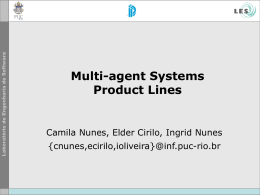
doi:10.3900/fpj.6.3.156.e EISSN 1676-5133 Cardiac frequency and blood pressure in different loads in the Cirilo´s ergometer step test in active women Original Article 1 Universidade Federal da Paraíba – UFPB, D.E.F., João Pessoa – PB – Brasil Laboratório de Cineantropometria (LABOCINE) UFPB-PB 3 Grupo de Pesquisa em Cineantropometria, Atividade Física e Saúde, Desenvolvimento e Desempenho Humano (GPCASD) / CNPq / UFPB 4 Laboratório de Atividades Físicas Professora Socorro Cirilo (LAAFISC), João Pessoa 5 Faculdade ASPER 6 Universidade Federal da Paraíba – UFPB, Departamento de Estatística, João Pessoa 7 UFPB, DEF, Bolsista PIBIC/CNPq/UFPB 8 Programa de Pós-graduação Stricto Sensu em Saúde da Criança e do Adolescente –Universidade Federal de Pernambuco (UFPE) – Recife – PE 9 Bolsista Capes/DS/UFPE Maria do Socorro Cirilo de Sousa1,2,3,4 [email protected] 2 Anderson Carlos Lourenço de Lima4,5 [email protected] João Agnaldo da Silva6 [email protected] Gigliola Cibele Cunha da Silva7 [email protected] Luciano Meireles de Pontes3,8,9 [email protected] Fábio Alexandre dos Santos Lira3 [email protected] Sousa MSC, Lima ACL, Silva JA, Silva GCC, Pontes LM, Lira FAS. Cardiac frequency and blood pressure in different loads in the Cirilo´s ergometer step test in active women. Fit Perf J. 2007;6(3):156-61. ABSTRACT: Introduction: HR and BP have been studied in the prediction of the physical performance. The objective of this work is to analyse the behavior of HR and BP in different loads in the step test Cirilo Protocol. Methodology: It is about an applied research, transversal, with 30 active women, according to norms of the ACSM, with age average 22.8+2.8 years, submitted to the anthropometrics tests, cardiorespiratory in Electronic Step Test Cirilo´s and hemodynamics. The statistical program SPSS 13.0 for average, deviation standard, minimum, maximum, correlation “r” of Pearson, “t” of Student, Qui-square of Friedman, level of significance of 5% was used. Results: The HR final defined the test as sub-maximum. The values in the load for 4 minutes: HRmax 179.40+6.58bfm, the SBP 132.00+13.04mmHg, the DBP 61.00+11.40mmHg. The SBP of the load for 3rdmin. 136.00+11.40mmHg and the DBP for the load 1stmin 62.00+4.47 mmHg was bigger. The Friedman´s test found p=0.05 for RT loads, SBP and DBP from the 1st to 4 th min. and the “t” of Student between the RT of 1st to 4 th min. (p=0.003). Conclusion: The behavior of the HR and the BP in different loads in step test under the Protocol of Cirilo of gradual form with daily intervals, in accordance with presents different the time of execution of the test indicating that it has alterations of the hemodynamics variables, and the HR increases in agreement the load linearly and SBP and DBP vary between 1st and 4th min. Keywords: human performance, blood hemodynamic, effort test. Correspondence to: Maria do Socorro Cirilo de Sousa - Rua Silvino Chaves, 1510 - Bairro Manaíra - CEP: 58038-040 - João Pessoa - PB - Brasil Submitted: November / 2006 Accepted: January / 2007 Copyright© 2008 Colégio Brasileiro de Atividade Física, Saúde e Esporte. 156 Fit Perf J Rio de Janeiro 6 3 156-161 May/Jun 2007 RESUMO RESUMEN Freqüência cardíaca e pressão arterial em diferentes cargas no ergômetro Banco de Cirilo em mulheres ativas Frecuencia cardiaca y presión arterial en diferentes cargas en el ergómetro banco de cirilo en mujeres activas Introdução: Freqüência Cardíaca (FC) e Pressão Arterial (PA) têm sido estudadas na predição do desempenho físico. O objetivo deste trabalho é analisar o comportamento da FC e PA em diferentes cargas, no teste de banco Protocolo Cirilo. Metodologia: Trata-se de pesquisa aplicada, transversal, com 30 mulheres ativas, segundo normas do ACSM, com média de idade 22,8 + 2,8 anos, submetidas aos testes antropométricos, cardiorrespiratório em Banco Eletrônico de Cirilo e hemodinâmicos. Utilizou-se programa estatístico SPSS 13.0 para cálculos de média, desvio