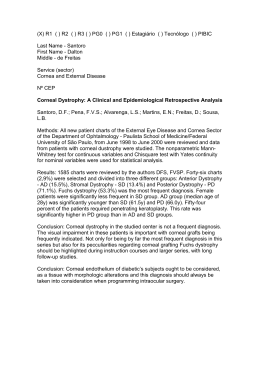
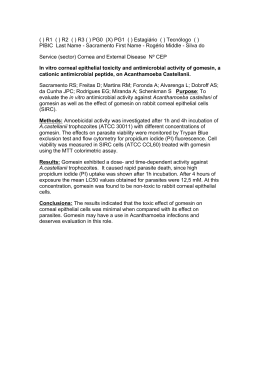
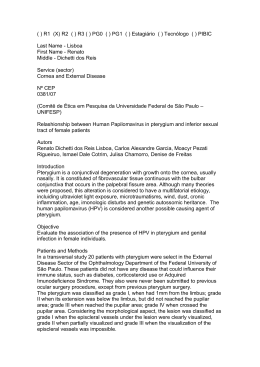
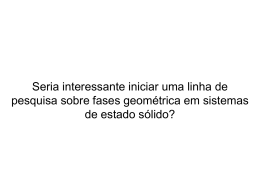
Surgical Device for Supporting Corneal Transplants Liliane Venturaa, Jean-Jacques De Grootea, Sidney J.F. Sousab Dept. of Elect. Engineering USP, Av. Trabalhador Saocarlense 400, S. Carlos, SP Brasil 13566-590 b Dept. of Opthalmology USP, Av. Bandeirantes 3900, Rib. Preto, SP Brasil 14100-900 [email protected] Abstract A system for supporting corneal suture for minimizing induced astigmatism, due to irregular manual stitches, has been designed. The system projects 48 light spots, from LEDs, displayed in a precise circle at the lachrymal film of the examined cornea. The displacement, the size and deformation of the reflected image of these light spots analysis providies the keratometry and the circularity of the suture. Measurements in the range of 32D – 55D and a self-calibration system has been designed in order to keep the system calibrated. The system has been tested in 13 persons in order to evaluate its clinical applicability and has been compared to a commercial keratometer Topcon OM-4. The correlation factors are 0.92 for the astigmatism and 0.99 for the associated axis. The system indicates that the surgeon should achieve circularity ≥98% in order to do not induce astigmatisms over 3D. 1. Introduction For many years, optometrists, ophthalmologists and researchers of the ocular area have used equipments to study the eye. Some of these equipments have been in use simply to observe parts of the eye, subjectively, such as: magnifying glasses, Slit Lamps and bio-microscopes. Other instruments referred to as keratometers or ophthalmology meters have been used to measure the radii of corneal curvature along the two main meridians of the eye. The physics principle of such instruments is already well known [1]. Currently, keratometers already have technological advancements that allow the measuring of corneal curvature radii, therefore measuring the corneal astigmatism, and some are equipped with rings projection covering the entire surface, showing the topography of the cornea. One of the significant factors that induces corneal astigmatism during the surgical procedure is the irregularity in suturing the tissue. Sutures are manually performed on the cornea and systems for monitoring the circularity of the suturing [2,3,4,5], are not often used. Most of them are just qualitative. The intention of the present work is to provide a system that allows automated keratometry as well as an objective real-time orientation for the surgeon for suturing the corneal tissue as most circular as possible, expecting to reduce the residual corneal astigmatism post- surgery. A brief description of the optical properties of the human cornea that concerns this work will be made as well as the calculus involved for determining the radii of curvature of the cornea will be described. 1.1 Optical Properties of the Human Cornea. The cornea has a curved surface with refractive index of 1.376 and thickness of 0.480mm [1,6,7]. The external curvature radius is approximately 7.8mm (it varies from 7.008.00mm for emmetrope eye) and the internal radius of curvature varies from 6.2-6.8mm. Hence, the cornea is equivalent to a positive lens. However it is very thin and for calculus regarding the central part of the cornea, it is possible to consider this region of the cornea as having parallel faces [7,8]. The light rays that strike the cornea refract mainly because of the relative difference of refractive index between the air and the corneal surface, rather than because of its corresponding refraction power (42.95D). The cornea is not perfectly spherical, actually it is ellipsoidal, and just the central part of the cornea, the so called central optical zone of approximately 4,0mm, may be considered spherical. The central zone is exactly where keratometry is obtained. The power of refraction of the small central portion of that region varies from 41-45D. In unusual conditions this region may be flattened down to 37D or may be curved up to 60D. Precisely, it its well known that the so called regular zone is not always spherical, actually it is toric, therefore the vertical and horizontal axes have different values. 