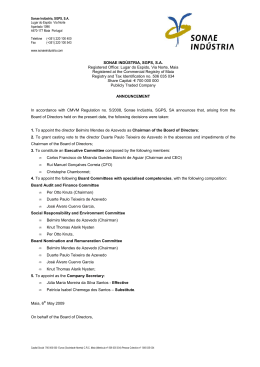
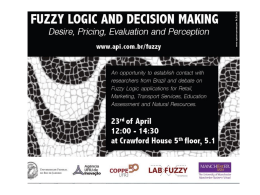
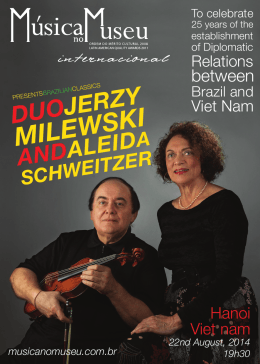
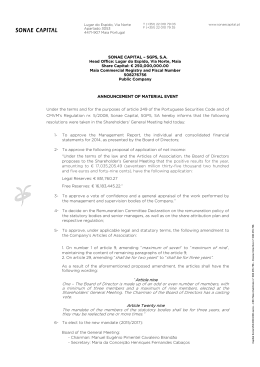
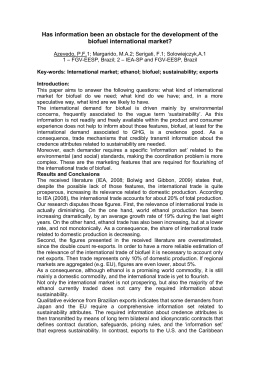
JOURNAL OF LAPAROENDOSCOPIC & ADVANCED SURGICAL TECHNIQUES Volume &, Number &, 2009 ª Mary Ann Liebert, Inc. DOI: 10.1089=lap.2009.0080 Full Report Intraperitoneal Pressure and Volume of Gas Injected as Effective Parameters of the Correct Position of the Veress Needle During Creation of Pneumoperitoneum João L.M.C. Azevedo, MD, PhD,1 Otavio C. Azevedo, MD, PhD,1 Albino A. Sorbello, MD, PhD,2 Otavio M. Becker, MD, PhD,1 Otavio Hypolito, MD, PhD,1 Dalmer Freire, MD, PhD,1 Susana Miyahira, MD,1 Afonso Guedes, Master, MD,1 and Glicia C. Azevedo , MD1 Abstract Objective: The aim of this work was to establish reliable parameters of the correct position of the Veress needle in the peritoneal cavity during creation of pneumoperitoneum. Methods: The Veress needle was inserted into the peritoneal cavity of 100 selected patients, and a carbon-dioxide flow rate of 1.2 L=min and a maximum pressure of 12 mm Hg were established. Intraperitoneal pressure (IP) and the volume of gas injected (VG) were recorded at the beginning of insufflation and at every 20 seconds. Correlations were established for pressure and volume in function of time. Values of IP and VG were predicted at 1, 2, 3, and 4 minutes of insufflation, by applying the following formulas: IP ¼ 2.3083 þ 0.0266time þ 8.310ÿ5time2 ÿ 2.4410ÿ7time3; and VG ¼ 0.813 þ 0.0157time. Results: A strong correlation was observed between IP and preestablished time points during creation of the pneumoperitoneum, as well as between VG and preestablished time points during creation of the pneumoperitoneum, with a coefficient of determination of 0.8011 for IP and of 0.9604 for VG. The predicted values were as follows: 1 minute ¼ 4.15; 2 minutes ¼ 6.27; 3 minutes ¼ 8.36; and 4 minutes ¼ 10.10 for IP (mm Hg); and 1 minute ¼ 1.12; 2 minutes ¼ 2.07; 3 minutes ¼ 3.01; and 4 minutes ¼ 3.95 for VG (L). Conclusions: Values of IP and VG at given time points during insufflation for creation of the pneumoperitoneum, using the Veress needle, can be effective parameters to determine whether the needle is correctly positioned in the peritoneal cavity. Introduction pressure level of over 20 mmHg. The position of the needle was changed until normal pressure was reached. Approximately 2.5 liters of carbonic gas were insufflated into the patient’s abdomen for five minutes. The patient’s abdominal wall was lifted and the first trocar was inserted. Vital signs were normal at that moment. Four minutes later, the patient was placed in the Trendelenburg position for the surgical procedure. Vital signs were checked and the systolic pressure could not be detected. No bleeding was observed upon inspection of the abdominal cavity, and resuscitation measures were carried out after removal of the laparoscope. After several minutes, a needle was inserted into the patient’s abdomen to check for bleeding. No blood was aspirated. The hypothesis of an anaphylactic reaction in response to the drug used was considered. In spite of the resuscitation measures, the patient I njury to the great vessels is the main cause of death during laparoscopic procedures.1 Various reports of injury to the great vessels caused by the Veress needle are found in the literature.2 These cases illustrate the difficulty in correctly diagnosing this complication, which is mainly due to the retroperitoneal position of the vessels.3–11 The following