * N.S.: Not significant; † ISHLT CAV0: International Society of Heart Lung Transplantation definition of cardiac allograft vasculopathy (reference: JHLT 2010;29(7):717‑727.); MMF: Mycophenolate mofetil. Table 2 – Analysis of volumes obtained with IVUS Vessel Previous Vessel after Lumen previous Intima previous Intima after Basiliximab group 131.32 [101.69;202.06] 127.77 [110.39;174.05] 113.22 [82.67;144.70] 99.23 [87.86;123.36] 20.23 [9.65;29.11] 26.69 [14.65;39.24] Control group 120.77 [111.92;191.57] 185.43 [142.23;229.76] 103.31 [86.52;149.16] 134.96 [105.50;158.79] 27.30 [13.65;42.41] 4915 [39.76;82.89] 1.00 0.042 1.00 0.05 0.62 0.05 p value and Graph 1. In the control group, vessel volume (delineated by the EEM) exhibited positive remodeling (increase in volume growth of 49.39 mm3), whereas in the basiliximab group, the effect was reversed (negative remodeling: –4.17 mm3), with a trend toward statistical significance (p = 0.051). The findings were similar with regard to luminal volume (-11.53 × 17.3 mm3; p = 0.051). Regarding the intimal layer (plate), a higher rate of growth (follow-up volume minus baseline volume) occurred in the control group (baseline value: 27.3 mm3; control group: 49.15 mm3; basiliximab group: 20.23–26.69 mm3; p = 0.015; Graphs 2 and 3). 178 Lumen after Arq Bras Cardiol. 2015; 105(2):176-183 In simple linear regression analysis assessment (Graph 4B), previous atherosclerosis was not associated with increased growth of the intima (r = 0.15; p = 0.96). Positive remodeling (increase in EEM) was associated with a greater increase in intimal volume (r = 0.85; p < 0.001; Graph 4A). Discussion This study revealed the following findings. (1) The use of induction therapy with basiliximab was associated with less intimal tissue growth in the first year after HT. (2) In the control Wang et al. Basiliximab and graft vasculopathy Original Article p = 0.051 80.00 30.00 0.00 40.0 20.0 100.00 B Volumetric Growth of the Plaque 90.00 A Volumetric Growth of the Lumen Volumetric growth of the artery (EEM) 120.00 p = 0.051 8 0.0 -20.0 Não Sim C 2 p = 0.051 60.00 40.00 20.00 0.00 -40.0 -30.00 80.00 Não Sim Baxilicimab Baxilicimab Não Sim Baxilicimab Graph 1 – Analysis of the volume change at 1 year after transplantation. A: Variation in the vessel. B: Variation in the lumen. C: Variation in the intima. 120 100 1 80 2 3 60 4 5 40 6 7 20 0 Previous Volume After Volume Graph 2 – Growth of plaque volume in patients undergoing induction therapy with basiliximab. group, we observed greater positive remodeling, which was probably related to increased intimal growth observed in this group. (3) With simple linear regression analysis, vessel growth was proportional to the increase of the plaque regardless of induction therapy. (4) Atherosclerosis in the donor was not associated with increased growth of the intima. Graft vascular disease begins with endothelial injury, followed by a repair process, cell proliferation, and accumulation of extracellular matrix3,6. The degree of organ preservation, ischemia/reperfusion injury, acute rejection, and viral infection (particularly cytomegalovirus) are cited as the main non-immunological factors that affect the endothelium in the first year after HT. In response to injury, endothelial cells express cell adhesion molecules (vascular cell adhesion molecule, intercellular cell adhesion molecule, and selectins); furthermore, recruitment of inflammatory cells and release of proinflammatory cytokines occur. This results in a vicious cycle of chronic inflammation, culminating in the obliteration of the lumen15-17. Growth inhibition by basiliximab, which exhibits its action 4–6 weeks after infusion9, reinforces the relationship between early recruitment of lymphocytes and the appearance of CAV6. Tori et al.18 and Young et al. 19 observed that the infiltration and activation of lymphocytes in the first days after HT are already sufficient for the appearance of CAV. The specific activation pathway of major histocompatibility complex II and proliferation of Th1 lymphocytes are considered to be the primary route of CAV formation20. Blocking various parts of this pathway has been proven effective in reducing the appearance of CAV21. IL-2 also plays a major role in the activation pathway of T helper 1 (Th1) lymphocytes, and this could explain the benefit of the Arq Bras Cardiol. 2015; 105(2):176-183 179 Wang et al. Basiliximab and graft vasculopathy Original Article 140 120 100 1 2 80 3 60 4 5 40 6 20 0 After Volume Previous Volume Graph 3 – Plaque volume in patients who received no induction therapy. Vessel growth 120.00 Plaque growth 100.00 A B 80.00 90.00 60.00 60.00 r = 0.85 p < 0.001 30.00 40.00 0.00 20.00 -30.00 0.00 0.00 20.00 40.00 60.00 Intimal growth 80.00 r = 0.15 p < 0.096 100.00 0.00 20.00 40.00 60.00 Previous plaque volume 80.00 Graph 4 – A. Vessel growth according to intimal growth. B. Impact of previous plaque atherosclerosis on CAV growth. use of basiliximab in the first weeks after HT to interrupt the cycle of injury and repair, thus preventing the chronic inflammatory process. The reduction of intimal growth induction therapy is not a new finding22. Zhang et al.22 observed that induction therapy with antithymocyte antibody (antithymocyte globulin, ATG) delays the onset of CAV. However, the effect did not translate 180 Arq Bras Cardiol. 2015; 105(2):176-183 into increased long-term survival. In addition, a higher incidence of cancer is observed in patients treated with ATG, which may explain the higher late mortality rate in this group. Long-term follow-up is indicated to determine the benefit and/or clinical harm of this therapy. As basiliximab is not associated with increased infection or neoplasia9,23, we expect a clinical benefit. Wang et al. Basiliximab and graft vasculopathy Original Article In the global registry of the ISHLT, the use of basiliximab for induction therapy has a neutral effect on CAV (relative risk [RR]: 1.16; confidence interval [CI]: 0.99–1.37); however, CAV increased with the use of muromonab-CD3 (OKT3; RR: 1.17; p = 0.038)2. This effect is probably due to selection bias. Patients with a higher risk of acute rejection in the post-transplantation period and those who have higher levels of a reactor panel of antibodies (PRA) are at greatest risk of developing CAV24,25. Another example of selection bias occurs with induction therapy, correlates with IL-2 receptor antagonists, and a risk of renal dysfunction, and this medication is indicated for patients at high risk for renal failure after transplantation26. As in atherosclerosis27, we observed positive remodeling to accommodate the increase of the intima, thus avoiding involvement of the arterial lumen. In previous studies, most intimal tissue growth and positive remodeling occurred during the first year post-HT28,29. From the second year onward, despite a lower growth of the intima, there is greater involvement of the arterial lumen due to negative vessel remodeling28. We found variation in the natural history of the process in patients treated with basiliximab. We also found a slight decrease in vessel remodeling and luminal volume reduction; however, to date, we do not know how it will progress following the second year. In our institution, induction therapy with basiliximab is routinely performed with the goal of delaying the onset of the need for caucineurin inhibitors and minimizing the nephrotoxic effects of cyclosporin26,30. Candidates for HT have a high prevalence of renal dysfunction; furthermore, after HT, renal function may deteriorate, particularly because of the use of nephrotoxic drugs, low cardiac output, and impaired cardiopulmonary bypass. Moreover, acute renal failure is associated with a poor outcome2. Due to low sensitivity of coronary angiography in detecting early CAV, IVUS is used in our institution for CAV research, because its high sensitivity and specificity provide an earlier diagnosis of CAV14,31. Clinically, IVUS has a good correlation with angiography; thus, it is a good prognostic tool32. Some evidence exists that early diagnosis of CAV, together with the adjustment of immunosuppressive therapy is associated with growth control. Furthermore, some studies have reported regression of CAV 21,33,34 . The volumetric measurement of the plate by IVUS has been previously validated by experimental11 and clinical studies12. This methodology has a strong correlation with histomorphometry. Moreover, it is a robust method and requires a smaller sample to demonstrate the effectiveness of strategies that have an impact on reducing the intima11. The major limitation of this study is its small sample size, possible bias in patient selection, and retrospective nature. Thus, a prospective, multicenter, randomized study with a larger sample size, which extends clinical follow-up to assess the long-term benefit, is indicated. Furthermore, our control group had greater plaque volume, probably due to atherosclerosis of the donor; this may have affected the outcome, as suggested by a recent study by Yamasaki et al.35. However, in our study, plaque volume did not correlate with higher growth of the intima (r = 0,24; p = 0.94), a finding that is consistent with those of previous studies36,37. Conclusion In this retrospective analysis, induction therapy with basiliximab was associated with less volumetric growth of intimal tissue (graft vasculopathy) in the first year after HT. Author contributions Conception and design of the research:Wang R, Moura LAZ, Costa FA, Souza Filho NS, Faria-Neto JR. Acquisition of data:Wang R, Moura LAZ, Lopes SV, Costa FA, Fernandes TL, Salvatti NB, Faria-Neto JR. Analysis and interpretation of the data: Wang R, Moura LAZ, Lopes SV, Costa FA, Souza Filho NS, Fernandes TL, Salvatti NB, Faria-Neto JR. Statistical analysis: Wang R, Faria-Neto JR. Obtaining financing: Wang R, Lopes SV, Souza Filho NS, Faria-Neto JR. Writing of the manuscript:Wang R, Moura LAZ, Faria-Neto JR. Critical revision of the manuscript for intellectual content: Wang R, Moura LAZ, Lopes SV, Costa FA, Souza Filho NS, Fernandes TL, Salvatti NB, Faria-Neto JR. Potential Conflict of Interest No potential conflict of interest relevant to this article was reported. Sources of Funding There were no external funding sources for this study. Study Association This article is part of the thesis of master submitted by Ricardo Wang, from Pontífica Universidade Católica do Paraná. References 1. Houser S, Muniappan A, Allan J, Sachs D, Madsen J. Cardiac allograft vasculopathy: real or a normal morphologic variant? J Heart Lung Transplant. 2007;26(2):167-73. 3. Benza RL, Tallaj J. Cardiac Allograft Vasculopathy (Chronic Rejection). In: Kirklin JK, Young JB, McGiffin DC. (eds.). Heart transplantation. 3 rd ed. Philadelphia: Churchill Livingstone; 2002. p. 615-65. 2. Stehlik J, Edwards LB, Kucheryavaya AY, Aurora P, Christie JD, Kirk R, et al. The Registry of the International Society for Heart and Lung Transplantation: twenty-seventh official adult heart transplant report -- 2010. J Heart Lung Transplant. 2010;29(10):1089-103. 4. Nagano H, Libby P, Taylor MK, Hasegawa S, Stinn JL, Becker G, et al. Coronary arteriosclerosis after T- cell-mediated injury in transplanted mouse hearts: role of interferon-gamma. Am J Pathol. 1998;152(5):1187-97. Arq Bras Cardiol. 2015; 105(2):176-183 181 Wang et al. Basiliximab and graft vasculopathy Original Article 5. Uehara S, Chase CM, Colvin RB, Madsen JC, Russell PS. T-cell depletion eliminates the development of cardiac allograft vasculopathy in mice rendered tolerant by the induction of mixed chimerism. Transplant Proc. 2006;38(10):3169-71. 6. Valantine HA. Cardiac allograft vasculopathy: central role of endothelial injury leading to transplant “atheroma”. Transplantation. 2003;76(6):891-9. 7. Bacal F, Souza-Neto J, Fiorelli A, Mejia J, Marcondes-Braga FG, Mangini S, et al. II Brazilian Guidelines for cardiac transplantation. Arq Bras Cardiol. 2010;941 Suppl):e16-76. 8. Church AC. Clinical advances in therapies targeting the interleukin-2 receptor. QJM. 2003;96(2):91-102. 9. Onrust SV, Wiseman LR. Basiliximab. Drugs. 1999;57(2):207-13. 10. Young JB, Lloyd KS, Windsor NT, Cocanougher B, Weilbaecher DG, Kleiman NS, et al. Elevated soluble interleukin-2 receptor levels early after heart transplantation and long-term survival and development of coronary arteriopathy. J Heart Lung Transplant. 1991;10(2):243-50. 11. Mehran R, Mintz GS, Hong MK, Tio FO, Bramwell O, Brahimi A, et al. Validation of the in vivo intravascular ultrasound measurement of in-stent neointimal hyperplasia volumes. J Am Coll Cardiol. 1998;32(3):794-9. 12. Nissen SE, Nicholls SJ, Sipahi I, Libby P, Raichlen JS, Ballantyne CM, et al. Effect of very high-intensity statin therapy on regression of coronary atherosclerosis. JAMA. 2006;295(13):1556-65. 13. Mintz GS, Nissen SE, Anderson WD, Bailey SR, Erbel R, Fitzgerald PJ, et al. American College of Cardiology Clinical Expert Consensus Document on Standards for Acquisition, Measurement and Reporting of Intravascular Ultrasound Studies (IVUS). A report of the American College of Cardiology Task Force on Clinical Expert Consensus Documents. J Am Coll Cardiol. 2001;37(5):1478-92. 14. Mehra MR, Crespo-Leiro MG, Dipchand A, Ensminger SM, Hiemann NE, Kobashigawa JA, et al. International Society for Heart and Lung Transplantation working formulation of a standardized nomenclature for cardiac allograft vasculopathy-2010. J Heart Lung Transplant. 2010;29(7):717-27. 15. Yamani MH, Haji SA, Starling RC, Tuzcu EM, Ratliff NB, Cook DJ, et al. Myocardial ischemic-fibrotic injury after human heart transplantation is associated with increased progression of vasculopathy, decreased cellular rejection and poor long-term outcome. J Am Coll Cardiol. 2002;39(6):970-7. 23. Chapman TM, Keating GM. Basiliximab: a review of its use as induction therapy in renal transplantation. Drugs. 2003;63(24):2803-35. 