padrão, mínimo, máximo, coeficiente de correlação “r” de Pearson, “t” de Student, Qui-quadrado de Friedman, com nível de significância de 5%. Resultados: A FC final definiu o teste como submáximo. Os valores na carga de 4 minutos: FCmáx 179,40+6,58 bpm; PAS, 132,00+13,04 mmHg; PAD, 61,00+11,40mmHg. A PA sistólica (PAS) da carga do 3ºmin, 136,00 + 11,40mmHg, e a PA diastólica (PAD) da carga de 1º min, 62,00 + 4,47 mmHg, foram maiores. O teste de Friedman teve p=0,05 para as cargas de FC, PAS e PAD do 1º ao 4º min e o “t” de Student entre a FC do 1º e 4º min. (p=0,003). Conclusões: O comportamento da FC e PA em diferentes cargas em teste de banco sob o Protocolo de Cirilo de forma progressiva com intervalos diários, apresentam-se diferentes de acordo com o tempo de execução do teste indicando que há alterações das variáveis hemodinâmicas, e a FC aumenta linearmente conforme a carga e a PAS e PAD variam entre o 1º e 4º min. Introducción: FC Y PA están siendo estudiadas en la predicción del desempeño físico. El objetivo de este trabajo es analizar el comportamiento de la FC y PA en diferentes cargas en el test de banco Protocolo Cirilo. Metodología: Se trata de investigación aplicada, transversal, con 30 mujeres activas, según normas del ACSM, con media de edad 22,8 + 2,8 años, sometidas a los tests antropométricos, cardiorrespiratorio en Banco Electrónico de Cirilo y hemodinámicos. Se utilizó programa estadístico SPSS 13.0 para media, desvío patrón, mínimo, máximo, coeficiente de correlación “r” de Pearson, “t” de Student, Jue-cuadrado de Friedman, nivel de acepción de 5%. Resultados: La FC final definió el test como submáximo. Los valores en la carga de 4 minutos: FCmáx 179,40+6,58 bpm, la PAS 132,00+13,04 mmHg la PAD 61,00+11,40 mmHg. Siendo que la PAS de la carga del 3º min. 136,00 + 11,40 mmHg y la PAD de la carga 1º min 62,00 + 4,47 mmHg fueron mayores. El test de Friedman encontró p=0,000 para las cargas de FC y PAS y PAD del 1º al 4º min. y el “t” de Student entre la FC del 1º y 4º min. (p=0,003). Conclusiones: El comportamiento de la FC y PA en diferentes cargas en test de banco bajo el Protocolo de Cirilo de forma progresiva con intervalos diarios, se presentan diferentes de acuerdo con el tiempo de ejecución del test indicando que hay alteraciones de las variables hemodinámicas, y la FC aumenta linealmente conforme la carga y la PAS y PAD varían entre el 1º y 4º min. Palavras-chave: Desempenho humano, hemodinâmica do sangue, Teste de esforço. Palabras clave: desempeño humano, hemodinámica de la sangre, test de esfuerzo. NTRODUCTION The hemodynamic variables and efficiency test in the step may be influenced by progressive stages of cargo during the climbs and descents. During the exercise, the musculature active receives a greater blood flow and heart receives more stimulation, compared with the state of rest. The most common physiological parameters for assessments about the health of the cardiorespiratory system during physical effort are the blood pressure (BP) and heart rate (HR). In tests with the use bench ergometer, there is a large participation of the musculature and joints of the lower limbs, realizing it is the involvement of different angles capable of causing changes in these variables during the response effort. Souza1 in studies with individuals untrained active and trained in tests of ascent and descent with bench ergometer, found values of HR effort in the range of 80-85% of HR maximum (FCM), featuring a sub-maximum test, which, probably, not elevates the BP at levels that pose damage to the system. It is known that one of the problems in the implementation of such tests is to estimate the BP due to the movement of climb and descent. Research in normotensive women and untrained in tests with loads continuous and progressive2,3, have found that levels of BP characterize hypertension reactive in tests of this nature. There is still that the first stage of step tests, with increments of continuous nature, shall begin with adequate