1.2 Calculus for obtaining the radii of curvature of the cornea using a fixed dimension mire target. The human cornea has specific mechanical properties, which defines its stability and which are correlated to the stroma structure, having connections among its layers and thickness. Hence the cornea may assume different shapes, being difficult to predict a theoretical model for it. Any proposed model will present negative and positive aspects. So, the choice of which model to be used is the one that is best suitable for the present system. The cornea may be considered as a convex mirror, which provides a virtual image of the projected light source structure. As earlier mentioned, the cornea assumes a spherical shape in the central optical zone. These features are relevant for considerations of the model to be used. The spherical model is a very good approximation for the mentioned zone, but due to the flattening of the cornea toward the peripheral zone, we may obtain a small discrepancy for the keratometric results in this zone when compared to the actual keratometry measurements obtained from the corneal topographers, for instance. However, for a more criterious and accurate study of the periphery of the cornea, the elliptical model is applied. In this model, the cornea is treated as an ellipsoid, and therefore the results of the keratometry obtained for the cornea are more realistic. The results presented by the elliptical model differ from the ones obtained by the spherical model, especially at the periphery of the cornea. For keratometry purposes it can be said that, since just the central optical zone will be analyzed, the spherical model, which is much simpler to be implemented than the elliptical model, is sufficient and accurate, but for small radii of curvature, no approximations should be made, as we have learned from the development and tests of our first keratometry system for slit lamps [9]. 1.3 Spherical Model Without Approximations. The central zone of the cornea where the circular light mire is projected (3mm in diameter) is spherical and therefore the cornea may be considered as a convex mirror. Figure 1 shows a schematic diagram of the keratometric principle. An object of size h (radius of the circular target mire) is positioned at a distance a from the cornea, where it is perfectly focused onto the cornea. The reflection of object h provides a virtual image y, which is half of the dimension of the projected target on the cornea (around 1.5mm) and is at a distance b from the corneal surface. Distance d is 200mm for the surgical ocular microscope that we have used. Dimension b is the distance between the corneal surface and the actual position of the virtual image of the object (projected target). Figure 1: Schematic diagram of the keratometric principle [9]. Considering that the light rays coming from h reach the optical axis at small angles, it is possible to say that the focusing distance is one half of the curvature radius of the cornea (R). Observing triangles HOV and VIM and since d =a+b (1) The radius of curvature of the surface to be determined is: r= 2d h y h2 − y2 (2) The keratometric results are usually presented in “Refraction Power” (F), given by expression (5) and the unit is expressed in diopters (D). F= nc − 1 r (3) nc (1.3375) is the corneal refractive index . This paraxial equation (3) provides the refractive power of the corneal surface for incident rays that are approximately normal to the cornea and it is validated just for the central optical zone. 2. The developed module The system consists of a projected light ring onto the cornea in such manner that any distortion of the reflected image is analyzed for keratometric measurements. The keratometry system can be divided in two distinct portions: the projection system and the image capturing system. The projection system consists in projecting onto the patient’s cornea a mire with 36 red LEDS displayed in a perfect circle, which is to be held by the surgeon as shown in figure 2. The mire has 5 extra LEDS (one for center alignment of the system and 4 others for angular alignment). The mire has a special design that projects the light spots homogeneously and in a precise circle of 3mm of diameter in a standard cornea, i.e., with radius of curvature of 7.895mm (a stainless steal sphere with precision of 0.0025mm for its radius of curvature has been used as a standard cornea for calibrating the system, as shown in figure 3a). Figure 3b shows the target’s mire projected onto a patient’s cornea. Figure 3: Target’s mire projected onto: (a) a stainless steal sphere; (b) the patient’s cornea during surgery. Figure 4: Devices for assisting regular corneal suturing. The digitized image is processed by dedicated software for the system. The