report by Peterson et al.12 is a good example to illustrate this situation: A 38-year-old female was hospitalized to undergo laparoscopic tubal esterilization. The patient was submitted to general anesthesia and placed supine. The abdominal wall was lifted using surgical forceps. A small infraumbilical incision was made for the introduction of the Veress needle. Immediately after needle insertion, the insufflator indicated a 1 Department of Surgery, Federal University of São Paulo, São Paulo, Brazil. Department of Surgical Gastroenterology, Hospital do Servidor Publico Estadual, São Paulo, Brazil. 2 1 2 AZEVEDO ET AL. died after two hours. Autopsy revealed a peritoneal cavity filled with blood and extensive hemorrhage. A 3-mm injury to the anterior and posterior walls of the abdominal aorta was observed, just before its ramification. The Veress needle is typically inserted through the abdominal midline, at the umbilicus. Albeit effective, insertion of the Veress needle through the midline poses danger. All injuries to the great vessels caused by the Veress needle reported in the literature resulted from midline punctures in the umbilical region.2 On the other hand, insertion of the Veress needle into the left hypochondrium has been reported as safe and effective,13 and potential injuries are less severe. Nevertheless, it is essential that the position of the needle after insertion be determined as accurately as possible. Needle-positioning tests prior to insufflation have been evaluated and considered adequate to guide surgeons with regard to the correct positioning of the Veress needle for creation of the pneumoperitoneum.14 These tests can avoid not only iatrogenic injury, but also gas insufflation into the wrong site, because surgeons intuitively know that intraperitoneal pressure (IP) and the volume of gas injected (VG) into the peritoneal cavity are predictable at certain time points during insufflation. In addition, high-pressure values and low carbon-dioxide (CO2) volume in the beginning of insufflation suggest incorrect positioning of the needle or lack of muscular paralysis, whereas low-pressure values and increased CO2 volume over a long insufflation period suggest injury to hollow viscera or gas leakage. Pressure and volume values can, therefore, be correlated with the position of the Veress needle in the abdominal cavity. Studies must be carried out in order to establish reliable, objective parameters to determine the position of the needle in the peritoneal cavity during creation of the pneumoperitoneum. Such studies might serve as guidelines for laparoscopic surgeons. No research has yet been carried out in humans, only in pigs.15 The aim of the present study was to determine reliable predictive values for Table 1. Descriptive Statistics of the Demographic Data from Patients of the Sample Parameters Age (years) mean (SD) Minimum=maximum Sex (n; %) Female Male BMI (kg=m2) Mean (SD) Minimum=maximum Height (m) Mean (SD) Minimum=maximum Weight (kg) Mean (SD) Minimum=maximum Intervention (n; %) Cholecystectomy Fundocardioplasty Bilat ing herniorrhaphy Unilat ing herniorrhaphy FIG. 1. Schematic illustration showing Veress needle puncture in the left hypochondriac region, at the costal margin, 8 cm from the midline. Note the entry point of the needle and the distance from the great vessels. IP and VG at given time points during creation of the pneumoperitoneum when using a Veress needle. Materials and Methods This study was approved by the Research Ethics Committees of the Health Care Institute of the São Paulo