time for any individual, even if it is considered low, which means minors in the knee joint angles involved in the effort. This causes comfort and accommodation in postural segments during the test. Tests using bench, despite being the oldest when it relates to ergometry, does not mean they are the least used. The remainder Fit Perf J, Rio de Janeiro, 6, 3, 157, May/Jun 2007 must be revised, restructured, as everything in science. They are the new techniques of application and development of instruments that compatibility with proposals for further evaluation in the field of tests. Research giving rise to new types of instruments and protocols were developed to expand the use of these ergometer1,3,4,5. It is known that in Brazil, as well as in the United States, these tests are widely available and used. Therefore, the proposal presented here is a new reading of tests in the area, specifically from the step where employ climbs and descents in cycles of four times, demarcated by metronomic or other form of cadence the rate. These may be able to quantify the exercises estimating the degree of physical ability, usually sub-maximum, which carry maximum prediction, usually through the index of volume of oxygen (VO2). Regarding the control of hemodynamic variables, where the BP and HR, bench ergometer in the form of manual verification may be impossible or impracticable, especially in the protocols of progressive and continuous load. Meanwhile, frequency meter and other resources as may be applicable to reduce the errors of estimate. As for the BP, the tests of bench usually last on average between three and six minutes, which may represent very little to increase the levels of pressure. Taking this variable to the end of the test, up to thirty seconds, can give us parameters of the values of BP achieved during the test. The security in the application of these tests is much greater in terms of time and effort into their characteristic sub-maximum. Studies show that, in thirty one thousand tests applied is not returned no 157 deaths when the use of climbs and descents of a step or bench by rate a demarcated1. So the question guiding this work is: is that the conduct of HR and the BP change in levels when test under different loads in trial of climb and descent of bench, using the Protocol of Bench Electronic of Cirilo. Therefore, the objective of this work is to analyse the behavior of HR and BP in different loads in the test of climb and descent of bench Cirilo Protocol. Figure 01: Bench Electronic Cirilo and processor of data MATERIALS AND METHODS Characterization of the study This study shows cross section with the completion of field testing and a predominantly quantitative approach. Population and sample The population of this study was composed of women practitioners of physical programme in the gym. The sample consisted of 30 active women, according to the standards of the American College of Sports Medicine8, average age 22.8 + 2.8 years, selected at random simple probabilistic method, practitioners of aerobic exercise, localized and weight training, systematically. The criteria for participation in the study were: be physically active at least six months; exercise is at least four times weekly; had not ingested alcoholic beverage; had not smoked; Tuesday slept eight hours, not being in the process of drug treatment, not be involved in infection, and normotensive be. Tools for collection of data and variables selected for the study Dependents: time of effort (s), height of ergometer (cm), BP (mmHg) at rest and post-effort, HR at rest and effort (bpm), volume of oxygen predicted a maximum (VO2max.), effort in climb and descent of steps, levels of subjective perception of effort (SPE) • Estadiometer portable, brand Sanny, precision 0.1 cm, height in cm; • Balance digital, brand Filizola, precision 100g, corporal mass in kg; • Bench Electronic Cirilo and processor of data: effort in climb and descent of steps to estimate the volume of