FROM 15 TO 115 YEARS OF LIFE Mortality trends in Portugal 2000 ‐ 2008 Maria do Céu Machado Luisa Couceiro Isabel Alves Ricardo Almendra Maria Cortes Pedro Pimentel Rui Cruz Ferreira Application to ‘Prémio Sociedade das Ciências Médicas de Lisboa / MSD em Epidemiologia Clínica 2010’ Application for the 2010 SCML Award 1 … Custa‐me morrer porque nunca tive tanta vida acumulada… Vitorino Nemésio, 1977 (at 76 years old) Application for the 2010 SCML Award 2 Index 1. Introduction 2. Objectives 2.1. Global objective 2.2. Specific Objectives 2.2.1. Evolution of adult mortality in Portugal in the first decade of the 21st century based on a comparative analysis of the years 2000, 2004 and 2008 2.2.1.1. Death registration based on death certificates 2.2.1.2. Diagnosis‐related Group data 2.2.2. Supporting terminally‐ill patients and their families 2.3. Questions to be answered 3. Methodology 3.1 Data sources and variables 3.1.1. Comparative analysis of adult mortality, by causes and premature mortality 3.1.2. Intra‐hospital lethality 3.1.3. Care for terminally‐ill patients and family: hospital services organization 3.1.4. Experience and training of doctors and nurses dealing with Terminally‐Ill Patients 3.2. Limitations of the study 3.3. Data Protection 4. Results 1 4.1 From 2000 to 2008 – mortality data trends 4.1.1 Birth rate, death rate and migrations 4.1.2 Comparative analysis of death rates in 2000, 2004 and 2008 Change in death rate Gender and age group Place of residence Marital status Occupation and status at work Nationality Place of death Causes of death Data quality 4.1.3 Potential Years of Life Lost by cause of death Overall Health‐care‐sensitive Application for the 2010 SCML Award 3 Index 4.2 Death in 2008 by place of death Gender and age group Place of residence Marital status Occupation and status at work Nationality Causes of death Data quality Specific aspects related to the place of death 5. Results 2 5.1 Change in intra‐hospital lethality rate from 2000 to 2008 5.1.1 Admissions, deaths and intra‐hospital lethality Gender and age group Place of residence Place of hospitalization Cause of hospitalization External causes 5.1.2 Circulatory diseases 5.1.2.1 Ischemic heart disease Gender and age group Place of residence Place of hospitalization Profile of the in‐patient (hospital discharge or death) 5.1.2.2 Stroke Gender and age group Place of residence Place of hospitalization Profile of the in‐patient (hospital discharge or death) 5.1.3 Cancer Female Breast, Cervical, Colo‐rectal, Prostate and Tracheal, bronchial and lung Gender and Age group Place of residence Place of hospitalization Profile of the in‐patient (hospital discharge or death) 5.1.4. Multivariate Logistic Regression Application for the 2010 SCML Award 4 Index 6. Terminally‐ill patients 6.1. Organization of Portuguese hospital Departmens Departments strategy for the TIPs Strategy to support family 6.2. Doctors and nurses experience and training Discussion Limitations of this paper Conclusions and recommendations 7. Discussion 8. Conclusions and Recommendations Bibliography Annex Application for the 2010 SCML Award 5 Acknowledges Acknowledges To Dr. Ricardo São João, professor at Departamento de Informática e Métodos Quantitativos (DIMQ) / Escola Superior de Gestão e Tecnologia de Santarém (ESGTS), for the development of logistic regression model. To Dr. Eduarda Góis and Dr. Maria dos Anjos Campos, from Statistics Portugal for the data disclosed. Application for the 2010 SCML Award 6 Introduction 1. Introduction Researchers, technicians and political decision makers believe that the analysis of a population's state of health, its determinants and distribution have become increasingly important in planning and defining intervention policies and programmes based on evidence as well as in monitoring and evaluating health systems (Mathers et al., 2003). Although the concept of health is complex, multidimensional and multisectoral, the study of mortality as a proxy indicator of the population's state of health is one of the most widely used indicators since it is an objective, unequivocal and universal event. The analysis of mortality by causes enables the study of diseases leading to death. There are new indicators, new approaches and challenges regarding records and the comparability, reliability, validity and interoperability between death registration systems. By definition, a death certificate is a civil registry instrument that certifies the death of any individual that occurred in Portuguese territory (citizen’s website). However, this document is extremely important not only at an administrative level but also for research purposes and should not be seen as a final act but rather “…an instrument of life… that enables the last moments of life to continue at the service of life” (cit. Ministry of Health, Brazil, 2006). Ideally, a country's vital statistics registry systems should include all deaths that take place within its borders and ensure the quality of basic desagregation such as gender, age, and cause of death. However, not all countries have systems with the same level of coverage and quality that enable data comparability, whereby this constitutes one of the World Health Organisation's goals (WHO, 2005). In Portugal, the most widely used databases to analyse mortality are the Statistics Portugal (INE) from the death records that identify all deaths that occur in Portugal, and the Diagnosis Related Group (DRG), under the responsibility of the Central Health System Administration (ACSS), that reports the deaths that take place at National Health Service (NHS) Hospitals. Application for the 2010 SCML Award 7 Introduction The comparability of data according to causes of death between different systems or time and local has been facilitated due to development and ongoing revision of International Statistical Classification of Diseases and Related Health Problems, currently undergoing its 10th revision. However, in Portugal, not all databases with information concerning diseases and causes of death based on last revision. In DRG´s databases, coding is done according to the 9th revision and in INE´s mortality base according to the 10th revision. The conversion of one to the other should be well defined and simple but this is not the case for all diseases. For example, liver cirrhosis that was coded with a single code in the 9th revision (571), in the 10th revision is described by a set of codes including a 4 digit code (K70.3, K71.7, K74.3, K74.4, K74.5, K74.6). As for motor vehicle accidents, they were initially represented with a small group of sequential codes (E810‐E825) and then changed to a more complex group (in which some interim codes were excluded because they referred to accidents with other types of vehicles): V02‐V04, V09, V12‐V14, V19‐V79, V86‐V89. Difficulties also arose regarding the cause responsible for the death, namely in elderly population with several chronic diseases. It becomes even more complicated when dealing with hospitalised patients´ deaths due to the fact that DRG bases do not have a field in which to identify the cause of death. Generally, the main cause of the hospitalisation is used in the study of intra‐hospital lethality. Records with an unspecified cause of death constitute one of the biggest constraints associated to the analysis of the deaths. In Portugal, there is still a large number of records with the cause of death classified as “Symptoms, signs, abnormal exams or ill‐defined causes”, representing over 10% of total deaths. According to data from the HFA‐WHO Database 2010, in 2004, Portugal had a standardized death rate classified as “symptoms, signs, abnormal exams and ill‐defined causes” for 62/100 000 inhabitants, which is much higher than in the rest of EU countries (average: 16,7; best value: 3,0 in the United Kingdom). Excessively high values without a defined diagnosis as well as injuries with undetermined intention, cancer of other locations and in ill‐defined locations or cardiac insufficiency compromise the usefulness of the information and have been Application for the 2010 SCML Award 8 Introduction identified as bad quality indicators when completing the death registration per causes (Mathers et al., 2005). The completeness of death certificates is an extremely important medical act and should be seen as an ethical obligation (Ministry of Health Brazil, 2006). The interoperability between different systems constitutes yet another challenge for the study of mortality and its determinants. In Portugal, the introduction and development of Information and Communication Technologies (ICT) in different health care levels has not been efficient in crossing information that is essential for epidemiological knowledge as well as for service and health system planning. The emerging of non‐integrated systems means wasting more resources (human and technical) and generates replicated or contradictory data that hinders the analysis and leads to wrong conclusions (Ferreira et al., na). Some points should be highlighted regarding information that is obtained through the analysis of official databases, namely life expectancy and mortality to evaluate a population's state of health, given the greater availability and comparability of these indicators, in comparison to morbidity indicators. The life expectancy is calculated considering the mortality observed for each gender and age group at a given time, summarising information regarding all population groups. In the European region, life expectancy at birth continues to increase (Eurostat, 2010). Between 2000 and 2007, for the 15 European countries, the longevity increased from age 75,48 to 77,65 for the male gender and 81,92 to 83,52 for the female gender. Average longevity in the 27 European Union countries is lower. According to data from 2007, European men and women live, on average, between 76,07 and 82,21 years. The European Health Report 2009 (WHO/Europe, 2010) ensures that the health of the population in the 53 countries of WHO European Region has improved in the past decades. Gains Application for the 2010 SCML Award 9 Introduction in life expectancy are attributed to overall decreasing mortality, mainly from declining communicable diseases in early childhood and delays in premature death among adults due to improved health care. Further changes in the patterns of mortality and the burden of disease, with chronic non‐communicable conditions, injuries and violence affecting health more strongly, are driven by changes in lifestyles and behaviour. When comparing the evolution of the life expectancy at birth in European countries, a generically uniform growth pattern stands out. Therefore, in the beginning of the observation period, countries like Sweden had the highest values and in 2007 its population still lived the longest. On the other hand, the Baltic countries and Eastern European countries continue to have a lower life expectancy at birth than the remaining countries. Greater longevity of citizens from most developed countries can be justified by higher life and educational levels, healthier life styles and easier access and better quality health services in comparison to other European countries (WHO, 2009). Several studies have been carried out on the inequalities in health associated to social and economic factors, as well as to gender. Among others, the Eurothine Project (Eurothine, 2007), funded by the public health programme of the SANCO Directorate General of the European Commission, followed by the EURO‐GBD‐SE project, aiming at assessing the potential for reduction of health inequalities in Europe (http://www.euro‐ gbd‐se.eu/index.php?id=371). In the 2004‐2010 Portuguese National Health Plan, a strategic instrument for national health planning, global mortality is analysed (all causes) according to lifecycle as well as mortality due to several specific causes such as cancer, cardiovascular diseases, HIV‐AIDS or suicide (priority areas that have national coordinations already in place), car accidents and work related accidents (Portuguese National Health Plan, Atlas, Alto Comissariado da Saúde, 2010). The analysis of traditional rates such as mortality and life expectancy should be done along with the study of other mortality indicators to obtain a more comprehensive understanding of the state of health, of necessities and priorities such as premature and avoidable mortality. Application for the 2010 SCML Award 10 Introduction The Potential Years of Life Lost (PYLL) have been used to determine premature mortality1. The traditional mortality rates referred above help identify the main causes of death based on the deaths count, regardless of the age in which they occurred. Higher PYLL means a premature death to which a greater social value is given, since death occurred during active life and potentially more productive, depriving society of its economic and intellectual potential (Peixoto et al., 1999). The concept of causes of avoidable mortality appeared in 1970 to evaluate the quality and performance of health systems (Nolte et al., 2008). In 1976, a study conducted by several researchers, led by Rustein (Treurniet et al., 2004) identified a group of causes (disease, handicap or death) that were considered avoidable through preventive or curative care. This list was amended in 1980 and since then several authors have amended or created new groups of causes. In Europe, the list presented in the study led by Nolte (2004) is the most used. It identifies causes of death and related age groups that are considered avoidable through primary prevention (3 causes) or timely and effective health care (34 causes). The analysis of the PYLL by this group of causes helps identify priority intervention areas and enhances the potential for gains in health. As referred above, cardiovascular diseases and cancers are the two main causes of death in Portugal. Differences in socioeconomic status have been consistently associated with stroke incidence and mortality across multiple populations. In a recent Swedish study, age‐standardised incidence of coronary heart disease was found to be high in high‐deprivation neighbourhoods (Winkleby et al., 2007). The inverse association between socioeconomic status and stroke is strongest for mortality and incidence of stroke, with low socioeconomic groups showing lower survival (Kunst, et al., 1998) and higher stroke incidence in many populations in developed countries Cancer is the second leading cause of death in Portugal, but the first amongst population under age 65. WHO calculates that in 2020, 10 million people will due of cancer which corresponds to 1 The main sources of European statistical information such as Eurostat or OCDE use the age limit of 69 (included) but there are researchers that calculate the PYLL based on life expectancy. Application for the 2010 SCML Award 11 Introduction an increase of 61%, in comparison to the year 2000. In Europe, there is a foreseen increase of 24% between the year 2000 and 2020 (WHO, 2003). Incidence rates vary depending on the type of cancer. Therefore, there has been a reduction in the incidence of certain types of cancer such as stomach cancer while colorectal and melanoma cancer have increased. In order to have a better understanding of oncological patient needs, attention has been placed on aspects that were neglected in the past, such as psychosocial issues and care for terminally‐ill patients. Patients receiving psychosocial support have a higher tolerance towards the effects of treatment and, in cases where there is no cure, palliative care helps patients live their last days with dignity and without suffering. In cases of the hospitalization of death, hospital services must be prepared to support the terminally‐ill patient and family. These situations are a professional and personal challenge for doctors and nurses because it depends on their emotional stability and attitude towards death and the disease and on previous personal experiences (Marques et al, 1991). Literature shows that there are differences in the perceptions and behaviour of doctors and nurses in approaching these issues as well as differences between generalist and specialize care professionals (Natan, et al., 2010; Murakawa et al., 2009). This work seeks to measure the reliability of death data (Death Certificate and Diagnosis‐related Group) and the comparability of databases; understand the organisations of hospital services and doctors and nurses’ experience and training on terminally‐ill patient and family support. The reliability of the information regarding adult mortality in Portugal conditions the adequacy of interventions to the real needs of the population. Application for the 2010 SCML Award 12 Objectives 2. Objectives 2.1. Global Objective There is evidence of a positive evolution of the Portuguese population’s health during the last two decades of the 20th century due to a drop in mortality rates regarding all ages and an increase in life expectancy. The period between 2000 and 2008 was marked by policies such as the Primary Care reform, the creation of Long Term Care and the elaboration and implementation of the first National Health Plan for 2004‐2010 that includes Priority Programmes such as National Coordination Bodies for Cardiovascular Diseases and Oncological Diseases. The evolution of mortality during this century is a parameter that needs to be monitored as a basis for future health strategic planning. There are official databases on mortality such as the Statistics Portugal, constructed from data registration on death certificates and the ones from hospital coding through the Diagnosis‐ related Groups. This study's objective was to become aware of the burden of diseases and death, in its demographic, social and clinical aspects, based on the death registration in Portugal. 2.2. Specific Objectives 2.1.1. Evolution of mortality in Portugal in the first decade of the 21st century. Comparative analysis of 2000, 2004 and 2008 2.1.1.1. Mortality registration based on death certificates • Gender, age groups, occupation, nationality and causes; • Potential Years of Life Lost due to the death • Specific aspects related to the Place of Death Application for the 2010 SCML Award 13 Objectives 2.1.1.2. Diagnosis‐related Group data • Hospitalisation and intra‐hospital lethality • Specific aspects related to Ischemic Heart Disease, Stroke and Cancer 2.1.2. Supporting terminally‐ill patients and their families 2.1.2.1. Organisation of the hospital services 2.1.2.2. Doctors and nurses experience and training 2.3. Questions to be answered What is the level of reliability of Portuguese mortality registration and the adequacy of the items registered in regards to the needs of epidemiological knowledge? What is the burden of premature death and avoidable death considered amenable to health care on the overall mortality? Are age and causes of death determinants in the place of death (hospital, at home or public places)? What are the diagnosis associated and related with the risk of dying due to cardiovascular disease and cancer? These research can drive improvements on registration systems and health policies, for the planning and execution of intervention models as well as to respond more efficiently to the patient's and their family's needs. Application for the 2010 SCML Award 14 Methodology 3. Methodology 3.1. Data sources and variables Data from the Statistics Portugal (INE) was used to make a comparative analysis of general mortality, by causes and premature mortality. For intra‐hospital lethality, data from records pertaining to Diagnosis‐related Group (DRG) of the Central Health System Administration (ACSS) was used. In the last decade, the Portuguese health‐care system was subject to various reforms that need to be monitored. For this study, 2000, 2004 and 2008 years data were used, which were considered most suitable, thus enabling an evolving analysis but under similar social organisational contexts and the health‐care system itself. It was also taken into account only the deaths of people ages 15 and up (≥15 years old), as it was thought that causes of death associated with children and young people are extremely specific for that group. Ages were grouped as follows: ages 15‐24; 25‐44, 45‐64, 65‐74, 75‐84; and ≥85. This is because the causes of death linked to each of these groups showed a more homogeneous pattern among themselves. The data pertain to Mainland Portugal. Concerning terminally‐ill patients and their family, data were collected regarding hospital services organization to support Terminally‐Ill Patients (TIP’s), as well as data related to doctors and nurses’ experience and training. Application for the 2010 SCML Award 15 Methodology 3.1.1. Comparative analysis of adult mortality, causes of death and premature mortality The information on mortality occurring in Portugal, particularly by causes of death, is registered in annual databases for which the INE is responsible, where each form contains vast information, including gender, age, nationality, date of birth, date of death, place of residence, cause of death, etc. (INE, 2009). According to standards set forth by the INE and the Statistical Council (CSE), no individual or institution may access the mortality database, as it contains data that is considered extremely sensitive. Thus, based on the latest report model regarding the death of individuals that are at least 28 days old (notation instrument no. 9466, of the INE2), available variables and those that are of interest to the study were identified. The aforementioned report contains information regarding causes of death (main cause, in sequence of some event), type of death (natural, non‐natural, under investigation), type of non‐ natural death (accidents, murder, suicide), date, place (hospital/clinic, at home, public places), basis for indicating the cause of death (data of a medical records, autopsy, official report drawn up by the administrative authority, other official documents), gender, date of birth, marital status, birthplace, nationality, customary residence, status at work, occupation, occupational situation, branch of activity. The following table summarises the data made available by the INE (for years 2000, 2004 and 2008). 2 The INE’s notation instrument no. 9466 has been used up to 2007; this was the year that marked the completion of the process for de‐materialising hard‐copy information. Since then, the information collected by Civil Registries is sent to the INE via electronic file transfer. However, these files contain fields that must be filled in, similar to fields in the previous report. Application for the 2010 SCML Award 16 Methodology Table 1 Summary of data made available by the INE Group General mortality Desegregation Place of residence (NUTS II – D.L. 1999), gender, marital status, age, nationality, status at work, occupation and occupational situation Mortality by cause of death Place of death, pace of residence (NUTS II – D.L. 1999), gender and age Place of death, basis for indicating the cause of death Place of death, marital status Place of death, status at work Place of death, occupational situation Place of death, occupation Place of death, nationality Potential Years of Life Lost Place of residence (Health Centre Group), cause of death Note: Selected causes of death are given in Annex 1. In addition, upon request, Foreigners and Borders Control Authority (SEF) made available estimates for foreign population residing in Portugal in 2004 and 2008, broken down by age group and nationality. Estimates for year 2000 weren’t available. Some quality‐cheeking techniques, based on a set of validations for coherence, were applied to data available. INE data was arrayed in tables according to the objectives set forth for each subchapter. Subchapter 4.1.1 – birth rate, mortality and migrations – chiefly aimed at general contextualisation, showed the evolution (2000‐2008) of overall results of birth rates, mortality rates and migratory growth rates as well as average life expectancy at birth for men and women (data collected at the INE website). Subchapter 4.1.2 – Comparative analysis of mortality rates in 2000, 2004 and 2008 – examined how the mortality rate evolved in the population age 15 and up by gender, age group, place of residence, marital status, status at work, occupational situation, occupation, nationality, place of death and cause of death, most notably the cause “Symptoms, signs, abnormal findings, ill‐ defined causes” as this is a good indicator of data quality. This subchapter also examined the basis for indicating the cause of death, particularly for autopsies. According to the aforementioned variables, we calculated age‐specific and crude death rates and respective 95% confidence intervals, to account for the uncertainty that arises from the natural variation inherent in the biological and random processes governing the occurrence of events as Application for the 2010 SCML Award 17 Methodology deaths and illnesses. Dealing with large samples of data (>100), confidence intervals were calculated using the normal approximation (Washington State Department of Health, 2002). Confidence intervals were used as a test of significance when comparing two death rates, since if respective confidence intervals do not overlap, a comparable statistical test would always indicate a statistically significant difference. When confidence intervals around the rates being compared overlap, the difference between those death rates can be significant or not. In accordance, in this situation, a statistical test for the difference of rates was performed, admitting that variance was the same. Null hypothesis was H0: rate’s difference equals zero and alternative hypothesis was Ha: rate’s difference not equal to zero. Under H0, test statistics has a t‐distribution with (n+m‐2) degrees of freedom, where n and m stand for dimension of each sample (Hogg et al., 1995). Along with figures for crude mortality rates, age‐standardised death rates were also calculated (using the direct standardizing method and the population of Mainland Portugal as standard population). This indicator was calculated for mortality by place of residence (taking into account geographical units corresponding to level II of Nomenclature of Territorial Units for Statistics ‐ NUT II, with delimitation according to Decree‐Law no. 317/99, dated 11 August), as well as mortality by marital status and nationality. Standardised death rates by age (SDR) were later analysed according to the measure of risk of death linked to the application of direct methods ‐ Comparative Mortality Index (CMI) ‐ to establish the correct comparison between figures for the Regions and those for Mainland Portugal. Thus, the quotient between the SDR for Region X and the SDR for Mainland Portugal was calculated and the result multiplied by 100. If the figure is close to 100, the risk in the Region is identical to that for Portugal; if the CMI is greater than 100, the risk in the Region is higher than that for the nation; and if the CMI is less than 100, the risk of death in the Region is lower than in Mainland Portugal. To test whether the differences between the Region being examined and the Mainland are statistically significant, hypothesis testing was conducted, where H0: CMI for Region X =100 and Ha: CMI of Region X ≠ 100, whose associated testing statistics can be consulted in Rabiais et al. (2004). A 5% level of significance is assumed. Application for the 2010 SCML Award 18 Methodology Subchapter 4.1.3 pertains to the evolution of the Potential Years of Life Lost (PYLL)3 according to the main groups of causes of death, as well as those considered to be avoidable through primary prevention and with appropriate health care. The methodology used for calculating the PYLL was that of the INE, which considers deaths from ages 0 to 69, while the one recommended by Ellen Nolte (2004) was used for selecting the causes of death. Annex 2 is the list of selected causes for each main group (primary prevention or health care), the corresponding codes from the International Classification of Diseases – 9th version (ICD 9) and 10th version (ICD 10), as well as the ages being considered. Subchapter 4.2 – Mortality rates in 2008 by place of death – sought to answer the question, “Where do people die in Portugal?” The tables given under the previous subchapters were reproduced and distributed according to the place where the death occurred: in the hospital/clinic, at a home (this category includes deaths occurring in private residences or nursing and residential homes) and elsewhere (public places). In this chapter, significance tests were developed to check whether there are significant differences in the distribution of deaths by place of death. For each cross analysis (place of death x each one of the other variables being studied) a Chi‐square test on independence of variables was performed, to test the existence of a relation between place of death and each one of the variables referred. Chi‐square test informs about independence between variables but not about the degree of association existent. In addition, this test is very influenced by the size of the group being studied. So, based on the Chi‐square values, some association measures were computed: Phi coefficient, Contingency coefficient and Cramer’s V, and null hypothesis (each of the measures being zero) was tested (Pestana et al., 2003). To outline the average profile of the population that died in 2008, was considered the greatest frequency recorded under the variables of gender, marital status, nationality, status at work, job status, occupation, place of death, cause of death and average age. The 2003 and 2007 versions of Microsoft Office Excel, as well as statistical analysis software SPSS 15.0 for Windows were used for the cross‐tabulation, statistical analysis and graphic and 3 Number of years that a given population theoretically does not live because of premature death (before age 70). Application for the 2010 SCML Award 19 Methodology alphanumeric depiction of data. The ArcMap version 9.2 geographical information system software was also used for illustrating the geographical distribution of the occurrences being studied. 3.1.2. Analysing intra‐hospital lethality Chapter 5 examines intra‐hospital lethality. Information regarding hospital admissions was obtained by recording the Diagnosis‐related Group (DRG) of the ACSS. This database includes every admission occurring at a hospital of the Portuguese National Health Service (NHS), except psychiatric hospitals. It contained information regarding the patient’s (age, gender, place of residence) as well as the admission (hospital service, admission and discharge dates, main and related diagnosis, external causes, procedures, type of discharge, number of days hospitalised, admission and discharge times, and DRG code). The databases examined pertain to years when hospital discharges were recorded (2000, 2004 and 2008). Recorded occurrences are equivalent to admissions, not to hospitalised individuals, and the same individual may be linked to a variable number of admissions, pertaining to different bouts of disease and/or to recurring admissions for occurrences of the same disease (Nicolau, 2009). According to the general definition of admission, these are the set of services intended for situations where an individual is admitted to a hospital or clinic, during a given period, where he/she takes up a bed, for diagnosis or treatment, with a stay of at least twenty‐four hours, except in cases where patients end up dying, discharging themselves against doctor’s orders, or being transferred to another hospital or clinic, and his/her stay at that hospital or clinic is less than twenty‐four hours (Ministry of Health, Portugal, 2010). As given under the definition, the research group also took into account admissions for less than 24 hours, with a few exceptions explained below. Application for the 2010 SCML Award 20 Methodology By 2006, DRG records included only occurrences of hospital admissions; however, as of that year, they also contained occurrences of clinical outpatient care4 (day hospital, radiotherapy, chemotherapy and haemodialysis). To minimise the effect caused by the introduction of medical outpatient DRG (in August 2006 for invoicing to subsystems and in 2007 to the Portuguese NHS), and in order to allow for the evolving and comparative analysis of data for the period being considered, the research team chose to exclude occurrences with zero‐day admissions grouped under DRG 409, 410, 876 and 317 (corresponding to direct admissions: radiotherapy, chemotherapy and haemodialysis) or those whose “Module” field showed day hospital (“HDI”) and direct admissions (“RAD”). Codes pertaining to complications during pregnancy, delivery and puerperium (ICD 9: 630‐676) were also removed. The ICD 9 code occurring in the main diagnosis5 was regarded as a cause of death. The intra‐hospital lethality rate is understood to be the rate of deaths occurring in hospitals relative to the number of recorded admissions. When calculating rates of intra‐hospital fatalities caused by specific deaths, the rates are calculated by taking into account the deaths and admissions due to such causes. The following diagram summarises inclusion and exclusion criteria being considered for calculating admissions and intra‐hospital lethality rate (Figure 1). 4 For the purposes of classifying DRG and their invoicing, a Clinical Outpatient DRG corresponds to one or more medical actions carried out with the same therapeutic and/or diagnostic objective, performed during the same diagnostic or therapeutic session within a 24‐hour period. By specialty, there can be only one DRG per day, which includes every action performed during the same session, except chemotherapy treatments carried out together with radiotherapy, or chemotherapy treatments carried out together with the insertion of a fully implanted vascular access device (http://portalcodgdh.min‐ saude.pt/index.php/Epis%C3%B3dio_de_ambulat%C3%B3rio_m%C3%A9dico) 5 Main Diagnosis is designated and defined as being that which, after examining the patient, is considered to be responsible for his/her admission to the hospital for treatment (http://portalcodgdh.min‐saude.pt) Application for the 2010 SCML Award 21 Methodology Intra-hospital lethality Figure 1 Inclusion and exclusion criteria for calculating intra‐hospital lethality rate Admission due to complication during pregnancy, delivery and Yes Exclude Yes Exclude Yes Exclude No Is he/she under age 15? No Add to the denominator (We consider every non-excluded occurrence up to…) Did he/she survive? No Add to the Numerator (only deaths are part of the numerator) Subchapter 5.1.1 examined occurrences such as hospitalisation, deaths of hospitalised patients and the intra‐hospital lethality rate by gender, age group, place of residence, place of Application for the 2010 SCML Award 22 Methodology hospitalisation and causes (hospitalisation‐related and external). Occurrences such as hospitalisation and deaths were linked to NUT II and NUT III, according to patients’ place of residence, and linked to Health Regions, taking into account the location of the hospital where the occurrence took place. However, in distributions involving the use of the residence code, the national totals are always higher than the sum of the Regions, since there are deaths with an invalid residence code based on which the Region cannot be verified. Based on the DRG records, origin – destination maps were also prepared, taking into account the hospitalisation location (hospitals) and residence of in‐patients, in terms of the municipality. These flows were carried out only for Hospitals and/or Hospital Centres considered to be more differentiated, with those selected being the following: Western Lisbon Hospital Centre (CHLO), Northern Lisbon Hospital Centre (CHLN), Central Lisbon Hospital Centre (CHLC), Coimbra University Hospitals (HUC), Coimbra HC (CHC), São João Hospital, Santo António Hospital and Faro Hospital. This analysis involved the use of tools found in the ET Geowizard available for ArcMap. In subchapter 5.1.2 previous analyses were repeated but specifically for circulatory diseases, with particular focus on ischemic heart disease and stroke, and cancer (female breast, cervical, colorectal, tracheal, bronchus and lung and prostate), the leading causes of death in Portugal. The following table summarises the ICD 9 codes used for identifying the aforementioned causes (Table 2). Table 2 Causes of death examined and their corresponding ICD 9 codes Causes of death Diseases of the circulatory system ICD 9 390 ‐ 459 Ischemic heart diseases 410 ‐ 414 Cerebrovascular diseases 430 ‐ 434 Cancers 140 ‐ 208 Cancer of female breast 174 Cancer of cervix uteri 180 Cancer of colon and rectum 153; 154.0 ‐ 154.1 Cancer trachea/bronchus/lung 162 Cancer of prostate 185 Application for the 2010 SCML Award 23 Methodology For each of these causes, it was outlined an average profile for the in‐patient and for the death, taking into account the average age and the greatest frequency for gender, place of residence, place of hospitalisation and related diagnoses. To depict the related diagnoses, the basis was broken down, as shown in Figure 2. Figure 2 Schematic depiction for the selection of related hospitalisations Dr 1 2 3 4 5 6 Ddx2 X X x x x Ddx3 X X X Dr 1 2 4 5 6 2 4 5 Ddx2+ ddx3 X X X X X X X X To identify the potential profile of the patient with hospital discharged or that died by the selected causes, we developed an exploratory multivariate analysis by logistic regression models. The dependent variable is the mortality and others are age, sex and secondary diagnoses. To test the suitability of the adjustment was applied Hosmer and Lemeshow test and to analyze the proportion of variance in the dependent variable that can be explained by the model Cox & Snell R Square and Nagelkerke R square values were used. The 2003 and 2007 versions of Microsoft Office Excel and the ArcMap version 9.2 geographical information system software were used for providing the graphic depiction of the results obtained. 3.1.3. Care for terminally‐ill patients and family: hospital services organization Chapter 7 examines how hospital services are organised, as well as the training and experience of professionals in following up on Terminally‐Ill Patients (TIPs). Application for the 2010 SCML Award 24 Methodology Support to TIPs and their families require some organisation on behalf of hospital services, as well as training the doctors and nurses accompanying them. TIPs are understood to be patients whose clinical status shows that they are near death, while medical decisions are directed toward relieving symptoms. Through inquiry no. 1, which targets all public Hospital Services (excluding Palliative Care Units), the idea is to become increasingly aware of how Portuguese hospitals deal with this situation. The target population that is eligible to fill in inquiry number 1 includes Hospital Directors, Service Directors, Service Heads and Head Nurses, all of whom work at a public hospital in Mainland Portugal. Inquiry number 1 was organised into three parts: i) in the first part – General Information – the idea was to collect information regarding the professional’s institutional position as well as features of the hospital where the said professional works; ii) in the second part – The Service’s Strategy for TIPs – there were gathered information on the guidelines for transferring patients to and from the hospital, written and non‐written protocols for following up on TIPs in various situations, training of professionals; psychological, social, religious or language support, patients’ participation in decision‐making, home health care and volunteering; iii) in the third part – Supporting TIPs' families and news of their death – information was collected with regard to information and options given to families for following up on TIPs, the availability of psychological and social aid for families and how the family and the GP inform the death communication. No sample was taken, as all public hospitals in Mainland Portugal have been identified and selected. A pre‐test on the inquiry was conducted with 5 doctors, all of whom were Service Directors at different hospitals. The questions for the inquiry were entered in an application for editing and disclosure of inquiries online (FreeOnlineSurveys.com). This application automatically enters collected data on a password‐protected spreadsheet, to which the inquiry’s authors have exclusive access. Application for the 2010 SCML Award 25 Methodology The hyperlink to access the inquiry online was sent to the Board of Directors of every public hospital in Mainland Portugal, as they were asked to forward them to their Clinical Directors, Directing Nurses and Service Directors. The same procedure was carried out at Nursing Schools, which were asked to send the questionnaire’s hyperlink to Hospitals collaborating in the training of the Schools' students, as well as to Scientific Societies. The inquiries were available from 15 September to 15 October 2010. At the end of the period given for gathering responses, the inquiry was no longer available online, as the data recorded on the spreadsheet was exported to the SPSS (Statistical Package for the Social Science) software, version 15.0., for statistical analysis. The application used for creating the inquiry online makes it impossible to identify respondents, as the inquiry’s authors are unable to access respondents’ e‐mail addresses or the IP (Internet protocol identifier) of computers used. Considering the low number of responses obtained, only a descriptive analysis of data was performed, using the SPSS 15.0 for Windows. It starts off by making a characterisation of participants and an overall assessment of results. 