Hospital for State Civil Servants (protocol no. 045=03), and of the Federal University of São Paulo, (under research protocol no. 1405=03). Table 1 shows the demographic data. A total of 100 patients were included in the present study. Such patients had been scheduled to undergo laparoscopic procedures at the Surgical Gastroenterology Service of São Paulo Hospital for State Civil Servants. All patients were older than 18 years of age and nonobese [body-mass index (BMI) lower than 30 kg=m2), with no history of peritonitis or abdominal surgery. A dose of 0.1 mg=kg of midazolam was administered to patients 30 minutes before anesthesia. Anesthesia was induced with doses of 2 mg=kg of propofol and of 0.5 mcg=kg (n ¼ 100) 53.7 (13.1) 27–77 58 42 25.4 (2.4) 20.6–29.7 1.64 (0.09) 1.45–1.87 68.7 (9.8) 49.5–90.00 80 9 3 8 n, number of patients; SD, standard deviation; %, percentage; BMI, body-mass index; bilat, bilateral; unilat, unilateral; ing, inguinal. FIG. 2. Degree of dispersion of pressure in function of time and respective regression curve. The regression model above was statistically significant (P < 0.001), with a coefficient of determination of 80.1% (R2 ¼ 0.8011), indicating good adjustment. PARAMETERS OF THE POSITION OF THE VERESS NEEDLE 3 Results FIG. 3. Degree of dispersion of volume in function of time and respective regression line. The regression model above was statistically significant (P < 0.001), with a coefficient of determination of 96.04% (R2 ¼ 0.9604), indicating very good adjustment. A strong positive correlation between pressure and given time points was observed during creation of the pneumoperitoneum (Fig. 2). The curve shows good adjustment, with a coefficient of determination of 0.80 (pressure ¼ ÿ2E ÿ07time3 þ 8E ÿ 05time2 þ 0.0266time þ 2.3083). A strong positive correlation between volume and given time points was observed during creation of the pneumoperitoneum (Fig. 3). The curve shows good adjustment, with a coefficient of determination of 0.96 (volume ¼ 0.0157time þ 0.1813). Prediction of IP and VG (Table 2) yielded the following results: 1 minute ¼ 4.15; 2 minutes ¼ 6.27; 3 minutes ¼ 8.36; and 4 minutes ¼ 10.10 for pressure (mm Hg); and 1 minute ¼ 1.12; 2 minutes ¼ 2.07; 3 minutes ¼ 3.01; and 4 minutes ¼ 3.95 for volume (L). Mean and standard deviation of measured values were: 1 minute ¼ 4.34 1.48; 2 minutes ¼ 6.05 1.44; 3 minutes ¼ 8.44 1.47; and 4 minutes ¼ 10.43 1.48 for IP (mm Hg); and 1 minute ¼ 1.11 0.14; 2 minutes ¼ 2.18 0.21; 3 minutes ¼ 3.13 0.27; and 4 minutes ¼ 3.87 0.40 for VG (L). Discussion of fentanyl. For curarization, a dose of 0.5 mg=kg of atracurium was used. Patients were submitted to general anesthesia with orotracheal intubation and controlled mechanical ventilation. An orogastric tube was then inserted for aspiration of the stomach contents. After inserting a Veress needle through the left hypochondrium (Fig. 1), the following tests were performed to determine whether the needle was in the peritoneal cavity11: the aspiration test, the injection test, the recovery test, the saline drop test, and the initial IP test.14 When all tests were positive, insufflation continued. Variations in IP and VG were recorded at every 20 seconds, until IP reached 12 mm Hg (maximum IP). The total amount of time required for insufflation was also recorded. The data collected were submitted to statistical analysis. Qualitative variables were expressed as absolute and relative frequencies. Quantitative variables were expressed as mean, standard deviation, and minimum and maximum values. The