oxygen (Figure 01); • Frequency Meter Heart, Polar brand, model S210, HR in beats for minute (bpm), in time effort, height the ergometer; • Sphygmomanometer the column of mercury, levels of SMP and DBP in mmHg; • Stethoscope BD, for heart auscultation, and • Panel with Table of Borg9, to levels of subjective perception of effort (SPE) Procedures for data collection Independent: age (years), height (cm), corporal mass (kg), heart auscultation; Only then was the test of climb and descent of bench ergometer, according to the protocol of Cirilo6,7. The test was to perform continuous climbs and descent in bench ergometer. The height of ergometer was continuous and progressive, with increments appropriate to the height of the individual, as shown in table 1. The test also was adjusted to the degree of physical measure Table 1: Number of periods of overload (heights) in cm. Source: Sousa (2001) height (cm) until 151.9 152.0 to 161.9 162.0 to 171.9 172.0 to 181.9 182.0 to 191.9 192.0 and above 158 1st stage (cm) 20 20 20 20 20 20 2nd stage (cm) 26 27 29 30 31 32.5 3rd stage (cm) 32 34 38 40 42 45 Initially the research was submitted to the Research Ethics Committee of the Centre for Health Sciences and approved under the registration number 118/01-B of 2005. The subjects of the sample signed an authorization for data collection, and the Statement of Consent for Research in Human Beings, as the Law 196/96 of the National Council of Saúde10. Then the anthropometric variables were measured for height and corporal mass, with the stadiometer and balance, respectively. Além disso, as hemodinâmicas, de FC, PA de repouso e controle subjetivo do esforço. Moreover, the hemodynamics, HR, BP rest and subjective control of the effort. Table 2: Number of taps for minute (tpm) corresponding to the degree of physical ability of untrained (DTR), active (ATC) and trained (TR), by gender. Source: Sousa (2001) gender female male DTR 116 tpm 120 tpm ATV 132 tpm 144 tpm TR 152 tpm 160 tpm Fit Perf J, Rio de Janeiro, 6, 3, 158, May/Jun 2007 Table 3: Time of application and implementation of increments of effort in untrained (DTR), active (ATC) and trained (TR). Source: Sousa (2001) classification of physical ability DTR ATV TR time running start (s) 0 a 50s 0 a 50s 0 a 50s time for action of the 1st increase (s) 10 10 10 Table 4: Classification of VO2max. in ml.kg-1.min-1 CLASSIFICATION Very Weak Weak Regular Good Very Good Excellent FEMALE less than 19.31 from 19.31 to 23.99 from 24.00 to 27.34 from 27.35 to 30.51 from 30.52 to 43.04 over 43.04 MALE less than 26.52 from 26.52 to 30.95 from 30.96 to 35.59 from 35.60 to 47.77 from 47.78 to 56.20 over 56.20 and gender, as shown in table 2. The rate used was 132 taps for minute, equivalent to 33 past / minute. The test consists of four minutes, composed of three stages, with two increases in the height of the bench, as shown in table 3. The same was divided into four stages for each day, with progressive effort. On 1st day was the effort of 1min, in 2nd of 2min, at 3rd of 3min and 4th day, 4 min. Estimate to HR and BP before the test, HR in the effort and BP post-effort (30s until after the test) by the technique of Koroktoff. Before the effort, took place heating with specific stretching and stationary march in the rate of metronomic. The angle of bending the knee ranged from 45º of the 90º, 1st to the 3rd stage. The VO2 predicted a maximum was obtained through conversion of values in the regression equation: VO2max = –93.402 - [0.0548 x (age)] - [x 0.152 (height)] - [0.0874 x (weight)] - [x 0.568 (gender)] + [x 0.05996 (time)] + [0.0118 x (HR end)] + [x 0.798 (bench height)] - [x 16.221 (degree of measure)] + [x 1.095 (nº in rings)] where: age in years; height in cm; weight, in kilograms, gender, female = 0 and male = 1; Time, total run time of the test; HR final, HR at the end of the test; bench height, height achieved in final bench; degree of proficiency: untrained = 1; active = 2 and trained = 3; number of rings: untrained