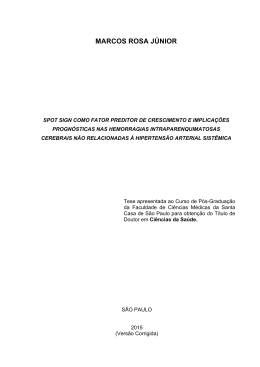
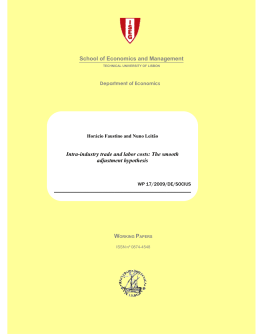
190 Relato de caso Spontaneous Subarachnoid Hemorrhage Induced by Warfarin Use - Case Report and Literature Review Hemorragia subaracnoidea espontânea induzida por Warfarina - Relato de Caso e Revisão da Literatura Ricardo Rezende Campos, MD1 Alexandre Martins Cunha, MD, MSc2 Marcelo Eduardo Sette dos Santos, MD1 Guilherme Brasileiro de Aguiar, MD1,2 RESUMO ABSTRACT Introdução: A causa mais frequente de hemorragia subaracnoidea (HSA) espontânea é a ruptura de aneurisma cerebral. Em aproximadamente 5% dos casos de HSA espontânea não se observam alterações à angiografia ou ressonância magnética do sistema nervoso central que explique o sangramento. O objetivo deste trabalho é apresentar um caso de HSA espontânea induzida por warfarina, onde não foi evidenciado nenhuma malformação vascular no sistema nervoso central. Relato de Caso: Paciente do sexo masculino, com 59 anos, apresentou quadro súbito de cefaléia durante o banho. O paciente tinha história de valvulopatia mitral com troca de vávula há 23 anos e hipertensão arterial sistêmica acompanhado por cardiologista, em uso de warfarina sódica ( 5mg diários ). A tomografia computadorizada de crânio demonstrou HSA Fisher III. Os exames laboratoriais mostraram uma razão normalizada internacional (RNI) de 2.2 (normal 1 a 1,2). Foram realizadas ressonância magnética do neuroeixo e angiografia cerebral que não demonstraram aneurisma ou qualquer outra malformação vascular. Conclusão: A ocorrência de hemorragia cerebral associada ao uso de warfarina é um evento bem documentado na literatura. Entretanto a ocorrência de HSA isolada nesses pacientes rara. Para atribuir a hemorragia subaracnoidea ao uso de warfarina é necessário excluir a presença de aneurisma ou outras malformações vasculares pelos exames de imagem. Introduction: The most frequent cause of spontaneous subarachnoid hemorrhage (SAH) is the rupture of a brain aneurysm. Approximately 5% of cases of spontaneous SAH did not show changes on magnetic resonance imaging (MRI) or angiography that explain such bleeding. The objective of this study was to report a case of spontaneous SAH induced by warfarin, where there was no evidence of any vascular malformation. Case Report: A 59 year-old male patient developed a sudden onset severe headache while in the shower. The patient had a history of mitral valve disease and valve replacement 23 years before and hypertension monitored by a cardiologist with 5 mg warfarin sodium daily. Computed tomography (CT) scan revealed a SAH. Laboratory tests showed an International Normalized Ratio (INR) of 2.22 (normal: 1 to 1.2). Cerebral angiography and neuraxis MRI were performed and showed no aneurysms or other vascular malformations.Conclusion: The occurrence of hemorrhage associated with warfarin treatment is a well-documented event in the literature. However, the isolated occurrence of SAH in these patients is a rare event. To prove that SAH is indeed attributed to anticoagulation, it is necessary to exclude the presence of aneurysms and other vascular diseases by imaging techniques. Palavras-chave: hemorragia subaracnoidea, hemorragia cerebral, warfarina, angiografia cerebral. Key words: cerebral hemorrhage, subarachnoid hemorrhage, warfarin, cerebral angiography. 1 - Division of Neurosurgery, Santa Marcelina de Itaquaquecetuba Hospital - São Paulo / SP / Brazil. 2 - Division of Neurosurgery, Department of Surgical Specialties, State University of Rio de Janeiro - Rio de Janeiro / RJ / Brazil. Recebido em 10 de julho de 2011, aceito em 16 de setembro de 2011 Campos RR, Cunha AM, Santos MES, Aguiar GB - Spontaneous Subarachnoid Hemorrhage Induced by Warfarin Use - Case Report and Literature Review J Bras Neurocirurg 22 (4): 190-193, 2011 191 Relato de caso Introduction A B C Spontaneous subarachnoid hemorrhage (SAH) accounts for approximately 5% of all strokes1. The estimated incidence varies from 8.1 to 23 cases per 100,000 inhabitants1,13, with high morbidity and mortality rates that can reach up to 45%1. In 85% of SAH cases, a ruptured cerebral aneurysm is evident on computed tomography (CT) scans1,13. Ruptured arteriovenous malformations, dural fistula or sinus thrombosis, among others, represent other causes of spontaneous SAH13. D E F Of patients with spontaneous SAH, 15% to 20% have no aneurysm detectable by cerebral angiography10,11. Rinkel et al.10 listed perimesencephalic idiopathic hemorrhage, cocaine use and coagulation disorders as possible causes of SAH in the absence of aneurysms and