3.1.4. Terminally‐ill patients family: doctors and nurses experience and training Inquiry number 2 is directed at all doctors and nurses working in a ward of a public hospital in Mainland Portugal, with the main objective of collecting information regarding the training and experience of these professionals in following up on TIPs. Inquiry number 2 was divided into three parts: i) part 1 – General Information – collecting information regarding the hospital where the professional works most of time (they were asked to consider their main institution); ii) in the second part – Characterising the health‐care professional – the idea was to find out the characteristics of doctor or nurse who was responding to the inquiry (gender, age, profession, specialty, year graduated and training); iii) in the third part ‐ Training of doctors and nurses in supporting TIPs ‐ the questions looked at the professional’s experience in following up on TIPs at the institution where he/she worked, in Application for the 2010 SCML Award 26 Methodology terms of frequency and type of follow‐up and support. The entire inquiry is enclosed (see Annex). A pre‐test on the inquiry was conducted with 7 doctors and nurses working in a hospital setting. The procedure used for making inquiry number 2 available online and collecting data on a spreadsheet was similar to that described for inquiry number 1. The inquiries were available from 15 September to 15 October 2010. As described in the previous inquiry, the analysis started off by characterising participants and by making an overall assessment of results. Next, the responses to the inquiry were arrayed according to respondent’s profession. 3.2. Limitations of the study Throughout the present study, the research team felt the need to deepen certain analyses but they were unable to do so, because of several constraints. Since they were unable to access the INE’s complete database of global death and causes of death, the cross‐tabulation of information, which would be of great value for this study and would enable the application of statistically sound methodologies, is limited or even non‐existent. The DRG database does not allow knowing the exact cause of death, as it indicates only the diagnoses identified and the procedures carried out throughout the hospitalisation period. On the other hand, this database contains NHS hospital records, thus excluding private facilities. Fields that were not filled in or which clearly have errors were also identified. The small number of responses to both inquiries hindered the possibility of carrying out statistical analyses that could provide sounder and more valid conclusions. This study, which basically involves hospitals and the experience of doctors and nurses, does not take into account the perception of the families of TIPs relative to the care provided. Application for the 2010 SCML Award 27 Methodology 3.3. Data Protection Data taken from the INE’s mortality database and from DRG record of the ACSS comply with all assumptions necessary to ensure data protection and statistical secrecy. The inquiries were also conducted while taking into account a set of regulations and procedures for ensuring the anonymity of professionals who answered them. From the outset, the research team has pointed out that this work would not disclose individual data or enable the identification of intervening parties. Therefore, a commitment of not revealing any identifying information was assumed by research team to the scientific community and to the intervening parties or their families. Application for the 2010 SCML Award 28 Results 1 4. Results 1 4.1. Change from 2000 to 2008 4.1.1. Birth rate, death rate and migrations From 2000 to 2008, the number of live births showed a relative decrease of 12,6%, and the crude birth rate dropped from 11,6 to 9,8 live births per 1000 population. The crude death rate showed a generally decreasing trend, with slight changes and a figure close to 10 deaths per 1000 population. The relative growth of the Portuguese population, during the same period, reached 3,9%. The increase in the number of residents was strongly determined by the migration balances, which were positive since the early 1990’s (over 60 000 new immigrants per year, from 2001 to 2003). In 2004, the migration balance was already below the figure achieved in 2000, and the migration growth rate continued to drop sharply. From 2000 to 2008, it decreased from 5,1 to 0,9 per 1000 population, thus representing a relative decrease of 83,1%. Life expectancy at birth (calculated for periods of three consecutive years) went from 76,63 years in 1999/2001 to 78,90 years in 2006/2008, for a relative increase of 3,0%. For males, the increase was slightly higher (3,3%, resulting from a change from 73,25 to 75,68 years) compared to the figure for females (2,6%, resulting from an increase from 79,84 to 81,94 years). The difference between genders was thus reduced, from 6,59 years at the start of the period to 6,26 years in 2006/2008. Table 3 Life expectancy at birth, birth rate, death rate and migration growth in Mainland Portugal 2000 (Pop=9 748 596) N Rate 2004 (Pop=10 017 709) N Rate 2008 (Pop=10 131 095) N Rate Variation 2000‐08 (%) N Rate Crude birth rate 1 113318 11,6 103309 10,3 99057 9,8 ‐12,6 ‐15,9 Crude death rate 1 100021 10,3 96946 9,7 99401 9,8 ‐0,6 ‐4,4 50000 5,1 45700 4,6 8800 0,9 ‐82,4 ‐83,1 Migration growth rate 1 2 Life expectancy at birth 76,63 77,62 78,90 3,0 (years) 73,25 74,32 75,68 3,3 M 79,84 80,73 81,94 2,6 F 1 Rate per 1000 population. 2 Life expectancy at birth obtained for the three‐year periods ending in 2001, 2004 and 2008, respectively. Source: INE, Demographic statistics, 2000 to 2008. The difference in life expectancy among the regions (NUTS II) in Mainland Portugal is 1,39 years. Generally speaking, residents along the central coast have a higher life expectancy at birth than Application for the 2010 SCML Award 29 Results 1 those living in the interior and in NUTS III regions further to the north and to the south of the country, with a maximum difference of 2,89 years. Figure 3 Life expectancy at birth in 2006‐2008 by place of residence Source: INE, 2010 Summary In 2008: • Birth rate: 9,8 per 1000 population; • Death rate: 9,8 per 1000 population; • Migration growth rate: 0,9 per 1000 population. • Life expectancy: 78,90 years 75,68 for males 81,94 for females Application for the 2010 SCML Award 30 Results 1 4.1.2. Comparative analysis of death rates in 2000, 2004 and 2008 Gender and age group To account for the uncertainty that arises from the natural variation inherent in the biological and random processes governing the occurrence of events as deaths and illnesses, 95% confidence intervals were computed for death rates. Confidence intervals were used as a test of significance when comparing two death rates, since if respective confidence intervals do not overlap, a comparable statistical test would always indicate a statistically significant difference. That was the case for all of death rates discussed below (see Annex 3). The relative change in the number of deaths among the population ages 15 and up, living in Mainland Portugal, was not very important: ‐0,2%, resulting from a decrease from 99025 deaths in 2000 to 98840 deaths in 2008. In the same period, the death rate dropped from 12,1 to 11,5 deaths per 1000 population. The death rate for males was slightly higher than for females. For men, it decreased from 13,2‰ in 2000 to 12,3‰ in 2008 (relative decrease of 6,5%) and for women, it edged lower, from 11,1‰ to 10,7‰ (relative decrease of 3,0%). As can be expected, age‐specific death rates rose systematically with age. Over the period from 2000 to 2008, there was a decline for all ages. Relative decrease was higher in lower age groups: around 50% for young people ages 15 to 24, and 33% for the 25‐44 age group. For the younger population (ages 15‐24) the rate was less than 1 death per 1000 population throughout the period from 2000 to 2008, and both the number of deaths and the death rate in 2008 were about half the figures achieved in 2000. In 2008 there were 476 deaths of young people ages 15 to 24, with the death rate at 0,4‰. In the 25‐44 age group, between 2000 and 2008, the death rate dropped from 1,7‰ to 1,1‰. For the population ages 45 to 64, there was a relative decrease of 14,1%, as it dropped from 5,9‰ in 2000 to 5,1‰. In the age group above this (ages 65‐74), the relative decrease was more noteworthy: 22%, resulting from a decline from 21,8‰ in 2000 to 17,0‰ in 2008. Application for the 2010 SCML Award 31 Results 1 Figure 4 Death rate1 by age group 200,0 150,0 100,0 50,0 0,0 15 ‐ 24 25 ‐ 44 45 ‐ 64 2000 65 ‐ 74 2004 75 ‐ 84 85+ 2008 1 Death rate per 1000 population. Source: INE, 2010 The number of deaths among the population ages 75 and up rose between 2000 and 2008: from 32675 to 34366 (+5,2%) for the 75‐84 age group, and from 26197 to 30894 (+17,9%) for the elderly ages 85 and up. Despite the increase in the absolute number of deaths during this period, there was a decrease in the death rate. This is because are increasingly more people in the age groups in question, as a result of the population’s greater longevity. Thus, from 2000 to 2008, the death rate for people ages 75 to 84 dropped from 63,5‰ to 52,7‰ (‐17,0%) and for people ages 85 and up, from 185,7‰ to 174,5‰ (‐6,0%). Table 4 Death rate by gender and age group 2000 Total Pop Death (x10 3) 8198 99025 Gender: M F 3911 4287 2004 12,1 Pop Death (x10 3) 8463 96249 51619 47406 13,2 11,1 4049 4414 Age‐group: 15 ‐ 24 years 1403 1135 25 ‐ 44 years 2880 4820 45 ‐ 64 years 2321 13718 65 ‐ 74 years 938 20480 75 ‐ 84 years 515 32675 85 and up 141 26197 1 Death rate per 1000 population. Source: INE, 2010. 0,8 1,7 5,9 21,8 63,5 185,7 1267 3035 2447 978 588 148 DR 1 2008 Variation 2000‐08 (%) DR 1 Pop Death DR 11,4 Pop Death (x10 3) 8595 98840 11,5 4,8 ‐0,2 ‐4,8 50109 46140 12,4 10,5 4115 4480 50798 48042 12,3 10,7 5,2 4,5 ‐1,6 1,3 ‐6,5 ‐3,0 704 4217 13068 18551 33621 26088 0,6 1,4 5,3 19,0 57,2 176,6 1150 3052 2594 970 652 177 476 3420 13164 16520 34366 30894 0,4 1,1 5,1 17,0 52,7 174,5 ‐18,0 6,0 11,8 3,4 26,7 25,5 ‐58,1 ‐29,0 ‐4,0 ‐19,3 5,2 17,9 ‐48,8 ‐33,0 ‐14,1 ‐22,0 ‐17,0 ‐6,0 DR 1 Application for the 2010 SCML Award 32 Results 1 The death rate is higher in the male than in the female population in every age group (Annex 4). For younger people (ages 15‐24) the relative decreases in the number of deaths and of the death rate between 2000 and 2008 were higher for boys (60,8% and 52,4%, respectively) than for girls (48,8% and 37,3%); however, the low levels achieved for females should be pointed out: from 0,4 deaths to 0,2 deaths per 1000 girls ages 15 to 24. In the 25‐44 age group, the death rate for men dropped from 2,5‰ to 1,6‰ (‐6,1%). The death rate for the female population decreased 25,5%, while remaining below 1 death per 1000 women throughout the entire period. For the population ages 45 to 64, however, relative decreases were more significant for females (‐10,9% for the number of deaths and ‐19,6% for the death rate). The number deaths for men ages 45‐64 dropped from 9100 in 2000 to 8826 in 2004, but once again rose to 9048 in 2008 (‐0,6% from 2000 to 2008). The death rate decreased 11,8%, as it slipped from 8,2‰ to 7,3‰. The disparity between death rates in male and females in the 65‐74 age group remains high (around double), both for the number of deaths and for the death rate. In 2008, there were around 24 deaths per 1000 men and 12 per 1000 women. For the population ages 75 and up, the disparity between genders lessens. Figure 5 Death rate1 by gender and age group (ages 65 and up) 250 200 150 100 50 0 M F M 65 ‐ 74 75 ‐ 84 2000 1 F Death rate per 1000 population. Source: INE, 2010 2004 M F 85+ 2008 Application for the 2010 SCML Award 33 Results 1 Place of residence The death rate is higher in Regions with an aging population; therefore, to compare the five Regions (with very diverse age structures) or the same Region over several years, age‐ standardized death rates (SDR) were calculated (direct standardizing method) and the population of Mainland Portugal was used as a standard. Figure 6 Age‐standardized death rate1 by place of residence 15,0 12,5 10,0 7,5 5,0 2,5 0,0 Norte Centro 2000 1 Death rate per 1000 population. Source: INE, 2010 LVT 2004 Alentejo Algarve 2008 From 2000 to 2008, there was population growth in every Region except in the Alentejo, where the number of residents over age 15 decreased 2,0%. The Region of the Algarve had the biggest population increase: 12,1%, during the same period. The number of deaths in 2008 remained close to the figure for the year 2000 in the Norte, Centro and Alentejo Regions, while it dropped in LVT (Lisboa e Vale do Tejo) (‐1,6%), but rose in the Algarve (4,3%). During the period from 2000 to 2008, the SDR decreased more sharply in the Norte and LVT Regions (5,8% and 7,7%, respectively). Only in the Alentejo was there an increase in the rate (2,9%), which reflects a decreasing population, since the number of deaths remained stable. It should be noted that, in this Region, the change from 2000 to 2004 had been favourable, with the SDR dropping from 12,5 to 11,7 deaths per 1000 population. In 2008, the SDR increased again, to 12,8‰. Application for the 2010 SCML Award 34 Results 1 Table 5 Age‐standardized death rate by place of residence 2000 Total 2004 2008 Pop Pop Death SDR 1 Death SDR 1 (x10 3) (x10 3) 8199 99025 12,1 8463 96249 11,4 Place of residence: Norte 2991 31066 11,9 Centro 1491 20318 11,6 LVT 2940 35594 12,4 Alentejo 453 7509 12,5 Algarve 324 4538 12,5 1 Death rate per 1000 population. Source: INE, 2010. Pop Death (x10 3) 8595 98840 Variation 2000‐08 (%) SDR 1 Pop Death SDR 11,5 4,8 ‐0,2 ‐4,8 3096 1530 3036 453 348 30542 19894 34105 7048 4660 11,2 11,2 11,4 11,7 12,3 3157 1542 3090 444 363 31238 20319 35035 7515 4733 11,2 11,5 11,4 12,8 12,2 5,5 3,4 5,1 ‐2,0 12,1 0,6 0,0 ‐1,6 0,1 4,3 ‐5,8 ‐1,3 ‐7,7 2,9 ‐1,8 To compare regional standardized rates to national one, it was used the Comparative Mortality Index (CMI), which is a measure of relative risk of death linked to the application of the direct method. For Mainland Portugal, the CMI assumes a figure of 100%. Statistical testing was conducted, assuming as a null hypothesis the equality between SDR of the Region in question and the SDR for Mainland Portugal, that is, H0: CMIRegion = 100%, and as an alternative hypothesis Ha: CMIRegion ≠ 100%. The Regions whose relative risk of death is significantly below the national figure were Centro in 2000 and Norte in 2008. The LVT (year 2000), Algarve (year 2004) and Alentejo (year 2008) Regions had a higher relative risk of death. Table 6 Comparative Mortality Index by place of residence 2000 1 2004 1 2008 1 SDR CMI p‐value SDR CMI p‐value SDR CMI p‐value 12,1 100,0 ‐‐‐‐‐ 11,4 100,0 ‐‐‐‐‐ 11,5 100,0 ‐‐‐‐‐ Place of residence: Norte 11,9 Centro 11,6 LVT 12,4 Alentejo 12,5 Algarve 12,5 1 Death rate per 1000 population. Source: INE, 2010 98,2 96,4 102,6 103,3 103,3 0,16 0,02 0,04 0,25 0,37 11,2 11,2 11,4 11,7 12,3 98,5 98,7 100,3 103,2 108,0 0,26 0,42 0,78 0,27 0,03 11,2 11,5 11,4 12,8 12,2 97,2 100,0 99,5 111,6 106,5 0,02 0,98 0,68 0,00 0,08 Total Marital status In the years being examined, the percentage of deaths for married (45%) and widowed individuals remained stable (39%). The number of deaths for divorced or legally separated individuals increased 40,0% during this period (from 2866 to 4011 deaths), thus accounting for Application for the 2010 SCML Award 35 Results 1 4,1% of deaths in 2008. The opposite trend occurred with deaths for single individuals, whose percentage declined from 13,4% in 2000 to 11,9% in 2008. Figure 7 Percentage of deaths in 2008 by marital status 4,1 11,9 45,2 38,6 Married Widower Single Divorced Source: INE, 2010 An explanation for the increasing number of deaths in divorced individuals could be the increase of this population. The crude divorce rate in Mainland Portugal went from 1,9 to 2,4 divorces per 1000 population, from 2000 to 2008. On the contrary, the crude marriage rate has been on the decline. In the period being examined, it decreased from 6,2 to 4,0 marriages per 1000 population. This situation, combined with a sharp drop in the death rate among younger population groups, could contribute toward a decrease in the number of deaths for single people. Table 7 Percentage of deaths by marital status 2000 2004 2008 Variation 2000‐08 (%) Death % Death % Death % Death % Total 99025 100,0 96249 100,0 98840 100,0 ‐0,2 0,0 Marital status: Single Married Divorced Widower Unknown Source: INE, 2010. 13300 44070 2866 38789 0 13,4 44,5 2,9 39,2 0,0 11924 42813 3296 37832 384 12,4 44,5 3,4 39,3 0,4 11741 44688 4011 38128 272 11,9 45,2 4,1 38,6 0,3 ‐11,7 1,4 40,0 ‐1,7 n. apl. ‐11,6 1,6 40,2 ‐1,5 n. apl. Considering male and female population separately (Annex 5), can be noticed that the percentage of deaths of single individuals is similar (M: 11,7% and F: 12,1%), unlike what is Application for the 2010 SCML Award 36 Results 1 noticed in the case of deaths among married and widowed individuals. Of the total number of deceased males in 2008, 62,3% were married. For the female population, the percentage was 27,1%. Widowed individuals accounted for 21,1% among males and 57,0% among females. Figure 8 Percentage of deaths in 2008 by gender, marital status and age group 100,0 80,0 60,0 40,0 20,0 0,0 H M H 55 a 64 Single M H 65 a 74 Married Divorced M 75+ Widower Source: INE, 2010 The difference in the distribution pattern of marital status of the deceased in each age group, depends on gender, becomes sharper for ages 55 and up, with particular emphasis on the population ages 75 and up. In this age group, deceased individuals who were married accounted for 59,4% for males and 18,6% for females. For widowed individuals, the percentages were 32,7% (men) and 67,9% (women). Information regarding the stratification of the Portuguese population by marital status is obtained through general population censuses conducted every ten years. As there are available census information for 2001 and provisional estimates of the resident population by marital status for the year 2003, that information was used to calculate death rates by marital status of the deceased, for 2000 and 2004. These concern the resident population in Portugal, since there are no available estimates for Mainland Portugal. Were used age‐standardized death rates, to remove differences in the age composition of the various population subgroups (single, married, divorced or widowed individuals). The population of Portugal was used as a standard. Comparative Mortality Index, as described previously, was also computed (Annex 5). Application for the 2010 SCML Award 37 Results 1 Table 8 Age‐standardized death rate by marital status 2000 3 Total 2004 1 3 Variation 2000‐04 (%) 1 Pop (x10 ) Death SDR Pop (x10 ) Death SDR Pop Death SDR 8689 104262 12,0 8826 100828 11,6 1,6 ‐3,3 ‐3,6 Marital status: Single 2204 14130 19,8 2208 12687 19,2 0,2 ‐10,2 ‐3,0 Married 5587 46435 9,0 5644 45033 8,7 1,0 ‐3,0 ‐3,7 Divorced 222 2985 16,4 292 3419 16,2 31,7 14,5 ‐1,7 Widower 677 40712 18,2 682 39689 16,3 0,8 ‐2,5 ‐10,6 1 Death rate per 1000 population ages 15 and up, residing in Portugal. To calculate the rate for the year 2000, it was used information collected in the 2001 Census; for the year 2004, it was used provisional estimates of the resident population by marital status in 2003. Source: INE, 2010. Relative risk of death was significantly lower among married individuals (around 25% below risk of death for total population, in 2000 and 2004). For single, divorced or widowed population, CMI for 2004 were as follows: 165,9%, 139,7% e 140,8%, respectively. All these values are significantly above total population’s risk of death (Annex 5). Table 9 Comparative Mortality Index by marital status 2000 1 2004 1 SDR CMI p‐value SDR CMI p‐value Total 12,0 100,0 ‐‐‐‐‐ 11,6 100,0 ‐‐‐‐‐ Marital status: Single Married Divorced 19,8 9,0 16,4 164,8 75,4 137,0 <0,0001 <0,0001 <0,0001 19,2 8,7 16,2 165,9 75,3 139,7 <0,0001 <0,0001 <0,0001 Widower 18,2 151,7 0,0022 16,3 140,8 0,0193 1 Death rate per 1000 population ages 15 and up, residing in Portugal. To calculate the rate for the year 2000, it was used information collected in the 2001 Census; for the year 2004, it was used provisional estimates of the resident population by marital status in 2003. Source: INE, 2010. Occupation and status at work In the year 2000, 61,2% of the population ages 15 and up living in Mainland Portugal was active in the job market; the non‐active population (students, domestic or retired individuals) reached 38,7%. 0,1% of the population was doing mandatory military service (Annex 6). In 2008, the percentage of active individuals had increased to 62,6% (relative growth: 2,3%). At the same time, there was drop in the percentage of the population whose status is inactive, to 37,4%. It Application for the 2010 SCML Award 38 Results 1 should also be noted that, from 2000 to 2008, the percentage of unemployed individuals went from 4,0% to 7,7% of the active population. As examining the work status for individuals who died from 2000 to 2008, it was noticed that, during the period in question, some 90% were non‐active and 82,3% (in 2008) were 65 or over (Annex 7) Figure 9 Percentage of deaths in 2008 by work status 6,9% 3,2% 7,6% 89,2% 82,3% Employed Unemployed Non active ‐ 15 to 64 years Non active ‐ 65 and up Source: INE, 2010 Death rate is significantly higher among non‐active than active population. In 2008 the values were 27,4‰ vs. 1,5‰, with p<0,05 (Annex 8). The death rate among the non‐active population edged lower, from 28,2‰ in 2000 to 27,4‰ in 2008 (‐3,0%), not only because of the slight drop in the number of deaths but also due to an increase in the number of non‐active individuals. For the active population, there was also a downward trend, with a decline from 1,9‰ to 1,5‰, from 2000 to 2008 (‐23,6%). When looking at the active population, considering the subgroup of employed individuals, it was noticed a drop in the mortality from 2000 to 2008: from 1,9 to 1,5 deaths per 1000 employed individuals (relative decrease: 21,9%). Application for the 2010 SCML Award 39 Results 1 Table 10 Death rate by work status 2000 Total Pop Death (x10 3) 8198 99025 2004 DR 1 12,1 Pop Death (x10 3) 8463 96249 2008 DR 1 11,4 Pop Death (x10 3) 8595 98840 Variation 2000‐08 (%) DR 1 Pop Death DR 11,5 4,8 ‐0,2 ‐4,8 Work status: Active 5017 9538 1,9 5262 8395 1,6 5381 7821 1,5 7,3 ‐18,0 Employed 4817 9339 1,9 4904 8229 1,7 4968 7521 1,5 3,1 ‐19,5 Unemployed 200 199 1,0 358 166 0,5 413 300 0,7 106,7 50,8 Looking 26 61 2,3 48 49 1,0 56 17 0,3 115,4 ‐72,1 for 1st job Looking for a new 174 138 0,8 310 117 0,4 357 283 0,8 105,2 105,1 job Non‐active 3169 89487 28,2 3204 87854 27,4 3216 88147 27,4 1,5 ‐1,5 1 Death rate per 1000 population. Note: The sum of the population of the various modalities shown for the variable ‘Work status’ is less than the total population, due to the existence of individuals doing their mandatory military service (12.000 in 2000 and 5.000 in 2004). The sum of deaths in the various modalities shows for the variable ‘Work status’ is less than the total number of deaths, due to the existence of cases where the work status of the deceased is unknown. Source: INE, 2010. For employed population death rates and respective 95% confidence intervals were computed (Annex 9), according with occupational situation and occupation. Differences between death rates obtained were significant at the 0,05 level. Taking into account the occupational situation, it was noticed that the death rate is particularly low among self‐employed individuals as employers: 0,4‰ in 2000 and 0,2‰ in 2008. However, in 2008, the employer deaths accounted for only 0,6% of the 7520 deaths that occurred among the employed population (Annex 11). For self‐employed people, it was obtained a death rate of 1,9‰ in 2000, which dropped to 1,3‰ in 2008. Slightly higher figures were obtained for dependent workers, with a continued decreasing trend over the course of the period (2,2‰ in 2000 and 1,5‰ in 2008). The deaths of dependent workers, in 2008, accounted for 74,1% of the total deaths of the employed population. Application for the 2010 SCML Award 40 ‐23,6 ‐21,9 ‐27,0 ‐87,1 0,0 ‐3,0 Results 1 Table 11 Death rate by occupational situation and occupation – average employed population Total Occupational situation: Employer Dependent worker Self‐employed 2000 Pop Death (x10 3) 4817 9339 DR 1 1,9 2004 Pop Death (x10 3) 4904 8229 DR 1 1,7 2008 Pop Death (x10 3) 4968 7521 Variation 2000‐08 (%) DR 1 Pop Death DR 1,5 3,1 ‐19,5 ‐21,9 294 3494 841 111 7565 1614 0,4 2,2 1,9 321 3606 879 76 6445 1600 0,2 1,8 1,8 279 3763 878 48 5576 1179 0,2 1,5 1,3 ‐5,1 7,7 4,4 ‐56,8 ‐26,3 ‐27,0 ‐54,4 ‐31,6 ‐30,1 Occupation (Major groups CNP94)2: Armed forces 32 61 1,9 35 60 1,7 30 82 2,7 ‐4,4 34,4 occupations (0) Managers and Professionals (1 e 661 1457 2,2 871 1220 1,4 763 600 0,8 15,4 ‐58,8 2) Technicians and associate 366 519 1,4 405 313 0,8 462 479 1,0 26,2 ‐7,7 professionals (3) Clerical support, service and sales 1102 1611 1,5 1135 1303 1,1 1208 1054 0,9 9,7 ‐34,6 workers (4 e 5) Skilled agricultural, forestry and 528 831 1,6 538 705 1,3 539 266 0,5 2,1 ‐68,0 fishery workers (6) Craft and related trades workers, 1473 3987 2,7 1333 3377 2,5 1342 2471 1,8 ‐8,9 ‐38,0 operators and assemblers (7 e 8) Elementary 657 718 1,1 588 1185 2,0 624 1901 3,0 ‐4,9 164,8 occupations (9) 1 2 Death rate per 1000 inhabitants. Major groups in the National Classification of Occupations for 1994: Annex 10 Note: The sum of all deaths in the different modalities presented, for each of the variables ‘Situation in ones occupation’ and ‘Occupation’, is less than the total deaths due to the fact that there are cases in which the situation in ones occupation and the occupation of the deceased is unknown. Source: INE, 2010. Considering the occupation of each individual, over half the deaths (50,4% in 2000 and 58,1% in 2008) occurred in less differentiated work groups: labourers and related employees, as well as unskilled workers. However, during the period from 2000 to 2008, the death rate decreased for labourers and related employees, but increased for unskilled workers. Besides this group, only among Armed Forces personnel were there an increase in the death rate. Application for the 2010 SCML Award 41 40,7 ‐64,3 ‐26,9 ‐40,3 ‐68,6 ‐32,0 178,5 Results 1 Figure 10 Percentage of deaths in 2008 by occupation 100% Elementary occupations Craft and similar workers 75% Skilled workers A&F 50% Service workers Technicians 25% Managers and Professionals 0% 2000 AF occupations 2008 Source: INE, 2010 Despite the drop in the number of Armed Forces personnel (‐4,4%, from 2000 to 2008), the number of deaths rose from around 60 in 2000 and 2004 to 82 in 2008, thus resulting in a relative increase of 40,7% in the death rate, in this work group (from 1,9‰ to 2,7‰). As can be seen in table (Annex 11), 95% confidence intervals around these rates overlap, so the difference between 2000 and 2008 death rates can be significant or not. In accordance, a statistical test for the difference of rates was performed, admitting that variance remained constant in this period. Null hypothesis (rate’s difference equals zero) was rejected at 0,05 level. Figure 11 Death rate1 by occupation – average employed population 4,0 3,0 2,0 1,0 2000 1 Death rate per 1000 population. Source: INE, 2010 2004 Elementary occupations Craft and similar workers Skilled workers A&F Service workers Technicians Managers and Professionals AF occupations 0,0 2008 Application for the 2010 SCML Award 42 Results 1 The increase in the death rate was also noticeable among unskilled workers, for which there were 718 deaths in 2000 and 1901 in 2008. This increase, combined with a slight drop in the number of workers in this work group, resulted in an increase from 1,1‰ to 3,0‰, from the years 2000 to 2008. All the other work groups experienced the opposite trend for the death rate, which decreased throughout the period being studied. Nationality In order to study the mortality of foreign citizens residing in Portugal and that died within national territory, the death rates standardised by age were calculated, for a group of the most representative countries. As standard population it was chosen the population with Portuguese nationality residing in Portugal. It was obtained the Comparative Mortality Index and performed the statistical tests as described above. The analysis was only made for the years 2004 and 2008, as it was not possible to access the data for foreign population residing in Portugal in 2000 broken down by age group. Table 12 Mortality by nationality (Continents) 2004 2008 Pop Death SDR 1 CMI p‐value Pop Death SDR 1 CMI p‐value Total of residents 8 853 756 101 251 12,6 100,1 0,87 8 996 492 103 685 11,9 100,2 0,77 Nationality: Europe 8 704 698 100 563 12,6 100,0 0,97 8 757 478 102 860 11,9 100,0 Portugal 8 633 022 100 072 12,6 100,0 ‐‐‐‐‐ 8 610 260 102 256 11,9 100,0 Others UE 66 079 362 9,1 72,6 0,00 75 659 497 13,3 112,2 Others non UE 5 597 129 33,6 267,0 0,34 71 559 107 8,3 69,8 Africa 99 953 499 14,0 111,1 0,50 110 378 607 16,6 139,5 America 37 865 142 8,9 70,4 0,03 104 029 177 13,9 116,7 Asia 10 515 26 6,3 49,8 0,01 24 287 36 7,9 66,3 Oceania 468 2 34,8 276,4 0,87 241 1 4,6 39,0 Unknown 257 19 584,9 4647,6 0,89 79 4 44,7 376,7 1 Death rate per 1000 inhabitants. Source: INE and Foreigners and Border Control Authority, 2010. 1,00 ‐‐‐‐‐ 0,37 0,40 0,05 0,64 0,31 0,29 0,76 The SDR (Standardised Death rate) varies widely both in 2004 as well as in 2008, according to ones nationality. However, as the number of foreign citizens that die in Portugal is relatively small, only in some cases there is enough statistical evidence to reject the null hypothesis (CMI for that country different from 100%). In 2004 the relative death risk was significantly lower than that of the Portuguese for citizens of other countries of the European Union and of American Application for the 2010 SCML Award 43 Results 1 and Asian continents, as well as for citizens from Spain, United Kingdom and USA. In 2008, that was the case for citizens from the Netherlands, Moldavia, Ukraine and China. Table 13 Mortality by nationality (Europe) Europe Nationality: Portugal Others UE Germany Belgium Spain France Italy Netherlands United Kingdom Romania Pop Death 8704698 100563 2004 SDR 1 12,6 CMI 100,0 8633022 100072 12,6 100,0 ‐‐‐‐‐ 9,1 8,8 7,0 7,7 25,9 9,9 8,1 8,1 124,3 72,6 70,3 56,0 61,0 205,7 78,4 64,8 64,0 987,9 0,00 0,20 0,23 0,00 0,45 0,58 0,23 0,00 0,83 66079 11244 2151 14126 7388 4148 4618 15744 1021 362 52 8 82 32 19 23 101 18 p‐value Pop Death 0,97 8757478 102860 8610260 102256 75659 7580 1437 6870 4171 3709 3961 14346 22992 497 92 14 79 39 22 24 174 24 2008 SDR 1 11,9 CMI 100,0 p‐value 1,00 11,9 100,0 ‐‐‐‐‐ 13,3 19,2 10,7 13,8 19,3 16,6 6,3 12,4 14,9 112,2 161,4 90,4 116,3 162,4 140,0 53,0 104,0 125,6 0,37 0,30 0,86 0,62 0,45 0,64 0,02 0,84 0,91 Others non UE 5597 129 33,6 267,0 0,34 71559 107 8,3 69,8 0,40 Moldavia 813 10 14,2 113,1 0,90 17527 12 0,5 4,2 0,00 Russia 1009 12 32,2 256,0 0,80 5448 6 14,0 117,8 0,93 Switzerland 845 6 18,8 149,5 0,79 959 7 7,3 61,1 0,38 Ukraine 1199 92 117,3 932,1 0,81 45615 72 2,3 19,3 0,00 1 Death rate per 1000 inhabitants. Note: This table does not include the countries for which 0 to 6 cases of citizens from those nationalities dies in Mainland Portugal. The countries and number of deaths in each year (2000/2004/2008) are: Austria (2/1/2), Bulgaria (0/6/3), Denmark (3/6/3), Finland (2/3/3), Greece (1/0/1), Hungary (1/1/0), Ireland (1/3/5), Latvia (0/1/0), Lithuania (0/2/1), Luxemburg (1/0/1), Poland (0/0/1), Czech Rep. (1/0/0), Sweden (5/3/6), Albania (1/0/2), Former Yugoslavian Rep. of Macedonia (0/0/1), Byelorussia (0/1/0), Croatia (0/1/1), Georgia (0/2/5), Monaco (1/0/0), Norway (3/4/1) and Turkey (1/0/0). Source: INE and Foreigners and Border Control Authority, 2010. Table 14 Mortality by nationality (Africa) Africa 2004 Pop Death SDR 1 CMI p‐value 99 953 499 14,0 111,1 0,50 2008 Pop Death SDR 1 CMI p‐value 110 378 607 16,6 139,5 0,05 Nationality: Angola 21 067 107 22,0 175,1 0,26 24 084 137 25,2 212,4 0,17 Cape Verde 45 995 234 10,6 84,5 0,32 44 386 278 14,1 118,9 0,37 Guinea‐Bissau 16 388 77 13,6 108,4 0,89 21 141 69 14,6 123,2 0,78 Mozambique 4 614 31 19,7 156,9 0,55 3 104 39 31,2 262,4 0,38 S. Tome and Príncipe 5 917 33 20,5 162,9 0,56 9 559 45 15,5 130,3 0,66 1 Death rate per 1000 inhabitants. Note: Countries with <7 cases (2000/2004/2008): South Africa (1/2/2), Algeria (1/0/1), Central‐African Rep. (1/0/0), Democratic Rep. of Congo (5/4/0), Gambia (0/1/0), Ghana (0/0/1), Gibraltar (1/0/0), Equatorial Guinea (1/1/0), Lesotho (0/0/1), Madagascar (0/0/1), Morocco (1/4/2), Nigeria (0/1/1), Kenya (1/0/0), Senegal (1/1/1), Togo (0/0/1), Tunisia (0/0/1) and Zimbabwe (1/1/2). Source: INE and Foreigners and Border Control Authority, 2010. Application for the 2010 SCML Award 44 Results 1 Table 15 Mortality by nationality (America) America Pop 37 865 Death 142 2004 SDR 1 8,9 CMI 70,4 p‐value 0,03 Pop 104 029 Death 177 2008 SDR 1 13,9 CMI 116,7 p‐value 0,64 Nationality: Brazil 25 131 106 12,5 99,5 0,99 95 870 142 18,4 155,3 0,48 EUA 6 163 21 4,2 33,1 0,00 2 053 15 8,2 69,3 0,37 1 Death rate per 1000 inhabitants. Note: Countries with <7 cases (2000/2004/2008): Canada (0/5/2), Mexico (0/0/1), Cuba (0/0/1), Panama (1/0/0), Argentina (2/1/3), Bolivia (0/0/1), Chile (0/0/1), Colombia (0/1/1), Ecuador (0/1/1), Peru (1/0/0), Uruguay (0/1/0) and Venezuela (1/2/6). Source: INE and Foreigners and Border Control Authority, 2010. Table 16 Mortality by nationality (Asia) Asia Pop 10 515 Death 26 2004 SDR 1 6,3 CMI 49,8 p‐value 0,01 Pop 24 287 Death 36 2008 SDR 1 7,9 CMI 66,3 p‐value 0,31 Nationality: China 4 202 7 6,6 52,4 0,39 10 612 4 0,8 7,0 0,00 India 1 565 6 8,7 69,4 0,58 5 030 16 19,7 165,6 0,72 1 Death rate per 1000 inhabitants. Note: Countries with <7 cases (2000/2004/2008): Bangladesh (2/1/3), Kazakhstan (0/3/2), Rep. of Korea (1/1/0), Philippines (1/0/1), Indonesia (2/1/0), Islamic Rep. of Iran (0/1/1), Japan (0/3/0), Pakistan (3/1/5), Singapore (0/1/0), East Timor (0/0/3), Turkmenistan (1/0/0) and Uzbekistan (0/1/1). Source: INE and Foreigners and Border Control Authority, 2010. Figure 12 Foreign population residing in Portugal in 2008, by nationality Source: INE and Foreigners and Border Control Authority, 2010 Application for the 2010 SCML Award 45 Results 1 Figure 13 Deaths among foreign population residing in Portugal in 2008, by nationality Source: INE and Foreigners and Border Control Authority, 2010 Place where the death occurred More than half of the deaths occurred in a hospital/clinic and the percentage has been increasing: from 54.2% in 2000 to 61.4% in 2008 (relative increase of: 13.3%). On the other hand, the percentage of deaths which occurred at home, which include all those which took place in private (even if not at the home of the deceased), collective and similar lodgings, such as nursing and residential homes, decreased from 35.8% in 2000 to 29.9% in 2008 (‐16.5%). In 2000, 10% of the deaths did not take place in a hospital/clinic, nor at a home. The percentage of these occurrences dropped to 8.7% in 2004, and the value remained the same in 2008. Table 17 Percentage of deaths by place of death 2000 2004 2008 Variation 2000‐08 (%) Death % Death % Death % Death % Total 99025 100,0 96249 100,0 98840 100,0 ‐0,2 0,0 Place of death: Hospital/clinic At home At public places Source: INE, 2010. 53636 35496 9893 54,2 35,8 10,0 55957 31897 8395 58,1 33,1 8,7 60692 29518 8630 61,4 29,9 8,7 13,2 ‐16,8 ‐12,8 13,3 ‐16,5 ‐13,0 Application for the 2010 SCML Award 46 Results 1 Figure 14 Percentage of deaths by place of death 70,0 60,0 50,0 40,0 30,0 20,0 10,0 0,0 Hospital/clinic At home 2000 2004 At public places 2008 Source: INE, 2010. Cause of death In order to register a death at the Civil Registry Office, it is mandatory that, among all information gathered, the cause of death is indicated. Regarding the deaths recorded in 2008, in 90.4% of the occurrences the cause of death was mentioned only based upon clinical elements (Annex 12). In the same year, for 6.1% of the deaths, the cause of death was mentioned based on the autopsy and for 1.7% the basis for the indication was unknown. In the remaining cases written documents made by the administrative authorities or other official documents were mentioned. Figure 15 Percentage of deaths in 2008 by basis for indicating the cause of death Clinical elements 1,7 6,1 1,0 0,7 Autopsy Unknown Other official documents 90,4 Source: INE, 2010. Application for the 2010 SCML Award Written documents made by administrative authorities 47 Results 1 In 2000, for 5.9% of the total deaths, the cause of death was mentioned based on the autopsy, corresponding to 5803 cases. Out of these, 43.6% occurred at a hospital/clinic, 17.5% at a home and 39.0% in another place (Annex 13). In 2008 the percentage of deaths whose cause was given based on the autopsy was similar (6.1%; 6075 deaths). However, the percentage of those that occurred at home almost doubled, compared to what was observed in 2000, reaching 30.0%. On the other hand, there was a decrease in the percentage of deaths in which the cause of death was mentioned based on the autopsy and that occurred during the hospital stay (36.7%) and in another place (33.4%). Figure 16 Percentage of autopsies by place of death 50,0 40,0 30,0 20,0 10,0 0,0 Hospital/clinic At home 2000 Source: INE, 2010. At public places 2008 Overall the predominant causes of death of the adult Portuguese population are diseases of the circulatory system and cancer. During the period 2000‐08 there was a growing trend in the number of cancer as the cause of death: 20.6% of the total deaths in 2000 and 23.2% in 2008, greater than the population growth during the period under analysis and, consequently, the death rate due to this cause in 2008 was greater than what was observed in 2000 (respectively 266.6 and 248.7 deaths per 100 000 inhabitants aged 15 and above). Considering only screenable cancers, it can be seen a more unfavourable evolution for cancer of the colon, rectum and anus, responsible for 2.8% of the total deaths in 2000; 3.3% in 2004 and Application for the 2010 SCML Award 48 Results 1 3.6% in 2008. The respective death rate increased 20.9% in this period, reaching 41.2 per 100 000 population in 2008. The relative growth of the death rate caused by cancer of the cervix was less significant (5.7%). In 2008 there were 5.2 deaths per 100 000 women. In the same year the death rate due to malignant breast cancer was much higher (33.6 per 100 000 women). The main causes of death by diseases of the circulatory system (ischemic heart disease‐IHD and stroke), were jointly responsible for 28.8% of all deaths occurred in 2000. Contrary to what was seen regarding cancer, the relative importance of deaths by IHD and stroke has been decreasing, so in 2008 the proportional mortality due to these two causes had decreased to 21.6%. In that year the death rate was 162.8 deaths per 100 000 population for stroke and 84.9 for IHD. However, between 2000 and 2008 the relative decrease of the death rate was more relevant for stroke (‐33.9%) than for IHD (‐16.2%). Figure 17 Proportional mortality for main causes of death 25,0 20,0 15,0 10,0 5,0 0,0 Cancers Stroke 2000 Ischemic heart Respiratory diseaese system diseases 2004 Ill‐deffined causes 2008 Source: INE, 2010. Infectious and parasitic diseases caused 2.2% of the total deaths in 2000 and 2.5% in 2008, while the respective death rate increased from 26.0 to 29.2 deaths per 100 000 inhabitants. The percentage of deaths caused by diseases of the respiratory system also showed a positive trend: 9.6% in 2000 and 11.0% in 2008. The death rate rose from 116.4 to 126.3 deaths per 100 000 inhabitants. For these groups of diseases more favourable values were seen in 2004. Application for the 2010 SCML Award 49 Results 1 The number of deaths caused by Diabetes increased from 2928 in 2000 to 4139 in 2004, again decreasing slightly in 2008 (3990). Between 2000 and 2008 the death rate caused by Diabetes increased 30%, from 35.7 to 46.4 deaths per 100 000 inhabitants. Table 18 Death rate by cause of death 2000 (Pop=8 198 476) % 1 DR 2004 (Pop=8 462 951) Death % 1 DR 2008 (Pop=8 595 229) Death % 1 Death Total 99025 100,0 1207,8 96249 100,0 1137,3 98840 100,0 1149,9 DR Variation 2000‐08 (%) Death % DR ‐0,2 0,0 ‐4,8 Cause of death2: Infectious and parasitic diseases 2133 2,2 26,0 1938 2,0 22,9 2513 2,5 29,2 17,8 13,6 Cancers 20391 20,6 248,7 21309 22,1 251,8 22914 23,2 266,6 12,4 12,6 Screenable Colon, rectum and anus 2794 2,8 34,1 3140 3,3 37,1 3542 3,6 41,2 26,8 28,6 Female breast 1447 1,5 33,8 1349 1,4 30,6 1504 1,5 33,6 3,9 0,0 Cervix uteri 211 0,2 4,9 193 0,2 4,4 233 0,2 5,2 10,4 0,0 Diabetes mellitus 2928 3,0 35,7 4139 4,3 48,9 3990 4,0 46,4 36,3 33,3 Alcohol abuse 55 0,1 0,7 102 0,1 1,2 134 0,1 1,6 143,6 0,0 Ischemic heart diseases 8314 8,4 101,4 8296 8,6 98,0 7300 7,4 84,9 ‐12,2 ‐11,9 Stroke 20186 20,4 246,2 16126 16,8 190,5 13994 14,2 162,8 ‐30,7 ‐30,4 Diseases of the respiratory system 9546 9,6 116,4 8039 8,4 95,0 10857 11,0 126,3 13,7 14,6 Diseases of the digestive system 3836 3,9 46,8 4346 4,5 51,4 4297 4,3 50,0 12,0 10,3 Diseases of the skin and subcutaneous ‐ tissue 199 0,2 2,4 334 0,3 3,9 24 0,0 0,3 ‐87,9 100,0 Diseases of the musculoskeletal system/connective tissue 202 0,2 2,5 242 0,3 2,9 252 0,3 2,9 24,8 50,0 Diseases of the genitourinary system 1507 1,5 18,4 2331 2,4 27,5 2753 2,8 32,0 82,7 86,7 Symptoms, signs, abnormal findings, ill‐ defined causes 12435 12,6 151,7 9372 9,7 110,7 10523 10,6 122,4 ‐15,4 ‐15,9 External causes of injury and poisoning 4281 4,3 52,2 4919 5,1 58,1 4197 4,2 48,8 ‐2,0 ‐2,3 1 Death rate per 100 000 inhabitants aged 15 or above, except for female breast cancer and cervical cancer in which the death rate is per 100 000 women aged 15 or above. 