female = 116; active female = 132; trained female = 152; male untrained = 120; active male = 144; trained male = 160. Plan analytical The analytical plan used the computerized package SPSS version 13.0 for descriptive statistics inferential average, standard deviation, minimum, maximum, correlation coefficient “r” of Pearson, “t” Student and Qui-square of Friedman. The level of significance was 5%. The calculation of VO2 to estimate the maximum was carried out as the equation proposed in this study, from the decline in Sousa1 and VO2 classified by the table 4. running time of 1st increase (min) 1 a 1min50 1 a 1min50 1 a 2min50 running time of 2nd increase (min) 2a3 2a4 3a6 Table 5: descriptive statistics of average, standard deviation, minimum and maximum of variables FCR, FCE1, FCE2, FCE3, FCE4, SBPR, SBPPE1, SBPPE2, SBPPE3, SBPPE4, DBPR, DBPPE1, DBPPE2, DBPPE3 and DBPPE4. (n=5) variables FCR FCE1 FCE2 FCE3 FCE4 SBPR SBPPE1 SBPPE2 SBPPE3 SBPPE4 DBPR DBPPE1 DBPPE2 DBPPE3 DBPPE4 Average and dp 82.80 ± 17.88 144.00 ± 9.95 163.20 ± 5.07 171.80 ± 8.29 179.40 ± 6.58 93.60 ± 10.29 115.00 ± 15.00 129.00 ± 15.97 136.00 ± 11.40 132.00 ± 13.04 59.40 ± 5.86 62.00 ± 4.47 59.00 ± 4.18 56.00 ± 4.18 61.00 ± 11.40 minimum 66 135 157 161 172 84 100 105 120 120 53 60 55 50 50 maximum 107 159 170 183 189 111 140 150 150 150 69 70 65 60 80 minutes (SBPPE1, SBPPE2, SBPPE3 and SBPPE4), DBP rest (DBPR) and the post-effort, in the 1st, 2nd, 3rd and 4th minute (DBPPE1, DBPPE2, DBPPE3 and DBPPE4), as prepared in table 5. When we examined the associations between the variables BP and HR, there was high correlation to DBPE1 and DBPE4 (1min and 4min of effort). Table 6 shows the values of “r” in the Pearson correlation and significance of these associations. Friedman’s test found significant differences for the BP and HR the 1st and 4th load (1min and 4min of effort) (p = 0.05) and between levels of the rest of the BP and HR and the effort (p = 0.05), as table 7. DISCUSSION The HR reached the end of the test, according to the mean age of the equation Karvonen of 220-age, did not achieve 85% of the HR estimated maximum, characterizing it as sub-maximum. The values found in charge of 4 minutes, were: HRmáx 179.40 + 6.58 bpm, SBP 132.00 + 13.04 mmHg and DBP 61.00 + 11.40mmHg. Since the SBP of the load 3rd of minutes was higher (136.00 + 11.40 mmHg) and DBP of the load of 1 minute also Table 6: Values of “r” in the Pearson correlation and significance (n = 30) * p <0.05 significant; ** p> 0.05 non-significant RESULTS Variables In this study, is considered the variables of HR rest (VCF), HR of effort in the 1st, 2nd, 3rd and 4th minute (HRE1, HRE2, HRE3 and HRE4), SBP rest (SBPR) and post-effort in the 1st , 2nd, 3rd and 4th FCE1& FCE4 SBPPE1& SBPPE4 DBPPE1& DBPPE4 Fit Perf J, Rio de Janeiro, 6, 3, 159, May/Jun 2007 time for action of the 2nd increase (s) 10 10 10 correlation “r” of Pearson 0.034 0.383 0.932 sigificance 0.956** 0.524** 0.021* 159 Table 7: statistical inference of the test “t” Student for the variables HR, SBP and DBP (n = 30) * p <0.05 significant; ** p> 0.05 non-significant variable FCE1& FCE4 SBPPE1& SBPPE4 DBPPE1& DBPPE4 significance 0.003* 0.072** 0.778** had higher (62.00 + 4.47 mmHg). It set up this cardiorespiratory the adjustments made between the 1st and 3rd minutes of test, causing a relaxation of arteries after this time in exercises submaximum4. The step test to increase provides more time for implementation of the effort, when it relates to mechanical efficiency and angulation of the lower limbs for climbs and descents, encouraging, therefore, better physiological responses, some research1,3,11 found that women in active the effort applied in different protocols for step test causes significant differences between the recovery of HR assessed. These studies explain that the tests of cargo single largest cause perception of effort, with less possibility of completing the test of time. But the test of continuous work and multiple loads and