vascular malformations by imaging studies10. The objective of this article was to report a case of spontaneous SAH induced by warfarin, in which there was no evidence of an underlying vascular malformation. We also performed a brief review of the literature on this subject. Figure 1. Axial head CT without contrast: A,B,C: Fisher III subarachnoid hemorrhage filling the basal cisterns and sylvian fissures; D,E,F: no signs of intracranial hemorrhage. A B C D E F Case Report A 59-year-old male had a sudden onset of severe headache while he was in the shower. Neurological examination revealed that the patient was alert and lucid, without any focal neurological deficits, with a mild degree of neck stiffness (graded as a HuntHess I SAH). The patient had a mitral valve disease with a valve replacement 23 years previously and hypertension that was under follow-up by a cardiologist. The patient was under antihypertensive medication, and on 5 mg warfarin sodium daily. A CT scan demonstrated a SAH (Fisher III) (Fig. 1A, 1B, 1C). Laboratory tests showed an International Normalized Ratio (INR) of 2.22 (normal range: 1 - 1.2) and Prothrombin Time Activity (PTA) by 21.8” and 42% (normal ranges: 10.2 to 14.2” / 70-130%). The patient remained in the intensive care unit of our hospital as part of the initial standard treatment for SAH, in addition to the discontinuation of his treatment with warfarin. Cerebral angiography was performed (Fig. 2) and showed no vascular malformation. Neuraxis MRI was performed, with no alterations. With the discontinuation of warfarin, the patient’s coagulation function normalized after 6 days. The patient left the hospital after 14 days asymptomatic, and continued to attend cardiological and neurological follow-up appointments. The most recent CT scan prior to his discharge from hospital was normal (Fig. 1D,1E,1F). Figure 2. Cerebral angiography. Right carotid artery injection, frontal (A) and lateral (B) view. Left carotid artery injection frontal (C) and lateral (D) view; Left vertebral artery injection, frontal (E) and lateral (F) views. No evidence of vascular malformation. Campos RR, Cunha AM, Santos MES, Aguiar GB - Spontaneous Subarachnoid Hemorrhage Induced by Warfarin Use - Case Report and Literature Review J Bras Neurocirurg 22 (4): 190-193, 2011 192 Relato de caso Discussion factors, such as the level of consciousness of the patient on admission, volume of the hemorrhage and site of bleeding, as bleeding induced by use of such medications can range from asymptomatic microbleedings to massive bleeding3,9,12,14. The most common cause of SAH is trauma13. If only spontaneous SAH is considered, its main cause is rupture of an intracranial aneurysm1,13. Among the cases of spontaneous SAH, between 15 and 20% present with normal cerebral angiography10,11, which requires further investigation to diagnose other possible causes. Intraparenchymal hemorrhage associated with warfarin is an event that is well-documented in the literature. However, the occurrence of isolated SAH in these patients is a rare event. For SAHs in anticoagulated patients to indeed be attributed to anticoagulation, it is necessary that the presence of aneurysms and other intracranial vascular diseases are excluded by imaging techniques, such as cerebral angiography and MRI of the neuraxis. Once confirmed, any SAH induced by warfarin should be managed with normalization of the INR to decrease the risk of further rebleeding, and the imposition of a standard treatment protocol for SAH. Intraparenchymal hemorrhage in patients with coagulation disorders, either through primary causes or in the presence of anticoagulation therapy, is well-reported in the medical literature3,10,11,13,14. Oral anticoagulation is a cause of intracerebral hemorrhage3,14, and has been reported as the most serious complication with the long-term use of this therapy in patients4. The location of anticoagulation-induced intracranial hemorrhage occurs, in decreasing order of frequency, deep in the brain , in the cerebral lobes, cerebellum and brainstem3. Olsen et al.8 in a population study, showed that there is no increase in the risk of SAH associated with the use of oral anticoagulation8. SAH-induced anticoagulation alone is a rare event, with only a few reported cases5,3,7. Mattle et al.6 reported 76 cases of extracerebral intracranial bleeding associated with use of oral anticoagulation. Of these, seven had hemorrhage in the subarachnoid space, and only four had no history of trauma. Of the four patients with spontaneous SAH, two were diagnosed with a cerebral