2 CID 9 and CID 10 codes associated to each of the death causes: Annex 2. Source: INE, 2010. Mortality by external causes for population aged 15 and above decreased, both in absolute number of deaths (‐2.0%), as well as in terms of death rate (‐6.5%). The death rate, which had increased in 2000‐04 from 52.2 to 58.1 deaths per 100 000 inhabitants, showed a lower figure once again in 2008 (48.8 per 100 000 inhabitants). Application for the 2010 SCML Award 50 12,4 7,2 20,9 ‐0,5 5,7 30,0 132,4 ‐16,2 ‐33,9 8,5 6,8 ‐88,5 19,0 74,2 ‐19,3 ‐6,5 Results 1 Data quality The information on deaths sent to the INE [Statistics Portugal], based on the transcription of the death certificate by the Civil Registry Offices, is then subject to a set of validations and returned whenever any errors are detected. If required, the INE also carries out further contacts in order to clarify any doubts or request any missing information and only when the data quality control process is concluded, the final tables for periodical dissemination are prepared or whatever other specific calculations that are requested, such as those upon which this chapter is based. Table 19 Number and percentage of cases with unknown information by variable 2000 Total 2004 2008 N % N % N % 99025 ‐‐‐ 96249 ‐‐‐ 98840 ‐‐‐ Variable: Gender 0 0,0 0 0,0 0 0,0 Age group 0 0,0 0 0,0 0 0,0 Place of residence 0 0,0 0 0,0 0 0,0 Marital status 0 0,0 384 0,4 272 0,3 Work status 0 0,0 0 0,0 2872 2,9 Occupational situation 0 0,0 0 0,0 438 5,8 Occupation 0 0,0 0 0,0 668 8,9 Nationality 63 0,1 16 0,0 2 0,0 Cause of death 12435 12,6 9372 9,7 10523 10,6 Place of death 0 0,0 0 0,0 0 0,0 Notes: For the variables ‘Condition before ones job’, ‘Situation in ones occupation’ and ‘Occupation’ the type of answer ‘Doesn’t know/ doesn’t answer’ is only included in the calculations for 2008; for the variables ‘Situation in ones occupation’ and ‘Occupation’ the cases with unknown information only refer to employed population; for the variable ‘Cause of death’ it was considered as a case with unknown information when the death was classified as caused by ‘Symptoms, signals, abnormal exams, poorly defined causes’. Source: INE, 2010. As a consequence of the procedure described above, usually the percentage of missing information is just residual regarding deaths and regarding the social and economic characterisation of the deceased in analysed years. However, it should be mentioned that, for variables associated to the professional status, the modality of answer ‘Doesn’t know/doesn’t answer’ only appears in the tables for 2008. Thus, between 2004 and 2008, the percentage of cases with no information for the variables ‘Work status’, ‘Occupational situation’ and ‘Occupation’ grew from 0% to 2.9%, 5.8% and 8.9%, respectively. The tables for 2000 and 2004 are based on information registered on paper, through the death record in force, which does not include the option of not knowing the condition of the deceased for the variables at stake. Application for the 2010 SCML Award 51 Results 1 Regarding the variable ‘Cause of death’ the use of a non specific code for cause of death (Symptoms, signs, abnormal findings, ill‐defined causes) was considered an indicator for the quality of the information related to mortality by causes. The percentage of deaths to which this code was assigned decreased from 12.6% to 9.7% of the total deaths, between 2000 and 2004. However, in 2008 it reached 10.6%, a figure which was greater than that of 2004. Summary Change from 2000 to 2008 • Death rate in 2008: Decreased to 12,3‰ for males and to 10,7‰ for females; Decline for all ages; relative decrease higher in lower age groups: around 50% for young people ages 15 to 24. • Comparative Mortality Index: Regions whose relative risk of death is significantly below national figure: Centro in 2000 and Norte in 2008; Regions with relative risk of death significantly above: LVT (year 2000), Algarve (year 2004) and Alentejo (year 2008) Regions. Relative death risk significantly lower than that of the Portuguese for citizens from the Netherlands, Moldavia, Ukraine and China (2008). • Death rate significantly higher among non‐active than active population; • Over half the deaths occurred in less differentiated work groups: labourers and related employees, as well as unskilled workers; • 61.4% of the deaths occurred in a hospital/clinic; 29.9% occurred at home and 8.7% at public places, in 2008; • Predominant causes of death of the adult population: cancer (growing trend in 2000‐8) and diseases of the circulatory system (decreasing importance); • Death rate caused by Diabetes increased 30%, in this period; • Mortality by external causes decreased (48.8 per 100 000 inhabitants in 2008) • The proportion of ill‐defined causes of death is still high in Portugal and increased between 2004 and 2008, to 10.6%. Application for the 2010 SCML Award 52 Results 1 4.1.3. Potential Years of Life Lost by Cause of Death Ranking the causes of death is generally made by the number of deaths generated by each cause, not considering the age at which it occurs. This analysis should be complemented with the study of premature mortality (below the age of 70). In the indicator Potential Years of Life Lost (PYLL) the information related to the number of deaths is weighed by the age at the time of death, highlighting the causes that are responsible, simultaneously, for high mortality and for deaths at younger ages. Cancer is also predominant among causes of premature mortality, as well as in mortality for all ages. In 2000 they were responsible for 1231.8 PYLL per 100 000 inhabitants, which represented 22.0% of the PYLL for all causes. In 2008 that percentage reached 29.4%, despite the fact that the PYLL rate caused by cancer decreased slightly to 1212.6 per 100 000 inhabitants. Cancer of the colon, rectum and anus are responsible for greater number of deaths than malignant female breast cancer. However, considering the age when the death occurred, the order reverses. As female breast cancer is responsible for deaths in lower age groups, the PYLL rate is higher (224.4 per 100 000 inhabitants, in 2008) than in cancer of the colon, rectum and anus (127.2 per 100 000 inhabitants, in the same year). The importance of ischemic heart disease and of cerebrovascular diseases, as causes for premature mortality has been decreasing. In 2000, the number of years of life lost by ischemic disease represented 4.3% of the total PYLL, having decreased to 4.1% in 2008. For cerebrovascular diseases, in this period, the percentage dropped from 5.3% to 4.3% and the PYLL rate dropped from 298.8 to 177.9 per 100 000 inhabitants (a relative decrease of 40.5%). Several causes of death gain relevance in the analyses of premature mortality, although the respective death rate is much lower than those mentioned before. In 2008, the external causes and the group of those with undefined diagnosis which represent respectively 16.1 and 12.7% of the total number of Potential Years of Life Lost should be highlighted. Application for the 2010 SCML Award 53 Results 1 Table 20 Potential Years of Life Lost by cause of death 2000 (Pop=8 671 286) 2004 (Pop=8 820 122) 2008 (Pop=8 829 011) 1 1 1 PYLL Total 485762 % Rate PYLL % Rate PYLL % Variation 2000‐08 (%) Rate PYLL % Rate 100 5602,0 414438 100 4698,8 364211 100 4125,2 ‐25,0 0,0 ‐26,4 2 Cause of death : Infectious and 42689 8,8 492,3 31847 7,7 361,1 23576 6,5 267,0 ‐44,8 ‐26,3 ‐45,8 parasitic diseases 106811 22,0 1231,8 106083 25,6 1202,7 107062 29,4 1212,6 0,2 33,7 ‐1,6 Cancers Screenable Colon, rectum 9845 2,0 113,5 10608 2,6 120,3 11228 3,1 127,2 14,0 52,1 12,0 and anus 11050 2,3 251,3 9853 2,4 221,0 9990 2,7 224,4 ‐9,6 20,6 ‐10,7 Female breast 2400 0,5 27,7 2175 0,5 24,7 2553 0,7 28,9 6,4 41,8 4,5 Cervix uteri 5123 1,1 59,1 6832 1,6 77,5 5145 1,4 58,3 0,4 34,0 ‐1,4 Diabetes mellitus 778 0,2 9,0 1423 0,3 16,1 1793 0,5 20,3 130,5 207,5 126,4 Alcohol abuse Ischemic heart 20885 4,3 240,9 22267 5,4 252,5 14975 4,1 169,6 ‐28,3 ‐4,4 ‐29,6 diseases 25909 5,3 298,8 20701 5,0 234,7 15707 4,3 177,9 ‐39,4 ‐19,1 ‐40,5 Stroke Diseases of the 16965 3,5 195,6 13601 3,3 154,2 12297 3,4 139,3 ‐27,5 ‐3,3 ‐28,8 respiratory system Diseases of the 24851 5,1 286,6 27199 6,6 308,4 21787 6,0 246,8 ‐12,3 16,9 ‐13,9 digestive system Diseases of the skin and subcutaneous 258 0,1 3,0 510 0,1 5,8 45 0,0 0,5 ‐82,5 ‐76,7 ‐82,8 tissue Diseases of the musculoskeletal 1255 0,3 14,5 1514 0,4 17,2 1203 0,3 13,6 ‐4,2 27,8 ‐5,9 system/connective tissue Diseases of the 3247 0,7 37,4 4007 1,0 45,4 3015 0,8 34,1 ‐7,1 23,8 ‐8,8 genitourinary system Symptoms, signs, abnormal findings, ill‐ 84971 17,5 979,9 23673 5,7 268,4 46216 12,7 523,5 ‐45,6 ‐27,5 ‐46,6 defined causes External causes of 87269 18,0 1007,3 93007 22,4 1054,5 58511 16,1 662,7 ‐33,0 ‐10,6 ‐34,2 injury and poisoning 1 Rate of Potential Years of Life Lost per 100 000 inhabitants below 70, except for female breast cancer and cervical cancer for which the rate is per 100 000 women below 70. 2 CID 9 and CID 10 codes associated to each of the death causes: Annex 2 Source: INE, 2010. Globally, there was a decrease in premature mortality between 2000 and 2008. The relative decrease of the rate of Potential Years of Life Lost by all causes of death was 26.4%. However, in the case of deaths by cancer, during the same period, there was a gain of only 1.6%. Among screenable cancers, premature mortality decreased for female breast cancers: the PYLL rate which had reached 251.3 in 2000 came down to 224.4 years per 100 000 women in 2008 (‐ 10.7%). For cervix, rectum, anus and colon cancers the opposite trend was observed, with an increase of the PYLL rate (4.5% and 12.0%, respectively). Application for the 2010 SCML Award 54 Results 1 Between 2000 and 2004 the evolution of premature mortality by Diabetes mellitus was unfavourable. The PYLL rate went up from 59.1 to 77.5 years per 100 000 inhabitants. From 2004 to 2008 this trend reversed and the PYLL rate dropped to 58.3 per 100 000 inhabitants. Ischemic heart disease and cerebrovascular diseases have contributed towards the reduction of premature mortality. The PYLL rate attributed to these causes decreased 29.6% and 40.5%, respectively, during the period 2000‐08. Diseases associated to alcohol abuse were responsible for more premature deaths in 2008 than in 2000. The PYLL rate went up from 9.0 to 20.3 years per 100 000 inhabitants, which corresponds to a relative increase of 126.4%, between 2000 and 2008. Figure 18 Variation 2000‐08 (%) in the rate of Potential Years of Life Lost by cause of death Infectious and parasitic diseases Cancers Colon, rectum and anus Female breast Cervix uteri Diabetes mellitus Alcohol abuse Ischemic heart diseases Stroke Diseases of the respiratory system Diseases of the digestive system Diseases of the skin and subcutaneous tissue Diseases of the musculoskeletal system/connective tissue Diseases of the genitourinary system Symptoms, signs, abnormal findings, ill‐defined causes External causes of injury and poisoning ‐100,0 ‐50,0 0,0 50,0 100,0 150,0 Source: INE, 2010. Application for the 2010 SCML Award 55 Results 1 Causes of death sensitive to primary prevention and to health care Premature deaths considered avoidable by having a healthy behaviour and attitude are those caused by cancer of the trachea, bronchus and lung; by liver cirrhosis and by motor vehicles accidents. This group of causes of death sensitive to primary prevention represented a loss of 770.3 years of potential life per 100 000 inhabitants in 2000. In 2004 this rate was higher (804.7 per 100 000 inhabitants), but the growth trend was reversed in the following period. In 2008 the rate for causes sensitive to primary prevention was 546.6 PYLL per 100 000 inhabitants. The list of causes of premature deaths that could have been avoided by timely access to health care is much more extensive and can be consulted in table A.1.10 of the attachment, where the age groups considered for each specific cause are also mentioned. Of the years of life potentially lost by all causes of death in 2000, about one forth (25.8%) were due to causes sensitive to health care, corresponding to 1447.1 PYLL per 100 000 inhabitants. In 2008 the percentage remained in 25.8%, despite the rate having decreased to 1063.5 per 100 000 inhabitants. Table 21 Potential Years of Life Lost by causes sensitive to primary prevention and health care Total 2000 (Pop=8 663 348) 2004 (Pop=8 821 043) 2008 (Pop=8 827 605) 1 1 1 PYLL % 485762 100 Rate PYLL % Rate PYLL % Rate 5602,0 414438 100 4698,8 364211 100 4125,2 ‐25,0 0,0 ‐26,4 546,6 ‐27,8 ‐3,6 ‐29,0 1063,5 ‐25,2 ‐0,2 ‐26,5 2 Rate PYLL % Variation 2000‐08 (%) Cause of death : Sensitive to primary 66 796 13,8 770,3 70 980 17,1 804,7 48 258 13,2 prevention Sensitive to health 125 478 25,8 1447,1 113 068 27,3 1281,9 93 898 25,8 care 1 Rate of Potential Years of Life Lost per 100 000 inhabitants aged below 70. 2 CID 9 and CID 10 codes associated to each of the groups of death causes: Annex 2. Source: INE, 2010. Regarding causes sensitive to primary prevention, motor vehicle accidents are those with greater weight, despite the decrease witnessed between 2000 and 2008 (2000: 7.3%; 2008: 6.2%). It is also highlighted, on the negative side, the evolution of the PYLL and of the PYLL rate due to trachea, bronchus and lung cancer as this was the only case that suffered an increase between 2000 and 2008: 10.2% for PYLL and 8.1% for PYLL rate. Application for the 2010 SCML Award 56 Results 1 Table 22 Potential Years of Life Lost by causes sensitive to primary prevention 2000 (Pop=8 663 348) Total PYLL 485762 2004 (Pop=8 821 043) % Rate 1 PYLL 100 5602,0 414438 2008 (Pop=8 827 605) % Rate 1 PYLL 100 4698,8 364211 Cause of death2: Cancer of trachea, 15080 3,1 174,1 15653 3,8 177,4 16618 bronchus and lung 16475 3,4 190,2 19895 4,8 225,5 16202 Cirrhosis of liver Motor vehicles 35241 7,3 406,8 42585 10,3 482,8 22733 accidents 1 Rate of Potential Years of Life Lost per 100 000 inhabitants below 70. 2 CID 9 and CID 10 codes associated to each of the groups of death causes: Annex 2. Source: INE, 2010. Variation 2000‐08 (%) % 100 Rate 1 PYLL 4125,2 ‐25,0 % 0,0 Rate 1 ‐26,4 4,6 188,2 10,2 47,0 8,1 4,4 183,5 ‐1,7 31,2 ‐3,5 6,2 257,5 ‐35,5 ‐14,0 ‐36,7 Out of the group of causes considered as avoidable by the correct access and use of health care could be stressed stroke, ischemic heart disease and some diseases originated during the perinatal period, as they present the greatest rates of premature mortality (PYLL, 2008: 15707, 14975 and 12580 years, respectively; PYLL rate per 100 000 inhabitants, 2008: 177.9, 169.6 and 142.5, respectively), despite having gradually decreased during the period under analysis. Cancer also present the highest PYLL values and stand out for their growing relative representativeness in total PYLL due to all causes, mainly skin and cervix cancer. Application for the 2010 SCML Award 57 Results 1 Table 23 Potential Years of Life Lost by causes sensitive to healthcare Total 2000 (Pop=8 663 348) 2004 (Pop=8 821 043) 2008 (Pop=8 827 605) PYLL % Rate 1 PYLL % Rate 1 PYLL % Rate 1 485762 100 5602,0 414438 100 4698,8 364211 100 4125,2 Cause of death2: Intestinal infections 130 0,0 1,5 67 0,0 0,8 Tuberculosis 2827 0,6 32,6 2165 0,5 24,5 Other infectious (Diphtheria, Tetanus, 0 0,0 0,0 0 0,0 0,0 Poliomyelitis) Whooping cough and measles 235 0,0 2,7 0 0,0 0,0 Septicaemia 5290 1,1 61,1 2732 0,7 31,0 Cancer of colon and rectum 7248 1,5 83,7 7368 1,8 83,5 Cancer of skin 1685 0,3 19,4 1935 0,5 21,9 Cancer of breast 11173 2,3 129,0 9923 2,4 112,5 Cancer of cervix uteri 2400 0,5 27,7 2175 0,5 24,7 Cancer of other parts of the uterus 408 0,1 4,7 198 0,0 2,2 Cancer of testis 650 0,1 7,5 568 0,1 6,4 Hodgkin’s disease 1100 0,2 12,7 830 0,2 9,4 Leukaemia 3688 0,8 42,6 3106 0,7 35,2 Diseases of the thyroid 38 0,0 0,4 205 0,0 2,3 Diabetes mellitus 1525 0,3 17,6 2302 0,6 26,1 Epilepsy 1077 0,2 12,4 1614 0,4 18,3 Chronic rheumatic heart disease 718 0,1 8,3 860 0,2 9,7 Hypertensive disease 1010 0,2 11,7 1332 0,3 15,1 Ischemic heart disease 20885 4,3 241,1 22267 5,4 252,4 Stroke 25909 5,3 299,1 20701 5,0 234,7 All respiratory diseases (excl. 201 0,0 2,3 561 0,1 6,4 pneumonia/influenza) Influenza 45 0,0 0,5 8 0,0 0,1 Pneumonia 8607 1,8 99,3 5748 1,4 65,2 Peptic ulcer 918 0,2 10,6 768 0,2 8,7 Appendicitis 85 0,0 1,0 163 0,0 1,8 Abdominal hernia 20 0,0 0,2 115 0,0 1,3 Cholelithiasis and cholecystitis 133 0,0 1,5 475 0,1 5,4 Nephritis and nephrosis 2792 0,6 32,2 3225 0,8 36,6 Benign prostatic hyperplasia 0 0,0 0,0 0 0,0 0,0 Complications of pregnancy, 108 0,0 1,2 308 0,1 3,5 childbirth and puerperium Certain conditions originating in the 16263 3,3 187,7 15221 3,7 172,5 perinatal period Congenital cardiovascular anomalies 5209 1,1 60,1 4307 1,0 48,8 Misadventures to patients during 0 0,0 0,0 140 0,0 1,6 surgical and medical care 1 Rate of Potential Years of Life Lost for every 100 000 inhabitants less than 70 years old. 2 CID 9 and CID 10 codes, associated to each set of causes of death: Annex 2 Source: INE, 2010. 0 1238 0,0 0,3 0,0 14,0 0 0,0 0,0 0 3374 7298 1983 10110 2553 203 435 703 2706 60 1525 1137 463 1215 14975 15707 0,0 0,9 2,0 0,5 2,8 0,7 0,1 0,1 0,2 0,7 0,0 0,4 0,3 0,1 0,3 4,1 4,3 0,0 38,2 82,7 22,5 114,5 28,9 2,3 4,9 8,0 30,6 0,7 17,3 12,9 5,2 13,8 169,6 177,9 58 0,0 0,7 8 5609 538 138 355 223 2082 0 0,0 1,5 0,1 0,0 0,1 0,1 0,6 0,0 0,1 63,5 6,1 1,6 4,0 2,5 23,6 0,0 145 0,0 1,6 12580 3,5 142,5 3622 1,0 41,0 488 0,1 5,5 Application for the 2010 SCML Award 58 Results 1 Summary Potential Years of Life Lost • Decrease in premature mortality between 2000 and 2008. • Importance of premature mortality by ischemic heart disease and stroke is decreasing; cancer presents the highest PYLL values and stand out for their growing relative representativeness, mainly skin and cervix cancer. • Evolution of premature mortality by Diabetes mellitus unfavourable in 2000‐4, but in 2008 this trend reversed. • Diseases associated to alcohol abuse were responsible for more premature deaths in 2008 than in 2000 • In 2008 the rate for causes sensitive to primary prevention was 546.6 PYLL per 100 000 inhabitants. Of the years of life potentially lost by all causes of death, about one forth (25.8%) were due to causes sensitive to health care. Application for the 2010 SCML Award 59 Results 1 4.2. Mortality in 2008 according to the place of death In 2008 more than 60% of deaths among population age 15 and older occurred in a hospital/clinic, about 30% took place at home and 8,7% happened at public places. Figure 19 Percentage of deaths in 2008 by place of death 8,7 29,9 Hospital/clinic 61,4 At home At public places Source: INE, 2010 The variable place of death was analysed together with each one of the other variables, namely gender, age, place of residence, marital status, occupation and status at work, nationality and cause of death. For each cross analysis a Chi‐square test on independence of variables was performed, to test the existence of a relation between place of death and each one of the variables referred. Null hypothesis was rejected with p<0,001 in all cases, so there is strong evidence that variable place of death is related with remaining variables. Chi‐square test informs about independence between variables but not about the degree of association existent. In addition, this test is very influenced by the size of the group being studied. The high values for Chi‐square obtained don’t imply that the existent relations are very intense. Based on these values some association measures were computed: Phi coefficient, Contingency coefficient and Cramer’s V, and null hypothesis (each of the measures being zero) was tested. According with results (Annex 15), it was concluded that associations were significantly different from zero but not very intense (association measures <0.3, in all cases). Application for the 2010 SCML Award 60 Results 1 Gender and age group Death in a hospital setting was more frequent in males (64,0% vs. 58,6%) and in 45‐64 year old (70,2%) and 65‐74 year old (69,4%) age groups. Figure 20 Percentage of deaths that occurred in a hospital/clinic in 2008 by gender and age group 80,0 60,0 40,0 20,0 0,0 Total M F 15‐24 25‐44 45‐64 65‐74 75‐84 85+ Source: INE, 2010 Out of the total deaths registered in 2008 among the male population, 27,0% occurred at home. For the female population, the percentage was higher (32,9%). It must also be pointed out a significant percentage (13,2%) of young people ages 15 to 24 with registered death at home. In people age 85 and older this situation was very frequent (38,2% of the cases). Figure 21 Percentage of deaths occurred at home in 2008 by gender and age group 80,0 60,0 40,0 20,0 0,0 Total M Source: INE, 2010 F 15‐24 25‐44 45‐64 65‐74 75‐84 85+ Application for the 2010 SCML Award 61 Results 1 As for other locations, the difference between males and females is of little notice (9,0% and 8,4%, respectively). However, considerable differences when information is disaggregated by age group are observed: 37,8% of deaths of young people did not occur in a hospital/clinic, nor at home. In the 25‐44 year old age group, the percentage is still quite high (19,7%). For the population aged 45 and older, the occurrence of deaths at public places is not frequent (less than 10% of the cases). Figure 22 Percentage of deaths in 2008 occurred at public places by gender and age group 80,0 60,0 40,0 20,0 0,0 Total H M 15‐24 25‐44 45‐64 65‐74 75‐84 85+ Source: INE, 2010 Table 24 Percentage of deaths by place of death, gender and age group Total Hospital/clinic At home At public places N % N % N % Total 98840 60692 61,4 29518 29,9 8630 8,7 Gender: M F 50798 48042 32521 28171 64,0 58,6 13702 15816 27,0 32,9 4575 4055 9,0 8,4 48,9 59,4 70,2 69,4 62,6 52,5 63 715 2717 3933 10280 11810 13,2 20,9 20,6 23,8 29,9 38,2 180 675 1209 1130 2578 2858 37,8 19,7 9,2 6,8 7,5 9,3 Age‐group: 15 ‐ 24 years 476 233 25 ‐ 44 years 3420 2030 45 ‐ 64 years 13164 9238 65 ‐ 74 years 16520 11457 75 ‐ 84 years 34366 21508 85 and up 30894 16226 Source: INE, 2010. * Statistically significant differences (p<0,01) In each age group, differences in the percentage of deaths by place are observed, when analysing the male and female population separately (Annex 14). For the youngest group (15‐24 year olds), the main difference lies in deaths that take place at public places: 41,4% for boys and Application for the 2010 SCML Award 62 Results 1 28,6% for girls. This disparity is also observed in the above mentioned age group, and the percentage of deaths at public places is 23,6% in male population and 10,4% in female population. From age 25 and above, the majority of male deaths occur in a hospital setting, which characterises the female population in all age groups. Figure 23 Percentage of male deaths in 2008 by place of death and age group 100% 80% 60% 40% 20% 0% Total 15‐24 Hospital/clinic 25‐44 At home 45‐64 65‐74 75‐84 85+ At public places Source: INE, 2010. Figure 24 Percentage of female deaths in 2008 by place of death and age group 100% 80% 60% 40% 20% 0% Total 15‐24 Hospital/clinic Source: INE, 2010. 25‐44 At home 45‐64 65‐74 75‐84 85+ At public places If the information is disaggregated on the place of death by gender and by age group, the largest inequalities are observed in the youngest population. For these age groups, mortality due to external causes is particularly important. For this reason, when analysing the place of death taking into account the different socio‐demographic variables, it is relevant to compare the Application for the 2010 SCML Award 63 Results 1 information obtained considering all causes of death with the specific information on mortality due to external causes of injury and poisoning. In general terms, the percentage of deaths that occurred in a hospital/clinic is higher for general mortality than for mortality due to external causes. However, in older age groups this situation reverses. For male population age 85 and older, 57,2% of the total deaths occurs in a hospital setting, but if considering only deaths due to external causes, the percentage of those that occur in a hospital/clinic is higher (64,9%). For the female population, a similar trend for age 75 and over is observed (Annex 16). For the male population, deaths at home are more frequent in mortality due to all causes than in mortality due to external causes. In extreme age groups (ages 15‐24 and age 85 and older) the difference between percentages is higher. For the female population, this difference is also more relevant in younger women and in ages 75‐84 and age 85 and older groups. However, unlike what happened in the male population, for 25 to 64 year old women death at home is more frequent when resulting from an external cause than in mortality due to all causes. In 15 to 24 year old boys, 58,4% of deaths due to an external cause occurred at public places. When considering all causes, the percentage is lower (41,4%). This pattern is repeated in all age groups in the male population, although it is stronger in people under age 65. The same pattern is observed for the female population, although the percentage of deaths occurred at public places is lower than for males, whether it be general mortality or due to an external cause. Place of residence In the Centro, Lisboa e Vale do Tejo and Algarve Regions, more than 60% of deaths due to all causes took place in a Hospital/clinic, especially in the Algarve region, where this situation occurred for 65% of cases (according to table 25). About half of deaths due to external causes in the Norte and Centro Regions occurred during a hospital stay. In the remaining Regions the percentage is lower, especially in Alentejo, where only 30,5% of deaths resulting from external causes took place in a hospital/clinic. In this Region, was observed a particularly high percentage of deaths due to an external cause that took place at home (30,5%) and at public places (39,0%). Application for the 2010 SCML Award 64 Results 1 Marital status The percentage of deaths due to all causes that occurred in a Hospital/clinic was higher in the married (67,1%) or divorced (63,3%) population when compared with deaths in single persons, widows or widowers. If only deaths due to external causes were considered, its occurrence in a hospital setting was more frequent among widows and widowers. For deaths registered somewhere else, sharp differences between general mortality and mortality due to external causes can be observed. The percentage of deaths due to all causes in the single population that occurred at public places is 12,3%, but in the case of deaths resulting from injury or poisoning the percentage is as high as 45%. For the divorced population, the situation is similar: 10,6% for general deaths and 42,1% for deaths due to external causes. Occupation and work status Out of the 7521 deaths registered among the active population in 2008, 64,6% took place in a hospital setting, but the percentage was only 30% in case of mortality due to external causes. Conversely, 16,1% of deaths occurred somewhere else when considering all causes, but well over 52% when considering external causes. For non active population, the percentage of deaths that occurred somewhere else was lower (8,0% for all causes and 24,8% for external causes), but death at home was more frequent. The percentage of deaths of qualified workers that took place in a hospital/clinic was 65,3%. In the case of non qualified workers the percentage was lower (61,7%). For mortality due to external causes, the same pattern was observed: a higher percentage for qualified workers (31,2%) than for non qualified workers (24,2%). For deaths at public places, the pattern is the opposite, that is, the percentage of deaths at public places is higher for non qualified workers, for general mortality as well as for external causes. It must be said that the percentages shown refer to a small fraction of deaths registered in 2008, since in 93% of cases, the occupation of the dead person has not been declared. Application for the 2010 SCML Award 65 Results 1 Nationality In 2008, 1398 deaths of foreign citizens, ages 15 and older were registered in Mainland Portugal, 59,9% of which took place in a hospital setting; this percentage is very similar to the one observed among national citizens (61,4%). However, if it is taken into account only mortality due to external causes, the occurrence of death in a hospital/clinic is higher for Portuguese citizens (46,7%) than for foreigners (31,9%). The occurrence of deaths at home was less frequent among the foreign population, be it in general mortality (27,0% vs. 29,9%) or in mortality due to an external cause (16,3% vs. 19,6%). On the contrary, deaths at public places were more frequent among foreign citizens than among national citizens. For deaths due to all causes, deaths occurred at public places account for 8,7% of deaths in Portuguese citizens and 13,0% in foreigners. The difference is even sharper for mortality due to external causes: 33,7% for Portuguese citizens and 51,8% for foreigners. Figure 25 Percentage of deaths in 2008 by place of death and nationality 100% 75% 50% 25% 0% Portuguese Foreign Nation. All Portuguese Nation. All causes causes Nation. External causes Hospital/clinic Source: INE, 2010 At home Foreign Nation. External causes Elsewhere Application for the 2010 SCML Award 66 Results 1 Table 25 Percentage of deaths by place of death, gender and age group Total (N) Total Hospital/clinic (%) External Total cause 4197 61,4 At public places (%) External Total cause 8,7 34,4 29,9 External cause 19,5 53,7 48,5 42,9 30,5 41,4 35,8 29,6 25,6 28,3 26,1 16,4 17,8 20,1 30,5 21,2 5,8 9,2 10,2 13,0 8,9 29,9 33,7 36,9 39,0 37,4 56,2 67,1 56,2 63,3 58,0 38,5 45,0 63,1 30,3 28,6 31,5 25,8 34,5 26,1 30,2 16,5 19,8 19,0 27,6 42,9 12,3 7,1 9,3 10,6 11,7 45,0 35,2 17,9 42,1 28,6 1276 2628 293 64,6 60,9 69,8 30,0 55,1 35,5 19,3 31,1 20,2 17,9 20,1 20,1 16,1 8,0 10,0 52,2 24,8 44,4 825 310 3062 65,3 61,7 61,2 31,2 24,2 52,4 19,0 20,8 30,6 17,5 19,7 20,0 15,7 17,5 8,2 51,4 56,1 27,6 Total 1 98856 Place of residence: Norte Centro LVT Alentejo Algarve 31243 20320 35045 7515 4733 1229 909 1430 351 278 58,5 61,3 64,2 58,7 65,0 Marital status: Single Married Divorced Widow Unknown 11746 44688 38130 4011 281 1031 1951 897 304 14 Work status: Active Non‐active Doesn’t know/Doesn’t answer 7521 88147 2888 Occupation (Major groups CNP94)2: Qualified workers (0 a 8) Non qualified workers (9) CNP Unknown 4952 1901 92003 External cause 46,2 At home (%) Total Nationality: Portuguese 97458 4031 61,4 46,7 29,9 19,6 8,7 33,7 Foreign 1398 166 59,9 31,9 27,0 16,3 13,0 51,8 1 This table shows the total number of deaths in 2008, among population aged 15 and older, living in Mainland Portugal, which is 98856 because it includes 16 deaths whose age was unknown, that were not included in the tables above. 2 Major groups from the National Classification of Professions of 1994: (Annex 10). Source: INE, 2010. Cause of death Although 60% of deaths in global terms – if considering all causes of death – occur in a hospital setting, we can observe considerable differences when we analyse specific causes of death. In fact, in the case of deaths due to infectious and parasitic diseases or diseases of the digestive system, the fraction of deaths in a hospital/clinic was much higher than the average (91,9% and 88,6%, respectively); it is also high ‐‐ 80% approximately – for diseases of the genitourinary system, of the musculoskeletal system /connective tissue and of the skin and subcutaneous tissue (Annex 16). Application for the 2010 SCML Award 67 Results 1 In the case of death due to cancer, approximately 75% occurred in a hospital/clinic, but the percentage is higher in the case of cervix cancer (83,3%). In 2008, only a little over half of deaths due to ischemic heart disease (IHD) and stroke occurred in a hospital setting (51,7% and 51,3%, respectively). Conversely, death at home was fairly common: 39,2% of deaths due to IHD and 40,5% of deaths due to stroke. Moreover, there is a fairly important percentage of deaths due to these causes that occurred at public places: 9,1% in the case of IHD and 8,3% for stroke. Out of the 10523 deaths in 2008 and classified as due to symptoms, signs, abnormal findings or ill‐defined causes, more than half (51,8%) took place at home, 25,5% in a hospital/clinic and 22,7% somewhere else. Deaths due to external causes occurred mainly in a hospital/clinic (46,2%), but a relevant fraction of these deaths occurred somewhere else (34,4%). Table 26 Percentage of deaths by place of death and cause of death Total Total Hospital/clinic N % At home N N 98840 60692 61,4 29518 29,9 Cause of death2: 2513 2310 91,9 152 6,0 Infectious and parasitic diseases 22914 17151 74,8 5077 22,2 Cancers 3542 2654 74,9 789 22,3 Colon, rectum and anus 1504 1085 72,1 340 22,6 Female breast 233 194 83,3 30 12,9 Cervix uteri 3990 2469 61,9 1243 31,2 Diabetes mellitus 134 72 53,7 48 35,8 Alcohol abuse 7300 3776 51,7 2860 39,2 Ischemic heart diseases 13994 7173 51,3 5666 40,5 Cerebrovascular diseases 10857 8334 76,8 2051 18,9 Diseases of the respiratory system 4297 3808 88,6 410 9,5 Diseases of the digestive system 24 19 79,2 NA NA Diseases of the skin and subcutaneous tissue 252 205 81,3 42 16,7 Diseases of the musculoskeletal system/connective tissue 2753 2295 83,4 366 13,3 Diseases of the genitourinary system 10523 2680 25,5 5454 51,8 Symptoms, signs, abnormal findings, ill‐defined causes 4197 1937 46,2 817 19,5 External causes of injury and poisoning 1 CID 9 and CID 10 codes, associated to each one of the causes of death: table A1.6, (see Annex 2). NA – Data not available due statistical confidentiality. Source: INE, 2010. At public places % N 8630 8,7 51 686 99 79 9 278 14 664 1155 472 79 NA 5 92 2389 1443 2,0 3,0 2,8 5,3 3,9 7,0 10,4 9,1 8,3 4,3 1,8 NA 2,0 3,3 22,7 34,4 Application for the 2010 SCML Award 68 Results 1 Quality of Data In 2008, there were 10523 deaths due to ill‐defined causes, which corresponds to 10,6% of the total of registered deaths. More than half of the deaths due to ill‐defined causes (51,8%) occurred at home, but 2680 (25,5%) of deaths to which it was impossible to attribute a specific cause took place in a hospital setting. A slightly lower percentage (22,7%) of deaths due to ill‐defined causes occurred at public places. If the total number of deaths that occurred in each place were considered, it is observed that an ill‐defined cause was more frequent whenever death did not occur in a hospital setting or at home, with a percentage of 27,7% of cases. For deaths that occurred at home and in a hospital/clinic, the percentages of deaths due to ill‐defined causes were 18,5% and 4,4%, respectively. Table 27 Percentage of deaths for ill‐defined cause by place of death Total Total Symptoms, signs, abnormal findings, ill‐ defined causes Source: INE, 2010. Hospital/clinic At home At public places N N % N N % N % 98840 100,0 60692 100,0 29518 100,0 8630 100,0 10523 10,6 2680 4,4 5454 18,5 2389 27,7 Profile of the population that died in 2008 by place of death The adult citizen (age 15 and older) living in Mainland Portugal who died in 2008 in a hospital/clinic was, on average, male, aged 45‐64, living in the Algarve and married. He was of working age, having a job as a qualified worker and of Portuguese nationality. Death was caused by infectious and parasitic diseases. Application for the 2010 SCML Award 69 Results 1 Table 28 Profile of the population who died in 2008 in a hospital/clinic % (N=98840) Gender: M 64,0 Age group: 45 ‐ 64 years 70,2 Place of residence: Algarve 65,0 Marital status: Married 67,1 Work status: Doesn’t know/Doesn’t answer Active 69,8 64,6 Occupation (7521 employees): Qualified worker (0 a 8) 65,3 Nationality: Portuguese 61,4 Cause of death: Infectious and parasitic diseases Source: INE, 2010 91,9 The person who died at home was of female gender, aged 85 or older. She lived in the Norte Region and was a widow. She belonged to the non active population and her profession is not known. She had Portuguese nationality. It was not possible to identify the exact cause of death in majority of cases. Table 29 Profile of the population who died at home in 2008 % (N=98840) Gender: F 32,9 Age group: 85 and up 38,2 Place of residence: Norte 35,8 Marital status: Widow 34,5 Work status: Non active 31,1 Occupation (7521 employees): CNP Unknown 30,6 Nationality: Portuguese 29,9 Cause of death: Symptoms, signs, abnormal findings, ill‐defined causes Stroke Source: INE, 2010 Application for the 2010 SCML Award 51,8 40,5 70 Results 1 The citizen who died at public places was male and young (age 15 to 24). He lived in Alentejo and was single. He belonged to the active population as a non qualified worker. The citizen had foreign nationality and died from external causes. Table 30 Profile of the population that died at public places in 2008 % (N=98840) Gender: H 9,0 Age group: 15 ‐ 24 years 37,8 Place of residence: Alentejo 13,0 Marital status: Single 12,3 Work status: Active 16,1 Occupation (7521 employees): Non qualified workers (9) 17,5 Nationality: Foreign 13,0 Cause of death: External causes of injury and poisoning Source: INE, 2010 34,4 Application for the 2010 SCML Award 71 Results 1 Summary Mortality by Place of Death • Strong evidence that variable place of death is related with remaining variables (gender, age, place of residence, marital status, occupation and status at work, nationality and cause of death). • Associations were significantly different from zero but not very intense. • Distribution of deaths by age group differs, according to place of death: Deaths at hospital/clinic: most frequent in age group 45‐74 years; At home predominate deaths of the oldest (75 years and up); Deaths at public places are more common for the youngest (15‐24 years). • Distribution of deaths by age group differs, according to causes of death: For major groups of causes, death occurs in hospital/clinic in more than 70% of the cases; For deaths caused by ischemic heart disease and stroke, the difference between the percentages of deaths in hospital/clinic and at home is smaller; For these two causes, as well for Diabetes Mellitus and alcohol abuse, the percentage of deaths at home varies between 25‐40%; Percentage of deaths in public places is higher when the cause is external (34,4%) or ill‐defined (22,7%). Application for the 2010 SCML Award 72 Results 2 5. Results 2 5.1. Change in the Intra‐hospital lethality rate from 2000 to 2008 5.1.1. Hospitalizations, deaths and lethality Gender and age group From 2000 to 2008, the total number of hospital admissions achieved a relative increase of 32,6%, as it went from 650.444 to 862.2046. Likewise, the number of deaths of in‐patients increased, with 37.224 deaths in 2000 and 46.450 in 2008. For its part, the intra‐hospital lethality rate resulting from the ratio of the number of deaths of in‐patients to the number of hospitalizations dropped from 5,7% in 2000 to 5,4% in 2004, while holding steady in 2008. The total number of hospitalizations is higher for women, throughout the entire period under analysis, although there tends to be an increase in the difference between genders, since the relative increase in women is sharper. In 2008, 457.815 females and 404.384 males were hospitalized. However, the total number of deaths is higher for men, resulting in a much higher intra‐hospital lethality rate (2008: men 6,2% and women 4,6%). The trend for decreased intra‐ hospital lethality rate occurs in both genders, although the decline is sharper for females (2008: men 1,8% and women 9,1%). The distribution of hospitalizations by age groups shows that there were increases in every age group, except for younger people (relative decrease of 14,5%7). As would be expected, and taking demographic change into account, the highest relative increases have occurred in older age groups (ages 85 and up: 75,6%; and ages 75‐85: 64,0%). The change in the number of deaths of in‐patients, by age group, is similar to that of hospitalizations, with an increase in older age groups and a decrease in younger ones. From 2000 to 2008, there were relative increases in the 45‐64 (10,4%), 75‐84 (36,5%) and 85 and over (70,4%) age groups, with a decrease in the 15‐24 (49,1%) and 25‐44 (‐22,0%) age groups. The 65‐ 74 age group rose slightly from 2000 to 2004, while decreasing from 2000 to 2008 (1,7%). The intra‐hospital lethality rate is higher in older age groups: in 2008, figures ranged from 17,5% in the 85 and over age group to 0,5% in the 15 to 24 age group. 