24. Kobashigawa JA, Patel JK, Kittleson MM, Kawano MA, Kiyosaki KK, Davis SN, et al. The long-term outcome of treated sensitized patients who undergo heart transplantation. Clin Transplant. 2011;25(1):E61-7. 25. Feingold B, Bowman P, Zeevi A, Girnita AL, Quivers ES, Miller SA, et al. Survival in allosensitized children after listing for cardiac transplantation. J Heart Lung Transplant. 2007;26(6):565-71. 26. Delgado DH, Miriuka SG, Cusimano RJ, Feindel C, Rao V, Ross HJ. Use of basiliximab and cyclosporine in heart transplant patients with pre-operative renal dysfunction. J Heart Lung Transplant. 2005;24(2):166-9. 27. Glagov S, Weisenberg E, Zarins CK, Stankunavicius R, Kolettis GJ. Compensatory enlargement of human atherosclerotic coronary arteries. N Engl J Med. 1987;316(22):1371-5. 28. Tsutsui H, Ziada KM, Schoenhagen P, Tyisoy A, Magyar WA, Crowe TD, et al. Lumen loss in transplant coronary artery disease is a biphasic process involving early intimal thickening and late constrictive remodeling: results from a 5-year serial intravascular ultrasound study. Circulation. 2001;104(6):653-7. 29. Yeung AC, Davis SF, Hauptman PJ, Kobashigawa JA, Miller LW, Valantine HA, et al. Incidence and progression of transplant coronary artery disease over 1 year: results of a multicenter trial with use of intravascular ultrasound. Multicenter Intravascular Ultrasound Transplant Study Group. J Heart Lung Transplant. 1995;14(6 Pt 2):S215-20. 30. Anselm A, Cantarovich M, Davies R, Grenon J, Haddad H. Prolonged basiliximab use as an alternative to calcineurin inhibition to allow renal recovery late after heart transplantation. J Heart Lung Transplant. 2008;27(9):1043-5. 31. Cai Q, Rangasetty UC, Barbagelata A, Fujise K, Koerner MM. Cardiac allograft vasculopathy: advances in diagnosis. Cardiol Rev. 2011;19(1):30-5. 32. Rickenbacher PR, Pinto FJ, Lewis NP, Hunt SA, Alderman EL, Schroeder JS, et al. Prognostic importance of intimal thickness as measured by intracoronary ultrasound after cardiac transplantation. Circulation. 1995;92(12):3445-52. 16. Land W, Messmer K, Events E. The impact of ischemia/reperfusion injury on specific and non-specific, early and late chronic events after organ transplantation. Transplant Rev. 1996;10:108-27. 33. Lamich R, Ballester M, Marti V, Brossa V, Aymat R, Carrió I, et al. Efficacy of augmented immunosuppressive therapy for early vasculopathy in heart transplantation. J Am Coll Cardiol. 1998;32(2):413-9. 17. Day JD, Rayburn BK, Gaudin PB, Baldwin WM 3rd, Lowenstein CJ, Kasper EK, et al. Cardiac allograft vasculopathy: the central pathogenetic role of ischemiainduced endothelial cell injury. J Heart Lung Transplant. 1995;14(6 Pt 2):S142-9. 34. Dambrin C, Klupp J, Birsan T, Luma J, Suzuki T, Lam T, et al. Sirolimus (rapamycin) monotherapy prevents graft vascular disease in nonhuman primate recipients of orthotopic aortic allografts. Circulation. 2003;107(18):2369-74. 18. Tori M, Kitagawa-Sakakida S, Li Z, Izutoni H, Horiguchi K, Ito T, et al. Initial T-cell activation required for transplant vasculopathy in retransplanted rat cardiac allografts. Transplantation. 2000;70(5):737-46. 35. Yamasaki M, Sakurai R, Hirohata A, Honda Y, Bonneau HN, Luikart H, et al. Impact of donor-transmitted atherosclerosis on early cardiac allograft vasculopathy: new findings by three-dimensional intravascular ultrasound analysis. Transplantation. 2011;91(12):1406-11. 19. Young JB, Windsor NT, Kleiman NS, Lowry R, Cocanougher B, Lawrence EC. The relationship of soluble interleukin-2 receptor levels to allograft arteriopathy after heart transplantation. J Heart Lung Transplant. 1992;11(3 Pt 2):S79-82. 20. Mitchell RN. Graft vascular disease: immune response meets the vessel wall. Annu Rev Pathol. 2009;4:19-47. 21. Eisen HJ, Tuzcu EM, Dorent R, Kobashigawa J, Mancini D, Valantine-von Kaeppler HA, et al. Everolimus for the prevention of allograft rejection and vasculopathy in cardiac-transplant recipients. N Engl J Med. 2003;349(9):847-58. 182 22. Zhang R, Haverich A, Strüber M, Simon A, Bara C. Delayed onset of cardiac allograft vasculopathy by induction therapy using anti-thymocyte globulin. J Heart Lung Transplant. 2008;27(6):603-9. Arq Bras Cardiol. 2015; 105(2):176-183 36. Botas J, Pinto FJ, Chenzbraun A, Linag D, Schroeder JS, Oesterle SN, et al. Influence of preexistent donor coronary artery disease on the progression of transplant vasculopathy: an intravascular ultrasound study. Circulation. 1995;92(5):1126-32. 37. Kapadia SR, Nissen SE, Ziada KM, Guetta V, Crowe TD, Hobbs RE, et al. Development of transplantation vasculopathy and progression of donortransmitted atherosclerosis: comparison by serial intravascular ultrasound imaging. Circulation. 1998;98(24):2672-8. Wang et al. Basiliximab and graft vasculopathy Original Article Arq Bras Cardiol. 2015; 105(2):176-183 183 Back to the Cover Brief Communication Diastolic Function in Paced Children with Cardiac Defects: Septum vs Apex Michel Cabrera Ortega, Adel Eladio Gonzalez Morejon, Giselle Ricardo Serrano, Dunia Barbara Benitez Ramos Cardiocentro Pediatrico William Soler, La Habana - Cuba Abstract In children with structural congenital heart disease (CHD), the effects of chronic ventricular pacing on diastolic function are not well known. On the other hand, the beneficial effect of septal pacing over apical pacing is still controversial. The aim of this study was to evaluate the influence of different right ventricular (RV) pacing site on left ventricular (LV) diastolic function in children with cardiac defects. Twenty-nine pediatric patients with complete atrioventricular block (CAVB) and CHD undergoing permanent pacing were prospectively studied. Pacing sites were RV apex (n = 16) and RV septum (n = 13). Echocardiographic assessment was performed before pacemaker implantation and after it, during a mean follow‑up of 4.9 years. Compared to RV septum, transmitral E-wave was significantly affected in RV apical pacing (95.38 ± 9.19 vs 83 ± 18.75, p = 0.038). Likewise, parameters at the lateral annular tissue Doppler imaging (TDI) were significantly affected in children paced at the RV apex. The E´ wave correlated inversely with TDI lateral myocardial performance index (Tei index) (R2 = 0.9849, p ≤ 0.001). RV apex pacing (Odds ratio, 0.648; confidence interval, 0.067-0.652; p = 0.003) and TDI lateral Tei index (Odds ratio, 31.21; confidence interval, 54.6-177.4; p = 0.025) predicted significantly decreased LV diastolic function. Of the two sites studied, RV septum prevents pacinginduced reduction of LV diastolic function. Introduction RV apical pacing is conventionally performed in pediatric patients with CAVB. However, ventricular pacing induces an abnormal electrical activation pattern, which causes mechanical dyssynchrony, LV structural remodeling and increased risk of heart failure1-3. Most pediatric studies published1,2 have focused on ventricular systolic function Keywords Heart Defects, Congenital; Ventricular Function, Right; Ventricular Function, Left; Child; Pacemaker, Artificial. Mailing Address: Michel Cabrera • Cardiocentro Pediatrico William Soler. 100 y perla, Boyeros. Postal Code 10800, La Habana – Cuba E-mail: [email protected], [email protected] Manuscript received December 09, 2014; revised manuscript April 22, 2015; accepted manuscript April 30, 2015. DOI: 10.5935/abc.20150077 184 assessment; therefore, the effects of chronic ventricular pacing on diastolic function are not well known, even less in children with CHD. Moreover, the benefit of RV septal stimulation is still controversial, with clinical studies 4 showing promising results, while a recent research did not demonstrate any superiority over RV apical pacing in children1; none of these studies1,2,4 reported the effects on LV relaxation phase. With the hypothetical premise that there are differences between RV septal and RV apical pacing in terms of dynamic alterations in LV filling, we performed the current study. Methods The study included all children with CHD and CAVB that underwent pacemaker implantation in a single tertiary pediatric cardiology center, paced from RV septum (n = 13) and from RV apex (n = 16). Patients with clinical or anamnestic evidence of heart failure were excluded. None of the patients were older than 18 years at pacemaker implantation, had ≤ 95% of ventricular pacing or ≤ 1 year of permanent cardiac pacing. The study protocol was approved by the institutional research ethics committee and parental written consent was obtained. Two experienced observers, blinded for the ventricular pacing site, performed prospective echocardiographic evaluations (Aloka α-10) before pacemaker implantation, immediately after and regularly during a mean period of 4.9 years. Three random measurements were made for every patient by each observer and the average of measurements was used for further analysis. For a comprehensive diastolic evaluation, the following mitral flow parameters were evaluated by pulsed wave Doppler echocardiography: E and A waves, E/A wave ratio and E-wave deceleration time. Likewise, pulse wave TDI velocities were obtained in the apical four-chamber view, at septal and lateral mitral annulus. In each segment, peak systolic (S´), early (E´) and late (A´) peak diastolic velocities were measured. The E/E´ ratio and TDI Tei index were also calculated. All data were prospectively collected. Statistical analysis According to the Kolmogorov-Smirnov test, the variables that showed a normal distribution were summarized as mean ± standard deviation. The differences between two groups were compared by unpaired t-test. Independent variables showing significant univariate differences related to the development of LV dysfunction were entered into a backward stepwise logistic regression analysis, where the Odds ratio (OR) and Wald statistics for each variable were identified. Significance level was set at 5%. The statistical software Medcalc Version 12 was used for the analyses. Cabrera Ortega et al. LV diastolic function in paced children Brief Communication Results Discussion A total of 29 patients (surgical atrioventricular block in 26), with mean age at first implantation of 9.82 ± 2.75 years were evaluated. Tetralogy of Fallot (8 cases, 27%) and ventricular septal defect (7 patients, 24.13%) were the main CHD corrected before pacemaker implantation. Anatomic surgical correction was performed in all patients and mild residual atrioventricular regurgitation was present in 10 (34.48%) children. Thirteen (44.82%) cases underwent treatment with angiotensin‑converting enzyme inhibitors at the time of implantation. Twelve children (41.37%) received a single‑chamber pacemaker, while 11 (24.13%) patients underwent DDD/DDDR pacing. Mean pacing duration was 4.9 years. Our study confirms that chronic stimulation from RV apex results in diastolic function impairment in pediatric patients with CHD and further demonstrates the superiority of septal stimulation in this context. Compared to RV septum, transmitral E-wave was significantly affected in RV apical pacing (95.38 ± 9.19 vs 83 ± 18.75, p = 0.038) (Table 1). Likewise, the following parameters of the lateral annular TDI were significantly affected in children paced at the RV apex compared with RV septum group: E´ wave (12.5 ± 4.42 vs 15.3 ± 2.1; p = 0.046), A´ wave (8.12 ± 2.63 vs 6.22 ± 2.11; p = 0.045), E/E´ ratio (8.2 ± 1.29 vs 6.3 ± 0.72; p = 0.0001) and Tei index (0.39 ± 0.04 vs 0.34 ± 0.04; p = 0.002). The E´ wave correlated inversely with TDI lateral Tei index (R2 = 0.9849, p ≤ 0.001) (Figure 1). At the logistic regression, pacing from the RV apex (OR, 0.648; confidence interval, 0.067-0.652; Wald, -0.915; p = 0.003) and TDI lateral Tei index (OR, 31.21; confidence interval, 54.6-177.4; Wald, 3.046; p = 0.025) predicted significantly decreased LV diastolic function. The deterioration of diastolic function after RV pacing has been previously reported in animals5 and in the adult population 6,7. Aoyagi et al 5 showed that wall motion asynchrony prolongs LV isovolumic relaxation time (IVRT) in dogs; this impairment correlated with the degree of wall motion asynchrony. In the research performed by Kolettis et al6, compared to RV outflow tract pacing, RV apical pacing decreased maximum negative dp/dt and increased the IVRT. These findings were confirmed in an analysis of nine studies7, reporting a significant benefit of RV outflow tract over apical pacing. On the other hand, few investigations3,8,9 have focused on LV diastolic function in the pediatric population. Forwalt et al8 evaluated the effects of acute ventricular pacing in children who underwent ablation therapy; the authors observed that RV apical pacing resulted in acute systolic dyssynchrony with preserved diastolic synchrony. Nevertheless, Koh et al9 provided evidence of LV diastolic dysfunction after chronic RV apical stimulation, associated with the presence of LV dyssynchrony. In our study, the impaired diastolic indices in the lateral mitral annulus could be associated with the pattern induced by RV apical pacing, characterized by early activation of the RV and delayed activation of the LV lateral wall. Table 1 - Comparison of LV function between RV septal and apical pacing RV Septum (n = 13) RV Apex (n = 16) p* Before PM implantation At last follow-up p Before PM implantation At last follow-up p 64.16 ± 1.75 61.43 ± 2.26 0.004 65.21 ± 2.08 64.22 ± 3.14 0.352 0.009 E(cm/s) 90.72 ± 13.81 95.38 ± 9.19 0.321 90.53 ± 11.45 83 ± 18.75 0.181 0.038 A(cm/s) 61.46 ± 15.19 56.69 ± 7.2 0.316 65.87 ± 18.31 67.06 ± 19.66 0.860 0.100 LVEF Mitral Inflow Doppler indices E/A 1.59 ± 0.51 1.71 ± 0.33 0.483 1.51 ± 0.54 1.41 ± 0.65 0.639 0.142 170.38 ± 23.54 172.07 ± 17.45 0.837 170.68 ± 24.06 172.8 ± 25.84 0.811 0.931 E´(cm/s) 15 ± 3.41 15.3 ± 2.1 0.789 15.6 ± 3.31 12.5 ± 4.42 0.032 0.046 A´(cm/s) 6.41 ± 2.13 6.22 ± 2.1 0.820 7.1 ± 2.11 8.12 ± 2.63 0.235 0.045 EDT(ms) Lateral Mitral Valve Annular TDI E/E´ 6.1 ± 0.81 6.3 ± 0.72 0.512 5.8 ± 0.62 8.2 ± 1.29 < 0.0001 0.0001 Tei index 0.33 ± 0.04 0.34 ± 0.04 0.529 0.35 ± 0.05 0.39 ± 0.04 0.018 0.002 E´(cm/s) 15.30 ± 4.23 14.84 ± 3.51 0.765 15.12 ± 3.28 13.81 ± 3.97 0.317 0.470 A´(cm/s) 7.23 ± 2.35 7.24 ± 2.33 0.991 7 ± 2.55 6.56 ± 2.65 0.616 0.474 E/E´ 6.19 ± 1.11 6.68 ± 1.22 0.294 6.11 ± 0.74 6.13 ± 0.56 0.931 0.118 Tei index 0.34 ± 0.06 0.35 ± 0.04 0.621 0.33 ± 0.01 0.36 ± 0.08 0.147 0.685 Septal Mitral Valve Annular TDI Data expressed by mean ± standard error. p*: septum vs. apex at last follow-up. EDT: E-wave deceleration time; LVEF: Left ventricular ejection fraction; PM: Pacemaker; RV: Right ventricular; TDI: Tissue doppler imaging. Arq Bras Cardiol. 