progressive, the rate of 132 taps for minute, decrease the levels of perceived effort and HR. Lim et al. 6 in an experiment with normotensive and hypertensive subject also suggested a protocol of bench ergometer in test of three minutes. According to the authors of the work, the step test showed good reproducibility and good correlation with the cycle-ergometer a load work equivalent (r = 0.930), and can be used in the relationship between physical activity and measures hemodynamic. In a study with women untrained in bench ergometer found values of HR end of 165 bpm for tests of 3 min rate with touches of 120 by minute12. And in this study, when it upped the intensity to 144 taps for minute, the HR also increased, indicating that even trained in women, increasing the intensity is associated with higher levels of hemodynamic variables in tests characterized as sub-maximum12. In research, analysing people trained, active and untrained of both genders found that it is possible to use the bench as ergometer indirect method of prediction of VO2máx by equation, when considering the appropriate height to height, age, HR, the corporal mass and height of bench3. It was observed that the consumption of oxygen appears on a minimum rate of 20 to 25 climbs and descents for minute. Other researchers have chosen to use the bench ergometer to study with a representative sample of men and women to estimate parameters of the function aerobics13. It is known that the practicality and feasibility of using this type of ergometer facilitates the completion of studies in cross section The rate of effort arises when the person performing the task in bench between 40 and 50 cm, a height which produces an angle of bending the knee articulation of 47-60º (thigh to the lower leg)13,14. It is emphasized that exceed the angle of 90º of the bending of the knee moving climb and descent, as well as to hinder the action biomechanics, exposes the individual to a higher risk of injury. Studies were based on tuning the height of the bench to better angulation of the knee in the movement to climb and descent, indicating that they ergometer must be adjusted to the 160 size of the individual corporal closer14,15,16. The biomechanical efficiency and work require compensation for the anatomical differences between the heights of individuals13. The levels of SBP in this study increased and DBP declined linearly with time of effort. In search similar pattern was found in individuals of both genders, in ergometry with rolling wake, that the magnitude of hypotension post-exercise is highly variable, but it is normal2. In another study with use of ergonometry cycle and rolling wake, noted the absence of DBP fall of post-exercise and only stabilization16. In search of verifying reductions BP, met up to 40 mmHg and oscillating decrease in SBP of 0-20 mmHg and DBP 2.5 to 12 mmHg in ergometer wake of rolling16,17. In studies examining the response of the BP and double product (DP) is test the physical sub-maximum in bench ergometer adjustable electronic Cirilo6,7, it was found that the BP response effort in post-hypertensive, in the routine step test ergometer, allow changes and reductions in the levels of DBP, control the levels of SBP and DP, suggesting that this type of dynamic and aerobic exercise is recommended for people hypertension8,18,19. In a study of coronary different ergometer, ergonometry cycle and a rolling wake of inferior limbs was possible to see that they had lower values for HRmax in both ergometer (p = 0.125), which probably is due to both the regular use of chronotropic negative action of medications, but also the presence of cardiovascular diseases, which tend to undermine the chronotropic response to exercise20. There are different protocols and procedures for conducting a test exercise (TE). However, there is always a real and practical difficulty in determining when an individual actually reached its maximum. Probably, for its ease of measurement, the HR has been one