6 Figures take into account the assumptions explained under the chapter on Methodology It should be pointed out that the resident population of people ages 15 to 24 in Mainland Portugal declined 18% during the same period (INE, 2010). 73 Application for the 2010 SCML Award 7 Results 2 Table 31 Number of hospitalizations, hospitalization deaths and intra‐hospital lethality rate, by age group 2004 2008 Let. (%) 762038 41365 5,4 Let. (%) 862204 46450 5,4 Variation 2000‐2008 (%) Let. Hosp. Death (%) 32,6 24,8 ‐5,9 364840 22534 397193 18831 5 0 404384 25172 457815 21278 5 0 24,7 40,4 ‐ 22,5 27,6 ‐ ‐1,8 ‐9,1 ‐ ‐14,5 14,8 33,2 25,6 64,0 75,6 ‐49,1 ‐22,0 10,4 ‐1,7 36,5 70,4 ‐40,4 ‐32,1 ‐17,1 ‐21,7 ‐16,8 ‐3,0 2000 Total 650444 37224 Let. (%) 5,7 Gender: M F Unknown 324254 20552 326188 16672 2 0 6,3 5,1 0,0 Hosp. Death. Hosp. Death 6,2 4,7 0,0 Hosp. Death 6,2 4,6 0,0 Age‐group: 15 ‐ 24 years 43342 369 0,9 40693 242 0,6 37065 188 0,5 25 ‐ 44 years 126804 2046 1,6 145144 2006 1,4 145584 1596 1,1 45 ‐ 64 years 191762 6618 3,5 223906 6688 3,0 255398 7303 2,9 65 ‐ 74 years 139578 9148 6,6 158516 9272 5,8 175371 8995 5,1 75 ‐ 84 years 110006 12035 10,9 145113 14620 10,1 180392 16426 9,1 85 up 38952 7008 18,0 48666 8537 17,5 68394 11942 17,5 Deaths of people ages 100 and up: 74 in 2000 and 2004; and 125 in 2008 Source: ACSS, DRG database When looking at hospital admissions by gender and age group simultaneously, it was noticed that female hospitalizations are higher than male hospitalizations in the following age groups: ages 25 to 44, 45 to 64 and 75 to 84. However, there is a small difference between the number of male and female hospitalizations in the following age groups: 45 to 64 and 65 to 74. As previously mentioned, the number of deaths of hospitalized patients is higher for men than for women; however, this is not the case in every age group. This difference between genders diminishes with increased age and, in people ages 85 and up, figures are higher for women (2008: 7.220 women and 4.722 men). Figure 26 Number of hospitalizations, hospitalization deaths, by gender and age group Source: ACSS, DRG database Application for the 2010 SCML Award 74 Results 2 The intra‐hospital lethality rate tends to be higher in men of every age group, except those in the 75‐84 and 85 and over age groups, where the given figures are close to each other. From 2000 to 2008, there was a more positive change (rate decrease) for males in younger age groups (15‐24 and 25‐44) and in the 85 and over age group, and for females in all the other age groups (45‐64, 65‐74 and 75‐84 years). Table 32 Number of hospitalizations, hospitalization deaths and intra‐hospital lethality rate, by gender and age group 2000 Total Gender: M F Unknown Gender and age‐group: 2004 Hosp. Death. Let. (%) Hosp. Death 2008 Let. (%) Hosp. Death Variation 2000‐2008 (%) Let. (%) Hosp. Death Let. (%) 650444 37224 5,7 762038 41365 5,4 862204 46450 5,4 32,6 24,8 ‐5,9 324254 20552 326188 16672 2 0 6,3 5,1 0,0 364840 22534 397193 18831 5 0 6,2 4,7 0,0 404384 25172 457815 21278 5 0 6,2 4,6 0,0 24,7 40,4 ‐ 22,5 27,6 ‐ ‐1,8 ‐9,1 ‐ 15 ‐ 24 years M 24996 249 1,0 22414 163 0,7 20368 123 0,6 ‐18,5 ‐50,6 F 18345 120 0,7 18278 79 0,4 16697 65 0,4 ‐9,0 ‐45,8 25 ‐ 44 years M 61194 1382 2,3 66392 1357 2,0 64285 1025 1,6 5,1 ‐25,8 F 65610 664 1,0 78752 649 0,8 81298 571 0,7 23,9 ‐14,0 45 ‐ 64 years M 96993 4248 4,4 108010 4354 4,0 122013 4855 4,0 25,8 14,3 F 94768 2370 2,5 115894 2334 2,0 133383 2448 1,8 40,7 3,3 65 ‐ 74 years M 74793 5568 7,4 82817 5643 6,8 89492 5608 6,3 19,7 0,7 F 64785 3580 5,5 75698 3629 4,8 85878 3387 3,9 32,6 ‐5,4 75 ‐ 84 years M 52012 6330 12,2 67338 7654 11,4 82846 8839 10,7 59,3 39,6 F 57994 5705 9,8 77774 6966 9,0 97545 7587 7,8 68,2 33,0 85 and up M 14266 2775 19,5 17869 3363 18,8 25380 4722 18,6 77,9 70,2 F 24686 4233 17,1 30797 5174 16,8 43014 7220 16,8 74,2 70,6 Deaths of people ages 100 and up: Men ‐ 35 in 2000, 21 in 2004, 34 in 2008; Women ‐ 39 in 2000, 53 in 2004, 91 in 2008 Source: ACSS, DRG database Place of residence The trend for an increased number of hospitalizations and hospitalization deaths, as previously described for Mainland Portugal, was also noticed in every Region8. The Algarve achieved the highest relative increase in the number of hospitalizations (55,0%) as well as in the number of deaths of in‐patients (57,5%). By contrast, the Alentejo Region obtained the lowest relative 8 NUT II pursuant to D.L. no. 317/99, dated 11 August (1999) Application for the 2010 SCML Award 75 ‐39,4 ‐40,5 ‐29,4 ‐30,6 ‐9,1 ‐26,6 ‐15,8 ‐28,6 ‐12,3 ‐20,9 ‐4,4 ‐2,1 Results 2 increase, both in the number of hospitalizations (22,5%) and deaths (16,9%). However, as concerns the intra‐hospital lethality rate, the Algarve Region recorded a slight increase (1,6%), from 2000 to 2008. For their part, the other Regions achieved a drop in this rate from 2000 to 2008, even though the lowest figure for the Center Region was obtained in 2004. Table 33 Number of hospitalizations, hospitalization deaths and intra‐hospital lethality rate, by place of residence (NUT II, pursuant to D.L. n. º 317/99, date 11 August) 2000 Hosp. Total NUT II – place of residence: Norte Centro LVT Alentejo Algarve Death. 650444 37224 199569 10166 138789 7426 233590 14823 36027 2454 21649 1535 20820 820 Unknown Source: ACSS, DRG database 862204 46450 Let. (%) 5,4 Variation 2000‐2008 (%) Let. Hosp. Death (%) 32,6 24,8 ‐5,9 4,6 5,0 6,2 6,6 6,2 299301 13451 182400 9342 288890 17742 44134 2868 33549 2417 4,5 5,1 6,1 6,5 7,2 50,0 31,4 23,7 22,5 55,0 32,3 25,8 19,7 16,9 57,5 ‐11,8 ‐4,3 ‐3,2 ‐4,6 1,6 5,1 13930 4,5 ‐33,1 ‐23,2 14,8 2004 Let. (%) 5,7 2008 762038 41365 Let. (%) 5,4 5,1 5,4 6,3 6,8 7,1 249667 11518 166220 8317 264062 16465 36775 2442 27953 1746 3,9 17361 Hosp. Death 877 Hosp. Death 630 The intra‐hospital lethality rate tends to achieve lower figures in the NUT III of the coastal areas of the North and Center, and higher figures in the interior of the Centro Region, the Alentejo and the Algarve. However, this analysis needs to consider age. In 2008, the NUT III Alto Alentejo and Pinhal Interior Sul achieved not only the highest intra‐hospital lethality rate (7,8% and 7,4%, respectively), but also the highest median age of in‐patient living in those areas (ages 71 and 79, respectively). The reverse situation occurs in the Tâmega and Entre Douro e Vouga, with the lowest intra‐hospital lethality rates (4,2% and 3,4%, respectively) and median age (57 and 59, respectively). From 2000 to 2008, 17 of the 28 NUTIII achieved a decrease in the intra‐hospital lethality rate, with the highest relative decrease occurring in the Entre Douro e Vouga area (23,1%). There was an increase in the other 11 NUTIII, with the Beira Interior Sul area achieving the highest relative increase (27,6%) (see Annex 17). Application for the 2010 SCML Award 76 Results 2 Figure 27 Intra‐hospital lethality rate, by place of residence (NUT III) Source: ACSS, DRG database Place of hospitalization From 2000 to 2008, the group of hospitals of the Algarve Health Region obtained the highest relative increase in hospital admissions (59,5%) and in in‐patients deaths (63,6%). By contrast, the hospitals of the Lisboa e Vale do Tejo (achieved the lowest relative increase in hospitalizations (23,7%) and deaths (18,7%). Throughout the period being analyzed, the intra‐hospital lethality rate dropped 5,4%. In regional terms, there were very different trends. The Norte Health Region obtained the greatest relative decrease (10,0%), while the Centro, Lisboa e Vale do Tejo and the Alentejo achieved small relative decreases (3,3%, 4,1 and 4,7%, respectively). The Algarve Region, on the other hand, rose 2,6%. Application for the 2010 SCML Award 77 Results 2 Table 34 Number of hospitalizations, hospitalization deaths and intra‐hospital lethality rate, by place of hospitalization (health Region) 2000 2004 Let. Hosp. Death (%) 650444 37224 5,7 762038 41365 Hosp. Death. Total Health Region – place of hopsitalization Norte 212574 10420 Centro 147799 7842 LVT 243729 15505 Alentejo 26467 2008 Algarve 19875 1449 Source: ACSS, DRG database 4,9 259392 11871 5,3 174614 8713 6,4 275040 17146 7,6 26913 1972 7,3 26079 1663 2008 Let. (%) 5,4 4,6 5,0 6,2 7,3 6,4 Hosp. Variation 2000‐2008 (%) Death 862204 46450 304453 13431 189976 9748 301533 18403 34546 2497 31696 2371 Let. (%) 5,4 Hosp. Death Let. (%) 32,6 24,8 ‐5,9 4,4 5,1 6,1 7,2 7,5 43,2 28,5 23,7 30,5 59,5 28,9 24,3 18,7 24,4 63,6 ‐10,0 ‐3,3 ‐4,1 ‐4,7 2,6 In both 2000 and 2008, the Alentejo Region showed the highest intra‐hospital lethality rate (7,6% and 7,2%, respectively), with the lowest figure achieved by the Norte Region (4,9% and 4,4%, respectively). Figure 28 Proportion of surviving and deceased (intra‐hospital lethality) in‐patients, by place of hospitalization (Health Region) Source: ACSS, DRG database As examining the flows of hospitalization and of hospitalization deaths among the selected major reference hospitals and patients’ place of residence, the range of their respective spheres of Application for the 2010 SCML Award 78 Results 2 influence it is pointed out. Although the flows are more significant in bordering areas served by these hospitals, it was noticed that they basically hospitalize people from the entire Health Region where they are located. Lisbon hospitals admit patients not only from the Lisboa e Vale do Tejo Health Region, but also from the entire Alentejo and the Algarve. Figure 29 Origin/destination flows between the place of hospitalization (hospitals) and the place of residence of in‐patients Source: Prepared by the work team, based on the DRG Cause of hospitalization The diseases of the circulatory system comprise the most important causes of hospitalization: in 2008, there was a total of 136.793 hospitalizations (15% of the total), followed by diseases of the digestive system (104.549 hospitalizations), diseases of the respiratory system (80.429 hospitalizations), diseases of the genitourinary system (75.851) and cancers (73.413 hospitalizations). For their part, respiratory diseases, circulatory diseases and cancers are the leading causes of death (24,7%, 23,3% and 22,5% of the total, respectively). The intra‐hospital lethality rate is higher in infectious and parasitic diseases (15,4%), cancers (14,3%) and diseases of the respiratory system (14,3%). Application for the 2010 SCML Award 79 Results 2 The biggest increase in the number of hospitalizations occurred in mental and behavioral disorders (88,1%), followed by diseases of the genitourinary system (54,4%) and diseases of the musculoskeletal system/connective tissue (47,9%). The biggest increases in the number of hospitalization deaths occurred with diseases of the genitourinary system (85,2%), diseases of the respiratory system (66,8%) and infectious and parasitic diseases (58,7%). The intra‐hospital lethality rate rose 57,3% for infectious and parasitic diseases and 18,3% diseases of the respiratory system, while the biggest decreases occurred in mental and behavioral disorders (59,4%) and in alcohol abuse (51,4%). Table 35 Number of hospitalizations, hospitalization deaths and intra‐hospital lethality rate, by cause of hospitalization (main diagnosis) 2000 2004 Let. Hosp. Death. (%) Hosp. Death 2008 Let. (%) Total 650444 37224 5,7 762038 41365 Infectious and parasitic d. Tuberculosis AIDS (HIV‐disease) Viral hepatitis 15440 2500 3465 1496 1507 9,8 203 8,1 588 17,0 14 0,9 16736 2161 3593 1348 2065 12,3 154 7,1 638 17,8 17 1,3 Cancers Gastrointestinal Colon, rectum and anus Larynx and trachea/bronchus/lung Skin Gynecologic Female Breast Cervix uteri Prostate Kidney and bladder Lymph./haematopoietic tissue 56050 15956 8152 8227 14,7 2736 17,1 1059 13,0 67360 17291 9090 5632 1285 22,8 474 8546 5368 1042 2770 4570 47 846 468 103 353 317 4314 Diabetes Mellitus Hosp. Variation 2000‐2008 (%) Let. Let. Death Hosp. Death (%) (%) 32,6 24,8 ‐5,9 15582 1543 3270 649 2392 15,4 0,9 100 6,5 ‐38,3 462 14,1 ‐5,6 19 2,9 ‐56,6 58,7 ‐50,7 ‐21,4 35,7 57,3 ‐20,2 ‐16,7 212,8 9529 14,1 3156 18,3 1233 13,6 73413 17871 9539 10465 14,3 3514 19,7 1447 15,2 31,0 12,0 17,0 27,2 28,4 36,6 ‐2,9 14,7 16,8 5878 1542 26,2 6176 1741 28,2 9,7 35,5 23,6 9,9 9,9 8,7 9,9 12,7 6,9 794 10178 6432 1211 3206 5226 55 810 427 105 403 346 6,9 8,0 6,6 8,7 12,6 6,6 1129 10929 7121 1006 3135 5985 69 761 373 105 452 425 6,1 138,2 7,0 27,9 5,2 32,7 10,4 ‐3,5 14,4 13,2 7,1 31,0 46,8 ‐10,0 ‐20,3 1,9 28,0 34,1 ‐38,4 ‐29,7 ‐39,9 5,6 13,1 2,4 796 18,5 4818 918 19,1 4471 886 19,8 3,6 11,3 7,4 10438 644 6,2 12169 660 5,4 12644 550 4,3 21,1 ‐14,6 ‐29,5 Alcohol abuse 2533 59 2,3 2741 21 0,8 2827 32 1,1 11,6 ‐45,8 ‐51,4 Drug dependence, toxicomania 566 2 0,4 354 1 0,3 493 1 0,2 ‐12,9 ‐50,0 ‐42,6 D. of the circulatory system Ischaemic heart diseases Stroke 119424 10960 9,2 131441 10803 8,2 136793 10836 7,9 29309 1753 6,0 30096 2012 6,7 28036 1642 5,9 36042 5355 14,9 35379 4899 13,8 33107 4443 13,4 14,5 ‐4,3 ‐8,1 ‐1,1 ‐6,3 ‐17,0 ‐13,7 ‐2,1 ‐9,7 D. of the respiratory system Pneumonia Chronic lower respiratory 57034 24115 10457 41,0 43,6 9,9 66,8 88,3 ‐8,0 18,3 31,1 ‐16,3 6887 12,1 4095 17,0 802 7,7 Application for the 2010 SCML Award 65852 26818 10965 5,4 862204 46450 5,4 8779 13,3 5403 20,1 775 7,1 80429 34626 11493 11486 14,3 7711 22,3 738 6,4 80 Results 2 2000 2004 2008 Hosp. Death. Let. (%) Hosp. Death Let. (%) Hosp. 1712 1,2 1561 23 1,5 1618 Variation 2000‐2008 (%) Let. Let. Death Hosp. Death (%) (%) diseases which asthma 21 23 1,4 ‐5,5 9,5 15,9 D. of the digestive system Chronic liver disease 92789 7981 3190 3,4 102729 915 11,5 7482 3563 3,5 104549 955 12,8 6521 3655 3,5 12,7 894 13,7 ‐18,3 14,6 ‐2,3 1,7 19,6 D. of the musculoskeletal system/connective tissue 14401 212 1,5 17438 235 1,3 18108 208 1,1 25,7 ‐1,9 ‐22,0 30602 137 0,4 40174 141 0,4 45262 177 0,4 47,9 29,2 ‐12,6 8398 32 0,4 11548 21 0,2 13158 18 0,1 56,7 ‐43,8 ‐64,1 Diseases of the genitourinary system 49133 946 1,9 65106 1262 1,9 75851 1752 2,3 54,4 85,2 20,0 Mental and behavioural disorders 11873 156 1,3 15893 111 0,7 22332 119 0,5 88,1 ‐23,7 ‐59,4 Injury and poisoning 66550 2091 3,1 64984 1942 3,0 67051 2454 3,7 0,8 17,4 16,5 Symptoms, signs, abnormal findings, ill‐defined causes 9428 572 6,1 9706 500 5,2 10046 424 4,2 6,6 ‐25,9 ‐30,4 Other situations* 38998 590 2 39579 540 2 39911 613 2 2,3 3,9 ‐6,7 Unknown 55 0 0,0 21 2 9,5 291 0 0,0 429,1 0,0 *The group “Other situations” consists of Factors that influence that health status and contact with health services (ICD9: V00 – V99), Congenital deformities and chromosomal abnormalities (ICD9: 740 ‐ 759) and A few ailments originating in the perinatal period (ICD9: 760 ‐ 779) Source: ACSS, DRG database 0,0 D. of the skin and subcutaneous tissue Rheumatoid arthritis and osteoarthrosis External causes The number of hospitalizations due to external causes rose 14,5%, from 2000 to 2008. There was an increasing trend for both genders, particularly for women compared to men (34% and 5%, respectively), although the figures for the latter remain slightly higher. In‐patient deaths due to external causes occur more often in men; however, the bigger increase occurred in women (2000‐2008: 37,3% and 38,9%, respectively). Also, the intra‐hospital lethality rate due to external causes is higher in men, with a strong tendency to increase, which has contributed toward greater gender differentiation. From 2000 to 2008, the intra‐hospital lethality rate rose 29,8% in men and 4,3% in women. Application for the 2010 SCML Award 81 Results 2 Table 36 Number of hospitalizations, hospitalization deaths and intra‐hospital lethality rate, by external causes of injury and poisoning 5674 Let. (%) 5,7 Variation 2000‐2008 (%) Let. Hosp. Death (%) 14,6 38,0 20,5 51636 48381 3149 2525 6,1 5,2 5,0 26,9 37,3 38,9 30,8 9,5 3,5 4,3 7325 31452 274 1421 3,7 4,5 ‐58,7 6,2 ‐51,9 14,7 16,4 8,0 144 4,4 2750 150 5,5 ‐6,1 11,9 19,2 2,28 1513 31 2,1 1244 18 1,5 ‐24,8 ‐50,0 ‐33,5 5,8 46 4,7 929 67 7,2 2,4 26,4 23,4 2000 2008 4111 Let. Hosp. Death (%) 4,7 99403 5308 Let. (%) 5,4 100017 2293 1818 4,7 53540 4,8 45863 2968 2340 5,4 5,1 570 1239 3,2 11114 4,2 31150 388 1351 134 4,6 36 53 Hosp. Death. Total 87298 Gender: M 49170 F 38128 External causes: Transport accidents 17738 Accidental falls 29618 Suicide and intentional 2927 self‐harm Homicide, assault 1655 Events of undetermined 907 intent Source: ACSS, DRG database 2004 3258 978 Hosp. Death Accidental falls are the most significant external causes with regard to hospitalizations and in‐ patient deaths, while events of undetermined intent are the leading causes of intra‐hospital lethality. From 2000 to 2008, of the external causes noted, transport accidents achieved the biggest decreases in the number of hospitalizations and deaths (58,7% and 51,9%, respectively) and homicide, assault in intra‐hospital lethality (33,5%). Figure 30 Hospitalizations and hospitalization deaths, due to external causes of injury and poisoning Source: ACSS, DRG database Application for the 2010 SCML Award 82 Results 2 In 2008, the DRG database showed 312 autopsies on the deaths of hospitalized patients, totaling less than 1% of the total number of hospitalization deaths. Of these 312 autopsies, 36% were performed at reference hospitals in Lisbon (CHLO, CHLN and CHLC). The main diagnoses on the most frequent autopsied deaths correspond to circulatory diseases, with the common ones being acute pulmonary heart disease, acute myocardial infarction, cardiac dysrhythmias and heart failure. It was also identified 82 occurrences indicating external cause, 39% of which refer to clinical and surgical procedures with an abnormal reaction in the patient or late complications with no reference to complications during the procedure, with 25% pertaining to accidental falls. There were identified only 3 autopsies on deaths whose main diagnosis included Symptoms, signs, abnormal findings, ill‐defined causes. Application for the 2010 SCML Award 83 Results 2 Summary Hospitalizations (862.204 in 2008) • Increase of 32,6% between 2000 and 2008 • More hospitalizations in women • The 45 to 64 age‐group has the highest number of hospitalizations • The most frequent primary diagnosis of hospitalizations is related to diseases of the circulatory system. Hospitalizations deaths (46.450 in 2008) • Increase of 24,8% between 2000 and 2008 • More hospitalization death in men • The 75 to 84 age‐group has the highest number of hospitalization deaths • The diseases of the respiratory system are the main cause of hospitalization deaths Intra‐hospital lethality rate (5,4% in 2008) • Decreased 5,9% between 2000 and 2008 • Is higher in men and in older age‐groups • The Norte Region has the lowest rate • The infectious and parasitic diseases are responsible for the highest rate Application for the 2010 SCML Award 84 Results 2 5.1.2. Diseases of the circulatory system From 2000 to 2008, hospitalizations due to circulatory system diseases showed a relative increase of 15,5%, as it went from 119.424 to 136.793, while the number of in‐patient deaths showed a slight decrease (1,1%), along with a drop in the intra‐hospital lethality rate (‐14,1%). Although the number of hospitalizations was higher for males during the years analyzed, the number of deaths and the intra‐hospital lethality rate were always higher for females. As would be expected, the higher intra‐hospital lethality rate occurs in older age groups. Table 37 Number of hospitalizations, hospitalization deaths and intra‐hospital lethality rate, by diseases of the circulatory system (ICD 9: 390‐459), according to age group Hosp. Death. Hosp. Death Let. (%) 131441 10803 8,2 Hosp. Death Total Let. (%) 119424 10960 9,2 Let. (%) 136793 10836 7,9 Variation 2000‐2008 (%) Let. Hosp. Death (%) 14,5 ‐1,1 ‐14,1 Gender: M F 63652 55772 5421 5539 8,5 9,9 67465 63976 5233 5570 7,8 8,7 70500 66293 5196 5640 7,4 8,5 10,8 18,9 ‐4,2 1,8 ‐12,9 ‐14,1 Age‐group: 15 ‐ 24 years 25 ‐ 44 years 45 ‐ 64 years 65 ‐ 74 years 75 ‐ 84 years 1093 9519 33675 33636 30546 22 191 1321 2754 4247 2 2 3,9 8,2 13,9 1151 11556 35569 34237 36213 11 192 1172 2322 4515 1 1,7 3,3 6,8 12,5 1100 11486 36614 32640 38511 19 181 1098 1937 4254 1,7 1,6 3 5,9 11,1 0,6 20,7 8,7 ‐3,0 26,1 ‐13,6 ‐5,2 ‐16,9 ‐29,7 0,2 ‐15,0 ‐20,0 ‐23,1 ‐28,0 ‐20,1 85 and up 10955 2425 Source: ACSS, DRG database 22,1 12715 2591 20,4 16442 3347 20,4 50,1 38,0 ‐7,7 2000 2004 2008 In 2008, hospitalizations for ischemic heart disease (IHD) and for stroke account for some 40% of all hospitalizations for circulatory diseases and in‐patient deaths due to these two causes, 55% of the total number of deaths caused by diseases of the circulatory system. Application for the 2010 SCML Award 85 Results 2 Table 38 Percentage of hospitalizations and hospitalization deaths due to ischemic heart disease and cerebral vascular accident relative to the total number of diseases of the circulatory system 2000 2004 2008 Hosp. Death. Hosp. Death. Hosp. Death. n.º % n.º % n.º % n.º % n.º % n.º % Diseases of the circulatory 119424 100,0 10960 100,0 131441 100,0 10803 100,0 136793 100,0 10836 100,0 system 29309 24,5 1753 16,0 30096 22,9 2012 18,6 28036 20,5 1642 15,2 Ischemic heart disease Cerebral vascular 24340 20,4 4048 36,9 25221 19,2 3909 36,2 28089 20,5 4204 38,8 accidents Source: ACSS, DRG database Although there were equal numbers of IHD and stroke in circulatory disease‐related hospitalizations (2008: 20,5% for both), stroke stands out as the leading cause of death (38,8%). Figure 31 Percentage of hospitalizations and hospitalization deaths due to ischemic heart disease and cerebral vascular accident relative to diseases of the circulatory system Source: ACSS, DRG database 5.1.2.1. Ischemic Heart Disease (IHD) Gender and age group From 2000 to 2008, there was a slight decrease in the number of hospitalizations for IHD (4,3%), with a drop from 29.309 to 28.036, although the highest figure was obtained in 2004 (30.096). A similar trend was noticed in the number of in‐patient deaths caused by this disease, with a relative decrease of 6,3%. Also, with regard to the intra‐hospital lethality rate due to IHD, there was an increase from 2000 (6,0%) to 2004 (6,7%) and a drop in 2008 (5,9%), to levels similar to initial figures. Application for the 2010 SCML Award 86 Results 2 Throughout the period being analyzed, the total number of hospitalizations due to IHD is twice as high in men as in women (2008: 18.914 males and 9122 females). However, as concerns deaths, the figures are close (2008: 896 male and 746 female deaths), thus resulting in a much higher intra‐hospital lethality rate in women (8,2%) than in men (4,7%). With regard to age groups, IHD‐related hospitalizations attained the highest figure in the 45‐64 age group (2008: 9623), with the lowest figure occurring in the 15‐24 age group (2008: 14). However, from 2000 to 2008, there were increases in the number of hospitalizations for this disease in the 75‐84 and 85 and over age groups. For their part, the number of IHD‐related in‐ patient deaths obtained is higher in the 75‐84 age group and, as expected and desired, null in the 15 to 24 age group. From 2000 to 2008, only the group of patients ages 85 and up achieved an increase (30,9%). IHD‐related intra‐hospital lethality rate increases with age, with the highest figure achieved in the 85 and over age group (21,9%). However, older age groups show decreases in this rate, with slight increases in the 25 to 44 and 45 to 64 age groups. Table 39 Number of hospitalizations, hospitalization deaths and intra‐hospital lethality rate due Ischemic Heart Disease (ICD 9: 410‐414), by age group 2000 2004 Total 2008 Variation 2000‐2008 (%) Let. Let. Let. Hosp. Death. Let. (%) Hosp. Death Hosp. Death Hosp. Death (%) (%) (%) 29309 1753 6,0 30096 2012 6,7 28036 1642 5,9 ‐4,3 ‐6,3 ‐1,7 Gender: M F 19733 9576 952 801 4,8 8,4 19547 1040 10549 972 5,3 9,2 18914 9122 896 746 4,7 8,2 ‐4,2 ‐4,7 ‐5,9 ‐6,9 ‐2,1 ‐2,4 Age‐group: 15 ‐ 24 years 25 ‐ 44 years 45 ‐ 64 years 65 ‐ 74 years 75 ‐ 84 years 17 1392 11256 9647 5621 1 21 205 529 660 5,9 1,5 1,8 5,5 11,7 10 1279 10324 9492 7112 0 20 226 453 877 0,0 1,6 2,2 4,8 12,3 14 1132 9623 8317 6936 0 18 185 334 664 0 1,6 1,9 4,0 9,6 ‐17,6 ‐18,7 ‐14,5 ‐13,8 23,4 ‐ ‐14,3 ‐9,8 ‐36,9 0,6 ‐ 6,7 5,6 ‐27,3 ‐17,9 1376 337 85 and up Source: ACSS, DRG database 24,5 1879 436 23,2 2014 441 21,9 46,4 30,9 ‐10,6 When combining gender with the age group, the number of IHD‐related hospitalizations in males is quite a bit higher than in females in the youngest age groups; however, as age increases, this difference diminishes, and the number of hospitalizations is higher in women in the 85‐and‐over age group. The same pattern occurs in IHD‐related in‐patient deaths. The IHD‐related intra‐ Application for the 2010 SCML Award 87 Results 2 hospital lethality rate shows even higher figures in women, in every age group, except in the 15‐ 24 and 45‐64 age groups, whose figures are identical to those for men. Figure 32 Number of hospitalizations and hospitalization deaths due to Ischemic Heart Disease (ICD 9: 410‐414), by gender and age group Source: ACSS, DRG database Table 40 Number of hospitalizations, hospitalization deaths and intra‐hospital lethality rate due to Ischemic Heart Disease (ICD 9: 410‐414), by to gender and age group 2000 2004 2008 29309 1753 Let. Hosp. Death (%) 6,0 30096 2012 M 19733 F 9576 952 801 4,8 8,4 19547 10549 1040 972 5,3 9,2 18914 9122 896 746 4,7 8,2 ‐4,2 ‐4,7 ‐5,9 ‐6,9 7,7 0,0 9 1 0 0 0,0 0,0 12 2 0 0 0 0 ‐7,7 ‐50,0 ‐ ‐ ‐ ‐ 1,4 2,2 1095 184 17 3 1,6 1,6 948 184 14 4 1,5 2,2 ‐21,7 1,1 ‐17,6 ‐ 7,1 ‐ 1,7 2,1 8045 2279 161 65 2,0 2,9 7625 1998 148 37 1,9 1,9 ‐13,1 ‐19,4 ‐3,3 ‐28,8 11,8 ‐9,5 5,2 6,1 6148 3344 270 183 4,4 5,5 5627 2690 210 124 3,7 4,6 ‐9,7 ‐21,2 ‐34,6 ‐28,8 ‐40,4 ‐24,6 11,3 12,3 3575 3537 427 450 11,9 12,7 3881 3055 357 307 9,2 10,1 30,5 15,4 6,6 ‐5,5 ‐18,6 ‐17,9 23,7 25,0 675 1204 165 271 24,4 22,5 821 1193 167 274 20,3 23 55,8 40,5 33,6 29,2 ‐14,3 ‐8,0 Hosp. Death. Total Let. (%) 6,7 Hosp. Death 28036 1642 Let. (%) 5,9 Variation 2000‐2008 (%) Let. Hosp. Death (%) ‐4,3 ‐6,3 ‐1,7 Gender: Gender and age‐group: 15 ‐ 24 years M 13 1 F 4 0 25 ‐ 44 years M 1210 17 F 182 4 45 ‐ 64 years M 8778 153 F 2478 52 65 ‐ 74 years M 6232 321 F 3415 208 75 ‐ 84 years M 2973 335 F 2648 325 85 and up M 527 125 F 849 212 Source: ACSS, DRG database Application for the 2010 SCML Award 88 ‐2,1 ‐2,4 Results 2 Place of residence The trend toward a decrease in IHD‐related hospitalizations occurring in Mainland Portugal, from 2000 to 2008, did not occur in every Region. There were increases In the Centro, Alentejo and Algarve Regions, with decreases in the Norte and Lisboa e Vale do Tejo. A similar pattern was identified in IHD‐related in‐patient deaths. As concerns the intra‐hospital lethality rate, the lowest figures occurred in the Norte and the Alentejo (5,4% for both), with the highest figures occurring in Lisboa e Vale do Tejo (6,4%). From 2000 to 2008, there were relative decreases in the intra‐hospital lethality rate in the Algarve (17,1%) and in the Centro (5,2%), while figures remained constant in the other Regions. Table 41 Number of hospitalizations, hospitalization deaths and intra‐hospital lethality rate due to Ischemic Heart Disease (CID 9: 410‐414), by place of residence (NUT II, pursuant to D.L. n. º 317/99, date 11 August) 2000 Total 29309 1753 Let. (%) 6,0 NUT II Norte Centro LVT Alentejo Algarve 7763 4166 13793 1992 1093 419 243 880 108 76 5,4 5,8 6,4 5,4 7,0 502 27 Unknown Source: ACSS, DRG database 5,4 Hosp. Death. 1642 Let. (%) 5,9 Variation 2000‐2008 (%) Let. Hosp. Death (%) ‐4,3 ‐6,3 ‐1,7 7572 4776 11711 2158 1429 406 265 755 116 83 5,4 5,5 6,4 5,4 5,8 ‐2,5 14,6 ‐15,1 8,3 30,7 ‐3,1 9,1 ‐14,2 7,4 9,2 0,0 ‐5,2 0,0 0,0 ‐17,1 390 17 4,4 ‐22,3 ‐37,0 ‐18,5 2004 2008 30096 2012 Let. (%) 6,7 28036 7870 499 5017 272 13740 1020 1916 125 1249 82 6,3 5,4 7,4 6,5 6,6 4,6 Hosp. Death 304 14 Hosp. Death The IHD‐related intra‐hospital lethality rate tends to be higher in the NUT of the interior of Portugal and in the Greater Lisbon area. In 2008, the highest figure occurred in Beira Interior Sul (10,0%), with the lowest occurring in Cávado (3,6%). From 2000 to 2008, there were decreases in the intra‐hospital lethality rate in 16 of the 28 NUT III (see Annex 18). Application for the 2010 SCML Award 89 Results 2 Figure 33 Intra‐hospital lethality rate due to Ischemic Heart Disease (ICD 9: 410‐414), by place of residence (NUT III) Source: ACSS, DRG database Place of hospitalization From 2000 to 2008, hospitals in the Algarve Health Region achieved the highest relative increase in the number of IHD‐related hospitalizations (60,2%) and in the number of in‐patient deaths due to this disease (14,9%). By contrast, Lisboa e Vale do Tejo obtained the biggest decrease, both in hospitalizations (13,4%) and in deaths (14,3%). Table 42 Number of hospitalizations, hospitalization deaths and intra‐hospital lethality rate due to Ischemic Heart Disease (ICD 9: 410‐414), by place of hospitalization (Health Region) 2000 Let. Hosp. Death. (%) 6,7 28036 1642 Let. (%) 5,9 Variation 2000‐2008 (%) Let. Hosp. Death. (%) ‐4,3 ‐6,3 ‐1,7 2004 2008 Total 29309 1753 Let. Hosp. Death. (%) 6,0 30096 2012 Health region: Norte Centro LVT Alentejo 7679 4774 14537 1380 415 261 908 95 5,4 5,5 6,2 6,9 7550 5437 14468 1391 479 305 1046 101 6,3 5,6 7,2 7,3 7373 5078 12583 1498 401 279 778 99 5,4 5,5 6,2 6,6 ‐4,0 6,4 ‐13,4 8,6 ‐3,4 6,9 ‐14,3 4,2 0,0 0,0 0,0 ‐4,3 939 74 Algarve Source: ACSS, DRG database 7,9 1250 81 6,5 1504 85 5,7 60,2 14,9 ‐27,8 Hosp. Death. Application for the 2010 SCML Award 90 Results 2 There were small fluctuations in the intra‐hospital lethality rate in every Region throughout the years being analyzed, except in the Alentejo and the Algarve, which achieved a decrease of 4,3% and 27,8%. Figure 34 Proportion of surviving and deceased (intra‐hospital lethality) in‐patients due to Ischemic Heart Disease (ICD 9: 410‐414), by place of hospitalization (Health Region) Source: ACSS, DRG database Profile of hospitalization due to Ischemic Heart Disease In 2008, the profile of an IHD‐related male in‐patient was as follows: median age: 66; related diagnoses: essential hypertension, disorders of lipoid metabolism, other forms of chronic ischemic heart disease, diabetes and other postprocedural states. When dealing with a hospitalization resulting in death, the median age rises to 77, with the following related diagnoses: cardiac dysrhythmias, essential hypertension, diabetes, other forms of chronic ischemic heart disease and heart failure. Application for the 2010 SCML Award 91 Results 2 Table 43 Profile of Male In‐patient (with discharge from the hospital or death) due to Ischemic Heart Disease (ICD 9: 410‐414) Median age: Most frequent related dignosis 1.º 2.º 3.º 4.º Survived Deceased 66 77 Essential hypertension Cardiac dysrhythmias Disorders of lipoid metabolism Other forms of chronic ischemic heart disease Essential hypertension Diabetes 5.º Other postprocedural states Source: ACSS, DRG database Diabetes Other forms of chronic ischemic heart disease Heart failure For its part, the profile of an IHD‐related female in‐patient is as follows: median age: 73; related diagnoses: essential hypertension, disorders of lipoid metabolism, diabetes, other forms of chronic ischemic heart disease and other postprocedural states. When dealing with a hospitalization resulting in death, the median age is 82, with the following related diagnoses: cardiac dysrhythmias, diabetes, essential hypertension, heart failure and other forms of chronic ischemic heart disease. Table 44 Profile of Female In‐patient (with discharge from the hospital or death) due to Ischemic Heart Disease (ICD 9: 410‐414). Median age: Survived deceased 73 82 Most frequent related dignosis 1.º Hipertensão arterial Cardiac dysrhythmias 2.º Disorders of lipoid metabolism Diabetes 3.º Diabetes Other forms of chronic ischemic heart 4.º disease 5.º Other postprocedural states Source: ACSS, DRG database Application for the 2010 SCML Award Hipertensão arterial Heart failure Other forms of chronic ischemic heart disease 92 Results 2 5.1.2.2. Stroke Gender and age group The number of stroke related hospitalizations achieved a relative increase of 15,4%, from 2000 to 2008, with the number of hospitalizations rising from 24.340 to 28.089. During the same period, the number of in‐patient deaths due to this disease also increased (3,9%), with 4048 deaths in 2000 and 4204 in 2008. Likewise, in the same period there was a relative decrease of 9,8% in the intra‐hospital lethality rate, which reached 15% in 2008. The number of stroke related hospitalizations is slightly higher in males: there were 14.386 male and 13.703 female in‐patients. However, there were more female than male in‐patient deaths (2171 and 2033, respectively). In this regard, the intra‐hospital lethality rate is higher in women (15,8%) compared to that obtained for men (14,1%). Both hospitalizations and stroke related in‐patient deaths increase with age, with the highest figure achieved in the 75 to 84 age group (2008: 10.132 and 1631, respectively). The trend toward an increase in the number of hospitalizations for all ages, from 2000 to 2008, does not occur the same way, when analyzing age groups separately. The 45‐64, 75‐84 and 85 and over age groups show relative increases (23,6% and 63,2%, respectively), with decreases in the other age groups. There was also an increase in stroke related in‐patient deaths in the highest age groups (75‐84 and 85 and over age groups: 3,6% and 63,2%, respectively), with a decrease in the other age groups. As concerns the intra‐hospital lethality rate, there was a reduction in every age group, except in the 25‐44 age group, which achieved a relative increase of 2,7%. Application for the 2010 SCML Award 93 Results 2 Table 45 Number of hospitalizations, hospitalization deaths and intra‐hospital lethality rate due to stroke (ICD 9: 430‐434), by age group 2000 3909 Let. (%) 15,5 Variation 2000‐2008 (%) Let. Let. Hosp. Death. Hosp. Death. (%) (%) 28089 4204 15,0 15,4 3,9 ‐9,6 2004 2008 Total 24340 4048 Let. (%) 16,6 Gender: M F 12411 11929 2005 2043 16,2 17,1 12804 12417 1880 2029 14,7 16,3 14386 13703 2033 2171 14,1 15,8 15,9 14,9 1,4 6,3 ‐13,0 ‐7,6 Age‐group:: 15 ‐ 24 years 25 ‐ 44 years 45 ‐ 64 years 65 ‐ 74 years 75 ‐ 84 years 78 833 5123 7239 8199 6 92 616 1035 1574 7,7 11,0 12,0 14,3 19,2 65 803 4996 7085 8952 5 84 548 918 1558 7,7 10,5 11,0 13,0 17,4 52 807 5321 7095 10132 5 91 507 806 1631 9,6 11,3 9,5 11,4 16,1 ‐33,3 ‐3,1 3,9 ‐2,0 23,6 ‐ ‐1,1 ‐17,7 ‐22,1 3,6 ‐ 2,7 ‐20,8 ‐20,3 ‐16,1 2868 725 85 and up Source: ACSS, DRG database 25,3 3320 796 24,0 4682 1164 24,9 63,2 60,6 ‐1,6 Hosp. Death. Hosp. Death. 25221 Generally speaking, the number of stroke related hospitalizations is higher in men; however, this does not occur in every age group. In the 75‐84 and 85 and over age groups, female hospitalizations were higher. The number of in‐patient deaths follows the same pattern, as there were more male in‐patient deaths in the youngest age groups, with female deaths in the two oldest age groups. The behavior of the intra‐hospital lethality rate is more irregular. In 2008, the rate is higher for men in the 15‐24, 24‐44 and 75‐84 age groups, whereas it is higher for women in the 45‐64, 65‐74 and 85 and over age groups. From 2000 to 2008, the number of stroke related hospitalizations decreased for both genders in the 15‐24 age group; that number decreased for males and rose for females in the 25‐44 age group; this rose for males and declined for females in the 45‐64 and 65‐74 age groups; it increased for both genders in the oldest age groups (75 to 84, and 85 and over). Application for the 2010 SCML Award 94 Results 2 Figure 35 Number of hospitalizations and hospitalization deaths due to stroke (ICD9: 430‐434), by gender and age group Source: ACSS, DRG database As concerns stroke related in‐patient deaths, an increase for both genders was noticed, from 2000 to 2008, in the oldest age groups (ages 75‐84 and 85 and over), along with an increase in intermediate groups (ages 45‐64 and 65‐74). In young adults (ages 25‐44), the number of male in‐patient deaths increased, while female in‐patient deaths decreased. The change in the stokes related intra‐hospital lethality rate shows a decrease, from 2000 to 2008, in every age group for both genders, except the 15‐24 age group, which showed increased lethality in male in‐patients. Application for the 2010 SCML Award 95 Results 2 Table 46 Number of hospitalizations, hospitalization deaths and intra‐hospital lethality rate due to stroke (ICD 9: 430‐434), by gender and age group 2000 2004 2008 Variation 2000‐2008 (%) Hosp. Death. Total 24340 4048 Let. Let. Let. Hosp. Death Hosp. Death Hosp. Death Let. (%) (%) (%) (%) 16,6 25221 3909 15,5 28089 4204 15 15,4 3,9 ‐9,6 Gender: H M 12411 2005 11929 2043 16,2 12804 1880 14,7 17,1 12417 2029 16,3 Gender and age‐group: 14386 2033 14,1 13703 2171 15,8 15,9 14,9 1,4 6,3 ‐13,0 ‐7,6 H M 43 35 3 3 7,0 8,6 34 31 2 3 5,9 9,7 31 21 3 2 9,7 9,5 ‐27,9 ‐40,0 ‐ ‐ ‐ ‐ H M 474 359 50 42 10,5 11,7 435 368 51 33 11,7 9,0 441 366 60 31 13,6 8,5 ‐7,0 1,9 20,0 ‐26,2 29,5 ‐27,4 H 3224 M 1899 386 230 12,0 12,1 3118 1878 353 195 11,3 10,4 3559 1762 336 171 9,4 9,7 10,4 ‐7,2 ‐13,0 ‐25,7 ‐21,7 ‐19,8 H 4069 M 3170 591 444 14,5 14,0 4142 2943 535 383 12,9 13,0 4212 2883 475 331 11,3 11,5 3,5 ‐9,1 ‐19,6 ‐25,5 ‐22,1 ‐17,9 H 3688 M 4511 749 825 20,3 18,3 3986 4966 676 882 17,0 17,8 4618 5514 782 849 16,9 15,4 25,2 22,2 4,4 2,9 ‐16,7 ‐15,8 913 226 24,8 1089 263 24,2 1525 377 24,7 67,0 66,8 ‐0,4 M 1955 499 Source: ACSS, DRG database 25,5 2231 533 23,9 3157 787 24,9 61,5 57,7 ‐2,4 15 ‐ 24 years 25 ‐ 44 years 45 ‐ 64 years 65 ‐ 74 years 75 ‐ 84 years 85 and up H Place of residence The trend toward an increase in the number of stroke related hospitalizations, which occurred in Mainland Portugal between 2000 and 2008, also took place in every Region, with figures ranging from 136,9% for the Algarve and 3,0% for the Centro Region. The change in the number of stroke related in‐patient deaths in the Regions showed a greater discrepancy, with increases in the Lisboa e Vale do Tejo and Algarve Regions (16,9% and 125,9%, respectively) and decreases in the Norte (3,2%), Centro (11,8%) and Alentejo (0,4%) Regions. Application for the 2010 SCML Award 96 Results 2 The stroke related intra‐hospital lethality rate decreased, from 2000 to 2008, in every Region, with the biggest decrease occurring in the Center (14,5%) and the smallest in the Algarve (4,8%) Regions. Table 47 Number hospitalizations, hospitalization deaths and intra‐hospital lethality rate due to stroke (ICD 9: 430‐434), by place of residence (NUT II, pursuant to D.L. n. º 317/99, date 11 August) 2000 Hosp. Total 24340 2004 2008 Variation 2000‐2008 (%) Death. Let. (%) Hosp. Death Let. (%) Hosp. Death Let. (%) Hosp. Death Let. (%) 4048 16,6 25221 3909 15,5 28089 4204 15,0 15,4 NUT II Norte 8683 1331 Centro 5553 1070 LVT 7875 1260 Alentejo 1637 278 Algarve 434 81 Unknown 158 28 Source: ACSS, DRG database 3,9 15,3 19,3 16,0 17,0 18,7 17,7 8930 1296 5907 914 8006 1289 1781 294 461 95 136 21 14,5 15,5 16,1 16,5 20,6 15,4 9216 5720 10042 1835 1028 248 1288 944 1473 277 183 39 14,0 16,5 14,7 15,1 17,8 15,7 6,1 ‐3,2 3,0 ‐11,8 27,5 16,9 12,1 ‐0,4 136,9 125,9 57,0 39,3 ‐9,6 ‐8,5 ‐14,5 ‐8,1 ‐11,2 ‐4,8 ‐11,3 The stroke related intra‐hospital lethality rate tends to be higher in the NUT of the interior of Portugal and in the Algarve. In 2008, the NUT III Pinhal Interior Sul obtained the highest figure (28,7%), with the lowest achieved by Oeste (12,1%). From 2000 to 2008, there were decreases in the intra‐hospital lethality rate in 21 of the 28 NUT III (see Annex 19). Figure 36 Stroke related Intra‐hospital lethality rate (ICD 9: 430‐434), by place of residence (NUT III) Source: ACSS, DRG database Application for the 2010 SCML Award 97 Results 2 Place of hospitalization From 2000 to 2008, there were increases in the number of stroke related admissions to hospitals in every Health Region, with figures ranging from 1,7% in the Centro to 191,4% in the Algarve Regions. The trend toward an increase in the number of in‐patient deaths due to this disease, as identified in Mainland Portugal, is not replicated in every Health Region, since there were decreases (3,9% and 11,1%, respectively) in the Norte and Centro Regions. Relative increases range from 142,1% for the Algarve and 13,7% for the Lisboa e Vale do Tejo Regions. Table 48 Number of hospitalizations, hospitalization deaths and intra‐hospital lethality rate due to Cerebral Vascular Accident (ICD 9: 430‐434), by place of hospitalization (Health Region) 4048 Let. (%) 16,6 Variation 2000‐2008 (%) Let. Let. Let. Hosp. Death. Hosp. Death. Hosp. Death. (%) (%) (%) 25221 3909 15,5 28089 4204 15 15,4 3,9 ‐9,6 1309 1090 1375 198 15,4 18,7 16,2 16,4 8700 6210 8474 1446 1257 970 1361 233 347 76 Algarve Source: ACSS, DRG database 21,9 391 88 2000 Hosp. Death. Total 24340 Health region: Norte Centro LVT Alentejo 8481 5844 8464 1204 2004 2008 14,4 9056 15,6 5944 16,1 10559 16,1 1519 1258 969 1564 229 13,9 16,3 14,8 15,1 6,8 1,7 24,8 26,2 ‐3,9 ‐11,1 13,7 15,7 ‐9,9 ‐12,6 ‐8,9 ‐8,2 22,5 184 18,2 191,4 142,1 ‐16,9 1011 The stroke related intra‐hospital lethality rate decreased in the hospitals of every Health Region. The highest figure occurred in the Algarve (‐16,9%), with the lowest occurring in Alentejo (‐8,2%). Application for the 2010 SCML Award 98 Results 2 Figure 37 Proportion of surviving and deceased (intra‐hospital lethality) in‐patients due to stroke (ICD 9: 430‐434), by place of hospitalization (Health Region) Source: ACSS, DRG database Profile of the stroke‐related in‐patient In 2008, the profile of a stroke‐related male in‐patient was as follows: median age: 72; and related diagnoses: essential hypertension; disorders of lipoid metabolism; diabetes; cardiac dysrhythmias; and late effects of cerebrovascular disease. When dealing with a hospitalization resulting in death, the median age increases to 76, and the related diagnoses include: essential hypertension, cardiac dysrhythmias, diabetes, general symptoms and late effects of cerebrovascular disease. Application for the 2010 SCML Award 99 Results 2 Table 49 Profile of Male In‐patient (with discharge from the hospital or death) due to stroke (ICD 9: 430‐434). Median age: Survived Deceased 72 76 Most frequent related dignosis: 1.