2015; 105(2):184-187 185 Cabrera Ortega et al. LV diastolic function in paced children Brief Communication 20 R2 = 0.9849 p ≤ 0.001 y = 31.1684 + -0,4868x 95% CI = -0.9965 - 0.9835 18 E (cm/s) 16 14 12 10 8 6 4 0.2 0.3 0.4 0.5 0.6 Tei index Figure 1 – Association between E´-wave and TDI Tei index at lateral mitral valve annulus. The Tei index has been used to assess LV function in a wide variety of diagnoses in children10; it is the most accurate for the detection of diastolic and combined dysfunction10. Considering that the results of our research reflect the high predictive value of this parameter, it could be used as an echocardiographic tool to predict the deterioration of both systolic and diastolic functions in patients with chronic ventricular pacing. Conclusions Potential Conflict of Interest No potential conflict of interest relevant to this article was reported. Of the two assessed sites, RV septum showed to prevent pacing-induced reduction of LV diastolic function. Sources of Funding Author contributions Study Association Conception and design of the research: Ortega MC, Morejon AEG; Acquisition of data, Analysis and interpretation 186 of the data and Critical revision of the manuscript for intellectual content: Ortega MC, Morejon AEG, Serrano GR, Ramos DBB; Statistical analysis: Ortega MC, Serrano GR, Ramos DBB; Writing of the manuscript: Ortega MC. Arq Bras Cardiol. 2015; 105(2):184-187 There were no external funding sources for this study. This article is part of the thesis of Doctoral submitted by Michel Cabrera Ortega, from Cardiocentro Pediátrico William Soller. Cabrera Ortega et al. LV diastolic function in paced children Brief Communication References 1. Janousek J, van Geldorp IE, Kuprikova S, Rosenthal E, Nugent K, Tomaske M, et al; Working Group for Cardiac Dysrhythmias and Electrophysiology of the Association for European Pediatric Cardiology. Permanent cardiac pacing in children: choosing the optimal pacing site: a multicenter study. Circulation. 2013;127(5):613-23. Erratum in: Circulation. 2013;127(15):e550. 2. Gebauer RA, Tomek V, Salameh A, Marek J, Chaloupecký V, Gebauer R, et al. Predictors of left ventricular remodeling and failure in right ventricular pacing in the young. Eur Heart J. 2009;30(9):1097-104. 3. Cabrera Ortega M, Gonzales Morejón AE, Serrano Ricardo G. Left ventricular synchrony and function in pediatric patients with definitive pacemaker. Arq Bras Cardiol. 2013;101(5):410-7. 4. Tse HF, Yu C, Wong KK, Tsang V, Leung YL, Ho WY, et al. Functional abnormalities in patients with permanent right ventricular pacing: the effect of sites of electrical stimulation. J Am Coll Cardiol. 2002;40(8):1451-8. 5. Aoyagi T, Lizuka M, Takahashi T, Ohya T, Serizawa T, Momomura S, et al. Wall motion asynchrony prolongs time constant of left ventricular relaxation. Am J Physiol. 1989; 257(3 Pt 2):H883-90. 6. Kolettis TM, Kyriakides ZS, Tsiapras D, Popov T, Paraskevaides IA, Kremastinos DT. Improved left ventricular relaxation during shortterm right ventricular outflow tract compared to apical pacing. Chest. 2000;117(1):60-4. 7. de Cock CC, Giudici MC, Twisk JW. Comparison of the haemodynamic effects of right ventricular outflow-tract pacing with right ventricular apex pacing: a quantitative review. Europace. 2003;5(3):275-8. 8. Forwalt BK, Cummings RM, Arita T, Delfino JG, Fyfe DA, Campbell RM, et al. Acute pacing-induced dyssynchronous activation of the left ventricle creates systolic dyssynchrony with preserved diastolic synchrony. J Cardiovasc Electrophysiol. 2008;19(5):483-8. 9. Koh C, Hong WJ, Yung TC, Lun KS, Wong SJ, Cheung YF. Left ventricular torsional mechanics and diastolic function in congenital heart block with right ventricular pacing. Int J Cardiol. 2012;160(1):31-5. 10. Patel DR, Cui W, Gambetta K, Roberson DA. A comparison of tei index versus systolic to diastolic ratio to detect left ventricular dysfunction in pediatric patients. J Am Soc Echocardiogr. 2009;22(2):152-8. Arq Bras Cardiol. 2015; 105(2):184-187 187 Back to the Cover Review Article Nobel Prizes: Contributions to Cardiology Evandro Tinoco Mesquita, Luana de Decco Marchese, Danielle Warol Dias, Andressa Brasil Barbeito, Jonathan Costa Gomes, Maria Clara Soares Muradas, Pedro Gemal Lanzieri, Ronaldo Altenburg Gismondi Universidade Federal Fluminense, Niterói, RJ – Brazil Abstract The Nobel Prize was created by Alfred Nobel. The first prize was awarded in 1901 and Emil Adolf von Behring was the first laureate in medicine due to his research in diphtheria serum. Regarding cardiology, Nobel Prize’s history permits a global comprehension of progress in pathophysiology, diagnosis and therapeutics of various cardiac diseases in last 120 years. The objective of this study was to review the major scientific discoveries contemplated by Nobel Prizes that contributed to cardiology. In addition, we also hypothesized why Carlos Chagas, one of our most important scientists, did not win the prize in two occasions. We carried out a non-systematic review of Nobel Prize winners, selecting the main studies relevant to heart diseaseamong the laureates. In the period between 1901 and 2013, 204 researches and 104 prizes were awarded in Nobel Prize, of which 16 (15%) studies were important for cardiovascular area. There were 33 (16%) laureates, and two (6%) were women. Fourteen (42%) were American, 15 (45%) Europeans and four (13%) were from other countries. There was only one winner born in Brazil, Peter Medawar, whose career was all in England. Reviewing the history of the Nobel Prize in physiology or medicine area made possible to identify which researchers and studies had contributed to advances in the diagnosis, prevention and treatment of cardiovascular diseases. Most winners were North Americans and Europeans, and male. Introduction The Nobel Prize was created by Alfred Nobel (1833-1896) (Figure 1)1,2. In his will, the Swedish researcher determined the creation of a foundation that would carry his name, of which main objective would be to reward every year, individuals that provided outstanding contributions to mankind in the areas of Peace/Diplomacy, Literature, Chemistry, Physics and Physiology/Medicine. The first prizes were awarded in 1901 and the first winner in Medicine was Emil Adolf von Behring, for his work with diphtheria serum1. Since that date, there have been 876 Nobel Prize winners, of which 104 awards and 204 researchers in the area of Medicine or Physiology1. Keywords Cardiology; Nobel Prize; History; Cardiovascular Diseases / trends. Mailing Address: Ronaldo Altenburg Odebrecht Curi Gismondi • Universidade Federal Fluminense. Rua Ministro Otávio Kelly, 185/701, Icaraí. Postal Code 24220-300, Niterói, RJ – Brazil E-mail: [email protected], [email protected] Manuscript received November 22, 2014; revised manuscript February 9, 2015; accepted February 11, 2015. DOI: 10.5935/abc.20150041 188 The objective of the present study was to review the major scientific discoveries that received the Nobel Prize and directly or indirectly contributed to advances in physiopathology, diagnosis and treatment of cardiovascular diseases. Methods We performed a systematic search of the main non Nobel Prize winners from 1901 to 2013. The winners list was obtained from the Nobel Prize site3 and, subsequently, information about the authors and their research were obtained from the Medline/PubMed database. Moreover, due to the specific nature of the research involving historical and bibliographical data, the Google search engine was utilized, using as descriptors the names of the researchers awarded the Nobel Prize. The results are displayed in ascending chronological order. Results A brief history of the Nobel Prize For many historians, the interest of Alfred Nobel in medicine derived from a poor health2. There are reports of dyspepsia, headaches and bouts of depression. In adulthood, he would have suffered from coronary artery disease, with frequent episodes of angina. His doctors recommended the use of nitroglycerin, a substance Nobel manipulated in the explosives industry, but he would have refused. In later life he had a stroke and had to live with motor sequelae. Skeptical and suspicious, Nobel expressed in his will the wish that after his death, his veins were "open" and the signs of death confirmed by "competent doctors," before the body was sent to be cremated1. Nobel’s choice of the Karolinska Institute in his will surprised many scientists. This institute was created in 1810 from the merging of a Medical School and a small surgical center where barbers were trained to perform amputations. For years it did not have the status of School of Medicine and depended on a contract with the University of Uppsala, in Sweden, for the training of its professionals1. Currently, the institute is one of the leading Assistance Medicine and Research centers in Europe. Five Nobel Prize winners over the last 120 years, came from this institute1. The Nobel Prize and Cardiology In the area of cardiology, specifically regarding heart failure (HF), knowledge of the history of the Nobel Prize helps to understand important diagnostic and therapeutic advances made in the last 120 years (Chart 1). The first laureate in this area was Alexis Carrel, for his discoveries related to blood Mesquita et al. Nobel Prize and Cardiology Review Article Figure 1 – Nobel Prize Logo. Source: http://en.wikipedia.org/wiki/Nobel_Prize vessel suture, an important step in the further development of cardiac surgery1,3. Only one Brazilian, who lived in England, was awarded. His name is Peter Medawar and he has carried out researches in the immunosuppression area, with future applicability in renal and cardiac transplant4,5. Although Carlos Chagas researched and discovered the etiological agent, the vector, the mode of transmission and clinical forms of trypanosomiasis, a unique feat in the history of world’s science, he was a candidate for the Nobel a few times, but was unsuccessful. There are hypotheses that attempt to explain why a genuinely Brazilian contribution in the field of cardiology has not been contemplated with the Nobel prize6,7. Major studies important for Cardiology that were awarded the Nobel Prize Alexis Carrel – 1912: blood vessel suture Alexis Carrel, was born in Sainte-Foy-lès-Lyon, France, graduated in Medicine from the School of Medicine of Lyon in 1893 and completed his doctorate in 1900, with a research on blood vessel sutures. He taught Anatomy and Surgery at the University of Lyons and moved to the United States in 1904, where he worked at the University of Chicago. Later, he joined the Rockefeller Institute for Medical Research in New York, where he performed most of the experiments that led to the Nobel Prize in Physiology or Medicine in 1912. He served the medical corps of the French Army during World War I (1914 -1918), where he successfully used the Carrel-Dakin method of constant irrigation of wounds with antiseptic solution, which decreased cases of death and amputations1-3,8. His early work was on surgical techniques in blood vessels and arteriovenous anastomoses. After 1908, he developed methods for organ cryopreservation and transplantation1-3,8. In 1935, he created a system for sterile oxygen supply and preservation of organs removed from the body. He also cooperated with other researchers for the development of cardiac valvotomy surgery and sarcoma cell culture. He published the books “The culture of organs” and “Treatment of infected wounds”1-3,8. The suture of blood vessels was essential for the development of vascular surgery in later years. Willem Einthoven – 1924: The Electrocardiogram Willem Einthoven was born on May 21, 1860 on the island of Java, now Indonesia, and moved to the Netherlands in 1870, where he graduated from Medical School at the University of Utrecht, one of the oldest and most traditional medical schools in Europe. He was a physiologist and in the early 20th century, he published several papers on the use of the galvanometer in the recording of the human electrocardiogram (ECG), which served as the basis for the current devices. The original equipment weighed more than 270 kg and was operated by several people in his laboratory. He described the P, QRS and T waves, as well as and their alterations in several diseases, especially in valvular heart disease. Showing great wisdom, he wrote after his initial research, “the electrocardiogram should not be used, at least exclusively, to diagnose valvular alterations, because the ECG is the expression of the heart muscle contraction and changes only to the extent that a valvular function failure has influence on such contraction”1,2,9. In addition to the ECG, Einthoven played an important role in the development of the phonocardiogram 1,2,9. Arq Bras Cardiol. 