of the clinical variables most often employed to characterize the acquisition of a maximum effort in conventional TE (no measure of expired gases) from the comparison with ceilings set by age when it is then called HR maximum (FCM) 20. The study conducted here applies for populations of coronary, the ability sub-maximum recommended in its protocol, and allow a more peaceful for the implementation assessed. Research in order to derive equations for predicting the widespread maximum load for young men and women, under the direct method of ergo spirometry VO2max and to determine the maximum load (Wmax) in the ergonometry cycle, 30 men and 30 women (26 ± 5 years), found that in multiple linear adjustment, the maximum load was explained by age and corporal mass21. The equations proposals passed by the cross-validation, using another sample with similar characteristics of age and VO2max composed of 15 men and 15 women. The authors concluded that the generalized equations were valid for determining the maximum load in the ergonometry cycle for men and women. These surveys corroborate the study conducted here, in that generalized equations for predicting the VO2max were developed for the test of bench using the ergo spirometry1, indicating be as practical and effective as its implementation of programmes aimed quantification of exercise for degree of proficiency . However, there are signs that the statistical theory says that at least 50% of healthy individuals should achieve values equal to or higher than predicted by the regression equation, making this Fit Perf J, Rio de Janeiro, 6, 3, 160, May/Jun 2007 criterion rather limited and probably invalid in many of clinical situations everyday20. But the environment of the practice of Physical Education, specifically test, it is perfectly acceptable, provided that applied for purposes of verification of physical ability and nonclinical, based on diagnoses of cardiorespiratory disorders. If an individual is not able to climb a step up to 20cm, overcoming their own corporal weight, probably is with your motor functions and organic limited or depressed, demanding an intervention of a medical professional or a Physical Education. Scholars say that for a better clinical result, a TE should preferably be maximum, thus allowing for the greatest amount of relevant information21. However, the decision to use the test maximum effort or sub-maximum depends largely on the reasons for carrying out the test, the type of individual to be tested and availability of equipment and human resources appropriate. CONCLUSION The behavior of the HR and the BP, on different charges in trial of climb and descent of bench Protocol Cirilo, gradually, with intervals daily, present themselves in accordance with the different time of execution of the test. This indicates that there are changes in hemodynamic variables, and the HR increases linearly as the time of loading, and the SBP and DBP indicate variability of the 1st to the 4th minute. Tests in different ergometer are applied exacerbatingly, allowing the researchers and evaluators in general parameters for different variables, mainly hemodynamic and degrees of physical ability. This favors the application of new techniques on tools for easy access, portability, reproducibility and able to quantify the performance of programs for prescribing a more effective, such as the test bench, specifically the protocol of Cirilo, which is a new preparation of tests such natural. It is important to emphasize that equipment for tests in ergometry to be employed in the most diverse options and special features. However, the procedure must be controlled and the type of protocol applied, considering the scope and the final product. REFERENCES 3. Sousa MSC, Pellegrinotti IL. Teste de banco com carga contínua para análise do volume de oxigênio (VO2) predito e analisado por tempo de esforço em pessoas treinadas (TRD), ativas (ATV) e destreinadas (DTR) a partir dos 13 anos: proposta de validação. In: III Simpósio Internacional em Treinamento Desportivo; 2002 nov 13-17; Centro de Convenções do Espaço Cultura. João Pessoa; Idéia; 2002. p.184. 