º Essential hypertension Essential hypertension 2.º Disorders of lipoid metabolism Cardiac dysrhythmias 3.º Diabetes Diabetes 4.º Cardiac dysrhythmias General symptoms 5.º Source: ACSS, DRG database Late effects of cerebrovascular disease Late effects of cerebrovascular disease The profile of a stroke‐related female in‐patient, in 2008, is as follows: median age: 77; and related diagnoses: essential hypertension; disorders of lipoid metabolism; diabetes; cardiac dysrhythmias; and late effects of cerebrovascular disease. When dealing with a hospitalization resulting in death, the woman’s median age would be 82, with the following main related diagnoses: essential hypertension; diabetes; cardiac dysrhythmias, general symptoms and disorders of fluid, electrolyte, and acid‐base balance. Table 50 Profile of Female In‐patient (discharge from the hospital or death) due to stroke (ICD 9: 430‐ 434). Median age: Survived Deceased 77 82 Most frequent related dignosis 1.º Essential hypertension Essential hypertension 2.º Disorders of lipoid metabolism Cardiac dysrhythmias 3.º Diabetes Diabetes 4.º Cardiac dysrhythmias 5.º Late effects of cerebrovascular disease General symptoms Disorders of fluid, electrolyte, and acid‐ base balance Source: ACSS, DRG database Application for the 2010 SCML Award 100 Results 2 Summary Ischemic heart diseases (28.036 hospitalizations in 2008) • Represent 20,5% of all hospitalizations due to diseases of the circulatory systems and 15,2% of the hospitalization death • Slight decrease of the intra‐hospital lethality rate between 2000 and 2008 • The 45 to 64 age‐group has the higher values of hospitalizations, and the 75 to 84 age‐ group the highest figures of hospitalization deaths • There are more hospitalizations in men but the lethality rate is higher in women • The intra‐hospital lethality is higher in LVT • The most hospitalizations deaths are related to cardiac dysrhythmia. Stroke (28.089 hospitalizations in 2008) • Represent 20,5% of all hospitalizations due to diseases of the circulatory systems and 38,8% of the hospitalization death • Intra‐hospital lethality rate decreased 9,6% between 200 and 2008 • The 75 to 84 age‐group has the higher values of hospitalizations and hospitalizations deaths • There are more hospitalizations in men but the intra‐hospital lethality rate is higher in women • The intra‐hospital lethality is higher in Algarve • The most hospitalizations and hospitalization deaths are related to essential hypertension Application for the 2010 SCML Award 101 Results 2 5.1.3. Cancer From 2000 to 2008, there was a relative increase of 31,0% in the number of hospital admissions for cancer, which went from 56.050 to 73.413 hospitalizations. Likewise, the number of in‐ patient deaths rose 27,2% (from 8.227 to 10.465). For its part, the intra‐hospital lethality rate due to this disease decreased from 2000 to 2004, the year when the lowest figure was achieved (14,1%), but rose slightly in 2008 (14,3%); even so, figures were lower than initial values. The highest figures for hospitalizations and hospitalizations deaths were achieved in the 45‐64 age group. The intra‐hospital lethality rate showed a different behavior, as it increased with age, with the highest figure obtained in the 85 and over age group. The number of hospitalizations for cancer increased in every age group, except in the 15‐24 age group, which achieved a relative decrease of 20,6%. The most important increase occurred in the 85 and over age group (77,0%). The number of in‐patient deaths decreased in younger age groups (15‐24: 29,5%; and 25‐44: 12,3%) and increased in the others. The intra‐hospital lethality rate decreased in every age group, except the 75 to 84 age group (1,5%). The 25‐44 age group achieved the biggest drop (27,5%). Table 51 Number of hospitalizations, hospitalization deaths and intra‐hospital lethality rate due to Cancer (ICD 9: 140‐208), by age group 2000 8227 Let. (%) 14,7 67360 4856 3371 16,1 13,0 61 497 2544 2536 1968 621 7,0 9,9 12,9 15,2 17,7 23,3 Hosp. Death. Total 56050 Gender: M F 30193 25857 Age‐group: 15 ‐ 24 years 867 25 ‐ 44 years 5009 45 ‐ 64 years 19715 65 ‐ 74 years 16682 75 ‐ 84 years 11114 85 and up 2663 Source: ACSS, DRG database 2004 Variation 2000‐2008 (%) Let. Let. Death. Hosp. Death. (%) (%) 10465 14,3 31,0 27,2 ‐2,9 2008 9529 Let. (%) 14,1 73413 35607 31753 5636 3893 15,8 12,3 38298 35115 6312 4153 16,5 11,8 26,8 35,8 30,0 23,2 2,5 ‐9,3 882 6051 22909 19294 14817 3407 55 484 2764 2892 2606 728 6,2 8,0 12,1 15,0 17,6 21,4 688 6063 25171 19615 17162 4714 43 436 3088 2849 3085 964 6,3 7,2 12,3 14,5 18,0 20,4 ‐20,6 21,0 27,7 17,6 54,4 77,0 ‐29,5 ‐12,3 21,4 12,3 56,8 55,2 ‐11,2 ‐27,5 ‐4,9 ‐4,5 1,5 ‐12,3 Hosp. Death. Hosp. Application for the 2010 SCML Award 102 Results 2 In 2008, the number of hospitalizations for traceable cancers ‐ female breast, cervix uteri and colo‐rectal ‐ together account for around 23% of all hospitalizations for cancer and some 17% of all in‐patient deaths caused by this disease. The contribution of each traceable tumor toward the total of cancer is, however, uneven. Colo‐ rectal cancer, which occurs most often, in 2008 accounted for 12,4% of hospitalizations and 13,1% of deaths; cervix uteri cancer represented 1,4% of hospitalizations and 1% of deaths; women’s breast cancer comprises 9,7% of hospitalizations and 3,6% of deaths. Figure 38 Percentage of hospitalizations and hospitalization deaths due to selected cancers, of the total of Cancer Source: ACSS, DRG database Table 52 Percentage of hospitalizations and hospitalization deaths due to selected cancers relative to the total numbers of cancer. 2000 Hosp. n.º % 2004 Death. n.º % Hosp. n.º % 2008 Death. n.º % Hosp. n.º % Death. n.º % Cancers Female Breast Cervix uteri 56050 100,0 8227 100,0 67360 100,0 5353 9,6 464 5,6 6426 9,5 1042 1,9 103 1,3 1211 1,8 9529 100,0 73413 100,0 10465 100,0 427 4,5 7112 9,7 373 3,6 105 1,1 1006 1,4 105 1,0 Colo‐rectal 7811 13,9 1004 12,2 8741 13,0 1181 12,4 9137 12,4 1373 13,1 Prostate 2770 4,9 353 4,3 3206 4,8 403 4,2 3135 4,3 452 4,3 Trachea/bronchus/lung 4483 Source: ACSS, DRG database 8,0 1153 14,0 4639 6,9 1414 14,8 4964 6,8 1618 15,5 Application for the 2010 SCML Award 103 Results 2 Female Breast Cancer From 2000 to 2008, there was a relative increase of 32,9% in the number of hospital admissions due to women’s breast cancer and a decrease in the number of in‐patient deaths (19,6%) and in the intra‐hospital lethality rate (39,5%). The trend toward an increase in the number of hospitalizations due to women’s breast cancer, as previously identified, for the total number of cases examined, also manifests itself in every age group, with particular emphasis on the 75‐84 age group (50,2%). The trend toward a decrease in the number of female in‐patient deaths did not occur in the 75‐84 and 85 and over age groups. The intra‐hospital lethality rate achieved positive change, from 2000 to 2008, as it decreased in every age group. Table 53 Number of hospitalizations, hospitalization deaths and intra‐hospital lethality rate due to Female Breast Cancer (ICD 9: 174), by age group 2000 2004 Total 5353 464 Let. (%) 8,7 Age‐group: 15 – 24 years 25 ‐ 44 years 45 ‐ 64 years 65 ‐ 74 years 75 ‐ 84 years 11 758 2591 1211 648 0 56 217 105 64 134 22 85 and up Source: ACSS, DRG database Hosp. Death. Variation 2000‐2008 (%) Let. Let. Death Hosp. Death (%) (%) 373 5,2 32,9 ‐19,6 ‐39,5 2008 6426 427 Let. (%) 6,6 ‐ 7,4 8,4 8,7 9,9 9 1017 3020 1444 795 1 53 177 104 76 ‐ 5,2 5,9 7,2 9,6 15 1060 3391 1475 973 1 27 158 78 86 ‐ 2,5 4,7 5,3 8,8 36,4 39,8 30,9 21,8 50,2 ‐ ‐51,8 ‐27,2 ‐25,7 34,4 ‐ ‐65,5 ‐44,4 ‐39,0 ‐10,5 16,4 141 16 11,3 198 23 11,6 47,8 4,5 ‐29,2 Hosp. Death Hosp. 7112 Between 2000 and 2008 the number of hospitalizations for female breast cancer increased in every NUT II, while the Norte’s figures nearly doubled (2000: 1140; 2008: 2172). The change in the number of female in‐patient deaths due to this disease was quite asymmetrical in the various Regions: it increased in the Centro, while holding steady in the Norte and decreasing in the others. The intra‐hospital lethality rate shows a positive change in every Region, with decreases ranging from 47,5% (Norte) and 7,6% (Centro). Application for the 2010 SCML Award 104 Results 2 Table 54 Number of hospitalizations, hospitalization deaths and intra‐hospital lethality rate due to Female Breast Cancer (ICD 9: 174), by place of residence (NUT II, pursuant to D.L. n. º 317/99, date 11 August) 2000 2004 Hosp. Death. Total 5353 464 Let. (%) 8,7 NUT II Norte Centro LVT Alentejo Algarve 1140 1047 2105 315 192 74 69 225 40 17 39 554 Unknown Source: ACSS, DRG database 373 Let. (%) 5,2 Variation 2000‐2008 (%) Let. Hosp. Death (%) 32,9 ‐19,6 ‐39,5 2008 6426 427 Let. (%) 6,6 6,5 6,6 10,7 12,7 8,9 1364 1294 2248 363 241 67 100 177 23 11 4,9 7,7 7,9 6,3 4,6 2172 1149 2677 376 314 74 70 165 28 16 3,4 6,1 6,2 7,4 5,1 90,5 9,7 27,2 19,4 63,5 0,0 1,4 ‐26,7 ‐30,0 ‐5,9 ‐47,5 ‐7,6 ‐42,3 ‐41,4 ‐42,5 7,0 916 49 5,3 424 20 4,7 ‐23,5 ‐48,7 ‐33,0 Hosp. Death Hosp. Death 7112 The intra‐hospital lethality rate tends to be higher in NUTs III in the interior of Portugal. In 2008, the highest figure was achieved in the NUT III of Cova da Beira (15,2%) with the lowest achieved in Entre Douro e Vouga (1,8%). From 2000 to 2008, only three NUT III achieved increases in the intra‐hospital lethality rate, while the other twenty‐five showed positive change (decrease). Figure 39 Intra‐hospital Lethality Rate due to Female Breast Cancer‐related (ICD9: 174), by place of residence (NUT III) Source: ACSS, DRG database Application for the 2010 SCML Award 105 Results 2 When the occurrences – hospitalizations and deaths – are analyzed by place of hospitalization (Health Region), it is noticed that the trend toward change from 2000 to 2008 is very similar to the analysis by place of residence. Hospitalizations increased in every Health Region; the number of deaths decreased in a few Regions (see Annex 20). Table 55 Number of hospitalizations, hospitalization deaths and intra‐hospital lethality rate due to Female Breast Cancer (ICD 9: 174), by place of hospitalization (Health Region) 2000 2004 Hosp. Death. Total 5353 464 Let. (%) 8,7 Health region: Norte Centro LVT Alentejo 1653 1171 2147 220 107 75 237 31 14 162 Algarve Source: ACSS, DRG database 2008 6426 427 Let. (%) 6,6 6,5 6,4 11,0 14,1 2224 1423 2284 276 114 102 185 15 8,6 219 11 Hosp. Death. Variation 2000‐2008 (%) Let. Hosp. Death. (%) 32,9 ‐19,6 ‐39,5 7112 373 Let. (%) 5,2 5,1 7,2 8,1 5,4 2481 1282 2772 283 85 77 169 27 3,4 6,0 6,1 9,5 50,1 9,5 29,1 28,6 ‐20,6 2,7 ‐28,7 ‐12,9 ‐47,1 ‐6,2 ‐44,8 ‐32,3 5,0 294 15 5,1 81,5 7,1 ‐41,0 Hosp. Death. From 2000 to 2008, the intra‐hospital lethality rate decreased in every Region, especially in the Norte (47,1%), Lisboa e Vale do Tejo (44,8%) and the Algarve (41%) Regions. Application for the 2010 SCML Award 106 Results 2 Figure 40 Proportion of surviving and deceased (intra‐hospital lethality) in‐patients due to Female Breast Cancer (ICD 9: 174), by place of hospitalization (Health Region) Source: ACSS, DRG database In 2008, the profile of a female in‐patient admitted for female breast cancer is as follows: median age: 59; and related diagnoses: essential hypertension, secondary and unspecified cancer of lymph nodes; diabetes; secondary cancer of other specified sites; and secondary cancer of the respiratory and digestive system. When dealing with a hospitalization resulting in death, the woman’s median age would be 65, with the following main related diagnoses: secondary cancer of the digestive and respiratory system; secondary cancer of other specified sites; diabetes; convalescence and palliative care; and secondary and unspecified cancer of lymph nodes. Application for the 2010 SCML Award 107 Results 2 Table 56 Profile of In‐patient (with discharge from the hospital or death) due to Female Breast Cancer (ICD 9: 174). Survived Deceased 59 65 Median age: Most frequent related dignosis 1.º Essential hypertension Secondary and unspecified cancer of lymph nodes 3.º Diabetes 4.º Secondary cancer of other specified sites Secondary cancer of the digestive and 5.º respiratory system Source: ACSS, DRG database 2.º Secondary cancer of the digestive and respiratory system Secondary cancer of other specified sites Diabetes Convalescence and palliative care Secondary and unspecified cancer of lymph nodes Cervical The number of cervix uteri cancer‐related hospitalizations fluctuated over the years, as it increased from 2000 to 2004, and then decreased in 2008 to figures that were lower than those originally achieved. The number of female in‐patient deaths due to this disease rose slightly from 2000 to 2004 and held steady in 2008. The intra‐hospital lethality rate increased overall from 2000 to 2008 (5,6%), but the lowest figure was achieved 2004. The distribution of cervix uteri‐related hospitalizations and in‐patient deaths by age group highlights the 45‐64 age group, which obtained the highest figures in both occurrences. For their part, the age groups at both extremes (15‐24 and 85 and over) achieved the lowest figures. The intra‐hospital lethality rate trends in rise with age, as the highest figures were obtained in the oldest age groups. The overall trend (2000‐2008) toward a decrease in the number of cervix uteri cancer‐related hospitalizations, as previously identified, does not occur in the 25‐44 (3,5%) and 45‐64 (3,6%) age groups. Also, the number of in‐patient deaths does not show increases in every age group, as the 65‐74 age group decreased 10,5%. The same thing occurred with regard to the intra‐hospital lethality rate, which decreased only in the 45‐64 age group (1,4%). Application for the 2010 SCML Award 108 Results 2 Table 57 Number of hospitalizations, in‐patient deaths and intra‐hospital lethality rate due to cervical cancer (ICD 9: 180), by age group 2000 Hosp. Total 1042 2004 Let. Death. (%) 103 9,9 Age‐group: 15 ‐ 24 years 2 0 25 ‐ 44 years 289 20 45 ‐ 64 years 475 47 65 ‐ 74 years 153 19 75 ‐ 84 years 100 13 85 and up 23 4 Source: ACSS, DRG database 1211 105 2 388 522 170 113 16 0 20 39 28 15 3 0,0 5,2 7,5 16,5 13,3 18,8 Hosp. Death. 0,0 6,9 9,9 12,4 13,0 17,4 2008 Let. (%) 8,7 Let. Hosp. Death. (%) 1006 105 10,4 8 299 492 110 81 16 0 21 48 17 16 3 0,0 7,0 9,8 15,5 19,8 18,8 Variation 2000‐2008 (%) Let. Hosp. Death. (%) ‐3,5 1,9 5,6 ‐ 3,5 3,6 ‐28,1 ‐19,0 ‐30,4 ‐ 5,0 2,1 ‐10,5 23,1 ‐ ‐ 1,5 ‐1,4 24,4 51,9 ‐ There are huge fluctuations between the distribution of occurrences by Region of residence, partly due to the fact that there are few cases. From 2000 to 2008, the number of hospitalizations achieved results ranging from relative decreases of 50% (the Alentejo) to increases of 16,2% (Norte); despite an increase in in‐patient deaths in nearly every Region (except the Alentejo), figures were triple in the Algarve and dropped quite sharply in the Alentejo; the intra‐hospital lethality rate also showed very dissimilar decreases and increases. Table 58 – Number hospitalizations, hospitalization deaths and intra‐hospital lethality rate due to cervical cancer (CID 9: 180), by place of residence (NUT II, pursuant to D.L. n. º 317/99, date 11 August) 2000 Hosp. Death. Total 1042 103 NUT II Norte 271 14 Centro 241 16 LVT 290 46 Alentejo 50 7 Algarve 39 3 Unknown 151 17 Source: ACSS, DRG database 2004 Let. (%) 9,9 5,2 6,6 15,9 14,0 7,7 11,3 Variation 2000‐2008 (%) Let. Let. Hosp. Death. Hosp. Death. (%) (%) 1006 105 10,4 ‐3,5 1,9 5,6 2008 Hosp. Death. Let. (%) 1211 105 8,7 330 213 297 32 84 255 17 22 46 1 4 15 5,2 10,3 15,5 3,1 4,8 5,9 315 178 320 25 37 131 21 17 47 2 9 9 6,7 9,6 14,7 8,0 24,3 6,9 16,2 ‐26,1 10,3 ‐50,0 ‐5,1 ‐13,2 50,0 29,0 6,3 43,9 2,2 ‐7,4 ‐ ‐ ‐ ‐ ‐47,1 ‐39,0 The change in the number of cervix uteri cancer‐related hospitalizations ranged from sharp decreases in the Alentejo (45,8%) and the increase in the Lisboa e Vale do Tejo (14,2%), while female in‐patient deaths due to this disease ranged from ‐23,3% in the Norte to 12,5% in the Centro. Application for the 2010 SCML Award 109 Results 2 Table 59 Number of hospitalizations, in‐patient deaths and intra‐hospital lethality rate due to cervical cancer (ICD 9: 180), by to place of hospitalization (Health Region) 2000 Hosp. Death. Total 1042 103 Health region: Norte 401 30 Centro 270 16 LVT 316 50 Alentejo 24 4 Algarve 31 3 Source: ACSS, DRG database 2004 Let. (%) 9,9 7,5 5,9 15,8 16,7 9,7 2008 Hosp. Death Let. (%) Hosp. Death 1211 105 8,7 1006 105 Let. (%) 10,4 560 233 346 13 59 28 24 50 0 3 5,0 10,3 14,5 0,0 5,1 398 206 361 13 28 23 18 54 1 9 5,8 8,7 15,0 7,7 32,1 Variation 2000‐2008 (%) Let. Hosp. Death (%) ‐3,5 1,9 5,6 ‐0,7 ‐23,7 14,2 ‐45,8 ‐9,7 ‐23,3 12,5 8,0 ‐ ‐ From 2000 to 2008, there was a very dissimilar change in the intra‐hospital lethality rate in Mainland Portugal, with the relative change ranging from ‐22,8% in the Norte to 47,5% in the Centro. The Alentejo and Algarve Regions achieved very low figures. Therefore, relative changes become pronounced over the years. Figure 41 Proportion of surviving and deceased (intra‐hospital lethality) in‐patients due to cervical cancer (ICD 9: 180), by place of hospitalization (Health Region) Source: ACSS, DRG database Application for the 2010 SCML Award 110 ‐22,8 47,5 ‐5,5 ‐ ‐ Results 2 In 2008, the profile of a female in‐patient admitted for cervix uteri cancer is as follows: median age: 51; and main related diagnoses: secondary cancer of other specified sites; secondary cancer of the digestive and respiratory system; essential hypertension; other and unspecified anemias; and secondary and unspecified cancer of lymph nodes. When dealing with a hospitalization resulting in death, the woman’s median age rises to 54, with the following main related diagnoses: secondary cancer of the digestive and respiratory system; secondary cancer of other specified sites; other and unspecified anemias; secondary and unspecified cancer of lymph nodes; and convalescence and palliative care. Table 60 Profile of In‐patient (with discharge from the hospital or death) due to cervical cancer (ICD 9: 180) Median age: Survived Deceased 51 54 Most frequent related dignosis 1.º Secondary cancer of other specified sites Secondary cancer of the digestive and respiratory system 3.º Secondary cancer of the digestive and respiratory system Essential hypertension 4.º Other and unspecified anemias 2.º Secondary and unspecified cancer of lymph nodes Source: ACSS, DRG database 5.º Secondary cancer of other specified sites Other and unspecified anemias Secondary and unspecified cancer of lymph nodes Convalescence and palliative care Colo‐rectal cancer From 2000 to 2008, there was a relative increase of 17,0% in the number of colo‐rectal cancer‐ related hospitalizations, which rose from 7811 to 9123. The number of hospitalization deaths rose at a higher rate, with a 36,8% increase (from 1004 to 1373 deaths). As would be expected, as a result of previous changes, there was a 16,9% increase in the intra‐hospital lethality rate. Both the number of colo‐rectal cancer‐related hospitalizations and in‐patient deaths as well as the intra‐hospital lethality rate are higher in men than in women, in all the years that were studied. Application for the 2010 SCML Award 111 Results 2 After analyzing the data by age groups, in 2008, it is noticed that hospitalizations most often occurred in the 65‐74 age group, followed by the 45‐64 and the 75‐84 age groups. The highest number of hospitalization deaths occurs in the 75‐84 age group, with the highest intra‐hospital lethality rate occurring in the 85 and over age group. The change (2000‐2008) in the number of colo‐rectal cancer‐related hospitalizations shows that the oldest age groups achieved the biggest increases. By contrast, the 15‐24 and 24‐44 age groups show hospitalizations decreased during the period being studied. The number of hospitalization deaths shows the same pattern, as it decreased only in the 25‐44 age group (26,7%), while achieving the biggest increase in the 85 and over age group (86,5%). The intra‐ hospital lethality rate decreased only in the 25‐44 age group (12,2%). Table 61 Number of hospitalizations, hospitalization deaths and intra‐hospital lethality rate due to Colo‐rectal Cancer (CID 9: 153; 154.0‐154.1), by age group Total Variation 2000‐2008 (%) Hosp. Death. Let. (%) Hosp. Death Let. (%) Hosp. Death Let. (%) Hosp. Death Let. (%) 7811 1004 12,9 8741 1181 13,5 9137 1373 15,0 17,0 36,8 16,9 Gender: M F 4489 3322 2000 2004 2008 582 422 13,0 12,7 5077 3664 706 475 13,9 13,0 5306 3831 804 569 15,2 14,9 18,2 15,3 38,1 34,8 16,9 16,9 Age‐group: 15 ‐ 24 years 16 0 25 ‐ 44 years 321 30 45 ‐ 64 years 2351 239 65 ‐ 74 years 2734 319 75 ‐ 84 years 1921 305 85 and up 468 111 Source: ACSS, DRG database 0,0 9,3 10,2 11,7 15,9 23,7 24 317 2463 2907 2449 581 1 34 236 353 406 151 4,2 10,7 9,6 12,1 16,6 26,0 8 268 2539 2864 2689 769 1 22 298 367 478 207 12,5 8,2 11,7 12,8 17,8 26,9 ‐50,0 ‐16,5 8,0 4,8 40,0 64,3 ‐ ‐26,7 24,7 15,0 56,7 86,5 ‐ ‐12,2 15,5 9,8 12,0 13,5 The number of hospitalizations colo‐rectal cancer‐related is only higher in females in the 85‐and‐ over age group. Also, the number of in‐patient deaths shows the same pattern. For its part, the intra‐hospital lethality rate shows similar figures for men and women in every age group. Application for the 2010 SCML Award 112 Results 2 Figure 42 Number of hospitalizations and hospitalization deaths due to Colo‐rectal Cancer (CID 9: 153; 154.0‐154.1), by age group and gender Source: ACSS, DRG database Table 62 Number of hospitalizations, hospitalization deaths and intra‐hospital lethality rate due to Colo‐rectal Cancer (CID 9: 153; 154.0‐154.1), by age group and gender Total 2000 2004 2008 Variation 2000‐2008 (%) Hosp. Death. Let. (%) Hosp. Death Let. (%) Hosp. Death Let. (%) Hosp. Death Let. (%) 7811 1004 12,9 8741 1181 13,5 9137 1373 15,0 17,0 36,8 16,9 Gender: H M 4489 3322 582 422 13,0 12,7 5077 3664 706 475 13,9 13,0 5306 3831 804 569 15,2 14,9 18,2 15,3 38,1 34,8 16,9 16,9 0,0 0,0 14 10 1 0 7,1 0,0 3 5 0 1 0,0 20,0 ‐57,1 ‐44,4 ‐ ‐ ‐ ‐ 8,9 9,9 159 158 19 15 11,9 9,5 137 131 11 11 8,0 8,4 ‐18,9 ‐13,8 ‐26,7 ‐26,7 ‐9,5 ‐14,9 9,9 10,5 1504 959 148 88 9,8 9,2 1531 1008 179 119 11,7 11,8 11,2 3,5 30,7 16,7 17,5 12,7 12,2 10,8 1831 1076 237 116 12,9 10,8 1770 1094 245 122 13,8 11,2 5,7 3,2 20,1 6,1 13,6 2,8 16,6 15,0 1305 1144 239 167 18,3 14,6 1524 1165 270 208 17,7 17,9 43,6 35,5 53,4 61,2 6,8 19,0 24,9 22,8 264 317 62 89 23,5 28,1 341 428 99 108 29,0 25,2 69,7 60,3 98,0 77,0 16,7 10,4 Gender and age‐group: 15 ‐ 24 years M 7 0 F 9 0 25 ‐ 44 years M 169 15 F 152 15 45 ‐ 64 years M 1377 137 F 974 102 65 ‐ 74 years M 1674 204 F 1060 115 75 ‐ 84 years M 1061 176 F 860 129 85 and over M 201 50 F 267 61 Source: ACSS, DRG database The trend (2000‐2008) toward the increase occurring in Mainland Portugal with regard to the number of colo‐rectal cancer‐related hospitalizations did not occur in an identical fashion in every Region. The Alentejo was the only Region, in 2008, with less hospitalizations than in 2000 Application for the 2010 SCML Award 113 Results 2 (relative decrease of 7,8%). The Norte and the Algarve Regions achieved the biggest relative increases (43,4% and 36,3%, respectively). The number of in‐patient deaths increased in every Region, with the biggest relative increases occurring in the Norte (68,7%) and in the Algarve (64,7%). The intra‐hospital lethality rate achieved negative change, with increases in every Region, from 2000 to 2008. Table 63 Number of hospitalization deaths and intra‐hospital lethality rate due to Colo‐rectal Cancer (CID 9: 153; 154.0‐154.1), by place of residence (NUT II, pursuant to D.L. n. º 317/99, date 11 August) 2000 2004 Total 7811 1004 Let. (%) 12,9 NUT II Norte Centro LVT Alentejo Algarve 1902 1817 2867 579 270 198 218 422 88 34 2008 8741 1181 Let. (%) 13,5 10,4 12,0 14,7 15,2 12,6 2197 1991 3184 586 336 245 247 499 93 42 44 11,7 Unknown 376 Source: ACSS, DRG database 447 55 Hosp. Death. Hosp. Death Variation 2000‐2008 (%) Let. Hosp. Death (%) 17,0 36,8 16,9 9137 1373 Let. (%) 15,0 11,2 12,4 15,7 15,9 12,5 2728 1900 3409 534 368 334 287 570 98 56 12,2 15,1 16,7 18,4 15,2 43,4 4,6 18,9 ‐7,8 36,3 68,7 31,7 35,1 11,4 64,7 17,6 25,9 13,6 20,7 20,8 12,3 198 28 14,1 ‐47,3 ‐36,4 20,8 Hosp. Death By distributing the intra‐hospital lethality rate by colo‐rectal cancer among the NUT III, the interior Alentejo and the Centro Regions are highlighted. In 2008, the lowest figure was achieved in the NUT III of Ave (9,4%), with the highest obtained at Lezíria do Tejo (23,4%) Application for the 2010 SCML Award 114 Results 2 Figure 43 Intra‐hospital lethality rate due to Colo‐rectal Cancer (ICD 9: 153; 154.0‐154.1), by place of residence (NUT III) Source: ACSS, DRG database From 2000 to 2008, there was an increase in the number of hospitalizations in every Region, except in the Alentejo, which achieved a relative decrease of 3,7%. The number of hospitalization deaths increased in every Region, with figures ranging from 83,3% in the Algarve to 9% in the Alentejo (see Annex 21). Table 64 Number of hospitalizations, hospitalization deaths and intra‐hospital lethality rate due to Colo‐rectal Cancer (ICD 9: 153; 154.0‐154.1), by place of hospitalization (Health Region) Let. Let. Hosp. Death. Hosp. Death. (%) (%) 12,9 8741 1181 13,5 9137 1373 Let. (%) 15,0 Variation 2000‐2008 (%) Let. Hosp. Death. (%) 17,0 36,8 16,9 10,6 12,1 14,5 16,9 11,7 12,2 14,9 16,8 19,1 15,6 28,1 6,1 16,9 ‐3,7 37,9 2000 Cancro do Cólon e Recto Total Hosp. Death. 7811 1004 Health region: Norte 2229 236 Centro 1872 227 LVT 2992 433 Alentejo 462 78 Algarve 256 30 Source: ACSS, DRG database 2004 2568 2059 3351 439 324 293 250 513 84 41 2008 11,4 12,1 15,3 19,1 12,7 2856 1986 3497 445 353 349 295 589 85 55 47,9 30,0 36,0 9,0 83,3 15,4 22,5 16,4 13,1 33,0 In 2008, this rate was higher in all the hospitals of the Alentejo Health Region (19,1%) and lower in the Norte (12,2%). Also, the intra‐hospital lethality rate increased in every Region, with the highest figures achieved in the Algarve (33%) and the lowest in the Alentejo (13,1%). Application for the 2010 SCML Award 115 Results 2 Figure 44 Proportion of surviving and deceased (intra‐hospital lethality) in‐patients due to Colo‐rectal Cancer (ICD 9: 153; 154.0‐154.1), by place of hospitalization (Health Region) Source: ACSS, DRG database In 2008, the profile of a colo‐rectal cancer‐related male in‐patient is as follows: median age: 70; and main related diagnosis: secondary cancer of the digestive and respiratory system; essential hypertension; diabetes; other complications of procedures, NEC and other and unspecified anemias. When dealing with a hospitalization resulting in death, the male’s median age rises to 73; and related diagnoses include: secondary malignant tumor of the digestive and respiratory system; secondary malignant tumor of other specified sites; disorders of fluid, electrolyte, and acid‐base balance; essential hypertension; palliative care and convalescence. Application for the 2010 SCML Award 116 Results 2 Table 65 Profile of Male In‐patient (with discharge from the hospital or death) due to Colo‐rectal Cancer (ICD 9: 153; 154.0‐154.1) Median age: Most frequent related dignosis: Survived Deceased 70 73 2.º Secondary cancer of the digestive and respiratory system Essential hypertension 3.º Diabetes 4.º Other complications of procedures, NEC 1.º 5.º Other and unspecified anemias Source: ACSS, DRG database Secondary cancer of the digestive and respiratory system Secondary cancer of other specified sites Disorders of fluid, electrolyte, and acid‐ base balance Essential hypertension Convalescence and palliative care For its part, the profile of a colo‐rectal cancer‐related female in‐patient is as follows: median age: 71; and main related diagnosis: secondary cancer of the digestive and respiratory system; essential hypertension; diabetes; other and unspecified anemias; and intestinal obstruction without mention of hernia. When dealing with a hospitalization resulting in the patient’s death, the median age is 76; and the main related diagnoses include: secondary cancer of the digestive and respiratory system; other and unspecified anemias, Secondary cancer of other specified sites; essential hypertension; and disorders of fluid, electrolyte, and acid‐base balance. Table 66 Profile of Female In‐patient (with discharge from the hospital or death) due to Colo‐rectal Cancer (ICD 9: 153; 154.0‐154.1). Median age: Most frequent related dignosis: 1.º 2.º Survived Deceased 71 76 Secondary cancer of the digestive and respiratory system Essential hypertension 3.º 4.º Diabetes Other and unspecified anemias Intestinal obstruction without mention of 5.º hernia Source: ACSS, DRG database Application for the 2010 SCML Award Secondary cancer of the digestive and respiratory system Other and unspecified anemias Secondary cancer of other specified sites Essential hypertension Disorders of fluid, electrolyte, and acid‐ base balance 117 Results 2 Prostate Cancer From 2000 to 2008, the number of prostate cancer‐related hospitalizations, in‐patient deaths due to this disease and the intra‐hospital lethality rate rose 13,2%, 28% and 13,1%, respectively. The evolving pattern of the total number of hospitalizations also occurred in every age group, with the most significant increases occurring in younger groups (25‐44: 16,7%; 45‐64: 44,4%). With regard to in‐patient death, the change in cases according to the various age groups occurred in a dissimilar fashion; the change in 2000‐2008 ranged from ‐8,3% (45‐64) to 54,4% (85 and over). The negative change (increase) in the intra‐hospital lethality rate for the entire population being studied does not occur in every age group, as important decreases occur with in‐patients under 65 (25‐44: 14,3%; 45‐64: 36,5%). Table 67 Number of hospitalizations, hospitalization deaths and intra‐hospital lethality rate due to Prostate Cancer (ICD 9: 185), by age group 2000 Hosp. Death. 2004 Let. Hosp. Death (%) 12,7 3206 403 2770 353 15 ‐ 24 years 1 1 ‐ 2 25 ‐ 44 years 45 ‐ 64 years 65 ‐ 74 years 75 ‐ 84 years 12 1 8,3 8 626 1034 882 36 103 155 Total 2008 Let. (%) 12,6 Variation 2000‐2008 (%) Let. Hosp. Death (%) 13,2 28,0 13,1 Hosp. Death 3135 452 Let. (%) 14,4 0 0 ‐ ‐ Age‐group: 215 57 85 and up Source: ACSS, DRG database 0 ‐ ‐ ‐ 1 12,5 14 1 7,1 16,7 0,0 ‐14,3 5,8 905 10,0 1201 17,6 879 41 110 182 4,5 9,2 20,7 904 1085 891 33 117 213 3,7 10,8 23,9 44,4 4,9 1,0 ‐8,3 13,6 37,4 ‐36,5 8,3 36,0 26,5 69 32,7 241 88 36,5 12,1 54,4 37,7 211 The Regions of Algarve, from 2000 to 2008, registered a important decrease, in the number of both prostate cancer‐related hospitalizations and in‐patient deaths. There were increases in the other Regions, during the said period. The intra‐hospital lethality rate rose in every Region, with the change ranging from 3,6% for Lisboa e Vale do Tejo to 90,1% for the Alentejo. Application for the 2010 SCML Award 118 Results 2 Table 68 Number hospitalizations, hospitalization deaths and intra‐hospital lethality rate due to Prostate Cancer (CID 9: 185), by place of residence (NUT II, pursuant to D.L. n. º 317/99, date 11 August) Variation 2000‐2008 (%) Hosp. Death. Let. (%) Hosp. Death Let. (%) Hosp. Death Let. (%) Hosp. Death Let. (%) 2000 2004 2008 Total 2770 353 12,7 3206 403 12,6 3135 452 14,4 13,2 28,0 13,1 NUT II Norte Centro LVT Alentejo Algarve 758 595 1021 148 104 63 75 160 21 22 8,3 12,6 15,7 14,2 21,2 752 745 1295 184 97 83 81 172 31 18 11,0 10,9 13,3 16,8 18,6 855 748 1219 152 83 88 101 198 41 19 10,3 13,5 16,2 27,0 22,9 12,8 39,7 25,7 34,7 19,4 23,8 2,7 95,2 ‐20,2 ‐13,6 23,8 7,1 3,6 90,1 8,2 144 12 Unknown Source: ACSS, DRG database 8,3 133 18 13,5 78 5 6,4 ‐45,8 ‐58,3 ‐23,1 The change (2000‐2008) in the distribution of cases by place of hospitalization (Health Region) follows the pattern previously identified in the analysis by place of residence. The number of hospitalizations and in‐patient deaths decreased for all the hospitals of the ARS Algarve (Regional health Administration) and rose in the rest. Table 69 Number of hospitalizations, hospitalization deaths and intra‐hospital lethality rate due to Prostate Cancer (ICD 9: 185), according to place of hospitalization (Health Region) Variation 2000‐2008 (%) Hosp. Death. Let. (%) Hosp. Death Let. (%) Hosp. Death Let. (%) Hosp. Death Let. (%) 2000 Total 2770 353 Health regions: 877 71 Norte 631 77 Centro 1085 169 LVT 83 14 Alentejo 94 22 Algarve Source: ACSS, DRG database 2004 2008 12,7 3206 403 12,6 3135 452 14,4 13,2 28,0 13,1 8,1 12,2 15,6 16,9 857 792 1340 124 101 84 174 26 11,8 10,6 13,0 21,0 908 774 1263 116 91 104 200 39 10,0 13,4 15,8 33,6 3,5 22,7 16,4 39,8 28,2 35,1 18,3 178,6 23,8 10,1 1,7 99,3 23,4 93 18 19,4 74 18 24,3 ‐21,3 ‐18,2 3,9 In 2000 and 2008, the intra‐hospital lethality rate was higher in the Alentejo and in the Algarve. However, the Alentejo and Norte Regions obtained the highest relative increases during this period (99,3% and 23,8%, respectively). Application for the 2010 SCML Award 119 Results 2 Figure 45 Proportion of surviving and deceased (intra‐hospital lethality) in‐patients due to Prostate Cancer (ICD 9: 185), by place of hospitalization (Health Region) Source: ACSS, DRG database In 2008, the profile of a male in‐patient for prostate cancer who was discharged from the hospital is as follows: median age: 69; and main related diagnoses: essential hypertension; secondary cancer of other specified sites; other and unspecified anemias; diabetes; and other disorders of urethra and urinary tract. When dealing with a hospitalization resulting in death, the median age rises to 79; and main related diagnoses include: Secondary cancer of other specified sites; other and unspecified anemias; disorders of fluid, electrolyte, and acid‐base balance; secondary cancer of the digestive and respiratory system; and other disorders of urethra and urinary tract. Application for the 2010 SCML Award 120 Results 2 Table 70 Profile of In‐patient (with discharge from the hospital or death) due to Prostate Cancer (ICD 9: 185). Median age: Most frequent related dignosis: Survived Deceased 69 79 1.º Essential hypertension Secondary cancer of other specified sites 2.º Secondary cancer of other specified sites 3.º Other and unspecified anemias 4.º Diabetes Other and unspecified anemias Disorders of fluid, electrolyte , and acid‐base balance Secondary cancer of the digestive and respiratory system 5.º Other disorders of urethra and urinary tract Other disorders of urethra and urinary tract Tracheal, Bronchus and Lung Cancer Tracheal, bronchus and lung cancer, which has been increasingly on the rise in Portugal, can also be seen by examining hospitalizations and deaths due to this disease. From 2000 to 2008, the number of hospitalizations rose 10,7%; in‐patient deaths increased 40,3%, and the intra‐hospital lethality was 26,7% higher. These increases were also identified in both genders, though differently. The change was greater in women from 2000‐2008 with regard to the number of hospitalizations and deaths, but not as great in the intra‐hospital lethality rate. Table 71 Number of hospitalizations, hospitalization deaths and intra‐hospital lethality rate due to Tracheal, Bronchus and Lung Cancer (ICD 9: 162), by age group Variation 2000‐2008 (%) Hosp. Death. Let. (%) Hosp. Death. Let. (%) Hosp. Death. Let. (%) Hosp. Death. Let. (%) 2000 2004 2008 Total 4483 1153 25,7 4639 1414 30,5 4964 1618 32,6 10,7 40,3 26,7 Gender: M F 3597 886 939 214 26,1 24,2 3734 905 1147 267 30,7 29,5 3775 1189 1286 332 34,1 27,9 4,9 34,2 37,0 55,1 30,5 15,6 Group age: 15 ‐ 24 years 25 ‐ 44 years 45 ‐ 64 years 65 ‐ 74 years 75 ‐ 84 years 7 217 1775 1538 824 0 46 438 400 222 0,0 21,2 24,7 26,0 26,9 5 167 1837 1585 919 1 36 510 486 331 20,0 21,6 27,8 30,7 36,0 2 212 1952 1523 1110 0 56 602 481 418 0,0 26,4 30,8 31,6 37,7 ‐ ‐2,3 10,0 ‐1,0 34,7 ‐ 21,7 37,4 20,3 88,3 ‐ 24,6 25,0 21,4 39,8 122 47 85 and up Source: ACSS, DRG database 38,5 126 50 39,7 165 61 37,0 35,2 29,8 ‐4,0 Application for the 2010 SCML Award 121 Results 2 There were a high relative increases (2000‐2008) in women of every age group, both in hospitalizations and in deaths, particularly in the 25‐44, 45‐64 and 75‐84 age groups. In men, the steepest increases occurred in the last two age groups; however, in a few groups, there was some improvements in terms of hospitalization (25‐44: ‐2,8%; 65‐74: ‐5,1%). The change in the intra‐hospital lethality rate by gender and age group varies greatly. In women, the change from 2000 to 2008 ranges from negative figures (decrease) in the 25‐44 (2,6%) and 85 and over (11,6%) age groups to positive figures in the other groups (45‐64: 11,3%; 65‐74: 12,1%; 75‐84: 43,7%). For men, the change is positive (increase) in every age group, with figures ranging from 2% (85‐and‐over) to 40,7% (25‐44). Figure 46 Number of hospitalizations and hospitalization deaths due to Tracheal, Bronchus and Lung Cancer (CID 9: 162), by gender and age group Source: ACSS, DRG database Application for the 2010 SCML Award 122 Results 2 Table 72 Number of hospitalizations, hospitalization deaths and intra‐hospital lethality rate due to Tracheal, Bronchus and Lung Cancer (ICD 9: 162), by age group and gender 2000 2004 Total 4483 1153 Let. Hosp. Death (%) 25,7 4639 1414 Gender: M F 3597 886 939 214 26,1 24,2 3734 905 1147 267 0 0 0,0 0,0 30 16 15 ‐ 24 years M 2 5 F 25 ‐ 44 years M 156 F 61 45 ‐ 64 years 1467 M F 308 65 ‐ 74 years 1267 M F 271 75 ‐ 84 years M 635 189 F 85 and up 70 M 52 F Source: ACSS, DRG database Let. (%) 30,5 Variation 2000‐2008 (%) Let. Hosp. Death (%) 10,7 40,3 26,7 4964 1618 Let. (%) 32,6 30,7 29,5 3775 1189 1286 332 34,1 27,9 4,9 34,2 37,0 55,1 30,5 15,6 0 5 0 1 0,0 20,0 1 1 0 0 0,0 0,0 ‐ ‐ ‐ ‐ ‐ ‐ 19,2 26,2 121 46 28 8 23,1 17,4 122 90 33 23 27,0 25,6 ‐21,8 47,5 10,0 43,8 40,7 ‐2,6 372 66 25,4 21,4 1514 323 431 79 28,5 24,5 1520 432 499 103 32,8 23,8 3,6 40,3 34,1 56,1 29,5 11,3 333 67 26,3 24,7 1311 274 409 77 31,2 28,1 1202 321 392 89 32,6 27,7 ‐5,1 18,5 17,7 32,8 24,1 12,1 178 44 28,0 23,3 707 212 246 85 34,8 40,1 835 275 326 92 39,0 33,5 31,5 45,5 83,1 109,1 39,3 43,7 26 21 37,1 40,4 81 45 33 17 40,7 37,8 95 70 36 25 37,9 35,7 35,7 34,6 38,5 19,0 2,0 ‐11,6 Hosp. Death. Gender and age‐ group: 2008 Hosp. Death From 2000 to 2008, the overall trend toward an increase in the number of tracheal, bronchus and lung cancer‐related hospitalizations, hospitalization deaths and the intra‐hospital lethality rate can also be seen in the distribution by place of residence. With the exception of the Alentejo, which achieved a relative decrease of 10,3% in hospitalizations, all the other occurrences experienced considerable relative increases in the various Regions. Noteworthy, in negative terms, is the Centro region, with regard to hospitalizations (23,9%), the Centro and Lisboa e Vale do Tejo Regions concerning hospitalization deaths (45,9% and 45,8%, respectively) and the Alentejo in terms of intra‐hospital lethality rate (53,2%). Application for the 2010 SCML Award 123 Results 2 Table 73 – Number of hospitalizations, hospitalization deaths and intra‐hospital lethality rate due to Tracheal, Bronchus and Lung Cancer (CID 9: 162), by place of residence (NUT II, pursuant to D.L. n. º 317/99, date 11 August) Variation 2000‐2008 (%) Hosp. Death. Let. (%) Hosp. Death Let. (%) Hosp. Death Let. (%) Hosp. Death Let. (%) 2000 2004 2008 Total 4483 1153 25,7 4639 1414 30,5 4964 1618 32,6 10,7 40,3 26,7 NUT II Norte Centro LVT Alentejo Algarve 1492 750 1636 253 179 346 157 469 72 58 23,2 20,9 28,7 28,5 32,4 1379 874 1661 294 191 354 198 610 98 59 25,7 22,7 36,7 33,3 30,9 1555 929 1919 227 211 481 229 684 99 81 30,9 24,7 35,6 43,6 38,4 4,2 23,9 17,3 ‐10,3 17,9 39,0 45,9 45,8 37,5 39,7 33,4 17,8 24,3 53,2 18,5 173 51 Unknown Source: ACSS, DRG database 29,5 240 95 39,6 123 44 35,8 ‐28,9 ‐13,7 21,3 Of the 28 NUT III, 25 achieved a relative increase in the intra‐hospital lethality rate from 2000 to 2008, whereas a decrease occurred in only 3 of them. As pointed out previously, intra‐hospital lethality rate is higher in the Alentejo, as this is the Region that shows the biggest increase from 2000 to 2008. The Central Alentejo was the NUT III with the steepest increases (51,3%), with the smallest occurring in the Serra da Estrela (11,1%) (see Annex 22). Figure 47 Tracheal, Bronchus and Lung Cancer‐related intra‐hospital lethality rate (ICD 9: 162), by place of residence (NUT III) Source: ACSS, DRG database Application for the 2010 SCML Award 124 Results 2 Only the Norte and the Alentejo Regions show a more positive trend in how hospitalizations evolve than that occurring for Mainland Portugal (‐0,8% and 10,4%, respectively). The same thing occurs in the Norte and Center (33,5% and 35,1%) for hospitalization deaths, even though the figures are still quite high. Table 74 Number of hospitalizations, hospitalization deaths and intra‐hospital lethality rate due to Tracheal, Bronchus and Lung Cancer (ICD 9: 162), by place of hospitalization (Health Region) Variation 2000‐2008 (%) Hosp. Death. Let. (%) Hosp. Death. Let. (%) Hosp. Death. Let. (%) Hosp. Death. Let. (%) 2000 2004 2008 Total 4483 1153 25,7 4639 1414 30,5 4964 1618 32,6 10,7 40,3 26,7 Health region: Norte Centro LVT Alentejo 1573 826 1771 163 373 174 491 62 23,7 21,1 27,7 38,0 1543 950 1763 228 430 205 642 83 27,9 21,6 36,4 36,4 1560 1014 2019 180 498 235 713 89 31,9 23,2 35,3 49,4 ‐0,8 22,8 14,0 10,4 33,5 35,1 45,2 43,5 34,6 10,0 27,4 30,0 Algarve 150 53 Source: ACSS, DRG database 35,3 155 54 34,8 191 83 43,5 27,3 56,6 23,0 Both in 2000 and in 2008, the tracheal, bronchus and lung cancer‐related intra‐hospital lethality rate was highest in the Alentejo and the Algarve Regions and lowest in the Centro. However, from 2000 to 2008, the biggest change in this rate occurred in the Norte (34,6%) and the Alentejo (30%). Application for the 2010 SCML Award 125 Results 2 Figure 48 Proportion of surviving and deceased (intra‐hospital lethality) in‐patients due to Tracheal, Bronchus and Lung Cancer (ICD 9: 162), by place of hospitalization Source: ACSS, DRG database In 2008, the profile of a male in‐patient for tracheal, bronchus and lung cancer who was discharged from the hospital was as follows: median age: 66; main related diagnoses: Secondary cancer of other specified sites; secondary cancer of the digestive and respiratory system; nondependent abuse of drugs; essential hypertension; and other diseases of lung. When dealing with a hospitalization resulting in death, the median age rises to 67; and main related diagnoses include: Secondary cancer of other specified sites; secondary cancer of the digestive and respiratory system; other diseases of lung; disorders of fluid, electrolyte, and acid‐base balance; and diabetes. Application for the 2010 SCML Award 126 Results 2 Table 75 Profile of Male In‐patient (with discharge from the hospital or death) due to Tracheal, bronchus and lung cancer (ICD 9: 162) Survived Deceased 66 67 Median age: Most frequent related dignosis 3.