2015; 105(2):188-196 189 Mesquita et al. Nobel Prize and Cardiology Review Article Chart 1 – Main scientific discoveries that received the Nobel Prize in Physiology or Medicine related to the Cardiology area Year Author Prize 1912 Alexis Carrel Work on vascular suture and transplant of blood vessels and organs 1924 Willem Einthoven Electrocardiogram 1953 Hans Adolf Krebs Citric acid cycle (Krebs cycle) 1956 Werner Forssmann, Andre Cournard and Dickinson W. Richards Cardiac catheterization 1960 Frank Burnet and Peter Medawar Discovery of the immunological tolerance mechanism 1964 Konrad Bloch and Feodor Lynen Understanding of cholesterol metabolism 1979 Allan Cormack and Godfrey Hounsfield Computed tomography techniques 1982 Bengt Samuelsson, Sune Bergström and John Vane "Discovery" of the angiotensin-converting enzyme inhibitors 1985 Michael Brown and Joseph Goldstein Discovery of LDL-cholesterol receptors 1988 James Black, Gertrude Elion and George Hitchings Development of beta-blockers 1990 Joseph Edward Murray and Edward Thomas Development of organ and tissue transplant 1998 Robert Furchgott, Ferid Murad and Louis Ignarro Discoveries about nitric oxide 2003 Paul Lauterbur and Peter Mansfield Magnetic Resonance LDL: low-density lipoprotein. This device, now a museum piece in many medical schools, was crucial in the supplementary examination to medical workup. Before the invention of echocardiography, many valvular heart disease diagnoses were attained by auscultation and the phonocardiogram. The valvular diseases were, until the early 20th century, one of the most important causes of heart failure, particularly those of rheumatic origin. Hans Adolf Krebs – 1953: Krebs cycle Hans Adolf Krebs was born on August 25, 1900, in Hildeshiem, northern Germany10. He served as a military in the German army in World War I. Although he graduated in Medicine, he had to go into exile and left Germany in the 1930s, because of his Jewish descent. He chose to live in England, where he developed his research related to cell physiology. He described, together with other researchers, the urea cycle, the citric acid cycle, and especially, cellular respiration, which produces adenosine triphosphate (ATP) from glucose and oxygen10,11. In his honor, this sequence of biochemical reactions is known as "Krebs cycle". It has long been known that mitochondrial diseases are a group of diseases related to neuromuscular dysfunction and cardiomyopathy12,13. Moreover, in cardiology, the study of the mitochondrial function in the myocyte is a new research frontier, which some have called "mitochondrial bioenergetics"12,13. One of the key areas is HF, due to the role of aerobic metabolism in myocardial performance. Drugs are being developed that act on mitochondrial pathways, correcting occasional dysfunctions, and it is expected that they can improve myocardial function14,15. Werner Otto Theodor Forssmann, André Cournard and Dickinson Richards – 1956: cardiac catheterization The history of cardiac catheterization started in 1711, based on the works of Stephen Hales, who inserted tubes 190 Arq Bras Cardiol. 2015; 105(2):188-196 in both ventricles of a horse 1,16-19. In the 19 th century, cardiac catheterization continued with the work of Claude Bernard, the father of modern physiology; it became more sophisticated with the skills of Chauveau and Marey; and started to be applied in the human heart thanks to the self‑confidence of Forssmann in 1929, becoming therapeutic in 196620. According to Cournnand17, cardiac catheterization can be considered the "key that opened the lock to reveal the secrets of the heart." Due to the advancement of the technique proposed by the laureates, currently the hemodynamic study has applicability in the diagnosis, treatment and monitoring of cardiovascular disease - including Coronary Artery Disease (CAD) and HF. The Nobel Prize in Physiology or Medicine in 1956 was awarded to three researchers, due to their researches on catheterization that revolutionized the studies on heart disease1. They would not accept with the scarcity of semiotic methods, of which provided diagnoses were rebuffed by autopsies, which served as motivation to initiate their studies1. Werner Forssmann was a German physician, born in Berlin, who developed the hypothesis that a catheter could be inserted through blood vessels to the heart, aiming to injecting medications, perform contrast studies and measure chamber pressures. In order to test his hypothesis, he performed the first human catheterization in himself, guiding a catheter into his left atrium with the aid of a fluoroscopy device1,16-19. Andre Cournard, born in Paris, France and Dickinson Richards, from Orange, United States, were physicians who worked in the development of the cardiac catheterization technique, with emphasis on pulmonary diseases and patterns of circulatory shock. They described the shock patterns, particularly cardiogenic and hemorrhagic (trauma) and analyzed the hemodynamic changes with treatment, either by fluid replacement or drug infusion1,16-19. Mesquita et al. Nobel Prize and Cardiology Review Article Frank Macfarlane Burnet and Peter Brian Medawar – 1960: immunological tolerance Sir Frank Macfarlane Burnet was born in Australia and was the son of Scottish parents. He obtained a degree in Medicine in his native country and post-graduated in England. He specialized in the virology area, with important research related to influenza virus and herpes simplex. He played a key role in virus isolation from human tissue, and the first attempts to develop a vaccine for influenza. After World War II, he also developed researches related to the immune system, especially autoimmune mechanisms and immunological tolerance1,2,21-23. Peter Brian Medawar (Figure 2) was born in Petropolis (RJ), and had an English mother and Lebanese father. The family moved to England when he was only 14, where he developed his studies and career. Differences with the Brazilian government, which required his mandatory military service, made him give up his Brazilian nationality. He majored in zoology at Oxford and began transplantation research during World War II. The main objectives were skin grafts in burned skin areas. His studies led to the theory of acquired immunological tolerance, the basis for the development of solid organ transplants in the future1,2,4,5. The connection made between his research and Cardiology was the applicability of his results on immunological tolerance for the future development of heart transplantation. Konrad Bloch and Feodor Lynen – 1964: cholesterol metabolism The Nobel Prize in Physiology or Medicine of 1964 was awarded jointly to two German chemists, Konrad Bloch and Feodor Lynen. Bloch was born on January 21, 1912, in Neisse (now Nysa), formerly part of Germany and currently in Poland. He graduated in chemical engineering in 1934 in Munich. In 1936, due to the persecution of Jews by the Nazis, Bloch immigrated to the United States and joined the Department of Biochemistry at Columbia University, where he developed the research that led him to be awarded the Nobel Prize. Feodor Lynen was born on April 6, 1911, in Munich, Germany, where he graduated in chemistry. He developed his entire career in Germany, living there even during the world wars1,24. Even without performing a real joint work, both researchers carried out important discoveries in their universities on the cholesterol regulation mechanism and the fatty acid metabolism1,24. Starting from the idea that the acetic acid, with slow reaction in the chemical essays, had to show a more rapid and spontaneous reaction in the body, the concept of activated acetic acid was formulated, in which, in addition to adenyl-phosphoric acid as an energy source, also included coenzyme A. They were able to determine not only the structure of cholesterol, as well as the participation of coenzyme A in the oxidation of the fatty acids 1,24. Years later, these discoveries were crucial to demonstrate the importance of cholesterol in atherosclerosis and, more importantly, helped the development of statins, the major class of drugs for treatment of hypercholesterolemia and atherosclerotic disease. Allan M. Cormack and Godfrey Hounsfield - 1979: computed tomography Allan Cormack was a South African biochemist and nuclear physicist born in Johannesburg (South Africa), who became a naturalized American in 1966. He is considered one of the inventors of computed tomography and shared the Nobel Prize in Physiology or Medicine with British professor Godfrey Hounsfield. Cormack performed his research in radiology initially at the University of Cape Town until he immigrated to the United States, where he worked at Harvard and Tufts University. There, he tested a mathematical model based on the X radiation, essential to the development of computed axial tomography1,25. Sir Godfrey Hounsfield was an electrical engineer who had the position of "inventor" at the Central Research Laboratories in London. He started his career working on a radar project as a weapon of war and designed the first British transistorized computer in 1958, "EMIDEC 1100". Based on the mathematical calculations of radiation developed by Cormack, he developed Computed Tomography (CT) – so that the first machine to "scan" the brain was marketed by EMI. Three years later, he developed the first CT for the entire body. He continued to make improvements in CT and received numerous awards and honors, in addition to the Nobel prize, with his latest award being the title of Knight of the Queen of England - Sir, in 19811,25. CT developed further in the following years and now has several applications in cardiology, for instance, determination of the coronary anatomy and the calcium score, and in the assessment of pulmonary thromboembolism. Bengt Samuelsso, Sune Bergström and John Vane – 1982: prostaglandin function and development of angiotensinconverting enzyme inhibitors Bengt Ingemar Samuelsso was a Swedish biochemist born in 1934 in Halmstad, a researcher at the Karolinska Institute in Sweden, and Nobel Prize laureate in Physiology or Medicine with his institute colleague and also Swedish biochemist Sune K. Bergström, and with the English chemist and pharmacologist John Robert Vane 1. His research involved prostaglandin function, purification, determination of their chemical structure and identification of their mechanism of formation from unsaturated fatty acids1,26,27. This information allowed the proposition of acetylsalicylic acid mechanism of action, practically indispensable treatment in coronary heart disease. In addition to the research on prostaglandins, John Vane is also considered one of the "discoverers" of AngiotensinConverting Enzyme inhibitors (ACE inhibitors) 1,26,27 . During the 1960s and 1970s, and with the participation of Brazilian Sergio Ferreira, Vane and his colleagues demonstrated key steps in the synthesis of angiotensin and bradykinin, which, in 1982, culminated in the launching of the first ACEI, captopril1,26,27. This class of drugs has a vital role in the treatment of hypertension, heart failure and coronary artery disease. Michael Brown e Joseph Goldstein – 1985: LDLcholesterol receptors Joseph L. Goldstein was born on April 18, 1940 in Sumter, South Carolina, in the United States. He initially graduated Arq Bras Cardiol. 2015; 105(2):188-196 191 Mesquita et al. Nobel Prize and Cardiology Review Article Figure 2 – Peter Medawar’s picture. Source: http://www.nobelprize.org/nobel_prizes/medicine/laureates/1960/medawar-facts.html in chemistry from Washington and Lee University and subsequently, obtained his medical degree at UT Southwestern Medical Center Dallas. He was a resident at Massachusetts General Hospital, where he met Michael S. Brown, who later would become his collaborator and together, they won the Nobel Prize3. During the two following years, he worked at the National Heart, Lung, and Blood Institute of the United States, which contributed to increase his skills and taste for scientific experimentation from the perspective of molecular biology in human disease1,28-30. Michael Stuart Brown was born on April 13, 1941, in Brooklyn, New York. Similarly to Goldstein, he first obtained a degree in chemistry and only then in Medicine. He also worked at the National Heart, Lung, and Blood Institute of the US, but in the area of gastroenterology and hereditary diseases. In biochemistry laboratory, he learned enzymatic manipulation techniques, among which, an enzyme that could be related to familial hypercholesterolemia1,28-30. Goldstein and Brown were awarded the Nobel Prize for scientific research in which they identified receptors on the surface of cells that mediate the uptake of Low-Density Lipoprotein (LDL) circulating in the bloodstream. Furthermore, they found that severe familial hypercholesterolemia is closely related to these receptors, as with the decrease in the number of membrane receptors, there is a lower uptake of circulating cholesterol in the form of LDL, thus increasing levels of the substance in the bloodstream from1,28-30. In this example, once again, one can observe the close association between high cholesterol levels, atherosclerosis, and ischemic heart disease. 192 Arq Bras Cardiol. 