software is based on the information provided by the structure of the projecting target, determining its distortion as its image is reflected back from the cornea. The distortions analyzed between the original shape of the projected target and its reflected image contains information to provide the keratometric data. Figure 2: The projection system: Mire with 36 LEDS displayed in a perfect circle to be used during a corneal suture. The image of the target projected onto the patient’s cornea is reflected back to the microscope and passes through the observation system. A beam-splitter is placed between the magnification system and the eyepiece lenses of the slit lamp, where 70% of the reflected light is deviated to the eyepiece lenses. A regular video optical adapter for slit lamps (lenses, pin-holes and prisms) is coupled to the beam-splitter and a CCD camera WATEC 221S is attached to it. The reflected image is analyzed by the software at a micro computer OQO – model 2 coupled to the CCD camera via a video bus cable, as show in figure 4. Unlikely the usual keratometers, the keratometric module for the ocular microscope is not usually operated in an environment free from external disturbances, as light, for example. Hence, the developed algorithm is capable to avoid these kinds of interferences in the image processing. The image provided by the system is initially described in a matrix Im[x,y], which gives the position of the image in pixels and its brightness value in grayscale, hence 0 ≤ Im[ x, y ] ≤ 255 (4) The result of the non-uniformity of the brightness distribution in the image of the light spots that reach the examined surface is loss of information in the identification process of the target’s shape. The developed algorithm considers this possibility, once it provides the keratometric results even if some light spot is missing in the identification process. The image to be processed is composed by the 36 spots of light displayed in a highly accurate circular form, where the size of the target mire as well as the focusing distance is accurately known. The reflected image captured by the optical system will carry the distortions of the examined surface, the cornea. As the intensities of the light spots are not homogeneously distributed, a convolution process is used having a circular mask with a radius of the size of the average radius obtained by the light spots. As the center of the mask has a well defined position it identifies its center and stores its position as Px[1], Py[1]. Proceeding similarly, structures with lower intensities are identified. When all the Ne structures have been identified, as well as the position of their center of mass (Px[i],Py), (xcm0, ycm0) may be determined, which defines the position of the center of mass of the image by: xcm0 = ∑Px[i] / Ne e ycm0 = ∑Py[i] / Ne (5) The mathematical fitting expression for representing the reflected image of the target onto the cornea is an ellipse, with an inclination angle of θ related to the x axis of the coordinate system, as represented in figure 5. The coordinate system is X,Y and a and b are the minor and major axis of the ellipse, respectively. It should be noted that for the ellipse 0<e<1, therefore circularity varies from 0% - 100%. A real time image is displayed at the OQO monitor with orientations for adjusting the target mire axis and center. Figure 6 presents the interface screen. There is a center guide denoted by 1 (small circle at the center of the image screen), as well as an angular guide, denoted by 2 (two rectangles orthogonally placed in the center of the image capturing screen). Region denoted by 3 is where the 36 reflected spots should be. There is a calibration button for calibrating the system. The calibration of the system should be performed every time its optical components are removed and then replaced back in the microscope. It consists in placing a standard stainless sphere with radius of curvature of 7,895mm± 0,0025mm, in the fixed focusing position provided by every slit lamp; set the microscope to a desired magnification and capturing its reflected image from the 36 light spots. Keratometry and circularity (eccentricity) are presented every time that the image is capture (either by the mouse, voice command, or stepping pedal). Figure 5: Representation of the ellipse used in the software’s algorithm. The eccentricity is a function added to the software to acquaint the surgeon with the circularity of the suturing, indicating whether the surgeon should stiffen the stitch or