º Secondary cancer of other specified sites Secondary cancer of the digestive and respiratory system Nondependent abuse of drugs 4.º Essential hypertension 1.º 2.º 5.º Other lung disease Source: ACSS, DRG database Secondary cancer of other specified sites Secondary cancer of the digestive and respiratory system Other lung disease Disorders of fluid, electrolyte, and acid‐base balance Diabetes The profile of a female in‐patient for tracheal, bronchus and lung cancer who was discharged from the hospital is as follows: median age: 66; and main related diagnoses: Secondary cancer of other specified sites; secondary cancer of the digestive and respiratory system; essential hypertension; diabetes; and secondary and unspecified cancer of lymph nodes. When dealing with a hospitalization resulting in death, the median age rises to 70; and main related diagnoses include: secondary malignant tumor in other specified sites; secondary malignant tumor of the digestive and respiratory system; other diseases of lung; essential hypertension; and secondary and unspecified cancer of lymph nodes. Table 76 Profile of Female In‐patient (with discharge from the hospital or death) due to Tracheal, bronchus and lung cancer (ICD 9: 162) Median age: Most frequent related dignosis: 1.º 2.º 3.º Survived Deceased 66 70 Secondary cancer of other specified sites Secondary cancer of the digestive and respiratory system Essential hypertension Secondary cancer of other specified sites Secondary cancer of the digestive and respiratory system Other diseases of lung 4.º Diabetes Essential hypertension Secondary and unspecified cancer of 5.º Secondary and unspecified cancer of lymph nodes lymph nodes Source: ACSS, DRG database Application for the 2010 SCML Award 127 Results 2 5.1.4. Multivariate Logistic Regression For the selected causes of hospitalization (cardiovascular diseases and cancers) was developed a multivariate logistic regression model based on the dependent variable mortality (hospital discharge or death) and the variables sex, age and secondary diagnoses. However, only sex and age are statistically significant and contributes to the model. For ischaemic heart disease, the age is statistically significant but the sex not (p‐value = 0,174). Both variables contribute to increased the risk (age: 8.5% per year of life). For stroke, variables sex and age are statistically significant (p‐value = 0,00). Sex is a protective factor but the age contributes to increase the risk by 3.6% for each additional year of life. For female breast cancer the age is statistically significant (p‐value = 0,00) and increase the risk of death by 1,9% per year of life. For cervix cancer the age isn’t statistically significant (p‐value=0,063) but boosts the risk of death by 1,4% per year of life. For colon and rectum cancer the age is statistically significant (p‐value = 0,00) and raise the risk of death (2,1% per year of life) but the sex isn’t significant (p‐value= 0,45). For prostate cancer the age also shows statistic significance and markedly increases the risk of death by 9,1% per year of life. For trachea, bronchus and lung cancer the age and sex are statistically significant (both p‐value = 0,001) but only the latter one increases the risk of death, albeit slightly (0,9% per year of life). Despite the age and sex are statistically significant in almost all selected causes the model doesn’t have a good fit and therefore should not be used for predictions. The model, in terms of suitability is approved by the Hosmer and Lemeshow test but the values for Cox & Snell R Square and Nagelkerke R square are very low. Application for the 2010 SCML Award 128 Results 2 Table 77 Tests results p‐value Ischaemic heart disease Age Sex Stroke Age Sex Female breast cancer Age Cervix cancer Age Colon and rectum cancer Age Sex Prostate cancer Age Trachea, bronchus and lung Age Sex 0,000 0,174 0,000 0,000 0,000 0,063 0,000 0,458 0,000 0,001 0,001 Exp (B) 1,085 1,078 1,036 0,866 1,019 1,014 1,026 0,958 1,091 1,009 0,769 Hosmer and Lemeshow test Cox & Snell R Square Nagelkerke R Square 0,000 0,045 0,120 0,000 0,020 0,037 0,005 0,004 0,663 0,005 0,000 0,012 0,020 0,038 0,091 0,147 0,870 0,005 0,007 0,011 0,009 Application for the 2010 SCML Award 129 Results 2 Summary Female breast cancer (7.112 hospitalizations in 2008) • Represent 9,7% of all hospitalizations due to malignant neoplasm and 3,6% of the hospitalization deaths • The number of hospitalizations increased 32,9% and the intra‐hospital lethality rate decreased 39,5% between 2000 and 2008 • The 45 to 64 age‐group has the higher values of hospitalizations and hospitalizations deaths and the 85 and upper the highest intra‐hospital lethality • The intra‐hospital lethality rate is higher in Alentejo • The most hospitalization deaths are related to metastasis. Cervix uteri cancer (1.006 hospitalizations in 2008) • Represent 1,4% of all hospitalizations due to malignant neoplasm and 1,0% of the hospitalization deaths • The number of hospitalizations decreases 3,5% and intra‐hospital lethality rate increased 1,9% between 2000 and 2008 • The 45 to 64 age‐group has the higher values of hospitalizations and hospitalizations deaths and the 75‐84 age‐group the highest intra‐hospital lethality • The intra‐hospital lethality rate is higher in Algarve • The most hospitalization and hospitalization deaths are related to metastasis. Colo‐rectal cancer (9137 hospitalizations in 2008) • Represent 12,4% of all hospitalizations due to malignant neoplasm and 13,1% of the hospitalization deaths • The number of hospitalizations increased 17% and the intra‐hospital lethality rate increased 16,9% between 2000 and 2008 • The 65 to 74 age‐group has the higher values of hospitalizations, and the 75 to 84 age‐ group has the highest figures of hospitalization deaths. The intra‐hospital lethality increased with age • The intra‐hospital lethality rate is higher in interior Alentejo • The most hospitalization deaths are related to metastasis. Prostate cancer (3135 hospitalizations in 2008) • Represent 4,3% of all hospitalizations due to malignant neoplasm and 4,3% of the hospitalization deaths • The intra‐hospital lethality rate increased 13,1% between 2000 and 2008 • The 65 to 74 age‐group has the higher values of hospitalizations, and the 75 to 84 age‐ group has the highest figures of hospitalization deaths. The intra‐hospital lethality rate increased with age • The intra‐hospital lethality rate is higher in Alentejo • The most hospitalization deaths are related to metastasis. Application for the 2010 SCML Award 130 Results 2 Summary Trachea, bronchus and lung cancer (4964 hospitalizations in 2008) • Represent 6,8% of all hospitalizations due to malignant neoplasm and 15,5% of the hospitalization deaths • The intra‐hospital lethality rate increased 26,7% between 2000 and 2008 • There are more men hospitalized, but the number of female hospitalizations reveals a more important increase • The 45 to 64 age‐group has the higher values of hospitalizations and hospitalization deaths and the group 75‐84 years old the highest intra‐hospital lethality • Alentejo has the highest values of lethality rate • The most hospitalization and hospitalization deaths are related to metastasis. Application for the 2010 SCML Award 131 Terminally‐ill patients 6. Terminally‐ill patients In the 1970´s, in Portugal, less than 20% of the patients died in hospitals. In 2008, 63% of deaths occurred in hospitals, sometimes without minimal conditions of respect for the dignity and humanity of the Terminally‐ill Patients (TIPs) and their families (Higginson et al. 2002). There also a lack of organized palliative care in Portuguese hospitals. High mortality and the characteristics of the dying patient with cancer led to the development of specialist care supporting the patient and his family with emphasis on the interconnection between technical care and human support, adapted to each person's needs (Twycross, 2003). Accompanying a TIP requires organisation on behalf of the Services and it is a professional and personal challenge for health professionals that depends on their emotional stability, their attitude towards death and previous personal experiences (Marques et al. 1991). There is scientific evidence that there are differences in the perception and attitudes of doctors and nurses as well as general service professionals versus specialists (Natan et al, 2010; Murakawa et al., 2009). The specialists have more positive and favourable approaches. (Jacobs et al. 2002; Natan et al.2010). As a complement to the research on mortality in Portugal, additional information was sought on the organisation of services (without palliative care units) and the health professionals´ training and experience. Two questionnaires were made to be completed on line and Directors of all mainland Portuguese hospitals were openly and voluntarily invited to promote the questionnaire to services and professionals. Responses obtained from 38 Services and 217 professionals enabled a simple and realistic analysis of the situation in Portugal. Application for the 2010 SCML Award 132 Terminally‐ill patients 6.1 Organisation of Portuguese hospital Departments In total, 36 persons in charge for 38 hospital Departments answered this questionnaire, 18 of which were Departments Directors and 18 Head Nurses. The majority of the Departments are from Hospitals in the Health Regions of Lisboa e Vale do Tejo(50%) and Norte (34,2%), mostly condensed in Great Lisbon and Oporto. Other hospitals were also identified from other coastal areas and only one in the interior, the Trás‐os‐Montes e Alto Douro Hospital Centre. Figure 49 Distribution of participating Hospitals and distribution of public hospitals in Mainland Portugal Application for the 2010 SCML Award 133 Terminally‐ill patients Departments Strategy for the TIPs Replies were obtained from 38 Departments of which 14 (36,9%) were from Medicine; 11 (28,9%) from Surgery; 4 (10,5%) from Intensive Care Units; 9 (23,7%) were not identified. Table 77 and 78 illustrate global results regarding Medicine, Surgery and Intensive Care Departments. The study's complete results are attached (see Annex 23). The majority of the Services never transfers TIPs (78,9%). Medicine Departments are those that transfer the patients the least. Approximately 36,8% of the Services have a proper local or room reserved for TIPs. Surgery Departments should be highlighted with 63,6%. There are guidelines regarding the monitoring of a TIP in 68,4% of the Departments although the majority does not have written protocols. Spiritual and Religious Assistance and linguistic support are the areas in which there are the most protocols (31,6%; 23,7% respectively). There are few health professionals with specific training, although there is a higher percentage of nurses (31,6%) than doctors (13,2%). Surgery and Intensive Care Departments have a greater percentage of professionals with training. Supporting this pattern, nursing professionals also show a higher percentage in service integration training (Doctors=13,4%; Nurses = 31,5%). An overwhelming majority of the Departments refer that they have the support of other health professionals, indicating that there are multidisciplinary teams (86,8%). The analysis per Departments indicates that these teams exist in all Medicine and Intensive Care Departments. Application for the 2010 SCML Award 134 Terminally‐ill patients Table 78 Service Strategy for TIPs Service Strategy for TIPs All Services Medicine Surgery Intensive Services Services care N % N % N % N % Total 38 100 14 36,8 11 28,9 4 10,5 The service never transfers TIPs 30 78.9 12 86 9 81,8 3 75 There is a reserved place for TIPs 14 36,8 3 24,1 7 63,6 2 50 There are guidelines for follow‐up on TIPs 26 68,4 12 85,7 7 63,6 3 75 n=26 68,4% n=12 85,7% n=7 63,6% n=4 100% Transfer to room / isolated space 3 7,9 1 8,3 0 0 1 25 Pain control 5 13,2 1 8,3 1 14,3 3 75 Possibility of family presence 10 26,3 3 25 2 28,6 3 75 Psychological Support 7 18,4 2 16,7 2 28,6 2 50 Spiritual and religious assistance 12 31,6 4 33,3 3 42,9 3 75 Language support 9 23,7 3 25 2 28,6 3 75 Medical discharge if the patient wishes 4 10,5 2 16,7 1 14,3 0 0 Specific training of service professionals and N= support from other professionals 38 There is a written protocol for: 100% n= 14 36,8% n = 11 28,9% n = 4 10,5% Medical Doctors 5 13,2 4 28,6 0 0 1 25 Integration into the service 5 13,2 3 21,4 0 0 1 25 Nurses 12 31,6 4 28,6 2 20 2 50 Integration into the service 12 31,6 4 28,6 1 9,1 4 100 Support from other professionals 33 86,8 14 100 10 90,9 4 100 Participation of TIP in the decision regarding Medical treatment 15 39,5 6 42,9 5 45,5 2 50 Strategies for pain control 19 50 6 42,9 9 81,8 2 50 Opportunity to go home 12 31,6 8 57,1 11 100 3 75 3 7,9 1 7,1 2 18,2 0 0 6 16,8 3 21,4 2 18,2 0 0 Domiciliary care scheme Referral to the assistant physician /family doctor The Departments were questioned regarding the participation of TIPs in making decisions related to care. 50% of the services refer that the TIP participates in decisions regarding strategies to control pain. 39,5% and 31,6% refer that the patient participates in decisions regarding medical treatment and the opportunity to go home, respectively. Application for the 2010 SCML Award 135 Terminally‐ill patients Of all the Departments that participated in the questionnaire, only 7,9% mention the possibility of the care being provided under a domiciliary care scheme, mainly Surgery. Only 16,8% of the Departments refer the patient to the Assistant Physician/Family Doctor, 21,4% of which are from Medicine (21,4%) and 18,2% from Surgery. Strategy to support the family Most of the Departments refer that the family can accompany the patient 24h a day (60,6%). This response trend is applicable to all participating Departments. 81,6% inform the family on the care to be delivered to the patient and 65,8% have guidelines on how to notify the family in case of imminent death. Above half of the Surgery Departments (54,5%) indicate that they have these guidelines. The phone call is the most used tool to notify the family of the death when they are not present (71,7%). Head doctors (76,3%) and head nurses (65,8%) are those who give the news more frequently. This response trend is common to the Departments that participated in the questionnaire. Less than half (42,1%) notify the Assistant Physician/ Family Doctor of the death with the exception of Intensive Care with 50%. The study's complete results are attached (see Annex 24). Application for the 2010 SCML Award 136 Terminally‐ill patients Table 79 Family support strategy All Services Medicine Surgery Services Services Family support strategy Intensive care N % N % N % N % Total 38 100 14 36,8 11 28,9 4 10,5 The family can accompany the TIP 24 hours per day 23 60,6 9 64,3 7 63,6 2 50 Only during the day 11 28,9 4 28,6 3 27,3 2 50 31 81,6 12 85,7 10 90,0 3 75 25 65,8 10 71,4 6 54,5 4 100 Personally 24 63,2 10 71,4 5 45,5 4 100 By phone 27 71,1 11 78,6 9 81,8 2 50 The family is frequently informed about the care to be provided Guidelines for communicating with the family in case of imminent death When the family is not present when death occurs, usually the news is given by Usually the news is given by: A medical doctor 29 76,3 10 71,4 9 81,8 4 100 A nurse 25 65,8 10 71,4 8 72,8 3 75 16 42,1 5 35,7 4 36,4 2 50 The news of death is frequently reported to the Assistant Doctors/ Family doctor Application for the 2010 SCML Award 137 Terminally‐ill patients Summary • 36,8% of the Departments have a proper local or room reserved for TIPs. Surgery Departments should be highlighted with 63,6%. • 68,4% of the Departments guidelines regarding the monitoring of a TIP, although the majority does not have written protocols. • 31,6% of nurses and 13,2% physicians are specific training. • 86,8 % of the Departments refer that they have a multidisciplinary teams. • 42,1% of the Departments refer to notify the Assistant Physician/ Family Doctor of the death. • 71,7% of participants refer that the phone call is the most used tool to notify the family of the death when they are not present (71,7%). • Head doctors (76,3%) and head nurses (65,8%) are those who give the news more frequently. • 42,1% of participants refer notify the Assistant Physician/ Family Doctor of the death. Application for the 2010 SCML Award 138 Terminally‐ill patients 6.2 Doctors and nurses experience and training 217 doctors and nurses answered the questionnaire, most of which were female (76%), 46,2% of which aged 25 to 34 (mean age of 38±11), 50,7% of which work in a hospital in the Health Region of Lisboa e Vale do Tejo 79,6% of which are Nurses. The participants' general characteristics are summarised in annex 25. As would be expected, the majority of the professionals are from hospitals located in large urban centres of Lisbon and Oporto. However, it is important to highlight that the answers come from many different points, with special focus on general hospitals on the coast. Figure 50 Distribution of the Hospitals whose Professionals participated in the survey and distribution of public hospitals in Mainland Portugal Source: Elaborated by a project team based on data from survey number 2 Most of the doctors are from Medicine (61%), as well as the nurses (36,4%). More than half of the sample (Doctors=56,1%; Nurses=50,6%) performs duties in a hospital located in the Health Region of Lisboa e Vale do Tejo. Application for the 2010 SCML Award 139 Terminally‐ill patients Table 80 Characterization of health providers Total Doctors Nurses N % N % 41 100,0 176 100,0 Departments Emergency Medicine Surgery Intensive Care Unanswered 6 25 7 3 0 14,6 61,0 17,1 7,3 0,0 27 64 44 21 20 15,3 36,4 25,0 11,9 11,4 Gastroenterology specialists (39,9%) and internal medicine specialists (29,3%) were the most mentioned. Nurses have the greatest variety of specialties (13 nursing specialties versus 11 in medicine). Most nurses indicated that they hold a medical‐surgical nursing speciality (see Annex 26). 39% of the doctors obtained their degree over 30 years ago and 37,5% of the nurses more than 5 to 10 years ago (see Annex 27). Medical and nursing training 95,1% of the doctors did not get specific pre‐graduate training in this area. Most nurses refer the opposite result (51,1%). With regards to specific post‐graduate training, the response pattern is the same for both doctors and nurses (Doctors=80,5%; Nurses=61,9%). Specific training in the area both for doctors (19,5%) and Nurses (37,5%) was acquired by participating in academic seminars/workshops (Doctors=62,5%; Nurses=53,0%) (see Annex 28). Application for the 2010 SCML Award 140 Terminally‐ill patients Table 81 Doctors and Nurses Training Total Doctors Nurses N % N % N % Total 217 100 41 18,9 176 81,8 Specific pre‐graduate training 92 42,4 2 4,9 90 51,1 Specific post‐graduate training 74 34,1 8 19,5 66 37,5 Type of specific post‐graduate training Seminars/Workshops 40 18,4 5 62,5 35 53,0 Incentive to training 85 39,2 10 24,4 75 42,6 22 10,1 2 4,9 20 11,4 Training when the provider entered the service Half of the physician participants (51,2%) stated that the Institution where they work does not provide incentives for training in this area. As for the nurses, they state the opposite, 42,6% refer that their institution does provide incentives for training. Most of the participants (Doctors=90,2%; Nurses=84,7%) refer that they did not get any specific training in this area when they integrated the Service where they work (see Annex 29 and Annex 30). Most doctors and nurses (Doctors=73,2%; Nurses=75,6%) deal with more than 10 terminal patients per year (see Annex 31 ). 26,8% of the doctors state that there are frequent discussions amongst the team regarding the possibility of TIPs being monitored at home and only 14,2% of nurses say the same (see Annex 32 ). As for training for family providers, doctors (39,0%) believe it is frequently given but nurses (38,1%) opted to answer “sometimes” (see Annex 33). Approximately half of the doctors sometimes (29,3%) or frequently (29,3%) refer patient families for psychological support during the process. The nurses gave similar answers. This reference to a psychologist is significantly less frequent after death: only 7,3% of doctors and 13,6% nurses (see Annex 34). Application for the 2010 SCML Award 141 Terminally‐ill patients Table 82 Support for families of TIPs Total N Doctors % N % Nurses N % Total 217 100 41 18,9 176 81,8 Psychological therapy to family members during the terminal process 120 55,3 24 58,6 962 54,5 Psychological therapy to family members after death 62 28,6 10 24,4 Social support to family members during the terminal process 164 75,6 33 80,5 131 74,4 Social support to family members after death 44 20,3 12 29,3 Multidisciplinary team to follow the TIP 130 59,9 25 61 52 28,4 32 18,2 105 59,6 The pattern is similar regarding social support: most doctors (56,1%) and nurses (46,6%) refer that they frequently seek social support for the family during the process. However, after the death of TIPs this happens only with a minority of doctors (4,9%) and nurses (5,1%) (see Annex 35). Table 83 Doctors and nurses who incorporate the multidisciplinary team Total Total Doctors Nurses N % N % N % 217 100 41 18,9 176 81,8 Health care providers in multidisciplinary team Family Doctors 16 7,4 2 8 14 13,3 Medical practitioners from another specialties 100 46,1 20 80 80 76,2 Nurse 126 58,1 22 88 104 99 Physiotherapist 28 12,9 5 20 23 21,9 Psychologist 71 32,7 17 68 54 51,4 Social Worker 122 56,2 25 100 97 92,4 Spiritual or religious assistant 73 33,6 8 32 65 61,9 14 6,5 7 28 7 6,7 2 Other 1 The Total is equal to the number of Health professionals that responded affirmatively to the previous question. Note: the sum is greater than the total because more than one alternative may be selected. 2 Other Professionals mentioned: Hospital Discharge Management Team, Palliative Care Team, Internal medicine physician in conjunction with a doctor from another speciality, Nutritionist, Pain Management Unit. Regarding the presence of a follow‐up strategy for TIPs by a multidisciplinary team within the Service, 41,5% of doctors and nurses (40,3%) mention the involvement of a team of professionals from several areas (see Annex 36). Application for the 2010 SCML Award 142 Terminally‐ill patients The majority of doctors that confirmed the existence of this multidisciplinary team also mentions there being doctors (80%) and nurses (88%) from other specialties. All doctors refer that there is a social worker (100%) and psychologists are also frequently present (68%). Nurses refer that multidisciplinary teams are constituted by nurses (99%), doctors from other specialities other than that of general practitioner (76,2%), social worker (92,4%) and psychologists (51,4%). Summary • 95,1% of the doctors did not get specific pre‐graduate training • 51,1% of the nurses got specific pre‐graduate training • Doctors and nurses refer patient families for psychological and social support during the process. • Doctors and nurses confirmed the existence of this multidisciplinary team. Application for the 2010 SCML Award 143 Terminally‐ill patients Discussion “The patient does not cease being a person in all its greatness when all means for a clinical cure have run out” (Silva, 1995) Results show that hospitals are concerned with issues associated to TIPs, although the organisation is still very fragile with little specialised training. Most departments do not have a local reserved for TIPs and their families due to a lack of physical space which is common in most health services in Portugal and which is connected to an increase in the search and need for care (Campos e Carneiro, 2009). For different reasons, Surgery and Intensive Care are the services that most provide for this space. The former due to a lower occupation rate and the latter because of the severity of admitted patients, who are transferred from other services in terminal situations that determine a greater mortality. A special area which might guarantee TIPs´ privacy is recommend in several guidelines (WHO, 2009) which also has a positive effect on other patients that are not confronted with the feelings and pain of those who are going through this phase. The terminal process is recognised as being complex and deserves a specific technical approach and human support (Emanuel et al. 1999; Pereira de Moura et al. 1995). Actually, services have specific guidelines regarding most situations associated to TIPs. However, few have written guidelines about the different procedures to be followed in this situation. An international study demonstrated that doctors and nurses admit that the absence of guidelines and protocols regarding the care to be provided constitutes a barrier and hinders good practices in their work (Jacobs, 2002). This study concluded that a small percentage of doctors and nurses have specific training in this area, which demonstrates a lack of attention toward the terminally ill patients and their families. Application for the 2010 SCML Award 144 Terminally‐ill patients A TIP has specific, particular and multifaceted needs which require team work and continuous and individualised attention (Pereira de Moura et al. 1995). In this regard, participating health services comply with international practices and recommendations that appeal to the need for TIPs to be accompanied by multidisciplinary teams that enable holistic and integrated support for the patient and the family (Pereira de Moura et al. 1995; WHO, 2009). Recent studies show the relevance and interest of patients participating in the decisions associated to their treatment (Ramos and Gonçalves, 2010; Tariman et al. 2009). The patient's participation in the treatment is associated to sharedecision‐making as a process that seeks a compromise between evidence‐based medicine and the ethical‐humanistic rationale that advocates citizen‐centered health (Ramos and Gonçalves, 2010). Medicine Departments are those which most recommend the participation of TIPs in medical treatment, in pain control strategies, in the opportunity of the patient to go home. This result may be related to the nature of the pathologies treated, which allow the patient to have a greater level of awareness and participation than patients who are in Intensive Care for example. The professionals´ concern in allowing patients to participate in decision‐making enables conclusions to be reached regarding efforts to provide quality care, centered on the patient and the family and guaranteeing the humanisation of care. In global terms, healthcare services do not cover the possibility of Home Care to terminally‐ill patients. This demonstrates the lack of flexibility in the organisation of services when dealing with TIPs, as they do not grant the patient the option to die at home. For the patient to be able to go home there must be a close relation between the hospital services and the domiciliary service so as to guarantee the best care to the patient (Pereira de Moura et al. 1995). The displacement of TIPs to their home is often impossible due to the absence of adequate equipment and an environment which is inappropriate for the patient’s situation (Higginson et al. 2002). On the other hand, relatives sometimes have the perception that the hospital will take better care of the TIPs because it will likely provide everything the patient needs (Jacobs et al. 2002). The impossibility of supporting the patient at home is a contradiction, since relevant literature mentions that healthcare services should offer the patient the possibility of dying “in a family environment” (Jonen‐Thielemann, 1998). Application for the 2010 SCML Award 145 Terminally‐ill patients The presence of the family is fundamental not only for the TIPs, but also to manage the family’s process of loss and mourning (Twycross, 2003; Kubler Ross, 2002). The family also plays a relevant role in providing healthcare services. The majority of participating healthcare services offer the family the possibility to accompany the TIPs 24 hours a day, or at least during the day. It also seems common practice for the services to inform the family regarding the care the patient should be given. The approach when communicating the patient’s situation to the family and death itself is very complex for both the healthcare provider and the family; therefore it is important for the professional to have proper training and the sensibility to carry this (Tariman et al. 2010; Twycross, 2003; Kubler‐Ross, 2002). Even though the family may already be expecting this moment, it may well trigger distress and anger that might influence their future emotional state (Twycross, 2003; Kubler‐Ross, 2002). On the other hand, this moment will possibly generate anxiety for the healthcare provider and have a profound effect on the way he will carry out his job afterward (Marques et al. 1991). Healthcare services seem to recognise this complexity and guidelines on how to deliver the information to the family are provided in most cases. One of the criticisms towards healthcare services has to do with the lack of articulation between the different levels of care (Dias and Queirós, 2009). This is corroborated by the fact that most services admit they do not notify the assistant physician/family doctor about the patient’s decease. The articulation between hospital services and primary care is fundamental as it provides an update of medical records and patients’ database as regards primary care, as well as the subsequent monitoring of the family. With reference to the specific responses of healthcare providers, they corroborate the study of the services and reinforce the conclusions and recommendations of this paper. Most healthcare providers are part of the Healthcare Services that, due to their nature, have a greater probability of being confronted with TIPs. For Marques et al (1991), the manner in which each healthcare provider manages the issue of death and the terminal process depends on their emotional stability, their attitude towards death and illness and their previous personal experiences. Within this context, the training received and the experience attained are fundamental for adequate care provision. Studies indicate that healthcare providers who Application for the 2010 SCML Award 146 Terminally‐ill patients perform tasks in specialised units have more favourable and positive approaches regarding these themes than the ones who do not practice in this type of unit (Jacobs et al, 2002; Natan et al. 2010). The age distribution of the sample shows the characteristics of human resources in Portugal, characterised by an ageing of the medical class and very young nurses (Dussault and Fronteira, 2010). Death is a taboo topic, which is rather discussed (Pereira de Moura, 2005; Veiga et al. 2009). Patients would formerly die at home with the support of family and friends. This viewpoint has changed, with the hospitalisation of death (Campos and Carneiro, 2010; Higginson et al. 2002). This transformation is, on the one hand, associated to social changes, such as the modification of the role of women who now work outside the home, as well as an ageing population which contributes to many elderly people not having relatives who can care for them (Higginson et al. 2002). Concurrently, the evolution of medical technology to minimise pain and lengthen life fosters an increasing trend for people to die in a hospital context (Jacobs, 2002; Higginson et al. 2002). This social, cultural and clinical change in death entails greater flexibility and adaptation on behalf of healthcare services, requiring healthcare providers to acquire new competences and proper knowledge on how to work in this area. Most doctors mention the absence of specific pre‐graduate training. The situation is different when it comes to nurses, as they mention having received specific training in this area. The reading of the curricula of the majority of medicine and nursing courses reveals that few curricular units discuss this theme. Nonetheless, these subjects are more frequent in nursing courses. Relevant literature points out differences in perceptions and behaviour of doctors and nurses when approaching these topics (Natan et al. 2010; Murakawa and Nihei, 2009). Doctors try to explain to the patient aspects related to their terminal process and death, and are more focused on the clinical dimension of the illness and immediate relief of physical symptoms; they are not as receptive to matters of emotional nature (Natan et al. 2010). On the other hand, nurses seem to be more open when it comes to listening to patients and communicating with them and their relatives (Natan et al. 2010; Veiga et al. 2009). This substantiates the response provided by the 147 Application for the 2010 SCML Award Terminally‐ill patients participants. Finally, the increase in the number of TIPs, the organisation of Palliative Care Units inside hospitals, the emergence of the National Network for Continuing and Palliative Care and the progress in knowledge within this field have all contributed to increase awareness of professionals in general and acknowledging the need to gain competences in this area. Following‐up on TIPs is a complex process which poses challenges to healthcare providers not only from a professional point of view, but also of an emotional nature (Veiga et al. 2009; Souza, Souza and Souza, 2005). Follow‐up on TIPs confronts professionals with various limitations, namely the need to face the fear of death and illness, adapting to the inexistence of a cure and confronting personal and professional limits (Pereira de Moura, et al. 1995; Souza, Souza and Souza, 2005; Veiga et al. 2009). The healthcare professional’s performance under these circumstances involves not only attenuating pain, but also developing a relationship between three poles: healthcare providers, patient and family (Twycross, 2003; Pereira de Moura et al. 1995). Not all professionals can adequately deal with TIPs, so they may perhaps use mechanisms of protection and defence (e.g. denial of the situation, detachment, etc.) and argue that they don’t have time and availability to listen to patients and be with them (Marques et al. 1991; Pereira de Moura et al. 1995). Professionals recognise that building communicative competences, providing emotional support for patients and relatives, and conveying bad news are all opportunities to improve their performance regarding the care provided to TIPs (Jacobs, 2002). Studies also indicate that TIPs present a set of other non‐medical needs which are often handled by relatives and friends (Emanuel et al. 1999). Consequently, there should be more structured institutional support for informal care providers, given that their role is fundamental to improve the quality of life of TIPs and possibly contribute to minimising expenses in Healthcare Services (Emanuel et al. 1999; Higginson et al. 2002). The presence of psychologists in hospitals is becoming a reality, although complete national coverage has not yet been assured. This aspect contributes to increasing recognition of the fact that psychological support plays a crucial role in minimising pain and all the other feelings associated to this phase (Pereira de Moura et al. 1995). Owing to the characteristics linked to the Application for the 2010 SCML Award 148 Terminally‐ill patients terminal process and emotional loss, along with social and material loss, the intervention of the social worker is imperative and acknowledged by healthcare professionals. In fact, as demonstrated in the previously discussed study on healthcare services, the existence of multidisciplinary teams is a reality in most Portuguese hospitals (Pereira de Moura et al.1995). There is an international study which addresses the coherence between the needs perceived by the healthcare professionals as regards the TIPs and the needs described by the patients themselves and by their relatives (Natan et al. 2010). Healthcare professionals, patients and family members all point out that apart from their clinical needs, such as pain relief and the necessary nursing care, it is relevant to have somebody to talk to and to die with dignity (Natan et al. 2010). On this matter, the emotional availability of healthcare professionals is fundamental in providing high quality care. To die with dignity means to be respected until the end and, for that to be possible, the healthcare professionals should come closer, listen to and touch those who suffer: not only the patient, but also their family. “...When facing terminal patients, we have to draw closer, stop and find time to listen and accompany those who suffer and ultimately they are just expecting for another hand to hold their own”. This type of attitude is perhaps one of the greatest challenges healthcare professionals are faced with: “contributing for the re‐socialization of death” (Feytor Pinto, 1991, cit. by Fernandes, 1999). Limitations of this paper: The present work has an exploratory nature and emphasises the need for further research in this area. Due to the characteristics of the sample, it was not possible to draw conclusions regarding the population. Application for the 2010 SCML Award 149 Terminally‐ill patients Conclusions and recommendations 1. The number of respondants, although small to conclude, seems to reflect an increasing interest on this subject. 2. There is a strategic planning from the Portuguese Ministry of Health to organize Palliative Care Units but it is not enough. All Hospital Departments should be organized to support the TIP and families. 3. Development of training and skills in health care providers, so they can perform their tasks with more accuracy and effectiveness, are mandatory and should be evaluated for career progression. 4. Pre‐graduate training should be added to curricula for medical students and nursing students. 