2015; 105(2):188-196 James Black, Gertrude Elion and George Hitchings – 1988: beta-blockers James W. Black, from Uddington, Scotland, studied medicine at the University of St. Andrews. In 1948, he started an investigation on cardiac adrenergic alpha and beta receptors, resulting in the synthesis of propranolol, the prototype of beta-blockers, essential medications for the treatment of heart failure and coronary artery disease. Later, in 1976, he concluded the synthesis of cimetidine, histamine H2-receptor antagonist, used in peptic disease treatments. Together with James W. Black, researchers Gertrude B. Elion (New York, United States) and George H. Hitchings (Hoquiam, United States) were also awarded the Nobel Prize of Medicine, for the development of drugs used in chemotherapy, antibiotics and antivirals1,31. Joseph Edward Murray and Edward Thomas – 1990: organ transplantation Joseph Murray was born on April 1st, 1919 in the city of Milford, State of Massachusetts (United States) and died in 2012 due to a stroke. He graduated from Harvard medical school and specialized in plastic surgery. He served in the US military and had a very important role in the care of wounded soldiers in World War II. When caring for burned patients, he observed that many patients responded well to donor skin grafts and decided to develop a research related to organ transplantation. On December 23, 1954, he was part of the team that made the first renal transplantation and, some years Mesquita et al. Nobel Prize and Cardiology Review Article later, the first transplantation using a cadaveric source. Over the years, he participated in studies on immunosuppressive drugs such as azathioprine, aimed at reducing graft rejection1,32. Edward Donall Thomas was born on March 20, 1920, in the city of Mart, State of Texas (United States), and also died in 2012. He graduated from medical school at Harvard and, early in his career, he devoted himself to laboratory studies related to bone marrow transplantation. Together with Joseph Edward Murray, he received the Nobel Prize in Physiology or Medicine as his studies helped to develop the transplantation of organs and tissues. In the field of HF, heart transplantation was indicated for patients that remained very symptomatic despite optimal medical treatment, which was performed for the first time in history in South Africa by Dr. Christiaan Barnard1,32. Robert F. Furchgott, Ferid Murad and Louis J. Ignarro – 1998: nitric oxide The Nobel Prize in Physiology or Medicine in 1998 was awarded jointly to Robert F. Furchgott (Charleston, United States), Louis J. Ignarro (New York, United States) and Ferid Murad (Whiting, United States) due to their findings on Nitric Oxide (NO) as a signaling molecule in the cardiovascular system1. NO is a soluble gas naturally found in the human body, which acts on the signaling of several biological processes. The synthesis of NO occurs through the action of an enzyme called NO synthase (NOS) from L-arginine and L-citrulline amino acids, requiring for this enzymatic reaction, the presence of two cofactors, oxygen and Nicotinamide Adenine Dinucleotide Phosphate (NADPH). There are three types of NOS, two of them called constitutive and calciumdependent NOS (cNOS), which are the endothelial and neuronal forms that synthesize NO in normal conditions and the calcium-independent form (iNOS), which is not expressed or is in a much lesser amount under physiological conditions. NO plays an important role in endothelial homeostasis, contributing with its vasodilating and anticoagulant properties. There is evidence that a decreased NO production is an important factor in ischemic events in patients with coronary artery disease and other suggesting that NO can exert antiatherosclerotic actions. Furthermore, the nitrates, the most widely used drugs in coronary artery disease and heart failure, act by indirectly increasing NO bioavailability33-36. Paul C. Lauterbur and Peter Mansfield – 2003: magnetic resonance Paul Lauterbur was born on May 6, 1929 in the United States, having obtained his PhD in Chemistry at the University of Pittsburgh in Pennsylvania (United States). Throughout his career has received numerous awards for his work related to magnetic resonance, including the gold medal of the Society of Magnetic Resonance in Medicine in 1982, the European Prize of Magnetic Resonance in 1986, the International Society for Magnetic Resonance in Medicine Award in 1992, the gold medal of the European Congress of Radiology in 1999, the NAS Award for Chemistry in Service to Society in 2001 and the Nobel Prize in Physiology or Medicine in 2003 together with Englishman Sir Peter Mansfield1,37-39. Peter Mansfield was born on October 9, 1933 in London and a received his Ph.D. in physics in his hometown in 1962. In the course of his career as an investigator he received several awards, including the Gold Medal of the Society for Magnetic Resonance in Medicine in 1983, the European Prize of Magnetic Resonance in 1988, the title of Sir of the British Crown in 1993, the Gold Medal of the European Congress of Radiology and the European Association of Radiology in 1995 and the Nobel Prize for Physiology and Medicine, for his discoveries related to nuclear magnetic resonance imaging in 20031,37-39. Based on the initial findings of Lauterbur and Mansfield, MRI has developed and now has wide application in cardiology. It is considered, for instance, the gold standard in non-invasive myocardial and heart function assessment. Special Considerations Carlos Chagas – 1911: an unjustly overlooked scientist in relation to the Nobel Prize Carlos Chagas (Figure 3) was the first researcher in the world's scientific history to describe the complete cycle of a disease, currently known as Chagas disease40. His research with Trypanosoma cruzi started between the years 1907 and 1909, when he was sent to the countryside of the state of Minas Gerais to help fight malaria among workers building the Brazilian Central Railway7. In 1909, he identified the parasite in the blood of a child with "fever, anemia, edema and generalized lymphadenopathy" and later described the life cycle of T. cruzi 7. Aided by a small team, he changed history as a scientist that inspired a new era of knowledge, as he was able to draw a clinical profile from his own observations. Throughout his career, he received honors of national importance, such as public health management positions, as well as international prizes, such as the Schauddinn award in Germany, for the most important discovery of protozoology. For these reasons, he was nominated four times for the Nobel Prize, but none fructified. Researchers and historians have assessed, among other sources, files from Oswaldo Cruz Foundation and the Karolinska Institute to identify the reasons why Carlos Chagas was not awarded the Nobel prize6,7,41-43. Bestetti et al.6,7,41,42, in their set of historical publications, solidly based the reasons why Chagas was not a Nobel Prize laureate. These researchers even went to the Swedish institute in person to review the original documents of the time; their research, published in prestigious international journals, are less disseminated than they should be in Brazilian cardiology. Gunnar Hedrèn was the board member of the Karolinska Institute who analyzed and issued an opinion on Chagas’ first nomination for the Nobel Prize in 19216,7. Although there is no formal written opinion, the analysis of documents from that time suggests that the counselor did not value Chagas’ discovery6,7. Although now recognized as renowned researcher, Chagas had opponents in South America and Brazil. A group linked to the Bacteriology Institute in Buenos Aires, including a Brazilian member, Arq Bras Cardiol. 2015; 105(2):188-196 193 Mesquita et al. Nobel Prize and Cardiology Review Article Figure 3 – Carlos Chagas picture. Source: Lagoeiro B, Gemal P. Carlos Chagas. Um homem, uma doença, uma história. Niterói: Ed. UFF; 2012. insisted in the early years of Chagas' discovery, that there was no association between the symptoms reported by Chagas and the presence of T. cruzi6,44. Another group, from the very Oswaldo Cruz Foundation and the School of Medicine of Rio de Janeiro, disagreed with Chagas for political reasons and, on several occasions, questioned the importance of trypanosomiasis6. Among his opponents were Figueiredo de Vasconcellos, Cardoso Fontes and Plinio Marques6. Chagas also lost prestige among the local population for unpopular measures at the time when he was appointed Director of Public Health, an equivalent post at the time of the "Minister of Health". The mandatory vaccine for smallpox was one of those most criticized measures, being even the reason of a popular revolt6,42. Finally, the methods used by the then President of the Karolinska Institute, JE Johansson, are criticized. It is suggested that he excessively valued researches related to physiology, rather than those related to clinical medicine42. A new indication and a Nobel award after Chagas’ death are no longer expected. It persists, though, in the light of the centenary of the discovery by Chagas, our pride in a great Brazilian who, with all the honors and merits, made such a contribution to humankind. Bernard Lown – a brilliant clinical cardiologist that received the Peace Nobel Prize of 1985 Bernard Lown was born on June 7, 1921, in the city of Utena, Lithuania, and moved at age 13 with his family to the USA and settled in the state of Maine, where he became a medical doctor and completed his specialization 194 Arq Bras Cardiol. 2015; 105(2):188-196 in cardiology at the current Brigham and Women's hospital in Boston 1,45. Together with engineer Baruch Berkowitz, in 1961, he created the direct current used in the defibrillator, allowing greater safety and efficacy in relation to the then AC defibrillator created by Paul Zoll. Lown also discovered the correct moment of the cardiac cycle in ECG for the electrical discharge in ventricular tachyarrhythmias. This therapy received the name of "cardioversion". The defibrillator designed by Lown and Berkowitz was used as standard therapy in cardiac arrhythmias until the 1980s, when the models with biphasic current were created. He also has researched the use of lidocaine as an antiarrhythmic drug and the importance of serum potassium in digitalis intoxication. Lidocaine, until then, was basically used as a local anesthetic by dentists. In the presence of HF, electrical therapies are essential in preventing sudden death (of which ventricular dysfunction is one of the most important risk factors) and in the treatment of symptomatic arrhythmias, highly prevalent in this group; digoxin is one of the drugs indicated for patients with reduced ejection fraction and symptomatic ones with functional class III or IV1,45. Despite all these contributions to Medicine, his Nobel Prize was won by other merits: a peacekeeper, he created the International Physicians for the Prevention of Nuclear War, in association with the then Soviet citizen Yevgeniy Chazov. His association has also had the participation of Brazilian physicians. He also published two famous books: “The lost art of healing” and “Prescription for survival: a doctor's journey to end nuclear madness”. He is currently a Professor Emeritus at Harvard University and founder of the Lown Institute, of which mission is described on their website as: “to help set up a sustainable and compassionate health system, where Mesquita et al. Nobel Prize and Cardiology Review Article doctors can serve as healers and lawyers, where patients receive the services they need and are protected from unnecessary treatment and damage, and where financial incentives are removed from clinical decision-making”1,45. Conclusion The Nobel Prize aims to reward researchers whose actions and discoveries have contributed exceptionally to the progress and the good of society. Regarding heart failure, the final pathway of several forms of heart disease, 33 researchers in 16 awards performed studies that yielded great contributions to its diagnosis and treatment. Brazil, despite its growing scientific contributions in recent decades, in the fields of Physiology and Medicine, has no "genuinely" Brazilian laureates, despite the contributions of Dr. Peter Medawar and Dr. Carlos Chagas - the latter unjustly not a recipient of this honor. Author contributions Conception and design of the research:Mesquita ET, Marchese LD, Gismondi RA. Acquisition of data: Marchese LD, Dias DW, Barbeito AB, Gomes JC, Muradas MCS, Gismondi RA. Analysis and interpretation of the data: Mesquita ET, Marchese LD, Gismondi RA. Writing of the manuscript:Mesquita ET, Marchese LD, Dias DW, Barbeito AB, Gomes JC, Muradas MCS, Lanzieri PG, Gismondi RA. Critical revision of the manuscript for intellectual content: Mesquita ET, Marchese LD, Gismondi RA. Potential Conflict of Interest No potential conflict of interest relevant to this article was reported. Sources of Funding There were no external funding sources for this study. Study Association The study is associated with the Post-Graduate Program in Cardiovascular Sciences of Universidade Federal Fluminense. References 1. The Nobel Prize in Physiology or Medicine. [Accessed on 2012 Jul 4]. Available from: http://www.nobelprize.org/nobel_prizes/medicine/ laureates/2014. 2. Noro J. Nobel, o premio o homem: 100 anos de medicina. São Paulo: JSN Editora; 1999. 3. Sade RM. Transplantation at 100 years: Alexis Carrel, pioneer surgeon. Ann Thorac Surg. 2005;80(6):2415-8. 4. Starzl TE. Peter Brian Medawar: father of transplantation. J Am Coll Surg. 1995;180(3):332-6. 5. Kyle RA, Shampo MA. Peter Medawar--discoverer of immunologic tolerance. Mayo Clin Proc 2003;78(4):401-3. 6. Bestetti RB, Cardinalli-Neto A. Dissecting slander and crying for justice: Carlos Chagas and the Nobel Prize of 1921. Int J Cardiol. 2013;168(3):2328-34. 7. Bestetti RB, Martins CA, Cardinalli-Neto A. Justice where justice is due: a posthumous Nobel Prize to Carlos Chagas (1879-1934), the discoverer of American Trypanosomiasis (Chagas’ disease). Int J Cardiol .2009;134(1):9-16. 8. 9. Making the Revolutionary New Carrel-Dakin Wound Treatment Available to Save Soldiers’ Lives During World War I. [Acessed on 2014 Jul 4]. Available from: http://www.kilmerhouse.com/2013/11/making-therevolutionary-new-carrel-dakin-wound-treatment-available-to-savesoldiers-lives-during-world-war-i/ Barold SS. Willem Einthoven and the birth of clinical electrocardiography a hundred years ago. Card Electrophysiol Rev. 2003;7(1):99-104. 14. Galindo CL, Kasasbeh E, Murphy A, Ryzhov S, Lenihan S, Ahmad FA et al. Anti-remodeling and anti-fibrotic effects of the neuregulin-1β glial growth factor 2 in a large animal model of heart failure. J Am Heart Assoc. 2014;3(5):e000773. 15. Yang Y, Zhang H, Li X, Yang T, Jiang Q. Effects of PPARα/PGC-1α on the myocardial energy metabolism during heart failure in the doxorubicin induced dilated cardiomyopathy in mice. Int J Clin Exp Med. 2014;7(9):2435-42. 16. Ventura HO. Dickinson Woodruff Richards and cardiac catheterization. Clin Cardiol. 2007;30(8):420-1. 17. Cournand A. Cardiac catheterization; development of the technique, its contributions to experimental medicine, and its initial applications in man. Acta Med Scand Suppl. 1975;579:3-32. 18. Bourassa MG. The history of cardiac catheterization. Can J Cardiol. 2005;21(12):1011-4. 