correlation coefficients between pressure and time and volume and time were tested, and polynomial regression models were constructed to estimate volume and pressure in function of time.12 The accuracy of the equations in predicting IP and VG was given by the determination coefficient. The results obtained by the equations were compared with the actual values observed at 1, 2, 3, and 4 minutes after the beginning of insufflation. The aim of this prospective clinical trial was to establish reliable parameters to guide surgeons through creation of the pneumoperitoneum in selected patients, providing objective data to determine the real position of the Veress needle. Predetermined time points during creation of the pneumoperitoneum were correlated with IP and VG. This was done in order to establish the expected values for IP and VG (dependent variables) in function of time (independent variable). This relation was mathematically expressed by an equation that correlated the variables.16 The correlation coefficient is a pure number that indicates whether correlation is perfect (¼1), strong (>0.75 and <1), average (>0.5 and <0.75), weak (<0.5), or absent (¼0).12 In the present study, a strong correlation was observed between IP and time and VG and time. The coefficient of determination indicates the accuracy of a predicted value of a variable (dependent) in the function of another variable (independent). In the present study, equations for pressure and volume prediction devised from the regression curves (Figs. 2 and 3) were tested, and a high determination coefficient was observed between pressure and time, as well as between volume and time. In order to minimize the effects of surgical scars, peritoneal adhesions, and obesity on the elasticity and complacency of the abdominal wall (which could work as confounding factors and influence the results), patients with a history of surgery and peritonitis, as well as with BMI over 30, were not included Table 2. Predicted Values of Pressure and Volume at Given Moments of Insufflation Applying the Estimated Modelsa Observation time in seconds Mean Mean Mean Mean values values values values and standard deviation of measured pressure (mm Hg) of estimated pressure (mm Hg) and standard deviation of measured volume (L) of estimated volume (L) 1 minute 2 minutes 3 minutes 4 minutes 4.34 (1.48) 4.15 1.11 (0.14) 1.12 6.05 (1.44) 6.27 2.18 (0.21) 2.07 8.44 (1.47) 8.36 3.13 (0.27) 3.01 10.43 (1.48) 10.10 3.87 (0.40) 3.95 a (pressure ¼ 2.3083 þ 0.0266time þ 8.310ÿ5time2 ÿ 2.4410ÿ7time3; volume ¼ 0.813 þ 0.0157time). Mean values and standard deviation of measured pressure and mean values of predicted pressure. 4 AZEVEDO ET AL. in the present study. In addition, the flow rate was set at 1.2 L=min, which is known to be adequate for gradual creation of the pneumoperitoneum (minimizing hyperreflexia of the parasympathetic nervous system), and the expected values of volume (0.2 L=s) were determined. The protocol for curarization was rigorously followed in order to avoid undesired effects on IP values. The present study allowed pressure and volume values to be accurately predicted at key moments during insufflation in a selected population (Table 2). Time points at 1, 2, 3, and 4 minutes were chosen to show the insufflation process from beginning to end. The resulting algorithms might be entered in an insufflator processor, as a safety device, helping the surgeon to identify the incorrect positioning of the Veress needle during insufflation or even an inappropriate degree of abdominal muscle paralysis. Further studies, involving a random population and investigating the effects of BMI, sex, and a history of abdominal surgery on pressure and volume curves, are being undertaken. 