5. Development of written procedure protocols and manuals to standardized best practices should be encouraged. 6. Articulation with other professionals to ensure the principle of multidisciplinarity (i.e. psychologists, social workers) is established in a satisfactory way, but should be stimulated. Application for the 2010 SCML Award 150 Discussion 7. Discussion In Portugal, the first decade of the 21st century featured health reforms, namely in Primary and Long Term Care and through the implementation of the first National Health Plan 2004‐2010, which develops according to the lifecycle, with priority given to those who are most vulnerable. This is monitored through indicators and evaluated according to set goals. Most indicators involve mortality in the various age groups as well as preventable and early mortality in pathologies constituting the leading causes of death, such as cardiovascular diseases and cancer (NHP Atlas, 2010). This fact determined the creation of 4 priority programs and the implementation of strategies for dealing with Ischemic Heart Disease and Stroke, as well as secondary prevention of screenable cancers: breast, cervical and colo‐rectal. Although the analysis of these policies is still at an early stage, it seems important to understand how death has evolved from 2000 to 2008, to correct and improve expected actions. The World Bank cites the example of Estonia, which, through appropriate and realistic policies, achieved a period of rapid decline of 35% in the overall mortality rate from 1995 to 2000 (Rajaratnam et al., 2010) Mortality indicators are traditionally the easiest to obtain, and that is also why they are most often used when examining the health of a population. The pattern of mortality by age and gender is an indicator of the epidemiological situation of a population and the burden of the disease but even in countries with an organized civil registry, there is a certain distrust with regard to data quality and completeness. Several studies and methods for exploring information and characterizing uncertainty have been presented (Lopez et al., 2006, Christopher M et al., 2010). The WHO publishes regular studies of mortality data by disease and external causes for over 100 countries, using several databases (Matters et al., 2009) as well as the OECD, which conducts comparative studies, of which Health at a Glance is an example in the field of health (OECD., 2010) (Mathers, 2003 a). Application for the 2010 SCML Award 151 Discussion In Portugal, there are two official databases regarding deaths: i) Data from the Statistics Portugal (INE) based on death certificates was used to make a comparative analysis of general mortality, by causes and premature mortality; ii) Data from records pertaining to Diagnosis‐related Group (DRG) of the Health‐Care System’s Central Administration (ACSS) was used for intra‐hospital lethality. In this work, as referred in the methodology, these two sources were analyzed to check for data reliability, while positively contributing toward improving registration. For 2011, the Directorate‐ General for Health and the Ministry of Justice propose that the form be electronically filled in and de‐materialized, thus facilitating and speeding up the entire information and public disclosure, which is currently about a year behind schedule. In the years being studied (2000, 2004 and 2008), the death certificate is filled in manually by a doctor who is presumed to be responsible for the patient at the hospital. When the death occurs at home or at another location, such as in the street, the doctor is often not fully aware of the medical problems collected through the family without examining or researching the medical record. As for DRGs, the medical record is fully filled in by the doctor who took care of the patient at the hospital when he/she leaves; afterwards, the information is coded by doctors with specific training and contract, and the database is put together later on. It should be pointed out that the results of the INE mortality basis were worked on by the institution, upon request from the authors. Thus, the most in‐depth study for concrete situations was conducted via DRGs bases, which could be accessed by researchers. If this is possible, the cross‐tabulation of these two sources would be vital for studying the impact of death. Slobbe (Slobbe et al., 2008) compares the data from death certificates with Dutch hospital discharge notes from 1996 to 2003, with particular emphasis on deaths that occurred, both in and outside the hospital, 30, 60 and 95 days after hospitalization as a means of evaluating not only the institution’s performance, but chiefly health care as a whole. The present study begins with birth rate, mortality rate and migrations, pillars of demographic change, as a framework for overall results. A sharp and worrisome drop in birth rate and in migrations were noticed with an expected result: ageing and a decrease in the active population. Application for the 2010 SCML Award 152 Discussion As for birth rate, it is urgent that a policy of incentives for young couples is set up, namely via appropriate parent licenses, job security, guarantees that their careers will not be cut short, and a suitable number of daycare centers with social support. Within the context of the current crisis, increased poverty and social exclusion can be expected, and there is evidence that support to these families and the future of children depend on food aid, affective and educational support from as early as the first year of life, all of which they have access to through daycare centers (Heckman, 2006). In the 1990’s, immigration was responsible for one quarter of population growth in industrialized countries, and migration influences demographic changes directly and indirectly by birth rate (Lutz and Scherbov, 2006). Immigrant families are usually young people with a much higher fertility profile, but quickly adopting the demographic characteristics of host countries. In a 2005 study, in the municipalities of Amadora and Sintra, 43% of newborns were born to immigrant mothers (Machado MC et al., 2006). In Portugal, this is a very asymmetric situation dependent on flows and on places of residence of this population, with a greater tendency toward the regions of Lisboa e Vale do Tejo (Lisbon and the Tagus River Valley) and the Algarve. In the present study, from 2004 to 2008, a sudden drop of 83% in new immigrants was found, worsened by an unquantified number of those wanting to return to their countries of origin, namely Angola and Brazil. This fact results from the social and financial crisis as well as from the growing unemployment rate all over Europe. This scenario will not be changing within the next few years. Therefore, even in this area, there is a need to develop strategies to control the disorderly entry of thousands of immigrants, as was the case in the 1990’s but which will stimulate expected movements, which are extremely useful for Portugal. Overall, even the mortality rate decreased 4,4% in the years being studied, due to improved socioeconomic conditions and advances in medicine, with new technologies and therapeutic innovation, in fields such as cardiovascular diseases and cancer. Life expectancy at birth increased 2,3 years, from 2000 to 2008, with differences going as high as 2,89 years between the Central Coast and the Interior. As for gender, women still hold the upper Application for the 2010 SCML Award 153 Discussion hand in longevity; however, in the period being studied, the age gap was narrowed between men and women. The consistent increase in life expectancy at birth can be regarded as a triumph over death at a young age, a display of progress, while reflecting the success of the human development process. However, it also constitutes a challenge from a social, medical and financial standpoint. With the 60‐and‐over age group experiencing the highest growth rate worldwide, this can be considered a veritable demographic revolution. With the framework provided, the discussion of the present study begins with adult mortality, preventable deaths and place of death; this is followed by intra‐hospital lethality and aspects of interest, comparable with the former. Finally, the characteristics and profiles of the most frequent causes of death are presented, such as cardiocerebrovascular diseases and cancer. Analysis of adult mortality through civil registration Upon reflection, adult mortality from age 15 was selected to be studied, the reason being that, in younger age groups, causes are heterogeneous and have been the subject of domestic and international research. The 1980’s and 1990’s focused public health on infant mortality and morbidity, and the implementation of strategies in children resulted in a substantial decline in mortality rates (Murray et al., 2010). Infant mortality is the factor that most influences Life Expectancy at Birth, and so the sharp drop in this indicator determined the increased life expectancy, with a deviation in death at adulthood, with a repercussion in the most economically and socially active groups. A study of the literature, namely the strategy of the World Bank and the WHO, which define a risk of mortality in adults 45q15, with the likelihood, at age 15, of dying prior to age 60, that is, the risk of early death (Rajaratnam et al., 2010), also determined the group’s option to study in this research. Application for the 2010 SCML Award 154 Discussion Thus, the evaluated results refer to a population, ages 15 to 113, which are, respectively, the ages on which data are collected and the oldest age for a national Portuguese female, as recorded in the bases being studied. The fact that it’s a female comes as no surprise. Since the causes of death linked to pregnancy and childbirth are controlled, women’s Life Expectancy is higher than men’s. In the years being studied, in Portugal, differences by gender are reduced, with life expectancy at birth for males (75,7 years) approaching that of females (81,9 years). In developed countries, an even greater approximation between both genders by female losses was found which shows losses in life expectancy, due to acquired habits such as smoking, alcoholism and greater day‐to‐day stress (Lefèvre et al., 2008; Juel, 2008) To support this evidence, it was noticed that the 65‐to‐74 age group showed the biggest differences between men and women. Men who live to age 75 have a life expectancy that is close to that of women. The biggest drop in mortality rate occurs in the 15‐to‐24 (50%) and 25‐to‐44 age groups (33%). This is good news because death in these groups will always be premature and eventually linked to health‐care‐sensitive causes and to the promotion of health, such as accidents and infections. The deviation in mortality for 75+should also be pointed out, with the 65‐to‐74 age group decreasing 22% and the 75‐to‐84 age group showing a relative drop in mortality rate, due to the growth of this population group. People die at an increasingly older age. The differences between genders still occur in a homogeneous fashion in every age group, favoring females, although these are diminished with age. External causes (accidents) and cardiovascular diseases may be chiefly responsible. To account for the uncertainty that arises from the biological and random processes governing the occurrence of events as deaths and illnesses, 95% confidence intervals were computed for death rates. Confidence intervals were used as a test of significance when comparing two death rates, since if respective confidence intervals do not overlap, a comparable statistical test would always indicate a statistically significant difference. That was the case for all of death rates discussed below. Application for the 2010 SCML Award 155 Discussion As for the place of residence, the results are shown as a standardized rate for a standard European population and, using the Comparative Mortality Index, differences among regions were found. The Lisbon and Tagus Valley, Alentejo and Algarve regions have a higher relative risk of death, which is one of the aspects suggesting health‐related inequalities. In Sweden, this difference is as high as 7 years; however, in Portugal, even excluding the effect of age, the standardized mortality rate varies from 7,4 in the North to 8,5 in the Alentejo. This region achieved the worst results in 2000 but improved during the period of time being studied. The North, which also showed a positive change, achieved the nation’s lowest mortality rate in 2008. When examining the mortality rate by marital status, for singles, divorced or widowed populations, the following figures were obtained for the Comparative Mortality Index in 2004: 165,9%, 139,7% and 140,8%, respectively. These figures are all well above the risk of death for the overall population. The exponential increase in the divorced population is in line with the rise in the number of divorced individuals in Portugal, from 1,9 to 2,4 per one thousand population, during the period being studied. The celebrated marriages dropped from 6,2 to 4,0 per 1000 population. This, combined with the sharp decline in the mortality rate in the younger age groups of the population, could contribute toward a decrease in the number of deaths of single individuals. As previously mentioned, early mortality rate among males justifies the discrepancy between 21,1% of deaths among widowers and 57,0% among widows. It would be very interesting to study the trend of higher morbidity and mortality rates linked to recent widowhood, regardless of the cause of death, as shown in the works conducted by Nicholas Christakis in broad series (Christakis N et al., 2006; Christakis et al., 2008). In another longitudinal study, the same author monitored 200,000 recently widowed individuals for a 9‐ year period (1993 to 2002) and concluded that the place of residence and the established social network are factors that influence mortality rate and which, in residential quarters where few widowed individuals live, the mortality rate is 22% for males and 17% for females, compared to 17 and 15% respectively, in residential quarters with higher numbers of elderly people with this marital status (Christakis et al., 2008) Application for the 2010 SCML Award 156 Discussion The Portuguese death certificate comprises 3 fields pertaining to Occupation: i) Occupation; ii) Occupational situation; iii) Work status. Each of these includes various fields to be filled in, such as active and non‐active, employed, unemployed or looking for 1st job, among others. These excessive items do not allow for much in the way of conclusions. Little can be said from the data provided in this field by the current death certificate, other than that 90% of deaths occurred among non‐active individuals, and 82,3% were over 65. It should be pointed out that, among the active population, the mortality rate was lower in individuals with jobs, from 2000 to 2008: from 1,9 to 1,5 deaths per 1000 employed (relative decrease: 21,9%). And 50,1% of deaths in 2000 and 58,1% of deaths in 2008 occurred in less differentiated professional groups. It can be inferred that these come from a lower socioeconomic class with less academic education; however, with the current scientific evidence showing that social determinants are vital factors in health, illness and death, it would be important for these aspects to be considered and registered on a regular basis. Health‐related inequalities emerge from social determinants such as the socioeconomic and educational level, lifestyles and access to health care. The health status is worse among the most disadvantaged socioeconomic groups, whereas wealthier individuals experience the reverse phenomenon: they become ill less often and are better off, health‐wise (Marmot, 2010). This constitutes a public health problem, with an impact on cohesion and social justice, while affecting socioeconomic development (Johnson et al., 2008). Differences in socioeconomic status have been consistently associated with CVD incidence and mortality across multiple populations. In a recent Swedish study, age‐standardized incidence of coronary heart disease was found to be high in high‐deprivation neighborhoods (Winkleby et al., 2007). The inverse association between socioeconomic status and CVD is strongest for mortality and incidence of stroke, with low socioeconomic groups showing lower survival (Kunst et al., 1998) and higher stroke incidence in many populations in developed countries. Application for the 2010 SCML Award 157 Discussion Deaths among immigrants were analyzed, since they are considered a vulnerable group. Portugal has become a Nation of Nations, as shown on world map 1, which displays multiple origins, thus comprising a large social, cultural and ethnic diversity. When examining deaths by nationality, it was noticed that apparently, excluding Portuguese nationals, deaths occur most often in people from countries in the European Union and Africa (world map 2), which can be justified by the age groups. In most cases, Europeans are retired people receiving a pension, hence, with more advanced ideas. African and Brazilians are young, active immigrants, and, as will be seen further below, the causes of death are very different. In the second case, socioeconomic deprivation and vulnerability of immigrants are reflected in the bad results achieved in health. According to the MIPEX (the British Council’s Migrant Integration Policy Index and of the Migration Policy Group, 2007), Portugal is the country in Europe with the second most favorable integration policies, surpassed only by Sweden. It should be referred that the creation of the High Commission for Immigrations and Intercultural Dialogue, with national plans of action and which includes health, schooling, employment and integration, along with an innovative Dispatch from the Health Minister in 2001, which ensures access to health care to people living in Portugal for over 90 days, regardless of their legal status. It is not enough to allow access without barriers: due to cultural reasons, and for fear of legal reprisals, immigrants are less often inclined to seek health services and primary care, and so they are admitted to hospital emergency wards at a more advanced and often irreversible stage of illness (Machado et al., 2007; Dias et al., 2008; Dias et al., 2009; Machado et al., 2010) One of the most important aspects involves the Place of Death and the variability of the quality of the registration, depending on the place. Also, the trend is toward death at the hospital, which rose 13,3%, from 54,2 to 61,4%, during the period being studied, with a drop from 35,8% to 29,9% of deaths at home (which includes homes and nursing and residential homes) and in other places such as the street and public places (from 10.0 to 8,7%). For 2008, these aspects were developed as a specific subchapter which will be suitable to discuss with regard to ages and causes, since ageing and death at an older age would lead authorities to presume more home deaths, and the still high percentage of deaths in other places suggests a number of sudden deaths and accidents that should not be neglected. Application for the 2010 SCML Award 158 Discussion With regard to Causes of Death, the record of a death requires the basis for indicating the cause of death, which shows that a percentage of 90,4% of the causes was decided on the basis of clinical data. The percentage of autopsies did not experience significant changes (around 6%) from 2000 to 2008. The number of those performed in the hospital decreased, from 43% to 36%, while it was twice the number of those at home. This finding could be explained by the sophistication of technology and access to hospital exams with suitable concrete diagnoses; however, as shall be seen further below, the number of unknown causes held steady throughout the period being studied. As for deaths at home and in other places, it is vital to have data regarding sudden death, to understand the increase in the number of autopsies, which still appears to be unavailable nationwide. As expected, the two leading causes of death are cancer and circulatory diseases, which will also be examined in chapter 5, through GDH bases. Cancer represented 20,6% of the total number of deaths in 2000 and 23,2% in 2008. This percentage is higher than the population increase, which is why there is a rise in mortality rate caused by this (per 100 000 population age 15 and up: 266,6 deaths in 2008 to 248,7 in 2000). Taking into account screenable tumors, a cause of premature death, a more unfavorable change was found for colo‐rectal and anal tumors (2,8% of the total number of deaths in 2000, 3,3% in 2004 and 3,6% in 2008), for a mortality rate of 41,2%ooo in 2008. Also, the mortality rate by a malignant female’s breast tumor was much higher (33,6%ooo). Ischemic Heart Disease (IHD) and stroke are responsible for 28,8% of all deaths that occurred in 2000. Unlike what was noticed for cancer, the relative importance of IHD‐ and stroke‐related deaths have been decreasing, and so, in 2008 the proportional mortality rate due to these two causes dropped to 21,6%, more noticeably for stroke (‐33,9%) than for IHD (‐16,2%). It should be emphasized/underlined that infectious, respiratory diseases and diabetes as causes of death are also identified as frequent. The mortality rate due to external causes decreased, but Application for the 2010 SCML Award 159 Discussion the mortality rate rose in 2000‐04, from 52,2 to 58,1 deaths per 100 000 population, thereby showing a lower figure in 2008 (48,8%ooo). A recent study by the Portuguese Road Safety Authority shows that 85% of deaths and 78% of serious injuries in road accidents occur in young males in the age group 18 to 24 years old. From 2003 to 2007, 16% of deaths and 18,7% of serious injuries also occurred in this age group (Trigoso, 2010). As for Data Quality, the information sent to the INE, based on the transcription of the death certificate by Civil Registration, is subject to a set of validations and always returned whenever errors are detected. If necessary, the Statistics Portugal also establishes contacts to clarify any queries or to request missing information, and only when the data quality control process is completed, tables are made for periodic disclosure or for specific figures requested. The figures obtained for 2000 and 2004 are based on information collected in hard copy format, via the death report in effect, which shall include not only the option where the status of the deceased is unknown for the variables in question. With regard to ‘Cause of death’, the use of a non‐specific code for cause of death (Symptoms, signs, abnormal exams and incorrectly defined causes) is an indicator of the quality of information regarding mortality rate by causes. The percentage of deaths to which this code was assigned decreased 12,6%, to 9,7% of the total number of deaths, from 2000 to 2004, only to rise again in 2008 (10,6%). Since it is consensual that determining causes of death is important for research and knowledge of epidemiology and for health policies, many authors discuss the source of the record (Polprasert et al., 2010), while proposing a verbal autopsy as a solution for countries with no official records but which can also be used in countries with such official records, as a way of validating the diagnosis, in cases where the clinical file cannot be accessed. A potential solution would be a precise, standardized verbal autopsy, on a sheet that has to be filled in and attached to the death certificate. The information is often given by family members, in a way that is not very objective, through repetition of what they were told during the occurrence. As a result, many deaths at home are referred to the immediate cause, thus limiting use of the records. Application for the 2010 SCML Award 160 Discussion The verbal autopsy involves filling in a detailed form, as applied by the local health‐care professional, with emphasis on symptoms and occurrences during the process as well as medication. The specific cultural or linguistic aspects should also be pointed out, influencing immigrants’ understanding and reply to specific questions, thus requiring linguistic support. The analysis of Potential Years of Life Lost (PYLL), which is vital when studying traditional mortality rates, enables the assessment of not only the number of deaths, but also the age at which they occur; therefore, this is a good indicator for identifying premature mortality, with greater emphasis (higher no. of PYLL) than at younger ages. Portugal is the country with the second highest PYLL figures by cancer among the EU15 (only France’s figures are higher), even though in every other country this is also one of the leading causes of premature mortality rate (Eurostat, 2009; OECD Health Data, 2009). Overall, the PYLL’s due to this cause is decreasing, but there is also a negative change, in a few screenable cancers such as colo‐rectal, anal and cervical cancers. Population‐based screenings for these malignant tumors are one of the strategies of the Portuguese National Program of Cancer Diseases, but the implementation is variable in the five ARSs (Regional Health Administrations), since they involve considerable organization and costs. External causes of injury or poisoning also account for a large chunk of the total PYLL (2008: 16,1%), largely due to road, home or leisure accidents, which are so prevalent in younger age groups. Cardiocerebrovascular diseases are another group of diseases highly representative of premature mortality, despite the positive change that has occurred in the last few years, in keeping with the trend shown in other EU countries. At the European level, this trend has been explained by multiple causes, namely increased wealth, better education and safety levels, less smoking and lower blood pressure, improved medical emergency and therapeutic intervention services (Cayotte et al., 2009). Application for the 2010 SCML Award 161 Discussion In Portugal, these improvements also occur, as they can justify the positive change over the last few years. The IHD and stroke Vias Verdes, a Portuguese national program for Coordinating Cardiovascular Diseases (Cruz Ferreira et al., 2010) has already obtained nationwide results, with very positive aspects in the Algarve and in the North Regions. However, smoking is on the rise among younger age groups, namely females, along with obesity (Atlas ACS, 2010). Other economic and social determinants and less appropriate lifestyles can also invert the situation. The significant increase in PYLL (absolute and rate) due to diseases linked to alcohol consumption (2000‐2008: relative increase of 130% in AVPP and 126% in the rate of AVPP) is also noteworthy. Practically all of the aforementioned causes are part of the list of those considered avoidable through primary prevention or through quality health care (see enclosed list). Due to the wealth of information it represents, this indicator of preventable mortality has also been proposed for measuring the performance of health systems and the quality of health care (Kossarova et al., 2009). The identification and analysis of preventable causes via primary prevention campaigns or through health care makes it possible to orient feasible strategies and with an impact on health status. The first set of causes – preventable through primary prevention – comprises tracheal, bronchial and lung cancer, cirrhosis of the liver and road accidents. Tracheal, bronchial and lung cancer was the only one that recorded a significant increase between 2000 and2008 (15080 to 16618). Since smoking is the leading cause of this cancer, once again there is a need to look at these figures and increased smoking among younger people as well as to design specific interventions in this regard. With the smoking ban in effect (Law no. 37/2007, dated 14 August), which approves rules for protecting citizens from involuntary exposure to tobacco smoke and measures for reducing demand linked to addiction and quitting the habit, a change in behavior with a positive impact on the results given is expected. Application for the 2010 SCML Award 162 Discussion The second group – preventable through health care – is headed by causes previously identified as being representative on the total of all the causes: cardiocerebrovascular (ischemic heart disease and stroke) and cancer (particular focus on screenable tumors). Finally, to examine the variables in greater detail, the place of death, in 2008 was considered. This variable was examined with each of the others, namely gender, age, place of residence, marital status, work status and occupation, nationality and cause of death, and the Chi‐square test for independence was performed for each case. There was rejection of the null hypothesis, with p<0,001 in all cases, that is, there is strong evidence that the place‐of‐death variable is linked to the other variables. The Chi‐square test provides information on the independence between the variables but not on the existing level of association; thus, measures of association were calculated, concluding that they exist but are not very intense (<0,3), in all cases. Hospital death (61,3%) was most frequent and statistically significant in men 45 to 74. Older women most often die at home. Death in the 15‐to‐24 age group occurs mostly in another place, that is, in the street or in a public place, mostly males (41,4% vs 28,6%), which matches figures obtained for accidents. Another noteworthy difference is nationality. Foreign citizens most often die in a public place other than the hospital or residence and due to external causes of injury which include accidents and murders, among others. The hospital is where 75% of people with cancer and over half the IHDs and strokes die. In the first case, this could be because of the low supply of palliative care, and, in the second, the probable sudden deaths at home or in public places. When examining the place of death, what draws attention is the fact that 25,5% of the incorrectly defined causes correspond to hospital death and with no autopsy result, which can be regarded as unacceptable, from a public health standpoint. Application for the 2010 SCML Award 163 Discussion Profiles according to the place of death show the following: for the hospital, Portuguese male, skilled workers, age 45 to 64, married and with residence in the Algarve; for the home, a Portuguese female, widowed, with residence in the North, aged over 85; for other places, a foreign male, young, with residence in the Alentejo, single, unskilled worker. Analysis of data coded through DRGs From 2000 to 2008, hospitalizations increased 32,6%. This is due to increasing life expectancy and more hospitalizations in older age groups and growing use of increasingly complex treatments and potential morbidity of cancer patients. An increase in hospitalizations was noticed in all age groups except for young people 15 to 24. Over 85 years old, as expected, there were 29 439 more hospitalizations in 2008 than in 2000, since there is a relation between the decline of functional capabilities in the elderly and in older adults and the increase in hospitalizations (Graf, 2008). Gender and age were simultaneously examined. There were more hospitalizations in women in every age group except ages 45 to 64, where there is an increase in male mortality rate and which includes causes sensitive to health care and to promoting health as well as premature deaths, which also occurs in other countries such as England (HES, 2007). The intra‐hospital lethality dropped 5,9% from 2000 to 2008. The trend toward a higher number of intra‐hospital deaths in males becomes less significant for ages over 75, as referred. Men and women simultaneously show different hospitalization risks and different risks of dying while hospitalized. The likelihood of hospitalization death is 5% higher in men than in women (CIHI, 2007). As for the area of residence, there are regional asymmetries: Lisboa e Vale do Tejo shows the biggest number of hospitalizations and deaths, in keeping with the results obtained in the 2004‐ 2010 NHP monitoring by Regions and NUTS III (NHP results in WEBSIG, ACS) and the Algarve Region shows very low figures. Application for the 2010 SCML Award 164 Discussion The WebSIG – Interactive Maps platform, from the Office of the High Commissioner for Health, makes it possible to examine various geographical distributions, including NUT III. Mortality rates by life cycle and specific causes of death as they evolve can be examined, while comparing them with reference values and targets, and through their geographical representation and at different scales. The fatality rates by NUTS III is lower in the Center and North regions and higher in the inner Center, Alentejo and Algarve regions, while they also decrease from South to North and from the Coast to the Interior. In 2008, the NUT III of the Alto Alentejo and Pinhal Interior Sul simultaneously show the highest intra‐hospital lethality rate and the highest mean age. According to CIHI (2007), age is one of the seven factors affecting the likelihood of a hospitalization death (the other six factors are gender, diagnosis, the existence of other co‐ morbidities, type of admission, delay in hospitalization and the need for transfer). If all the other factors were equal, the chance of dying would increase 5% for every year one ages. There were regional differences between the place of residence and the location of the hospital where the patient is admitted. This could depend on the access to equipment/public services, a determining factor characterizing the quality of the area and other factors that minimize the importance of distance when searching for care, namely, greater efficiency, greater accessibility ‐ cultural, organizational, waiting times – location of workplace/residence of close family and relatives, perception of the seriousness of illness, no family doctor assigned, etc. These aspects need to be examined, not only by age and cause of death, but also by the asymmetry of the geographical distribution of health‐related resources, namely human resources and equipment (Dussault and Fronteira, 2010). Causes of hospitalization were compared with those of death. Hospitalizations are mostly due to circulatory diseases, but there are others including respiratory diseases and malignant tumors, which are the biggest causes of death. In data collected at 82 Japanese hospitals, Miyata and others (2008) identified respiratory diseases as the leading cause of hospitalization and hospitalization death. After calculating the intra‐hospital lethality, there is a decrease in infectious, with malignant tumors and respiratory diseases experiencing the biggest increases during the period being studied. Tuberculosis and AIDS are among the most noteworthy infectious diseases; however, Application for the 2010 SCML Award 165 Discussion pneumonias and hospital‐acquired infections as a cause of in‐patient death should be analyzed as a strong factor determining hospital fatality. There are no data for Portuguese hospitals regarding hospitalization incidents and accidents, even though clinical risk management is one of the most important factors in the quality of care (Campos and Carneiro, 2010). The recent Portuguese National Quality Program approved by the relevant ministry and under the responsibility of the Directorate‐General for Health includes risk management as well as aspects inherent to patient safety. In 2010, a specific commission was appointed for approaching hospital‐acquired infection and anti‐microbial resistance (Ministerial Order from 2010). External causes have an altogether different profile: male features now show a trend toward an increase in females, although death is more significantly higher in men, with intra‐hospital fatality rate reaching 29,8%, compared to 4.3% for women. The increase in falls should also be pointed out (once again, linked to greater longevity in women and with less seriousness), as well as the decrease in road accidents and murders. As for circulatory diseases, in 2008, hospitalizations for ischemic heart disease (IHD) and for stroke account for some 40% of all hospitalizations for circulatory diseases and in‐patient deaths due to these two causes, 55% of the total number of deaths caused by circulatory diseases. In the last few decades, there was a continued decline in mortality rate due to ischemic heart disease – a disease of the coronary arteries, in Western countries, such as the USA, England or Finland; however, this trend does not occur in the stroke mortality rate (Copper et al., 2000). It should be pointed out that the mortality rate by this cause only exceeds the mortality rate by IHD in 2 European Union countries: Portugal and Greece (Mladovsky et al., 2009). There is also a clear SW‐NE European gradient when considering the cause of death due to ischemic heart disease (DIC) – WHO Framework – Europe Region. Deaths occurring outside the Hospital constitute most of the cases in every epidemiological study and, therefore, take on specific significance in Public Health. In the Finnish study, FINAMI (Salomma, 2003) accounted for 73% of deaths from ischemic heart disease for males and 60% for females, in the 35‐to‐64 age group. In the same study, the decline in IHD‐related mortality rate was proved and due to a decrease in death both intra‐hospital and outside the hospital. Application for the 2010 SCML Award 166 Discussion With regard to the cervical cancer‐related intra‐hospital lethality, there was no statistically significant difference between patients in the various age groups. Registered death diagnoses are all associated with neoplastic disease. In colo‐rectal cancer patients, there was an increase in the intra‐hospital mortality rate from 2000 to 2008, which was more pronounced in patients aged 85 and over. There is no difference between genders. With regard to death diagnoses, along with those linked to malignant disease, there were other diagnoses that could represent co‐morbidities or complications linked to treatment. The available data suggests that the intra‐hospital lethality in breast, cervical and colo‐rectal cancer patients, in the vast majority of cases, results in the advance of the primary cancer disease. This aspect brings us back to the issue of the place of death of cancer patients. Around ¾ of cancer patients (74,9%) died in the hospital or clinic. There are no significant differences between genders, or differences linked to the type of cancer. The percentage of home deaths is around 22%, while it is low in public places (about 3%). In Portugal, just like virtually every developed country, most cancer patients die in a hospital setting. This situation appears to differ from what is shown in several studies conducted in other countries: over half the people express their willingness to be treated at home, with the illness in its terminal stage (Higginson et al., 2000). Although no studies in Portugal have addressed this issue, the situation is likely to be similar to that in other countries. For a good quality of life in the terminal stage, it is vital that patients be treated with respect and dignity, without suffering, in a family setting, and in the company of family and friends. The lack of access to palliative home care is certainly one of the determining factors, though not the only one, rendering it unfeasible for patients to remain at home at the terminal stage, when they wish to do so. In Portugal, notwithstanding the progress achieved in providing palliative care, there is still a huge shortage of this type of assistance, thus placing the country near the bottom among European countries with regard to access to palliative care (Wright et al., 2006) Application for the 2010 SCML Award 167 Discussion A study conducted by the Economist Intelligence Unit evaluated the “quality of death” in 40 countries – 30 OECD and another 10 selected countries (Quality, 2010). To this end, it used a “quality‐of‐death index” to score countries with regard to four categories: the environment of basic end‐of‐life health care; the availability of end‐of‐life care; the cost of end‐of‐life care; and the quality of end‐of‐life care. Overall, Portugal’s score ranks 31st among the 40 countries. As concerns the score breakdown into the various categories, Portugal ranks as follows: 27th in the environment of basic end‐of‐ life health care; 38th in the availability of end‐of‐life care; 22nd in the cost of end‐of‐life care; and 27th in the quality of end‐of‐life care. Although in a few indicators Portugal ranks among the top countries with the best quality care, such as regarding the availability of opioid analgesics (Wright et al., 2006), Portugal still has a long way to go with regard to providing end‐of‐life care with the desired quality. Vital statistics generated through civil registration systems are the major source of continuous monitoring of births and deaths over time. The usefulness of vital statistics depends on their quality. Given the increasing availability of other measurements of adult