19. Mueller RL, Sanborn TA. The history of interventional cardiology: cardiac catheterization, angioplasty, and related interventions. Am Heart J. 1995;129(1):146-72. 20. Gottschall CA. 1929-2009: 80 anos de cateterismo cardíaco - uma história dentro da história. Rev Bras Cardiol Invasiva. 2009;17(2):246-68. 21. Norrby E. Nobel Prizes and Life Sciences. Washington, DC: World Scientific; 2010. 22. Norrby E. A century of nobel prizes. Proc Am Philos Soc. 2002;146(4):323-36. 10. Raju TN. The Nobel chronicles. 1953: Hans Adolf Krebs (1900-81) and Fritz Albert Lipmann (1899-1986). Lancet. 1999;353(9164):1628. 23. R a j u T N . T h e N o b e l c h r o n i c l e s - - t h e f i r s t c e n t u r y. L a n c e t .2000;356(9227):436. 11. Leigh FW. Sir Hans Adolf Krebs (1900-81), pioneer of modern medicine, architect of intermediary metabolism. J Med Biogr. 2009;197(3):149-54. 24. Raju TN. The Nobel chronicles. 1964: Konrad Bloch (b 1912) and Feodor Lynen (1911-79). Lancet. 1999;354(9175):347. 12. Finsterer J, Kothari S. Cardiac manifestations of primary mitochondrial disorders. Int J Cardiol. 2014;177(3):754-63. 25. Raju TN. The Nobel chronicles. 1979: Allan MacLeod Cormack (b 1924); and Sir Godfrey Newbold Hounsfield (b 1919). Lancet. 1999;354(9190):1653. 13. Shires SE, Gustafsson ÅB. Mitophagy and heart failure. J Mol Med (Berl). 2015;93(3):253-62. 26. Chast F. [John Vane, 1927-2004, the pharmacologist of the vascular endothelium [corrected]]. Ann Pharm Fr. 2006;64(6):416-24. Arq Bras Cardiol. 2015; 105(2):188-196 195 Mesquita et al. Nobel Prize and Cardiology Review Article 27. Raju TN. The Nobel chronicles. 1982: Sune Karl Bergström (b 1916); Bengt Ingemar Samuelsson (b 1934); John Robert Vane (b 1927). Lancet. 1999;354(9193):1914. 28. Raju TN. The Nobel chronicles. 1985: Joseph Leonard Goldstein (b 1940), Michael Stuart Brown (b 1941). Lancet. 2000;355(9201):416. 29. Lefkowitz R, Goldstein J, Brown M. A conversation with Robert Lefkowitz, Joseph Goldstein, and Michael Brown. Interview by Ushma S. Neil and Howard A. Rockman. J Clin Invest. 2012;122(5):1586-7. 30. Cortés V, Vásquez T, Arteaga A, Nervi F, Rigotti A. [The contribution of Goldstein and Brown to the study of cholesterol metabolism]. Rev Med Chil. 2012;140(8):1053-9. 31. Raju TN. The Nobel chronicles. 1988: James Whyte Black, (b 1924), Gertrude Elion (1918-99), and George H Hitchings (1905-98). Lancet. 2000;355(9208):1022. 32. Raju TN. The Nobel chronicles. 1990: Joseph Edward Murray (b 1919) and E Donnall Thomas (b 1920). Lancet. 2000;355(9211):1282. 33. Dias RG, Negrão CE, Krieger MH. Nitric oxide and the cardiovascular system: cell activation, vascular reactivity and genetic variant. Arq Bras Cardiol. 2011;96(1):68-75. 196 36. Bian K, Doursout M-F, Murad F. Vascular system: role of nitric oxide in cardiovascular diseases. J Clin Hypertens (Greenwich). 2008;10(4):304-10. 37. Pincock S. US and UK researchers share Nobel prize. Paul C Lauterbur and Peter Mansfield share award for seminal work on MRI. Lancet. 2003;362(9391):1203. 38. Wehrli FW. On the 2003 Nobel Prize in medicine or physiology awarded to Paul C. Lauterbur and Sir Peter Mansfield. Magn Reson Med. 2004;51(1):1-3. 39. Geva T. Magnetic resonance imaging: historical perspective. J Cardiovasc Magn Reson. 2006;8(4):573-80. 40. Lagoeiro B, Gemal P. Carlos Chagas. Um homem, uma doença, uma historia. Niteroi: Ed. UFF; 2012. 41. Bestetti RB, Cardinalli-Neto A. Did death hinder the process of justice? Carlos Chagas and the Nobel Prize of 1935. Int J Cardiol. 2011;147(1):172-3. 42. Bestetti RB, Couto LB, Cardinalli-Neto A. When a misperception favors a tragedy: Carlos Chagas and the Nobel Prize of 1921. Int J Cardiol 2.013;169(5):327-30. 43. Coutinho M, Freire O, Dias JC. The noble enigma: Chagas’ nominations for the Nobel prize. Mem Inst Oswaldo Cruz. 1999;94 Suppl 1:123-9. 34. Li H, Horke S, Förstermann U. Vascular oxidative stress, nitric oxide and atherosclerosis. Atherosclerosis. 2014;237(1):208-19. 44. Kraus R, Maggio C, RosenbuschF. Bocio, cretinismo y enfermedad de Chagas. Prensa Med Argent. 1915;2:2-5. 35. Mitka M. 1998 NObel Prize winners are announced: three discoverers of nitric oxide activity. JAMA. 1998;280(19):1648. 45. Lown Institute. [Accessed on 2014 Jul 4]. Available from: http://www. lowninstitute.org. Arq Bras Cardiol. 2015; 105(2):188-196 Back to the Cover Viewpoint Sudden Death in Brazil: Epilepsy Should be in Horizon Fulvio Scorza and Paulo José Ferreira Tucci Escola Paulista de Medicina – Unifesp, São Paulo, SP - Brazil To date, a considerable amount of valuable information about the problem of sudden cardiac death (SCD) has been described. The incidence of SCD in the United States ranges between 180000-400000 cases per year 1. Martinelli et al demonstrated an incidence of 21270 cases of SCD per year in the Metropolitan Area of São Paulo2. Recently, Braggion-Santos et al.3 described the characteristics of SCD in Ribeirão Preto, Brazil, according to autopsy reports3. Revising 4501 autopsies, they identified 899 cases of SCD (20%); the rate was 30/100000 residents/year3. The vast majority of SCD cases involved coronary artery disease (64%). Based on available scientific knowledge related to SCD, it is extremely important to identify new areas of research that might improve understanding of this problem and to establish effective preventive measures to minimize or even control the occurrence of SCD. Although studies have shown that the increase in the number of SCD caused by a combination of factors2,3, an equally important risk factor for SCD which is not reported and not explored in cardiologic research is epilepsy. Indeed, a series of data could be put forward to explain it. Epilepsy affects approximately 65 million individuals worldwide and is one of the most common, chronic and severe neurological diseases4-7. In developing and poor countries, the incidence of epilepsy is higher when compared with that of developed countries4-7. The prognostic evolution has clearly shown that seizures are successfully controlled with currently available antiepileptic drugs in approximately two-thirds of individuals with epilepsy, which results in one-third with refractory epilepsy4,8. For these patients with uncontrolled seizures, epilepsy should be considered a malignant condition, as it carries a mortality rate that is 2‑3 times higher than that in the general population9. Therefore, sudden unexpected death in epilepsy (SUDEP) is the most frequent cause of epilepsy-related death9-12. By definition, SUDEP is a sudden, unexpected, witnessed or unwitnessed, non‑traumatic and non-drowning death in individuals with epilepsy, with or without evidence of seizures, in which post-mortem examination does not reveal a toxicological or anatomical cause of death 13. Keywords Death, Sudden / prevention & control; Death, Sudden, Cardiac; Coronary Artery Disease / mortality; Epilepsy / mortality. Mailing Address: Paulo José Ferreira Tucci • Escola Paulista de Medicina – UNIFESP. Rua Estado de Israel, 181/94, Vila Clementino. Postal Code 04022-000, São Paulo, SP – Brazil E-mail: [email protected], [email protected] Manuscript received February 05, 2015; revised March 18, 2015; accepted March 30, 2015. DOI: 10.5935/abc.20150072 197 Epidemiological studies indicate that SUDEP is responsible for 7.5% to 17% of all deaths in epilepsy and has an incidence among adults between 1:500 and 1:1000 patient/year14. The main risk factors for SUDEP include the number of generalized tonic–clonic seizures, nocturnal seizures, young age at epilepsy onset, longer duration of epilepsy, dementia, absence of cerebrovascular disease, asthma, male gender, symptomatic etiology of epilepsy and alcohol abuse12,15. The cause or causes of SUDEP are still unknown, but one of the main proposed mechanisms is related to autonomic dysregulation, promoting cardiac abnormalities during and between seizures16-18. In this line of reasoning, our experimental data clarified some possibilities. Using the pilocarpine model of temporal lobe epilepsy, we evaluated heart rate in rats with epilepsy in vivo and in an isolated ex vivo preparation (Langendorff preparation)17. Baseline heart rate in vivo in animals with chronic epilepsy (346 ± 7 bpm) was higher than in control rats (307 ± 9 bpm) 17. Incidentally, no difference was observed in the isolated ex vivo situation (control animals: 175 ± 7 bpm; chronic epilepsy: 176 ± 6 bpm), suggesting that autonomic modulation of the heart is altered in epileptic animals, explaining the maintenance of an increased basal heart rate in these animals17. In addition, we also evaluated heart rate responses during stage 5 of amygdala kindling model, the phase when animals develop generalized seizures18,19. Animals did not show significant differences in basal heart rate; however, basal heart rate was higher during stage 5 of kindling, possibly resulting from sympathetic activation caused by the chronic epileptic condition 18,19. As demonstrated in previous studies20, intense bradycardia at the beginning of seizure was followed by rebound tachycardia18,19. Moreover, the intensity of tachycardia was directly related to the number of generalized seizures, suggesting that repeated generalized tonic-clonic seizures affect sympathetic outflow18,19. For that reason, a plausible explanation is that continuous and intermittent sympathetic activation due to uncontrolled seizures is capable of maintaining cardiac rhythm, modulating the heart in accelerated-state permanently. Considering all these translational information, it is clear that epilepsy-related mortality, particularly SCD, is a significant public health concern. Thus, it is crucial that a concerted and collaborative approach be implemented to solve this problem. In order to do so, it is extremely necessary to attain a real convergence between cardiologists and neurologists to carefully evaluate and discuss the electroencephalographic and electrocardiographic recordings, the cardiac and cerebral imaging findings and refined histopathological studies in order to detect or prevent the occurrence of a tragic fatal event among individuals with epilepsy. Scorza & Tucci Epilepsy and sudden cardiac death Viewpoint Acknowledgements This study has been supported by: UNIFESP, FAPESP (Fundação de Amparo à Pesquisa do Estado de São Paulo); CNPq (Conselho Nacional de Desenvolvimento Científico e Tecnológico); CEPID/FAPESP; FAPESP/ PRONEX and FAPESP/CNPq/MCT (Instituto Nacional de Neurociência Translacional). Author contributions Conception and design of the research:Scorza F, Tucci PJF. Acquisition of data:Scorza F. Analysis and interpretation of the data: Scorza F, Tucci PJF. Statistical analysis: Scorza F. Writing of the manuscript:Scorza F, Tucci PJF. Critical revision of the manuscript for intellectual content: Tucci PJF. Potential Conflict of Interest No potential conflict of interest relevant to this article was reported. Sources of Funding This study was funded by FAPESP, CNPq, Capes e Unifesp. Study Association This study is not associated with any thesis or dissertation work. References 1. Chugh SS, Reinier K, Teodorescu C, Evanado A, Kehr E, Al Samara M, et al. Epidemiology of sudden cardiac death: clinical and research implications. Prog Cardiovasc Dis. 2008;51(3):213-28. 12. Hesdorffer DC, Tomson T, Benn E, Sander JW, Nilsson L, Langan Y, et al. Commission on Epidemiology; Subcommission on Mortality. Combined analysis of risk factors for SUDEP. Epilepsia. 2011;52(6):1150-9. 2. 13.Nashef L. Sudden unexpected death in epilepsy: terminology and definitions. Epilepsia. 1997;38(11 Suppl):S6-8. Martinelli M, Siqueira SF, Zimerman LI, Neto VA, Moraes AV Jr, Fenelon G. Sudden cardiac death in Brazil: study based on physicians’ perceptions of the public health care system. Pacing Clin Electrophysiol. 2012;35(11):1326-31. 3. Braggion-Santos MF, Volpe GJ, Pazin-Filho A, Maciel BC, Marin-Neto JA, Schmidt A. Sudden cardiac death in Brazil: a community-based autopsy series (2006-2010). Arq Bras Cardiol. 2015;104(2):120-7. 4. Laxer KD, Trinka E, Hirsch LJ, Cendes F, Langfitt J, Delanty N, et al. The consequences of refractory epilepsy and its treatment. Epilepsy Behav. 2014;37:59-70. 5. Banerjee PN, Filippi D, Allen Hauser W. The descriptive epidemiology of epilepsy -- a review. Epilepsy Res. 2009;85(1):31-45. 6. Forsgren L, Beghi E, Oun A, Sillanpää M. The epidemiology of epilepsy in Europe -- a systematic review. Eur J Neurol. 2005;12(4):245-53. 7. Sander JW. The epidemiology of epilepsy revisited. Curr Opin Neurol. 2003;16(2):165-70. 8. Kwan P, Sander JW. The natural history of epilepsy: an epidemiological view. J Neurol Neurosurg Psychiatry. 2004;75(10):1376-81. 9. Gaitatzis A, Sander JW. The mortality of epilepsy revisited. Epileptic Disord. 2004;6(1):3-13. 14. Schuele SU, Widdess -Walsh P, Bermeo A, Lüders HO. Sudden unexplained death in epilepsy: the role of the heart. Cleve Clin J Med. 2007;74(Suppl 1):S121-7. 15. Hesdorffer DC, Tomson T. Sudden unexpected death in epilepsy: potential role of antiepileptic drugs. CNS Drugs. 2013;27(2):113-9. 16. Surges R, Taggart P, Sander JW, Walker MC. Too long or too short? New insights into abnormal cardiac repolarization in people with chronic epilepsy and its potential role in sudden unexpected death. Epilepsia. 2010;51(5):738-44. 17. Colugnati DB, Gomes PA, Arida RM, de Albuquerque M, Cysneiros RM, Cavalheiro EA, et al. Analysis of cardiac parameters in animals with epilepsy: possible cause of sudden death? Arq Neuropsiquiatr. 2005;63(4):1035-41. 18. Pansani AP, Colugnati DB, Sonoda EY, Arida RM, Cravo SL, Schoorlemmer GH, et al. Tachycardias and sudden unexpected death in epilepsy: a gold rush by an experimental route. Epilepsy Behav. 2010;19(3):546-7. 19. Pansani AP, Colugnati DB, Schoorlemmer GH, Sonoda EY, Cavalheiro EA, 10. Nashef L, Ryvlin P. Sudden unexpected death in epilepsy (SUDEP): update and reflections. Neurol Clin. 2009;27(4):1063-74. Arida RM, et al. Repeated amygdala-kindled seizures induce ictal rebound 11. Nei M, Hays R. Sudden unexpected death in epilepsy. Curr Neurol Neurosci Rep. 2010;10(4):319-26. 