6. 7. 8. 9. 10. 11. 12. Conclusions Values for IP and VG at certain time points during insufflation for creation of the pneumoperitoneum, using the Veress needle in a selected population, are effective parameters to determine whether the needle is correctly positioned in the peritoneal cavity. 13. 14. Disclosure Statement No competing financial interests exist. 15. References 1. Rajesh V, Gupta JK. Laparoscopic entry techniques: Clinical guideline, national survey, and medicolegal ramifications. Surg Endosc 2008;22:2686–2697. 2. Azevedo JLMC, Azevedo OC, Miyahira SA, Miguel GPS, Becker JOM, Hipólito OHM, Machado ACCG, Cardia W, Aguiar GS, Godinho LS, Freire DF, Moreira CH, Almeida CES. Injuries caused by Veress needle insertion for creation of pneumoperitoneum: A systematic literature review. Surg Endosc 2009;23:in press. 3. Baadsgaard SE, Bille S, Egeblad K. Major vascular injury during gynecologic laparoscopy. Report of a case and review of pubished cases. Acta Obstet Gynecol Scand 1989;68:283–285. 4. Bergqvist D, Bergqvist A. Vascular injuries during gynecologic surgery. Acta Obstet Gynecol Scand 1987;66:19–23. 5. Bonjer HJ, Hazebroek EJ, Kazemier G, Giuffrida MC, Meijer WS, Lange JF. Open versus closed establishment of pneu- 16. moperitoneum in laparoscopic surgery. Br J Surg 1997:84: 599–602. Catarci M, Carlini M, Gentileschi P, Santoro E. Major and minor injuries during the creation of pneumoperitoneum. A multicenter study on 12,919 cases. Surg Endosc 2001;15: 566–569. Chapron CM, Pierre F, Lacroix S, Querleu D, Lansac J, Dubuiosson JB. Major vascular injuries during gynecologic laparoscopy. J Am Coll Surg 1997;185:461–465. Fruhwirth J, Koch G, Mischinger HJ, Werkgartner G, Tesch NP. Vascular complications in minimally invasive surgery. Surg Laparosc Endosc 1997;7:251–254. Hanney RM, Alle KM, Cregan PC. Major vascular injury and laparoscopy. Aust N Z Surg 1995;65:533–535. Roviaro GC, Varoli F, Saguatti L, Vergani C, Maciocco M, Scarduelli A. Major vascular injuries in laparoscopic surgery. Surg Endosc 2002;16:1192–1196. Schafer M, Lauper M, Krahenbuhl L. Trocar and Veress needle injuries during laparoscopy. Surg Endosc. 2001;15: 275–280. Peterson HB, Greenspan JR, Ory HW. Death following puncture of the aorta during laparoscopic sterilization. Obstet Gynecol 1982;59:133–134. Azevedo OC, Azevedo JLMC, Sorbello AA, Miguel GPS, Guindalini RSC, Godoy AC. Veress needle insertion in the left hypochondrium in creation of the pneumoperitoneum. Acta Cir Bras 2006;21:296–303. Azevedo OC, Azevedo JLMC, Sorbello AA, Miguel GPS, Wilson JL, Jr, Godoy AC. Evaluation of tests performed to confirm the position of the Veress needle for creation of pneumoperitoneum in selected patients: A prospective, clinical trial. Acta Cir Bras 2006;21:385–391. Azevedo JLMC, Guindalini RSC, Sorbello AA, Silva CEP, Azevedo OC, Aguiar GS, Menezes FJC, Delorenzo A, Pasqualin RC, Kozu FO. Evaluation of the positioning of the tip of the Veress needle during creation of closed pneumoperitoneum in pigs. Acta Cir Bras 2006;21:26–30. Guyatt G, Walter S, Shannon H, Cook D, Jaeschke R, Heddle N. Basic statistics for clinicians: 4. Correlation and regression. CMAJ 1995;152:497–504. Address correspondence to: João L.M.C. Azevedo, MD, PhD Department of Surgery Federal University of São Paulo R. Joaquim Tavora, 550, Apt. 101-A São Paulo 04015011 Brazil E-mail: [email protected]
Baixar