relax it. The eccentricity, denoted e, is a parameter associated with every conic section. It can be thought of as a measure of how much the conic section deviates from being circular. [10]: (6) For any ellipse, let a be the length of its semi-major axis, b be the length of its semiminor axis and K=1. Therefore, the circularity has been defined in our software as C = 100 (1 – e)% (7) Figure 6: Screen presented for the surgeon during suturing. Figure 7 presents a measurement performed in a patient during suturing. A 98% of eccentricity has been achieved by the surgeon, however, it shows that almost 1D of astigmatism remains for this circularity. correlation between our system and the Topcon OM-4 is r2=0.97 for the axis. 4. Discussions and Conclusion Regarding figure 7, it may be noticed that high postoperatory astigmatisms are usually induced by the irregular manual suturing of the tissue. Even a high eccentricity (98% of circularity) achieved during the suture indicates that an astigmatism of the order of 1D still remains. Figure 7: Real time surgery measurement of keratometry and eccentricity of a cataract surgery. 3. Results In order to know the accuracy of our system, 21 standard steal spheres have been analyzed. Figure 8 shows the correlation curve between our system and the data provided by the manufacturer of the standard spheres, in a range of 3.0000mm – 17.0000mm ±0.0025mm. Spheres with radius of curvature of 7.8mm, which are the best representative for the corneal model, is 90% reproducible. Around 290 patients have been tested and it has been observed that circularity is corneal geometrical structure dependent. For instance, in order to remain astigmatisms lesser then 3D, for patients with corneas having radii of curvature around 7.8mm, a 97% of eccentricity should be achieved; for flatter corneas (refractive power of 38D) and more warped corneas (refractive power of 55D), eccentricities of 95% and 99%, respectively should be accomplished. This may lead to an awareness that manual suture should be carefully performed in order to obtain better post-operatory results related to remaining astigmatism. Maybe automated systems for suturing should be considered in the near future. 5. Acknowledgements The authors would like to thank CNPq (477226/2003-5) for all the financial support for this research and for some of the researchers, and Hospital das Clínicas de Ribeirão Preto (São Paulo – BRASIL), which is the Hospital that has always been contributing for the success of our researches. 6. References Figure 8: Correlation curve between our system and the data provided by the manufacturer of the standard spheres, in a range of 3,0mm – 17,0mm. Patients have been submitted to our system and the obtained results have high correlation factors (r2=0.96) with the keratometers available on the market (Topcon OM-4). In order to know the accuracy of the axis component of our system a device for distorting a contact lens coupled to a precise angular ruler was developed. It consisted of a vertical wedge, where the lens was placed and slightly pushed to be vertically deformed. Three different deformations were performed and they were precisely rotated at steps of 10 for the 3600. The 1. G. Smith and D.A. Atchison, The eye and Visual Optical Instruments, Cambridge University Press, p.175, 1941. 2. Ballin, N.; Flieringa ring - the poor man's operating keratometer. Ophthalmic. Surg., v. 12, p.443-4, 1981. 3. Igarashi, H.; Akiba, J.; Hirokawa, H. ; Yoshida, A. Measurement of the radius of corneal curvature with the Maloney surgical keratometer. Am. J. Ophthalmol., v. 112, p.211-2, 1991. 4. Troutman, R. C.; RUSSA, J. A. L. ; Surgical Microsystems, Inc. Indicating an asphericity of the cornea of an eye - US 4046463. Sept. 6, 1977. 5. Troutman, R.; Surgical keratometer in the management of astigmatism in keratoplasty. Ann. Ophthalmol., v. 19, p.473-4, 1987. 6. D.J. Spalton, R.A. Hitchings and P.A. Hunter, “The Cornea”, in Ophthalmology, Merck Sharp & Dohme International, 1987. 7. B. Jue and D.M. Maurice, “The Mechanical Properties of the Rabbit and Human Cornea”, J. Biomechanics, vol. 19, n. 10, pp. 847-853, 1986. 8. M.J. Hogan, J.A. Alvarado, E. Weddell, Histology of the Human Eye, Philadelphia, WB Saunders, 1971. 9. Ventura, L.; Riul, C.; Sousa, S.J.F.;De Groote, J.G.S.; Rosa, A.B.; Oliveira, G.C.D.; Corneal astigmatism measuring module for slit lamps – Phys. Med. Biol. 51 p. 1–14 (2006). 10. Steinbruch, A.; Winterle, P.; Geometria Analítica -2.ª edição – São Paulo, McGraw-Hill, 1987.
Baixar