aneurysm and the other two were considered to have SAHs that were directly related to the use of vitamin K antagonists. There was no information on any additional investigation with cerebral angiography in these two patients, or elsewhere6. Zubrov et al.14 reported a retrospective study of patients presenting with intracranial hemorrhage in use of oral anticoagulants who were treated with drug withdrawal, the administration of antihypertensive drugs to maintain a mean arterial pressure below 130 mmHg, the correction of the INR with vitamin K associated with fresh frozen plasma infusion, besides the administration of recombinant factor VII for cases whose response to vitamin K and fresh frozen plasma were unsuccessful14. In contrast, Flaherty et al.3 reported during the same year that there was no consensus with regards to indications for the suspension or manteinance of oral anticoagulation in cases of intracranial hemorrhages3. Claassen et al.2 published a prospective study in 2008, which reported that there was no difference in relation to rebleeding in cases where anticoagulation was suspended completely or early resumed (between 2 weeks and 2 months post-SAH), or late (>2 months of bleeding)2. As regards to prognosis, the severity of hemorrhagic stroke in the presence of oral anticoagulation therapy depends on several Disclosure The authors have no conflict of interest involved. References 1. Bederson JB, Connolly Jr ES, Batjer HH, Dacey RG, Dion JE, Diringer MN, et al. Guidelines for the management of aneurysmal subarachnoid hemorrhage: a statement for healthcare professionals from a special writing group of the Stroke Council, American Heart Association. Stroke. 2009; 40(3): 994-1025. 2. Claassen DO, Kazemi N, Zubkov AY, Wijdicks EF, Rabinstein AA. Restarting anticoagulation therapy after warfarin-associated intracerebral hemorrhage. Arch Neurol. 2008; 65(10): 1313-8. 3. Flaherty ML, Tao H, Haverbusch M, Sekar P, Kleindorfer D, Kissela B, et al. Warfarin use leads to larger intracerebral hematomas. Neurology. 2008; 71(14): 1084-9. 4. Foerch C, Arai K, Jin G, Park KP, Pallast S, van Leyen K, et al. Experimental model of warfarin-associated intracerebral hemorrhage. Stroke. 2008; 39(12): 3397-404. 5. Mathiesen T, Benediktsdottir K, Johnsson H, Lindqvist M, von Holst H. Intracranial traumatic and non-traumatic haemorrhagic complications of warfarin treatment. Acta Neurol Scand. 1995; 91(3): 208-14. 6. Mattle H, Kohler S, Huber P, Rohner M, Steinsiepe KF. Anticoagulation-related intracranial extracerebral haemorrhage. J Neurol Neurosurg Psychiaty. 1989; 52:829-37. Campos RR, Cunha AM, Santos MES, Aguiar GB - Spontaneous Subarachnoid Hemorrhage Induced by Warfarin Use - Case Report and Literature Review J Bras Neurocirurg 22 (4): 190-193, 2011 193 Relato de caso 7. Nilsson OG, Lindgren A, Stahl N, Brandt L, Säveland H. Incidence of intracerebral and subarachnoid hemorrhage in southern Sweden. J Neurol Neurosurg Psychiatry. 2000; 69: 601-7. 8. Olsen M, Johansen MB, Christensen S, Sorensen HT. Use of vitamin K antagonists and risk of subarachnoid haemorrhage: a population-based case-control study. Eur J Intern Med. 2010; 21(4): 297-300. 9. Orken DN, Kenangil G, Uysal E, Forta H. Cerebral microbleeds in ischemic stroke patients on warfarin treatment. Stroke. 2009: 40(11): 3638-40. 10. Rinkel GJ, van Gijn J, Wijdicks EF. Subarachnoid hemorrhage without detectable aneurysm. A review of the causes. Stroke. 1993; 24(9): 1403-9. 11. Sarabia R, Lagares A, Fernández-Alén JA, Arikan F, Vilalta J, Ibáñez J, et al. Idiopathic subarachnoid hemorrhage: a multicentre series of 220 patients. Neurocirugia (Astur). 2010; 21(6): 441-51. 12. Ueno H, Naka H, Ohshita T, Kondo K, Nomura E, Ohtsuki T, et al. Association between cerebral microbleeds on T2*-weighted MR images and recurrent hemorrhagic stroke in patients treated with warfarin following ischemic stroke. Am J Neuroradiol. 2008; 29(8): 1483-6. 13. van Gijn J, Rinkel GJ. Subarachnoid haemorrhage: diagnosis, causes and management. Brain. 2001; 124(2): 249-78. 14. Zubkov AY, Mandrekar JN, Claassen DO, Manno EM, Wijdicks EF, Rabinstein AA. Predictors of outcome in warfarin-related intracerebral hemorrhage. Arch Neurol. 2008; 65(10): 1320-5. Corresponding Author Guilherme Brasileiro de Aguiar, MD Rua Abílio Soares, 121 – apto 84 – Paraíso São Paulo – SP. Brazil 04005-000 Email: [email protected] Campos RR, Cunha AM, Santos MES, Aguiar GB - Spontaneous Subarachnoid Hemorrhage Induced by Warfarin Use - Case Report and Literature Review J Bras Neurocirurg 22 (4): 190-193, 2011
Baixar