20. Devinsky O. Effects of seizures on autonomic and cardiovascular function. Epilepsy Curr. 2004;4(2):43–6. tachycardia in rats. Epilepsy Behav. 2011;22(3):442-9. Arq Bras Cardiol. 2015; 105(2):197-198 198 Back to the Cover Clinicoradiological Session Case 6 / 2015 – A 27-Year-Old Male Patient with Double Aortic and Pulmonary Valve Lesion after Double Valvotomy in Childhood Edmar Atik Clínica Privada Dr. Edmar Atik, São Paulo, SP – Brazil Clinical data: The patient underwent correction of congenital pulmonary and aortic valve stenosis, both with manifestations, at 7 years of age. Afterwards, there was progressive residual lesion of both valves, with predominance of regurgitation, and development of acute arrhythmias such as paroxysmal atrial fibrillation, in addition to ventricular extrasystoles. The obstructions were significant, with pressure gradients of 90 and 60 mmHg in the pulmonary and aortic valves, respectively. The patient was asymptomatic, and the loud systolic murmur was accompanied by thrill all over the precordium and neck vessels. There was right ventricular overload on the electrocardiogram (ECG). Double valvoplasty in the three-leaflet valves resulted in a good anatomical solution initially. To date, the patient reports shortness of breath on moderate exertion and precordial palpitations. He is on antiarrhythmic drug (amiodarone), after atrial fibrillation was controlled. Physical examination: Good general state of health, normal breathing, acyanotic, normal pulses. Weight: 77 kg; height: 181 cm; blood pressure (BP): 110/70 mmHg; and heart rate (HR): 51 bpm. The aorta (Ao) was moderately palpable on the suprasternal notch. The apical impulse was not palpable on the precordium, and there were mild systolic impulses on the left sternal border. Heart sounds were normal, and there was a grade 1-2/4 coarse systolic murmur in the pulmonic and aortic areas, and a grade 1-2/4 coarse diastolic murmur along the left sternal border. The liver was not palpable and the lungs were clear to auscultation. Laboratory tests: Electrocardiogram showed normal sinus rhythm and signs of left anterior hemiblock, with no chamber overload, and normal ventricular repolarization. PA: +20o, QRSA: -60o, TA: +40o. QRS complex duration was 0.11”, PR = 0.16” and QTc = 0.45” (Figure 1). Chest radiograph showed moderately enlarged cardiac silhouette due to enlarged atrial and ventricular arches; the Keywords Pulmonary Valve Stenosis; Aortic Valve Stenosis; Balloon Valvoplasty; Heart Defects, Congenital. Mailing address: Edmar Atik • Rua Dona Adma Jafet, 74, conj. 73, Bela Vista. Postal Code 01308-050. São Paulo, SP – Brazil E-mail: [email protected]; [email protected] Manuscript received July 23, 2014; revised manuscript October 06, 2014; accepted October 06, 2014. DOI: 10.5935/abc.20140214 199 pulmonary vascular network was normal. Cardiomegaly progressed since the surgical correction, and the current cardiothoracic ratio was 0.58 (Figure 1). Echocardiogram showed dilated right and left cardiac chambers (right ventricle − RV = 35, left atrium − LA = 46; left ventricle − LV = 64; Ao = 31 mm); RV ejection fraction (RVEF) of 53% (Simpson’s method); LV ejection fraction (LVEF) of 58%; RV- pulmonary trunk (PT) pressure gradient of 14 mmHg; LV - Ao pressure gradient of 15 mmHg; and severe pulmonary and aortic regurgitation. The pulmonary systolic pressure was 40 mmHg. Ascending aorta and PT dilatation (40-mm diameter). Magnetic resonance imaging (Figure 2) also showed enlargement of right and left cardiac chambers with preserved ventricular function. RV end-diastolic volume of 200 mL/m2, LV end-diastolic volume of 211 mL/m2, RVEF of 54% and LVEF of 58%. Ascending aorta of 45 mm, and PT of 36 mm. 24-hour dynamic ECG (Holter monitoring) showed 627 ventricular extrasystoles and 121 supraventricular extrasystoles. Two episodes of non-sustained ventricular tachycardia with 6 complexes and two of atrial tachycardia with 16 complexes. Clinical diagnosis: Double pulmonary and aortic valve lesion with manifestations, showing signs of progressive dilatation of both ventricles, in late course after surgical correction in childhood. Clinical reasoning: during the course of the disease, the clinical elements were consistent with the diagnosis of double pulmonary and aortic valve lesion, with predominance of the first. Shortness of breath and development of ventricular arrhythmias and paroxysmal atrial fibrillation are related to the residual lesions, which progressively increased since childhood. Noteworthy, despite the evident biventricular dilatation, no electrical overload of these chambers was observed. Perhaps both ventricular dilatations had electrically counterbalanced one another. Differential diagnosis: Concomitant lesion of both semilunar valves as congenital defects is usually associated with some genetic syndrome, which was not the case. Residual lesions of both valves commonly occur after correction of obstructive defects alone or in association, as occurs in the tetralogy of Fallot. Management: in view of the progression of the residual defects with excessive dilatation of both ventricles, although with biventricular function still preserved, a surgical approach was chosen with valve replacement for a mechanical prosthetic valve in the aortic position and for a biological prosthetic valve in the pulmonary position. Because of the ascending aorta dilatation, a dacron tube was inserted inside the vessel. Edmar Atik Double aortic and pulmonary valve lesion Clinicoradiological Session Figure 1 – Chest radiograph shows moderate enlargement of the cardiac silhouette. Electrocardiogram shows left anterior hemiblock, with no signs of cardiac overload. Commentaries: residual valve regurgitation after surgical or percutaneous valvotomy, whether pulmonary or aortic, has become a common outcome that requires the performance of other operative techniques, such as Ross’ technique. It is estimated that approximately 30% of these patients undergoing heart valve correction require surgical reintervention to prevent further progression of the heart valve defects, which ultimately result in ventricular dilatation and dysfunction. The reintervention usually implies the need for valve replacement. The values currently recommended to prevent further deterioration of the ventricular function are 120 mL/m2 for the end-diastolic volume and of 90 mL/m2 for the end-systolic volume. In practice, however, we have observed much higher values until surgical reintervention is indicated, as incidentally occurred in the present case. Ideally, these patients should be duly monitored, in order to follow the parameters recommended for a more favorable outcome in the long term. Arq Bras Cardiol. 2015; 105(2):199-201 200 Edmar Atik Double aortic and pulmonary valve lesion Clinicoradiological Session Figure 2 – Magnetic resonance imaging shows clear enlargement of the right and left ventricles, with preserved function of both, in four-chamber and cross-sectional views. 201 Arq Bras Cardiol. 2015; 105(2):199-201 Back to the Cover Case Report Profound Sustained Hypotension Following Renal Denervation: A Dramatic Success? Ganiga Srinivasaiah Sridhar1, Timothy Watson1,2, Chee Kok Han1, Wan Azman Wan Ahmad1 Departamento de Cardiologia - Universidade Malaya Medical Center - Kuala Lumpur Malaysia1; Departamento de Medicina - Universidade de Auckland - Auckland, New Zealand2 Introduction A 67-year-old woman with drug-refractory essential hypertension was admitted for renal sympathetic denervation (RDN). The secondary causes of hypertension were fully investigated in this patient. A 24-h ambulatory blood pressure (BP) monitor documented a mean daytime BP of 172/101 mmHg, a mean nighttime BP of 151/84 mmHg, and an overall mean BP of 167/97 mmHg despite compliance with metoprolol (50 mg twice daily), amlodipine (10 mg once daily), lisinopril (20 mg once daily), prazosin (2 mg thrice daily), and hydrochlorothiazide (50 mg once daily). The patient was fasted for 4 h. Her usual antihypertensive drug therapy was continued. After the administration of 5,000 international units of heparin and 100 μg of fentanyl, a 7-F Renal Double Curve guide catheter (Cordis Corporation, Fremont, CA ,USA) was inserted into the right renal artery (no accessory vessel). A 0.014-in Runthrough floppy guide wire (Terumo Medical Corporation, Somerset, NJ, USA) was advanced into place. A 6-mm ONESHOTTM (Covidien, Mansfield, MA, USA) irrigated RDN balloon was advanced into place (Figure 1), and a single ablation was performed. The procedure was then repeated on the other side. The patient remained hemodynamically stable throughout and at the completion of the procedure with a BP of 150/80 mmHg. Hemostasis was achieved with the Perclose ProGlide Suture-Mediated Closure System (Abbott Vascular, Santa Clara, CA, USA), and the patient was then returned to our ward for monitoring. One hour later, the patient complained of dizziness and blurring of vision. Her Glasgow Coma Scale score remained 15 with preserved mentation. She was not in pain. Her pulse rate was 87 bpm, and her BP was 77/38 mmHg. However, she appeared well perfused and was clinically euvolemic. There was no evidence of a groin hematoma, and her abdomen was soft. A 12-lead electrocardiogram showed no change, and a transthoracic echocardiogram Keywords Hypertension; Sympatectomy; Medication Therapy; Management; Hypotension. Mailing Address: Timothy Watson • Department of Cardiology, University Malaya, Lembah Pantai, Postal Code 59100, Kuala Lumpur, Malaysia Email: [email protected] Manuscript received July 26, 2014; revised manuscript August 21, 2014; accepted October 06, 2014. DOI: 10.5935/abc.20150100 202 showed normal left ventricular function. Her hemoglobin level was similar to baseline, and her arterial blood gas levels, including lactate, were unremarkable. She was given intravenous dopamine that was titrated to response. At 10 μg/kg/min, her BP rose to 120/70 mmHg, and her symptoms resolved entirely. Over the subsequent 48 h, she was extremely sensitive to reductions in the dose of dopamine and exhibited a markedly fluctuating BP. However, by 72 h, the dopamine had been carefully weaned and discontinued. She was discharged home after she remained stable for a further 24 h. At a 3-month review, she remains well with a mean daytime office BP of 124/72 mmHg while on amlodipine (5 mg once daily). Discussion Around 12% of patients with essential hypertension who are considered resistant to conventional therapy have persistently elevated BP despite the use of three or more pharmacological agents1,2. In such instances, abnormal renal excretory function, which is largely influenced by renal sympathetic nerve activity, may have a central role3. Catheter-based RDN, which is a modern incarnation of a historically effective treatment, has recently emerged as a novel therapeutic strategy. Proof of concept and subsequent randomized (unblinded) data that were collected while using the Symplicity® catheter (Medtronic, Inc., Minneapolis, MN, USA) have demonstrated reductions in office BP of 20/10, 24/11, 25/11, and 23/11 mmHg at 1, 3, 6, and 12 months, respectively, in a group of patients taking an average of five antihypertensive drugs4,5. Such early exciting reports have stimulated the development of numerous other similar devices, including the ONESHOTTM catheter that was used in this case6. In some cases, early BP reductions have been reported following RDN. However, in other cases, the response is not always immediate, or it can take several months to appear. Additionally, RDN is associated with a failure rate of 10%–30%, and the only predictor of response in early studies is the magnitude of the systolic BP elevation at baseline7. Explanations for this broad variability in outcome are uncertain, except that raw BP measurements may lack the sensitivity required for them to be considered a true measure of successful RDN8. This may in part explain the lackluster performance of RDN in the Symplicity-3 trial, in which RDN failed to demonstrate superiority over conventional treatments when compared to a sham-control procedure9. However, despite this, the use of RDN does seem to significantly reduce renal norepinephrine spillover10. Therefore, it is possible that those patients who exhibit more sympathetic over-activity may experience a greater degree of BP reduction with RDN. Because sympathetic over-activity is not routinely measured in clinical practice, this remains speculative. Sridhar et al. Dramatic success of RDN Back to the Cover Case Report Right Kidney Left Kidney Figure 1 – Renal Denervation Procedure. Selective angiography performed with a 7-F Renal Double Curve guide catheter in the left anterior oblique 10° projection. Note that a single renal artery supplies each kidney and that the caliber and length of the main renal artery prior to bifurcation is ideally suited to denervation. Nonetheless, the role of RDN in the treatment of resistant hypertension remains uncertain, but the sustained and impressive BP reductions that were observed in this and other cases should encourage further research to improve the understanding of the mechanisms through which hypertension is mediated and to identify those patients who are likely to achieve the most dramatic responses with RDN. Potential Conflict of Interest No potential conflict of interest relevant to this article was reported. Sources of Funding There were no external funding sources for this study. Author contributions Study Association Acquisition of data: Sridhar GS, Han CK, Ahmad WAW; Writing of the manuscript: Sridhar GS, Watson T, Han CK, Ahmad WAW; Critical revision of the manuscript for intellectual content: Watson T. This study is not associated with any thesis or dissertation work. Arq Bras Cardiol. 2015; 105(2):202-204 203 Sridhar et al. Dramatic success of RDN Case Report References 1. Persell SD. Prevalence of resistant hypertension in the United States, 20032008. Hypertension. 