4. Powers SK, Howley ET. Fisiologia do exercício: teoria e aplicação ao condicionamento e ao desempenho. 3ª ed. São Paulo: Manole; 2000. 5. Lim P, Shiels P, Anderson J, MacDonald T. Dundee step test: a simple method of measuring the blood pressure response to exercise. J Hum Hypertens. 1999;13(8):521-526. 6. Fernandes Filho J. A prática da avaliação física. Rio de Janeiro: Shape; 1999. 7. Pitanga JG. Teste, medidas e avaliação em Educação Física e Esportes. São Paulo: Phorte; 2004. 8. American College of Sports Medicine. ACMS’s guidelines for exercise testing and prescription. 6ª ed. USA: Willians & Wilkins; 2000. 9. Borg G. Escala de Borg para a dor e o esforço percebido. 1ª ed. São Paulo: Manole; 2000. 10. Brasil, Ministério da Saúde. Conselho Nacional de Saúde. Manual operacional para comitês de ética em pesquisa. Brasília (DF): Ministério da Saúde; 2002. 11. Sousa MSC, Silva JMFL, Gomes ERM, Sousa SJG, Pinheiro SS, Ceriani RB, et al. Resposta da PA e duplo produto em teste físico submáximo no ergômetro banco regulável eletrônico de Cirilo (Sousa, 2001) em mulheres hipertensas e destreinadas. In: Anais XII Congresso Norte-riograndense de Cardiologia, III Simpósio de Nutrição em Cardiologia, III Jornada de Fisioterapia Cardiorrespiratório, VI Jornada de Enfermagem em Cardiologia e I Jornada de Atividade Física e Saúde; 2004 mai 27-29; Natal (RN). 12. Sousa MSC, Silva JMFL, Gomes ERM, Reis EES, Cirilo JB, Ceriani RB, et al. Resposta da freqüência cardíaca de recuperação em ergômetro banco eletrônico de Cirilo (Sousa, 2001), em mulheres normotensas destreinadas de diferentes faixas etárias. In: Anais do IX Congresso Paraibano de Cardiologia, III Simpósio de Nutrição em Cardiologia, III Simpósio de Psicologia em Cardiologia; 2004 ago 19-21; João Pessoa (PB). 13. Paterson DH, Cunningham DA, Koval JJ, St Croix CM. Aerobic fitness in a population of independently living men and women aged 55-86 years. Med Sci Sports Exerc. 1999;31(12):1813-1820. 14. Francis K, Brasher J. A height-adjusted step test for predicting maximal oxygen consumption in males. J Sports Med Phys Fitness. 1992;32(3):282-287. 15. Francis K, Culpepper M. Validation of a three minute hight-adjusted step test. J Sports Med Phys Fitness. 1988;2(3):229-233. 16. Shapiro A, Shapiro Y, Magazanik A. A simple step test to predict aerobic capacity. J Sports Med Phys Fitness. 1976;16:209-213. 17. Cléroux J, Kouamé N, Nadeau A, Coulombe D, Lacourcière Y. After effects of exercise on regional and systemic hemodynamics in hypertension. Hypertension. 1992;19:183191. 18. Wilcox RG, Bennett T, Brown AM, McDonald IA. Reductions up to 40 mmHg and rocking decrease of the blood pressure. Br Med J. 1982;285:767-769. 19. Sousa MSC, Pellegrinotti IL. Respostas metabólicas pela ergoespirometria em teste de banco com incremento em homens destreinados faixa etária ate 69 anos: proposta de equação de regressão na estimativa de volume máximo de oxigênio (VO2máx). In: Anais do II Simpósio Internacional em Treinamento Desportivo; 2000 nov 16-19; Centro de Convenções do Espaço Cultural. João Pessoa: Universitária; 2000. p. 70. 1. Sousa MSC. Teste de banco pra avaliação da potência aeróbia em pessoas destreinadas (DTR), ativas (ATV) e treinadas (TRD) a partir de 13 anos de ambos os sexos: proposta de validação. Campinas (SP): Universitária; 2001. 20. Araújo CGS, Pinto VLM. Freqüência cardíaca máxima em testes de exercício em esteira rolante e em cicloergômetro de membros inferiores. Arq bras cardiol. 2005 jul;85(1):45-50. 2. Rebelo FPV, Beneti M, Lemos LS, Carvalho T. Magnitude da hipotensão pós-exercício. Rev bras ativ fís saúde. 2001;6(2):28-38. 21. Nogueira FS, Pompeu FAMS. Modelos para predição da carga máxima no teste clínico de esforço cardiopulmonar. Arq bras cardiol. 2006 ago;87(2):137-145. Fit Perf J, Rio de Janeiro, 6, 3, 161, May/Jun 2007 161
Baixar