2011;57(6):1076-80. 2. Mancia G, Fagard R, Narkiewicz K, Redon J, Zanchetti A, Böhm M, et al. 2013 ESH/ESC guidelines for the management of arterial hypertension: the Task Force for the Management of Arterial Hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). Eur Heart J. 2013;34(28):2159-219. 3. DiBona GF. The sympathetic nervous system and hypertension: recent developments. Hypertension. 2004;43(2):147-50. 4. Krum H, Barman N, Schlaich M, Sobotka P, Esler M, Mahfoud F, et al; Symplicity HTN-1 Investigators. Catheter-based renal sympathetic denervation for resistant hypertension: durability of blood pressure reduction out to 24 months. Hypertension. 2011;57(5):911-7. 5. 204 Esler MD, Krum H, Sobotka PA, Schlaich MP, Schmieder RE, Bohm M. Renal sympathetic denervation in patients with treatment-resistant hypertension (The Symplicity HTN-2 Trial): a randomised controlled trial. Lancet. 2010;376(9756):1903-9. Arq Bras Cardiol. 2015; 105(2):202-204 6. Ormiston JA, Watson T, van Pelt N, Stewart R, Stewart JT, White JM, et al. Renal denervation for resistant hypertension using an irrigated radiofrequency balloon: 12-month results from the Renal Hypertension Ablation System (RHAS) trial. Eurointervention. 2013;9(1):70-4. 7. Thomas G, Shishehbor MH, Bravo EL, Nally JV. Renal denervation to treat resistant hypertension: guarded optimism. Cleve Clin J Med. 2012;79(7):501-10. 8. Sathananthan J, Watson T, Whitbourn RJ, Stewart JT, Doughty RN, Ormiston JA, et al. Renal sympathetic denervation: indications, contemporary devices and future directions. Interv Cardiol. 2014;6(1):57-69. 9. Bhatt DL, Kandzari DE, O’Neill WW, D’Agostino R, Flack JM, Katzen BT, et al; SYMPLICITY HTN-3 Investigators. A controlled trial of renal denervation for resistant hypertension. N Engl J Med. 2014;370(15):1393-401. 10. Krum H, Schlaich M, Whitbourn R, Sobotka PA, Sadowski J, Bartus K, et al. Catheter-based renal sympathetic denervation for resistant hypertension: a multicentre safety and proof-of-principle cohort study. Lancet. 2009;373(9671):1275-81. Back to the Cover Imagem Giant Right Atrial Mass Following Surgical Aortic Valve Replacement Teresa Bastante and Fernando Alfonso Hospital Universitario de La Princesa, Madrid – Spain A 75-year-old man underwent elective biological aortic valve replacement. Two weeks after surgery, transthoracic echocardiography (TTE) showed a small pericardial effusion. On the following day, the patient suffered from syncope. A repeated TTE revealed a “giant” echo-dense mass (90x80 mm) occupying the entire right atrium and severely limiting tricuspid valve inflow. Although the initial differential diagnosis included the development of an intracavitary process, the rapidly-growing mass with a characteristic echo‑lucent layer at its atrial aspect (consistent with the atrial wall and visceral pericardium) (arrows) led to the final diagnosis of a pericardial hematoma mimicking a huge atrial mass. Emergency surgical exploration confirmed the diagnosis. Author contributions Acquisition of data: Bastante T. Analysis and interpretation of the data: Bastante T. Writing of the manuscript: Bastante T, Alfonso F. Critical revision of the manuscript for intellectual content: Bastante T, Alfonso F. Supervision / as the major investigador: Alfonso F. Potential Conflict of Interest No potential conflict of interest relevant to this article was reported. Sources of Funding There were no external funding sources for this study. Keywords Aortic Valve/surgery; Pericardial Effusion; Heart Atria/ abnormalities. Study Association This study is not associated with any thesis or dissertation work. Mailing Address: Fernando Alfonso • Hospital Universitario de La Princesa. C. Diego de Leon, 62, Madrid. Postal Code 28006. Madrid – Spain E-mail: [email protected] Manuscript received March 09, 2015; revised manuscript March 13, 2015; accepted March 24, 2015. DOI: 10.5935/abc.20150066 Figure 1 – Transthoracic echocardiography: giant eco-dense mass occupying the entire right atrium (Panel A) and severely limiting tricuspid valve inflow (Panel B). Atrial wall and visceral pericardium (arrows) 205 Back to the Cover Letter to the Editor Subclinical Ventricular Dysfunction Detected by Speckle-Tracking Two Years after Use of Anthracycline Aguinaldo Figueiredo Freitas Jr., Raquel Oliveira Santos, Salvador Rassi Serviço de Cardiologia da Faculdade de Medicina da Universidade Federal de Goiás, Goiânia, Goiás - Brazil Dear Editor We would like to congratulate the authors for the publication of their article “Subclinical Ventricular Dysfunction Detected by Speckle-Tracking Two Years after Use of Anthracycline”, considering the great practical applicability of the theme. Cardiotoxicity secondary to chemotherapy drugs is a reality that imposes, on cardiologists and oncologists, the challenge of prevention and/or early detection of this complication, which has high morbidity and mortality1. In this regard, we read with interest the abovementioned article, which highlights the usefulness of speckle-tracking to attain an early diagnosis of subclinical ventricular dysfunction, Keywords Heart Failure; Ventricular Dysfunction Left/chemically induced; Echocardiography; Anthracyclines/adverse effects. Mailing Address: Aguinaldo Figueiredo de Freitas Junior • Rua T-51, n 964 – apto. 1902, Bueno. Postal Code 74215-210, Goiânia, GO – Brazil E-mail: [email protected], [email protected] Manuscript received May 11, 2015; revised manuscript June 29, 2015; accepted June 29, 2015. although this finding does not directly imply in implementing treatment due to the lack of current scientific evidence, which makes studies in this area even more important. However, we would like to point out some aspects to add to the scientific information brought on by this article. In the Results section, the authors demonstrate that almost 80% of patients had also received cyclophosphamide as a chemotherapy drug, an alkylating agent that may be associated with ventricular dysfunction rates of up to 25% of the cases2,3, which cannot be minimized in the Discussion and Conclusion sections of this study. This same rationale can be applied to the more than 50% of patients receiving radiotherapy in the mediastinal region, regardless of the treated hemithorax, since the incidence of coronary heart disease in these patients is a side effect of significant incidence4. We also observed a high rate of hypertension in both groups of patients and controls and that the systolic and diastolic BP levels were higher in the latter than in the first group. We would like to know if there was any difference between the groups regarding the class of antihypertensive drug used, as data in the literature suggest some protective effect of ACE inhibitors and beta-blockers on the incidence of ventricular dysfunction and major clinical outcomes5. DOI: 10.5935/abc.20150102 References 1. Vejpongsa P, Yeh ET. Topoisomerase 2: a promising molecular target for primary prevention of anthracycline-induced cardiotoxicity. Nature. 2014;95(1):45-52. 206 2. Kalil Filho R, Hajjar LA, Bacal F, Hoff PM, Diz Mdel P, Galas FR, et al; Sociedade Brasileira de Cardiologia. I Brazilian guideline for cardio‑oncology from Sociedade Brasileira de Cardiologia. Arq Bras Cardiol. 2011;96(2 Suppl1):1-52. 3. Gardner SF, Lazarus HM, Bednarczyk EM, Creger RJ, Miraldi FD, Leisure G, et al. High-dose cyclophosphamide-induced myocar- dial damage during BMT: assessment by positron emission tomography. Bone Marrow Transplant. 1933;12(2):139-44. 4. Kirova YM. Recent advances in breast cancer radiotherapy: evolution or revolution, or how to decrease cardiac toxicity? World J Radiol. 2010;2(3):103-8. 5. Kalam K, Marwick TH. Role of cardioprotective therapy for prevention of cardiotoxicity with chemotherapy: A systematic review and meta‑analysis. Eur J Cancer. 2013;49(13):2900-9. Freitas Jr. et al. Subclinical ventricular dysfunction and anthracyclines Letter to the Editor Reply Dear authors We appreciate your interest and comments about our article. Cyclophosphamide-associated cardiotoxicity presents as a syndrome of heart failure, myocarditis, pericarditis, or their association and can lead to death. It has an acute onset, with signs and symptoms occurring within one to ten days after the first dose, lasting for approximately one week1. Delayed cardiotoxicity development (> 3 weeks) is very rare in patients that survive the initial event2-4. In our sample, patients were assessed after a median of two years after the end of chemotherapy, making it unlikely that the obtained results can be attributed to the use of cyclophosphamide. The observation about the increased incidence of coronary artery disease (CAD), as a side effect of radiotherapy in patients with breast cancer is absolutely pertinent. This increase is proportional to the number of cardiovascular risk factors the patients have and the mean dose of radiation to the heart. Previous data demonstrated that CAD development after radiation therapy occurred after a longer period of follow-up: 82 months, on average5. Recently, Darby et al6 showed an increase of 16.3% (per Gray of radiation) in the rate of major coronary events in the first four years after radiation therapy in women with breast cancer6. This increase begins in the first five years after radiotherapy and persists for at least 20 years6. The development of new technologies in the field of radiation therapy has shown to be favorable to reduce this side effect7. In our study, however, none of the patients had coronary event during the study period. Although there was no difference in the percentage of participants considered hypertensive in both groups (p = 0.71), the controls had higher levels of systolic and diastolic BP at the time of evaluation. As stated in the Discussion section, we attribute this fact to greater adherence to antihypertensive therapy among patients who were undergoing more stringent medical follow-up in the post-chemotherapy period. The increase in blood pressure levels tends to compromise strain values8. However, despite these higher blood pressure levels in the control group, the strain values were more compromised in the group using doxorubicin (DOX), which reinforces the importance of this drug as an independent predictor of reduced εLL and εCC in our patients. There was no significant difference between the groups regarding the class of antihypertensive drug used: fourteen patients (34%) from the control group used angiotensin‑converting enzyme inhibitors or Angiotensin II‑receptor blockers vs. ten patients (25%) in the group treated with DOX (p = 0.367). One (2.4%) participant from the control group used a beta-blocker vs. five (12.5%) in the DOX group (p = 0.109). Sincerely, André L C Almeida Edval Gomes dos Santos Júnior References 1. Ayash LJ, Wright JE, Tretyakov O, Gonin R, Elias A, Wheeler C, et al. Cyclophosphamide pharmacokinetics: correlation with cardiac toxicity and tumor response. J Clin Oncol 1992;10(6):995-1000. 5. Kalil Filho R, Hajjar LA, Bacal F, Hoff PM, Diz M del P, Galas FR, et al; Sociedade Brasileira de Cardiologia. I Brazilian guideline for cardio‑oncology from Sociedade Brasileira de Cardiologia. Arq Bras Cardiol. 2011;96(2 Supll.1):1-52. 2. Gottdiener JS, Appelbaum FR, Ferrans VJ, Deisseroth A, Ziegler J.Cardiotoxicity associated with high dose cyclophosphamide therapy. Arch Intern Med. 1981;141(6):758-63 6. Darby SC, Ewertz M, McGale P, Bennet AM, Blom-Goldman, Bronnum D, et al. Risk of ischemic heart disease in women after radiotherapy for breast cancer. N Engl J Med. 2013;368(11):987-98. 3. Braverman AC, Antin JH, Plappert MT, Cook EF, Lee RT. Cyclophosphamide cardiotoxicity in bone marrow transplantation: a prospective evaluation of new dosing regimens. J Clin Oncol. 1991;9(7):1215-23. 4. Pai VB, Nahata MC. Cardiotoxicity of chemotherapeutic agents - incidence, treatment and prevention. Drug Saf. 2000;22(4):263-302. 7. Travis LB, Ng AK, Allan JM, Pui CH, Kennedy AR, Xu XG, et al. Second malignant neoplasms and cardiovascular disease following radiotherapy. J Natl Cancer Inst. 2012;104(5):357-70. 8. Marwick TH, Leano RL, Brown J, Sun JP, Hoffmann R, Lysyansky P, et al. Myocardial strain measurement with 2-dimensional speckle-tracking echocardiography: definition of normal range. JACC Cardiovasc Imaging. 2009;2(1):80-4. Arq Bras Cardiol. 2015; 105(2):206-207 207 Back to the Cover Erratum December issue of 2014, vol. 103 (6), pages. e73-e80 In the Original Article “Case 6/2014 – A Case of a 61-Year-old Woman with Diastolic Heart Failure”, pages e73-e80, by authors Fabio Grunspun Pitta, Natalia Quintella Sangiorgi Olivetti, Diego Simões Peniche, Andrea Maria Dercht, Paulo Sampaio Gutierrez, Luiz Alberto Benvenuti, please be aware that the correct spelling for to Andrea Maria Bercht is Andrea Maria Dercht. June 2015 Issue, vol. 104 (6), pages 433-442 In the original article “I Brazilian Registry of Heart Failure - Clinical Aspects, Care Quality and Hospitalization Outcomes”, published in the June 2015 of the Arquivos Brasileiros de Cardiologia [Arq Bras Cardiol. 2015; 104(6): 433-442], suffered the following correction: Correcting the text: In the analysis of the etiologies by region, patients from the South, Southeast and Northeast showed a predominance of the ischemic etiology (33.6%, 32.6%, and 31.9%, respectively). In patients in the Northern region the hypertensive etiology (37.2%) predominated, while among patients in the Northern region the Chagasic etiology predominated (42.4%) (Table 2). And considering the following text: In the analysis of the etiologies by region, patients from the South, Southeast and Northeast showed a predominance of the ischemic etiology (33.6%, 32.6%, and 31.9%, respectively). In patients in the Northern region the hypertensive etiology (37.2%) predominated, while among patients in the west-central region the Chagasic etiology predominated (42.4%) (Table 2). DOI: 10.5935/abc.20150103 208
Baixar