mortality such as corrected sibling survival, corrected death registration data should be interpreted in the context of all other data sources. In the arena of child mortality, it is now standard practice to examine all data sources for a country over time and generate a composite estimate of levels and trends in child mortality. With improved DDMs, there continues to be a role for partial vital registration data in measuring adult mortality levels and trends. But such results should only be interpreted alongside all other data sources on adult mortality and the face validity of the resulting levels, trends, and age‐patterns of adult death considered (Murray et al., 2006) Valid, reliable and comparable measures of the health states of individuals and of the health status of populations are critical components of the evidence base for health policy. There is a need to develop population health measurement strategies that coherently address the relationships between epidemiological measures (such as risk exposures, incidence, and mortality rates) and multi‐domain measures of population health status, while ensuring validity and cross‐population comparability (Matters, 2003) Application for the 2010 SCML Award 168 Discussion The desired interconnection with hospital information systems could detect proximity to recent hospitalizations, with the two‐fold advantage of better clarifying the cause of death while providing data for evaluating the quality of assistance in clinical follow‐up. Application for the 2010 SCML Award 169 Conclusions and Recommendations 8. Conclusions and Recommendations Questions to be answered What is the level of quality of Portuguese death registration and the adequacy of the items registered with regards to the needs of epidemiological knowledge? Mortality based on death certifications Conclusion 1. The highest percentage of missing data is related to socioeconomic characterization, especially occupation and education. Recommendation – The filling‐in of field Occupation must be mandatory. In case the deceased was non‐active, his active‐age occupation should be registered. Education‐related fields should be added. Conclusion 2. The proportion of ill‐defined causes of death is still high in Portugal and it has increased between 2004 and 2008. It is particularly high for deaths occurring at home. Recommendation – (i) Doctors who are responsible for death certification, as well as those who codify the cause of death should have access to medical records to determine the correct cause of death, namely information gathered at different levels of healthcare (family doctor, long term care, hospital care); (ii) There should exist a quality control process to verify attribution of cause of death, with periodic evaluation, comparing the deceased health information available with the cause of death assigned to him. Diagnosis‐related Groups (DRGs) Coding Conclusion 3. Some inconsistencies in the DRG data base were found: (i) men and women between 65 and 84 years old discharged with complications in pregnancy, childbirth and puerperium; (ii) women discharged for cancer of prostate; (iii) people ageing > 150 years (one with 1071 years); (iv) recorded autopsies on alive patients and with hospital discharge code. Recommendation– Reviewing system’s structure by (i) prohibiting the registration of certain causes (ICD) in a gender when they are specific to the opposite sex, (ii) limiting the age and (iii) not allowing the registration of autopsies when the cause of hospital discharge does not refer to a death. Application for the 2010 SCML Award 170 Conclusions and Recommendations Conclusion 4. The analysis of variables related to socio‐economic status contributes to a more comprehensive and multi‐sectoral concept of health. The items currently included on the databases either do not allow the analysis of social determinants of health or they have gaps in what concerns their filling. As an example, the place of residence, an item demonstrating a strong association with health, is not well recorded. Recommendation – (i) Adding items related to social determinants of health; (ii) mandatory filling of the place of residence with reference to the official codes of the administrative division (DICOFRE9); (iii) for expatriates, listing of a specific and universally accepted code (e.g. those used by Eurostat and OECD) to identify the country of residence. Conclusion 5. It is not possible to cross and match the analyzed databases and a large and diverse number of information systems were identified at different levels of health care which do not allow any type of interoperability between them. Recommendation – (i) Focusing on the interoperability between information systems so that the health data could be crossed with other information, including the death certificate or other Ministries’ databases (e.g. the MTSS’s database on the allocation of allowances for disability); (ii) single clinical process computerized. What is the impact of premature death and avoidable death considered amenable to health care on the overall mortality? Conclusion 6: Among cardiovascular diseases, the most representative are stroke and ischemic heart disease (IHD), which totalized 8,4% of total PYLL in 2008. Recommendation: Continue with the public campaigns on stroke and IHD, created by the Office of the High Commissioner for Health (ACS) and increase investment on the expansion of IHD and stroke Vias Verdes to the whole national territory. Conclusion 7: Screenable cancers are more sensitive to interventions holding a higher potential to decrease. They represent 6,5% of total PYLL in 2008. The colon and rectum cancer is the most 9 Respecting the Official Administrative Charter of Portugal (CAOP).DI refers to the district, CO to the municipality and FRE to parish 171 Application for the 2010 SCML Award Conclusions and Recommendations expressive and also the one whose population‐based screening program is the least developed, showing a greater asymmetry in terms of population coverage among the different Health Regions and less consensus among the technique that should be applied. Recommendation: (i) Consensual definition of the most cost‐effective colon‐rectum cancer’s screening technique, which must be extended to all Health Regions; (ii) increasing investment to expand population coverage; (iii) ensuring high rates of participation. Conclusion 8: All causes listed above are also, at certain ages, considered amenable to adequate health care. Thus, one may conclude that these causes have a great potential to be reduced through adequacy of care, in terms of access, equity, quality and efficiency. Recommendation: These causes should be prioritized and analyzed from a macro scale of intervention (national policies) to a micro level (the level of Healthcare Centre Groups) Are the age and cause of death decisive in the place of death (hospital, residence or other location)? Conclusion 9: Age and causes of death are significantly related to place of death. Considering all age groups and adult mortality, deaths in hospital/clinic are more frequent (61,4%) than deaths at home (29,9%) or at public places (8,7%). For deaths that occurred at hospital/clinic, the most frequent age groups are the central ones (45‐74 years); for deaths at home, 75 years and over are the predominant age group, while deaths at public places are more common for the youngest age groups (15‐24 years). For most of major groups of causes, death occurs in hospital/clinic in more than 70% of the cases. Regarding ischemic heart disease and stroke, the difference between the percentages of deaths in hospital/clinic and at home is smaller. For these two causes, as well as for Diabetes Mellitus and alcohol abuse, the percentage of deaths at home varies between 25‐40%. The percentage of deaths in public places is higher when the cause is external (34,4%) or ill‐defined (22,7%). Recommendation: There is a need of further research to design adequate and specific interventions. Application for the 2010 SCML Award 172 Conclusions and Recommendations What are the pathologies associated to death due to a cardiovascular disease and cancer that are decisive as a risk of death? Conclusion 10: Admissions due to IHD and stroke include other diagnosis as essential hypertension, disorders of the lipoid metabolism and diabetes, in both genders. However patients who died were admitted with the cardiac dysrhythmia as the most important associated pathology. The disorders of the lipoid metabolism are not referred in the top‐five associated pathologies. Admissions and death‐associated pathologies due to cancer are usually related to metastasis of the primary diagnosis or anaemia. Recommendations: Patients admitted with cardiac dysrhythmia associated to IHD or stroke should be carefully monitored and probably need Intensive Care. Application for the 2010 SCML Award 173 Bibliography Bibliography Abouzahr C, Gollogly L, Stevens G. Better data needed: everyone agrees, but no one wants to pay. Lancet 2010;375(9715):619‐21. Abreu P. Comunicação e Medicina. Ed. Virtualidade, Coimbra; 1996. Alto Comissariado da Saúde. Atlas do Plano Nacional de Saúde. Ed. Alto Comissariado da Saúde, Lisboa; 2010. Campos L, Carneiro A. A Qualidade no PNS 2011‐2016. Ed. Alto Comissariado da Saúde, Lisboa; 2009. Canadian Institute for Health Information. HSMR: A New Approach for Measuring Hospital Mortality Trends in Canada. Ed. Canadian Institute for Health Information, Ottawa; 2007. Carrilho M. A situação demográfica recente em Portugal. Revista de estudos demográficos 2009; 46: 59‐108. Claxton‐Oldfield S, Gosselin N, Claxton‐Oldfield J. Imagine you are dying: would you be interested in having a hospice palliative care volunteer? Am J Hosp Palliat Care. 2009; 26(1):47‐51. Conselho nacional de ética para as ciências da vida. Parecer sobre aspectos éticos dos cuidados de saúde relacionados com o final da vida. Ed. Presidência do Conselho de Ministros, Lisboa; 2005. Cooper R, Cutler J, Desvigne‐Nickens P, Fortmann P, Friedman L, Havlik R, Hogelin G, Marler J, McGovern P, Morosco G, Mosca L, Pearson T, Stamler J, Stryer D, Thom T. Trends and Disparities in Coronary Heart Disease, Stroke, and Other Cardiovascular Diseases in the United States: findings of the national conference on cardiovascular disease prevention. Circulation 2000; 102(25):3137‐49. Cruz R, Neves R, Rodrigues V. Vias Verdes Coronária e do Acidente Vascular Cerebral. Indicadores de actividade. Ed. Alto Comissariado da Saúde, Lisboa; 2010. Dias S, Severo M, Barros H. Determinants of health care utilization by immigrants living in Portugal. BMC Health Serv Res 2008; 8:207‐13. Application for the 2010 SCML Award 174 Bibliography Dias S, Cortes M, Cargaleiro H, Carreira M, Silva A, Alarcão V, Horta R, Lemos M. Impact of length of stay, legal status and the other social demographics determinants in use of health care services by migrants. Eur J Public Health 2009; 19(1):159. DH. End of Life Care Strategy: Second Annual Report. Ed. Department of Health, London; 2010. Dussault G, Fronteira I. Human Resources for Health (HRH) Plan Component of National Health Plan 2011‐16. Ed. Alto Comissariado da Saúde, Lisboa; 2009. Economic Intelligence Unit. The Quality of Death: Ranking end‐of‐life care across the world. [cited 2010 Nov]. Available from: http://graphics.eiu.com/upload/QOD_main_final_edition_Jul12_toprint.pdf Emanuel E, Fairclough D, Slutsman J, Alpert H, Baldwin D, Emanuel L. Assistance from family members, friends, paid care givers, and volunteers in the care of terminally ill patients. The N Engl J Med 1999; 341(13):956‐63. Fall K, Garmo H, Andrén O, Axelson A, Adolfsson J, Adami H, Johansson J, Holmberg L. Prostate‐ Specific Antigen Levels as a Predictor of Lethal Prostate Cancer. J Natl Cancer Inst 2007; 99(7): 526‐32. Fernandes, H. Reflectindo sobre a morte do doente oncológico. Enfermagem Oncológica. 1999; 9: 38‐40. Fernandes, M. Cuidar de um doente em fase terminal. Enfermagem Oncológica. 1999;12:20‐24. Ferreira M, Felix N. Interoperabilidade numa perspectiva Hospitalar. Braga: Universidade do Minho; ano? [cited 2010 Nov]. Available from: http://www3.di.uminho.pt/~prh/uce15‐ 0809/g42.pdf Fried TR, O´Leary MA. Using the Experiences of Bereaved Caregivers to Inform Patient‐ and Caregiver‐centered Advance Care Planning. J Gen Intern Med 23(10):1602–7. Frosch DL, Kaplan RM. Shared decision making in clinical medicine: past research and future directions. Am J Prev Med 1999;17:285‐94. Gakidou E, King G. Estimating adult mortality without selection bias from sibling survival data. Demography 2006;43(3):569‐85. Application for the 2010 SCML Award 175 Bibliography Garcell G, Arzola E, Isla J, Zaldivar E, Montero P. Tendencias de la morbilidad y letalidad hospitalaria por câncer. An Med Interna 2007;24(1):12‐14. Girgis A, Johnson C, Currow D, Waller A, Kristjanson L, Mitchell G, Yates P, Neil A, Kelly B, Tattersall M, Bowman D. Palliative Care Needs Assessment Guidelines. Ed. The Centre for Health Research & Psycho‐oncology, Newcastle; 2006. Gonçalves J, Costa L. El equipo interdisciplinar en cuidados paliativos. Conflito del equipo e su resolución. In: Trill M, Imedio M, editors. Aspectos Psicológicos en Cuidados Paliativos. La comunicación con el enfermo y família. Ed. Ades Ediciones, Madrid; 2000. p.601‐9. Graf C. The Hospital admission Risk Profile (HARP). Ed. Hartford Institute for Geriatric Nursing, New York; 2008. Haene I, Stichele R, Pasman H, Noortgate N, Bilsen J, Mortier F, Deliens L. Policies to improve end‐of‐life decisions in Flemish hospitals: communication, training of health care providers and use of quality assessments. BMC Palliat Care 2009;8:20. Heckman J. Skill formation and the economics of investing in disadvantaged children. Science 2006; 312(5782):1900‐02. Heijink R, Koolman X, Pieter D, Veen A, Jarman B, westert G. Measuring and explaining mortality in Dutch hospitals; The Hospital Standardized Mortality Rate between 2003 and 2005. BMC Health Serv Res 2008; 8: 73‐81. Higginson J, Sen‐Gupta J. Place of care in advanced cancer: a qualitative systematic literature review of patient preferences. J Palliat Med 2000;3: 287‐300. Higginson I, Finlay I, Goodwin D, Cook A, Hood K, Edwards A, Douglas H, Norman C. Do Hospital‐ Based Palliative Teams Improve Care for Patients or Families at the End of Life? J Pain Symptom Manage 2002; 23(2): 96‐106. Hogg R, Craig A. Introduction to mathematical statistics. 5th ed. Prentice Hall, Inc., New Jersey; 1995. Instituto Nacional de Estatística (INE). Óbitos por Causas de morte. Documento metodológico. Ed. INE, Lisboa; 2009. Application for the 2010 SCML Award 176 Bibliography Jacobs LG, Bonuck K, Burton W, Mulvihill M. Hospital Care at the End of Life: An Institutional Assessment. J Pain Symptom Manage 2002;4: 291‐8. Johnson S, Abonyi S, Jeffery B, Hackett P, Hamptom M, McIntosh T, Martz D, Muhajarine N, Petrucka P, Sari N. Recommendations for action on the social determinants of health: a Canadian perspective. Lancet 2008; 372(9650):1690‐3. Jonen‐Thieleman I. Organization of palliative medicine in the clinic and ambulatory care. Zentralbl Chir 1998;123(6): 640‐8. Juel K, Christensen K. Sex mortality differences in Denmark 1840‐2005. Women live longer than men, but great changes during the last 50 years. Ugeskr Laeger 2007; 169(25):2398‐2403. Juel K. Life expectancy and mortality in Denmark compared to Sweden. What is the effect of smoking and alcohol? Lancet 2008; 170(33):2423‐30. Kossarova L, Holland W, Nolte E, McKee M. Measuring ‘Avoidable’ Mortality, Methodological note. London: School of Economics and Political Scienc; 2009. Kunst A, Rios M, groenhof F, Mackenbach J. Socioeconomic inequalities in stroke mortality among middle‐aged men: an international overview. Stroke, 1998; 29(11): 2285‐91 Latado A, Passos L, Braga J, Santos A, Guedes R, Moura S, Almeida D. Preditores de Letalidade Hospitalar em Pacientes com Insuficiência Cardíaca Avançada. Arq Bras Cardiol 2006; 87(2):185‐ 91. Lefèvre H, Jougla E, Pavillon G, Le Toullec A. Gender differences in premature mortality and avoidable deaths. Rev Epidemiol Sante Publiqu 2004; 52(4):317‐31. Lin C, Farrel M, Lave J, Angus D, Barnato A. Organizational Determinants of Hospital End‐of‐Life Treatment Intensity. Med Care 2009; 47(5):524‐30. Lopez AD, Mathers CD, Ezzati M, Jamison DT, Murray CJ. Global and regional burden of disease and risk factors, 2001: systematic analysis of population health data. Lancet. 2006;367(9524):1747‐1757. Lopez AD, Mathers CD. Measuring the global burden of disease and epidemiological transitions: 2002‐2030. Ann Trop Med Parasitol 2006; 100(5‐6):481‐99. Application for the 2010 SCML Award 177 Bibliography Lopez AD, AbouZahr C, Shibuya K, Gollogly L. Keeping count: births, deaths, and causes of death. Lancet 2007;370(9601):1744‐6. Luijkx KG, Schols JM. Volunteers in palliative care make a difference. J Palliat Care. 2009;25(1):30‐9. Lutz W, Scherbov S. Future Demographic change in Europe: the contribution of migration in Europe and its immigrants in the 21st century new deal on a continuing dialogue of the deaf? Ed. Migration Policy Institute and Luso‐American Foundation, Washington; 2006. Macedo M, Lima M, Silva A, Alcântara P, Ramalhinho V, Carmona J. Prevalência, Conhecimento, Tratamento e Controlo da Hipertensão em Portugal. Estudo PAP. Rev. Port. Cardio 2007;26:21‐ 39. Machado MC, Santana P, Carreiro MH, Nogueira H, Dias A, Barroso R. Iguais ou Diferentes? Cuidados de saúde materno‐infantil a uma população de imigrantes. Ed. Bial, Lisboa; 2006. Machado MC, Pereira F, Machaqueiro S. Approaches to migrant health in Portugal. Eurohealth 2010;16(1):30‐1. Maciel M. Morte no domicílio: Experiência da equipe de Cuidados Paliativos do Hospital do Servidor Público Estadual de São Paulo. [cited 2005 Mar]. Available from: http://www.cuidadospaliativos.com.br/artigo.php?cdTexto=218 Mahapatra P, Shibuya K, Lopez AD, Coullare F, Notzon FC, Rao C, Szreter S . Civil registration systems and vital statistics: successes and missed opportunities. Lancet 2007; 370:1653‐63. Marmot M. Interim first report on social determinants of health and the health divide in the WHO European Region. Ed. WHO‐Europe, Copenhagen; 2010. Mathers CD, Murray CJL, Ezzati M, Gakidou E, Salomon JA, Stein C. Population health metrics: crucial inputs to the development of evidence for health policy. Popul Health Metr 2003; 1:6. Mathers CD, Murray CJ, Salomon JA, Sadana R, Tandon A, Lopez AD, Ustün B, Chatterji S. Healthy life expectancy: comparison of OECD countries in 2001. Aust N Z J Public Health 2003;27(1):5‐ 11.(a) Application for the 2010 SCML Award 178 Bibliography Mathers C, Fat D, Inoue M, Rao C, Lopez A. Counting the dead and what they died from: an assessment of the global status of cause of death data. Bull World Health Organ 2005;83(3):171‐ 7. Mathers CD, Boerma T, Ma Fat D. Global and regional causes of death. Br Med Bull 2009; 92:7‐ 32. Mazanec P, Tyler M. Cultural Considerations in End‐of‐Life Care ‐ How ethnicity, age, and spirituality affect decisions when death is imminent. Am J Nurs 2003;103(3):50‐8. Ministério da Saúde. A Declaração de Óbito Documento necessário e importante. Ed. Ministério da Saúde, Basília; 2009. Miyata H, Hashimoto H, Horiguchi H, Matsuda S, Motomura N, Takamoto S.Performance of in‐ hospital mortality prediction models for acute hospitalization: Hospital Standardized Mortality Ratio in Japan. BMC Health Serv Res 2008; 8: 229‐38. Mladovsky P. Allin S, Masseria C, Hernández‐Quevedo C, McDaid D, Mossialos E. Health in European Union. Trends and Analysis. Ed. Observatory on Health Systems and Policies; 2009 Murray S, Boyd K, Kendall M, Worth A, Benton T, Clausen H. Dying of lung cancer or cardiac failure: prospective qualitative interview study of patients and their carers in the community. Br Med J 2002; 325(7370): 915‐21. Murray CJL, Kulkarni SC, Ezzati M. Understanding the coronary heart disease versus total cardiovascular mortality paradox: a method to enhance the comparability of cardiovascular death statistics in the United States. Circulation 2006; 113(17):2071‐81. Murray CJL, Rajaratnam JK, Marcus J, Laakso T, Lopez A. What Can We Conclude from Death Registration? Improved Methods for Evaluating Completeness. PLoS Med 2010;7(4):e1000262. Moura P, Simões A, Lopes S, Lourenço A, Silva P. O doente terminal, aspectos práticos. Medicina Interna 1995; 2(3): 181‐5. Natan M, Garfinkel D, Shachar I. End‐of‐life needs as perceived by terminally ill older adult patients, family and staff. Eur J Oncol Nurs 2010; 14(4): 299‐303. Application for the 2010 SCML Award 179 Bibliography Nicolau R, Machado, A, Falcão J, Lira M. Distribuição dos Internamentos Hospitalares em Portugal Continental: Agregação geográfica e determinantes. Ed. INSA, Lisboa; 2009. Nolte E, McKee M. Does care save Lives? Avoidable mortality revisited. Ed. The Nuffield Trust, London; 2004. Nolte E, McKee M. Measuring the Health of Nations: updating an earlier analysis. Health Aff 2008; 27(1): 58‐71. Nunes A. Preparação dos profissionais de enfermagem para o acompanhamento de doentes em situação terminal de vida [master's thesis]. Lisboa: Instituto Superior de Psicologia Aplicada; 2005. Peixoto H, Souza M. O Indicador Anos Potenciais de Vida Perdidos e a Ordenação das Causas de Morte em Santa Catarina, 1995. IESUS 1999;8(1):17‐25. Pereira M. Comunicação de más notícias em saúde e gestão do luto ‐ Contributos para a formação em enfermagem [PhD thesis]. Porto: Faculdade de Psicologia e de Ciências de Educação da Universidade do Porto; 2005. Pestana MH, Gageiro JN. Análise de dados para as ciências sociais. A complementaridade do SPSS. 3rd ed. Edições Sílabo, Lisboa; 2003. Pinto, C. O respeito no cuidado de enfermagem: perspectiva do doente terminal [master's thesis]. Porto: Faculdade de Medicina da Universidade do Porto; 2003. Polprasert W, Rao C, Adair T, Pattaraarchacai J, Porapakkham Y, Lopez AD. Cause‐of‐death ascertainment for deaths that occur outside hospitals in Thailand: application of verbal autopsy methods. Popul Health Metr 2010; 8: 13‐28. Rabiais S, Braco M, Falcão J. Atlas da mortalidade por doenças não neoplásicas em Portugal 1999‐2001. Ed. INSA, Lisboa; 2004. Rajaratnam JK, Marcus JR, Levin‐Rector A, Chalupka NA, Wang H, Dwyer L, Costa M, Lopez AD, Murray CJL. Worldwide mortality in men and women aged 15‐59 years from 1970 to 2010: a systematic analysis. Lancet 2010; 375(9727):1668‐70. Application for the 2010 SCML Award 180 Bibliography Rosa M, Santos H, Seabra T. Contributos dos Imigrantes na Demografia Portuguesa: o papel das populações de nacionalidade estrangeira. Ed. Alto‐Comissariado para a Imigração e Minorias Étnicas (ACIME), Lisboa; 2004. Salomaa V, Ketonen M, Koukkunen H, Immonen‐Räihä P, Jerkkola T, Kärjä‐Koskenkari P, Mähönen M, Niemelä M, Kuulasmaa K, Palomäki P, Mustonen J, Arstila M, Vuorenmaa T, Lehtonen A, Lehto S, Miettinen H, Torppa J, Tuomilehto J, Kesäniemi YA, Pyörälä K. Decline in Out of Hospital Coronary Heart Disease Deaths: The FINAMI Study. Circulation 2003;108:691‐6. Santana P. Poverty, social exclusion and Health. Soc Scienc & Medic 2002;55:132‐45. Santana P. Geografias da saúde e do desenvolvimento. Evolução e tendências em Portugal. Ed. Almedina, Coimbra; 2005. Scott S. Life‐Support Interventions at the End of Life: Unintended Consequences. Am J Nurs 2010; 110(1):32‐9. Slobbe L, Arah O, Bruin A, westert G. Mortality in Dutch hospitals: Trends in time, place and cause of death after admission for myocardial infarction and stroke. An observational study. BMC Health Serv Res 2008; 8: 52‐63. Souza L, Souza L, Souza A. A ética no cuidado durante o processo de morrer: relato de experiência. Rev Bras Enferm 2005; 58(6): 731‐5. Subramanian SV, Elwert F, Christakis N. Widowhood and mortality among the elderly: the modifying role of neighborhood concentration of widowed individuals. Soc Sci Med 2008; 66:873‐84. Tilden V, Thompson S. Policy issues in end‐of‐life care. J Prof Nurs 2009;25(6)363‐8. Tilden VP, Thopmson SRN. Policy issues in end‐of‐life care. J Prof Nurs. 2009; 25: 363‐8. Tovim D, Woodman R, Harrison J, Pointer S, Hakendorf P, Henley G. Measuring and reporting mortality in hospital patients. Ed. Australian Institute of Health and Welfare, Camberra; 2009. Treurniet H, Boshuizen H, Harteloh P. Avoidable mortality in Europe (1980–1997): a comparison of trends. J Epidemiol Community Health 2004; 58: 290‐5. Application for the 2010 SCML Award 181 Bibliography Trigoso JM. Dimensão e características dos acidentes rodoviários com jovens 18‐24. Presented at: jovens 18‐24 anos e sinistralidade rodoviária; 2010 Oct 25‐26; Lisboa. Rosenberg, Steven A. Human cancer immunotherapy: progress and problems. Paper presented at: Cancer Vaccines 2005: Barriers, Endpoints & Opportunities; 2005 Oct 5‐7; New York, NY. Tu J, Nardi L, Fang J, Liu J, Khalid L, Johansen H. National trends in rates of death and hospital admissions related to acute myocardial infarction, heart failure and stroke, 1994–2004. Can Med Assoc J 2009; 180(13): 118‐25. Veiga A, Barros C, Couto P, Vieira P. Pessoa em fase final de vida: que intervenções terapêuticas de enfermagem no serviço de urgência? Referência 2009; 2(10): 47‐56. Washington State Department of Health. Guidelines for Using Confidence Intervals for Public Health Assessment. Washington: Washington State Department of Health; 2002 Jan 8. [cited 2010 Nov]. Available from: http://www.doh.wa.gov/data/guidelines/confintguide.htm Winkleby M, Sundquist K, Cubbin C. Inequities in coronary heart disease incidence and case fatality by neighbourhood deprivation. Am J Prev Med 2007; 32(2):97‐106. Wingate S, Wiegand D. End‐of‐Life Care in the Critical Care Unit for Patients with Heart Failure. Crit Care Nurse 2008; 28(2): 38‐45. Wood J, Smith C. End‐of‐life care: preparing patients and families. Nat Rev Urol 2010; 7(8): 425‐ 34. Wright M, Wood J, Lynch T, Clark D. Mapping levels of palliative care development: a global view International Observatory on End of Life Care. Lancaster: Lancaster University; 2006 [cited 2010 Nov]. Available from: http://www.eolc‐observatory.net/global/pdf/world_map.pdf WHO. Global action against cancer. Ed. World Health Organization/UICC, Geneva; 2003. Application for the 2010 SCML Award 182 Bibliography Other sources: www.ine.pt http://portalcodgdh.min‐saude.pt/index.php/P%C3%A1gina_principal http://epp.eurostat.ec.europa.eu/portal/page/portal/eurostat/home/ http://www.hesonline.nhs.uk Application for the 2010 SCML Award 183 Annex Annex 1 Codes from the 9th and 10th International Statistical Classification of Diseases and Related Health Problems (ICD) revisions (selected causes) Cause of death ICD‐9 ICD‐10 Total 001‐E999 A00‐Y89 Infectious and parasitic diseases 001‐139 A00‐B99 Malignant neoplasms 140‐208 C00‐C97 Screenable Colon, rectum and anus 153‐154 C18, C19‐C20‐C21 Female breast 174‐175 C50 Cervix uteri 180 C53 Diabetes mellitus 250 E10‐E14 Alcohol abuse 291,303 F10 Ischemic heart diseases 410‐414 I20‐I25 Stroke 430‐438 I60‐I69 Diseases of the respiratory system 460‐519 J00‐J99 Diseases of the digestive system 520‐579 K00‐K93 Diseases of the skin and subcutaneous tissue 680‐709 L00‐L99 Diseases of the musculoskeletal system/connective tissue 710‐739 M00‐M99 Diseases of the genitourinary system 580‐629 N00‐N99 Symptoms, signs, abnormal findings, ill‐defined causes 780‐799 R00‐R99 External causes of injury and poisoning E800‐E999 V01‐Y89 Source: International Statistical Classification of Diseases and Related Health Problems, 9th e 10th revisions – ICD‐9 and ICD‐10. Application for the 2010 SCML Award i Annex Annex 2 Codes from the 9th and 10th International Statistical Classification of Diseases and Related Health Problems (ICD) revisions (amenable causes of death due to primary prevention and health care) Cause of death ICD‐9 ICD‐10 Sensitive to primary prevention Malignant neoplasm of trachea, bronchus and lung 162 Cirrhosis of liver 571 C33‐C34 K70.3, K71.7, K74.3, K74.4, K74.5, K74.6 V02‐V04, V09, V12‐V14, V19‐V79, V86‐V89 Motor vehicles accidents Sensitive to health care Intestinal infections (0‐14 years) Tuberculosis Other infectious (Diphtheria, Tetanus, Poliomyelitis) Whooping cough and measles (0‐14 years) Septicaemia Malignant neoplasm of colon and rectum Malignant neoplasm of skin E810‐E825 001‐009 010‐018, 137 032, 037, 045 33, 55 38 153‐154 A00‐A09 A15‐A19, B90 A36, A35, A80 A37, B05 A40‐A41 C18‐C21 173 C44 Malignant neoplasm of breast 174 C50 Malignant neoplasm of cervix uteri 180 C53 Malignant neoplasm of other parts of the uterus (0‐44 179, 182 C54, C55 years) Malignant neoplasm of testis 186 C62 Hodgkin’s disease 201 C81 Leukaemia (0‐44 years) 204‐208 C91‐C95 Diseases of the thyroid 240‐246 E00‐E07 Diabetes mellitus (0‐49 years) 250 E10‐E14 Epilepsy 345 G40‐G41 Chronic rheumatic heart disease 393‐398 I05‐I09 Hypertensive disease 401‐405 I10‐I13, I15 Ischemic heart disease 410‐414 I20‐I25 Stroke 430‐438 I60‐I69 All respiratory diseases (excl. pneumonia/influenza) (1‐ 460‐479, 488‐519 J00‐J09, J20‐J99 14 years) Influenza 487 J10‐J11 Pneumonia 480‐486 J12‐J18 Peptic ulcer 531‐533 K25‐K27 Appendicitis 540‐543 K35‐K38 Abdominal hernia 550‐553 K40‐K46 Cholelithiasis and cholecystitis 574‐575.1 K80‐K81 Nephritis and nephrosis 580‐589 N00‐N07, N17‐N19, N25‐N27 Benign prostatic hyperplasia 600 N40 Complications of pregnancy, childbirth and puerperium 630‐676 O00‐O99 Certain conditions originating in the perinatal period 760‐779 P00‐P96, A33, A34 Congenital cardiovascular anomalies 745‐747 Q20‐Q28 Misadventures to patients during surgical and medical E870‐E876, E878‐ Y60‐Y69, Y83‐Y84 care E879 For the calculation of the Potential Years of Life Lost for this groups of causes were considered the deaths from 0‐69 years, except when other age‐group is referred Source: Nolte et al, 2004. Application for the 2010 SCML Award ii Annex Annex 3 Confidence interval of the mortality rate by sex and age‐group 2000 2004 1 Total Gender: M F Age‐group: 15 ‐ 24 years 25 ‐ 44 years 45 ‐ 64 years 65 ‐ 74 years 75 ‐ 84 years 85 and up 1 Per 1000 population. Source: INE, 2010. 2008 1 1 DR (95% CI) 12,1 (12,0;12,2) DR (95% CI) 11,4 (11,3;11,4) DR (95% CI) 11,5 (11,4;11,6) 13,2 (13,1;13,3) 11,1 (11,0;11,2) 0,8 (0,8;0,9) 1,7 (1,6;1,7) 5,9 (5,8;6,0) 21,8 (21,5;22,1) 63,5 (62,8;64,2) 185,7 (183,4;187,9) 12,4 (12,3;12,5) 10,5 (10,4;10,5) 0,6 (0,5;0,6) 1,4 (1,3;1,4) 5,3 (5,2;5,4) 19,0 (18,7;19,2) 57,2 (56,6;57,8) 176,6 (174,5;178,7) 12,3 (12,2;12,5) 10,7 (10,6;10,8) 0,4 (0,4;0,5) 1,1 (1,1;1,2) 5,1 (5,0;5,2) 17,0 (16,8;17,3) 52,7 (52,1;53,2) 174,5 (172,6;176,4) Annex 4 Evolution of the mortality rate by age‐group and gender 2000 DR Death. 8198 99025 12,1 8463 15 ‐ 24 years M F 712 691 875 260 25 ‐ 44 years M F 1427 1453 45 ‐ 64 years M F 2008 Variation 2000‐08 (%) DR Pop (x103) Death. DR Pop Death. DR 96249 11,4 8595 98840 11,5 4,8 ‐0,2 ‐4,8 1,2 0,4 645 622 519 185 0,8 0,3 586 563 343 133 0,6 0,2 ‐17,6 ‐18,4 ‐60,8 ‐48,8 ‐52,4 ‐37,3 3549 1271 2,5 0,9 1513 1522 3084 1133 2,0 0,7 1528 1524 2427 993 1,6 0,7 7,1 4,9 ‐31,6 ‐21,9 ‐36,1 ‐25,5 1106 1216 9100 4618 8,2 3,8 1173 1274 8826 4242 7,5 3,3 1247 1347 9048 4116 7,3 3,1 12,8 10,8 ‐0,6 ‐10,9 ‐11,8 ‐19,6 65 ‐ 74 years M F 417 521 12522 7958 30,0 15,3 438 540 11443 7108 26,1 13,2 436 534 10280 6240 23,6 11,7 4,5 2,6 ‐17,9 ‐21,6 ‐21,4 ‐23,5 75 ‐ 84 years M F 206 309 16460 16215 80,1 52,4 233 354 17031 16590 73,0 46,8 260 392 17676 16690 68,0 42,5 26,4 26,9 7,4 2,9 ‐15,1 ‐18,9 9113 205,6 17084 176,5 48 100 9206 16882 193,8 168,4 58 119 11024 189,3 19870 167,2 31,4 22,8 21,0 16,3 ‐7,9 ‐5,3 Age‐group and gender: Death. 2004 Pop (x103) Total Pop (x103) 85 and up M 44 F 97 1 Per 1000 population. Source: INE, 2010. 1 Application for the 2010 SCML Award 1 1 iii Annex Annex 5 Number and percentage of death in 2008 by gender, age‐group and marital status Total M F Total Death % 50798 100,0 48042 100,0 15 a 24 Death % 343 133 100,0 100,0 25 a 34 Death % 790 100,0 305 100,0 35 a 44 Death % 45 a 54 Death % 1637 688 100,0 100,0 3485 1463 100,0 100,0 55 a 64 Death % 65 a 74 Death % 5563 100,0 10280 100,0 2653 100,0 6240 100,0 75 and up Death % 28700 36560 100,0 100,0 Marital status: Single M F Married M F Divorced M F Widower M F Unknown M F 5926 5815 11,7 12,1 335 121 97,7 91,0 591 180 74,8 59,0 794 219 48,5 31,8 920 244 26,4 16,7 712 338 12,8 12,7 883 648 8,6 10,4 1691 4065 5,9 11,1 31652 13036 62,3 27,1 8 9 2,3 6,8 166 96 21,0 31,5 646 369 39,5 53,6 1986 900 57,0 61,5 3953 1703 71,1 64,2 7842 3175 76,3 50,9 17051 6784 59,4 18,6 2360 1651 4,6 3,4 0 3 0,0 2,3 31 22 3,9 7,2 177 72 10,8 10,5 498 217 14,3 14,8 625 245 11,2 9,2 498 294 4,8 4,7 531 798 1,9 2,2 10732 27396 21,1 57,0 0 0 0,0 0,0 1 4 0,1 1,3 14 25 0,9 3,6 65 92 1,9 6,3 244 358 4,4 13,5 1023 2109 10,0 33,8 9385 24808 32,7 67,9 128 144 0,3 0,3 0 0 0,0 0,0 1 3 0,1 1,0 6 3 0,4 0,4 16 10 0,5 0,7 29 9 0,5 0,3 34 14 0,3 0,2 42 105 0,1 0,3 Source: INE, 2010. Annex 6 Resident population with 15 and more years in Mainland Portugal, by work status 2000 Total Work status Active Employment Unemployment Non‐active Mandatory conscription Source: INE, 2010. Pop (x10 3) 2004 % Pop (x10 3) Variation 2000‐08 (%) 2008 % Pop (x10 3) % Pop % 8198 100,0% 8463 100,0% 8595 100,0% 4,9 0,0 5017 4817 200 3169 12 5262 4904 358 3204 5 62,1% 93,2% 6,8% 37,8% 0,1% 5381 4968 413 3216 0 62,6% 92,3% 7,7% 37,4% 0,0% 7,3 3,1 106,7 1,5 ‐100,0 2,3 ‐3,8 92,7 ‐3,2 ‐100,0 61,2% 96,0% 4,0% 38,7% 0,1% Application for the 2010 SCML Award iv Annex Annex 7 Number and percentage of death by work status 2000 2004 2008 Variation 2000‐08 (%) Deaths % Deaths % Deaths % 99025 100,0 96249 100,0 98840 100,0 ‐0,2 0,0 61 17 42 0,1 0,0 0,0 49 14 34 0,1 0,0 0,0 17 6 11 0,0 0,0 0,0 ‐72,1 ‐64,7 ‐73,8 ‐100,0 0,0 0,0 8394 945 8,5 1,0 7466 763 7,8 0,8 7247 273 7,3 0,3 ‐13,7 ‐71,1 ‐13,5 ‐71,1 Looking for new job 15‐64 years 25‐44 years 45‐64 years 138 88 41 0,1 0,1 0,0 117 67 45 0,1 0,1 0,0 283 112 160 0,3 0,1 0,2 105,1 27,3 290,2 105,5 0,0 n. apl. Non‐active 15‐64 years 15‐24 years 25‐64 years 65 and up 11080 594 10486 78407 11,2 0,6 10,6 79,2 10358 407 9951 77496 10,8 0,4 10,3 80,5 6817 220 6597 81324 6,9 0,2 6,7 82,3 ‐38,5 ‐63,0 ‐37,1 3,7 ‐38,4 ‐62,9 ‐37,0 3,9 0 0,0 0 0,0 2879 2,9 n. apl. n. apl. Total Deaths % Work status Looking for 1st job 15‐64 years 15‐24 years 25‐44 years Employed 15‐64 years 65 and up Doesn’t know/ doesn’t answer Source: INE, 2010. Annex 8 Confidence interval for death rate by work status 2000 Total Work status: Active Employed Unemployed Looking for 1st job Looking for new job Non‐active Death rate per 1000 population. Source: INE, 2010 1 2004 1 2008 1 DR (95% CI) DR (95% CI) DR (95% CI) 12,1 11,4 11,5 (12,0;12,2) (11,3;11,4) (11,4;11,6) 1,9 1,6 1,5 (1,9;1,9) (1,6;1,6) (1,4;1,5) 1,9 1,7 1,5 (1,9;2,0) (1,6;1,7) (1,5;1,5) 1,0 0,5 0,7 (0,9;1,1) (0,4;0,5) (0,6;0,8) 2,4 1,0 0,3 (1,8;2,9) (0,7;1,3) (0,2;0,4) 0,8 0,4 0,8 (0,7;0,9) (0,3;0,4) (0,7;0,9) 28,2 27,4 27,4 (28,1;28,4) (27,2;27,6) (27,2;27,6) 1 Application for the 2010 SCML Award v Annex Annex 9 Confidence intervals for death rate by occupational situation and occupation – average employed population 2000 1 2004 2008 DR (95% CI) DR (95% CI) DR (95% CI) 1,9 1,7 1,5 (1,9;2,0) (1,6;1,7) (1,5;1,5) 0,4 0,2 0,2 (0,3;0,4) (0,2;0,3) (0,1;0,2) 2,2 1,8 1,5 (2,1;2,2) (1,7;1,8) (1,4;1,5) 1,9 1,8 1,3 (1,8;2,0) (1,7;1,9) (1,3;1,4) 1,9 1,7 2,7 (1,4;2,4) (1,3;2,1) (2,1;3,3) Managers and Professionals (1 e 2) 2,2 1,4 0,8 (2,1;2,3) (1,3;1,5) (0,7;0,8) Technicians and associate professionals (3) 1,4 0,8 1,0 (1,3;1,5) (0,7;0,9) (0,9;1,1) Clerical support, service and sales workers (4 e 5) 1,5 1,1 0,9 (1,4;1,5) (1,1;1,2) (0,8;0,9) Skilled agricultural, forestry and fishery workers (6) 1,6 1,3 0,5 (1,5;1,7) (1,2;1,4) (0,4;0,6) Craft and related trades workers, operators and assemblers (7 e 8) 2,7 2,5 1,8 (2,6;2,8) (2,4;2,6) (1,8;1,9) Elementary occupations (9) 1,1 2,0 3,0 (1,0;1,2) (1,9;2,1) (2,9;3,2) 1 Per 1000 population. 2 Major groups of National Classification of Occupations (1994): annex 10. Source: INE, 2010 Total Occupational situation: Employer Dependent worker Self‐employed Occupation (Major groups CNP94)1: Armed forces occupations (0) 1 1 Annex 10 Major Groups of National Classification of Occupations (1994) Codes Designation 0 Armed forces occupations 1 Managers 2 Professionals 3 Technicians and associate professionals 4 Clerical support workers 5 Service and sales workers 6 Skilled agricultural, forestry and fishery workers 7 Craft and related trades workers 8 Plant and machine operators, and assemblers 9 Elementary occupations Source: National Classification of Occupations (1994) ‐ CNP94. Application for the 2010 SCML Award vi Annex Annex 11 Number and percentage of death by work status and profession – average employed population 2000 2004 Variation 2000‐08 (%) 2008 Death % Death % Death Total 9339 100,0 8229 100,0 Occupational situation: Employer Dependent worker Self‐employed 111 7565 1614 1,2 81,0 17,3 76 6445 1600 0,9 78,3 19,4 % Death % 7520 100,0 ‐19,5 0,0 48 5576 1179 0,6 74,1 15,7 ‐56,8 ‐26,3 ‐27,0 ‐46,3 ‐8,5 ‐9,3 Occupation (Major groups CNP94)1: Armed forces occupations (0) 61 0,7 60 0,7 82 1,1 34,4 66,9 Managers and Professionals (1 e 2) 1457 15,6 1220 14,8 600 8,0 ‐58,8 ‐48,9 Technicians and associate professionals (3) 519 5,6 313 3,8 479 6,4 ‐7,7 14,6 Clerical support, service and sales workers (4 e 5) 1611 17,3 1303 15,8 1054 14,0 ‐34,6 ‐18,7 Skilled agricultural, forestry and fishery workers (6) 831 8,9 705 8,6 266 3,5 ‐68,0 ‐60,2 Craft and related trades workers, operators and assemblers (7 e 8) 3987 42,7 3377 41,0 2471 32,9 ‐38,0 ‐23,0 Elementary occupations (9) 718 7,7 1185 14,4 1901 25,3 164,8 228,8 1 Major groups of National Classification of Occupations (1994): annex 10. Note: Death sums for modalities presented, for each of the variables ‘Occupational situation’ and ‘Occupation’, is inferior to total deaths due to existence of cases where occupational situation and occupation of the deceased are unknown. Source: INE, 2010. Annex 12 Number and percentage of deaths by basis for indication of cause of death Total Basis for indication: Medical elements Histological examination Autopsy Written documents made by the administrative authorities Other official documents Unknown Source: INE, 2010. 2000 Death % 99025 100,0 2004 Death % 96249 100,0 2008 Death % 98840 100,0 Variation 2000‐08 (%) Death % ‐0,2 0,0 90353 2313 5803 91,2 2,3 5,9 89159 0 6229 92,6 0,0 6,5 89327 0 6075 90,4 0,0 6,1 ‐1,1 n. apl. 4,7 ‐1,0 n. apl. 4,9 289 267 0 0,3 0,3 0,0 338 523 0 0,4 0,5 0,0 736 999 1703 0,7 1,0 1,7 154,7 274,2 n. apl. 155,1 274,9 n. apl. Application for the 2010 SCML Award vii Annex Annex 13 Number and percentage of autopsies by place of death Total 2000 2004 Death % Death % 5803 100,0 6229 100,0 Place of death: Hospital/clinic 2528 43,6 2355 At home 1014 17,5 ND At public places 2261 39,0 ND NA – Data not available due statistical confidentiality. Source: INE, 2010. 2008 Death % 6075 100,0 37,8 ND ND 2227 1821 2027 Variation 2000‐08 (%) Death % 4,7 0,0 36,7 30,0 33,4 ‐11,9 79,6 ‐10,3 ‐15,9 71,5 ‐14,4 Annex 14 Number and percentage of deaths in 2008 by local of death, age group and gender Hospital/clinic Total Death At home % Death At public places % Death % Total 98840 60692 61,4 29518 29,9 8630 8,7 Gender: H M 50798 48042 32521 28171 64,0 58,6 13702 15816 27,0 32,9 4575 4055 9,0 8,4 15 ‐ 24 years H M 476 343 133 233 159 74 48,9 46,4 55,6 63 42 21 13,2 12,2 15,8 180 142 38 37,8 41,4 28,6 25 ‐ 44 years H M 3420 2427 993 2030 1342 688 59,4 55,3 69,3 715 513 202 20,9 21,1 20,3 675 572 103 19,7 23,6 10,4 45 ‐ 64 years H M 13164 9048 4116 9238 6187 3051 70,2 68,4 74,1 2717 1901 816 20,6 21,0 19,8 1209 960 249 9,2 10,6 6,0 65 ‐ 74 years H M 16520 10280 6240 11457 7119 4338 69,4 69,3 69,5 3933 2423 1510 23,8 23,6 24,2 1130 738 392 6,8 7,2 6,3 75 ‐ 84 years H M 34366 17676 16690 21508 11413 10095 62,6 64,6 60,5 10280 5034 5246 29,9 28,5 31,4 2578 1229 1349 7,5 7,0 8,1 85 and up H M Source: INE, 2010. 30894 11024 19870 16226 6301 9925 52,5 57,2 49,9 11810 3789 8021 38,2 34,4 40,4 2858 934 1924 9,3 8,5 9,7 Age group: Application for the 2010 SCML Award viii Annex Annex 15 Results of Chi‐square independence test and association measures Place of death 1 Pearson Chi‐Square 1 Value 2 3 Gender: M 64,0 27,0 9,0 417,9892 F 58,6 32,9 8,4 Age group: 15 ‐ 24 48,9 13,2 37,8 3267,0132 25 ‐ 44 59,4 20,9 19,7 45 ‐ 64 70,2 20,6 9,2 65 ‐ 74 69,4 23,8 6,8 75 ‐ 84 62,6 29,9 7,5 85 and up 52,5 38,2 9,3 Place of residence: Norte 58,5 35,8 5,8 1267,1182 Centro 61,3 29,6 9,2 LVT 64,2 25,6 10,2 Alentejo 58,7 28,3 13,0 Algarve 65,0 26,1 8,9 Marital status: 56,2 31,5 12,3 1352,1112 Single 67,1 25,8 7,1 Married 56,2 34,5 9,3 Divorced 63,3 26,1 10,6 Widow 58,0 30,2 11,7 Unknown Work status: 64,6 19,3 16,1 993,3562 Active 60,9 31,1 8,0 Non‐active 69,8 20,2 10,0 Doesn’t know/Doesn’t answer Occupation (Major groups CNP94)2: 65,3 19,0 15,7 751,2762 Qualified workers (0 a 8) 61,7 20,8 17,5 Non qualified workers (9) 61,2 30,6 8,2 CNP Unknown Nationality: 61,4 29,9 8,7 34,0522 Portuguese 59,9 27,0 13,0 Foreign Note 1: Modalities for the variable Place of death: 1 – Hospital/Clinic 2 – At home 3 ‐ Elsewhere Note 2: 0 cells (,0%) have expected count less than 5. Application for the 2010 SCML Award Phi Cramer's V Contingency Coeff. df Asymp. Value Approx. Value Approx. Value Approx. Sig. (2‐ Sig. Sig. Sig. sided) 2 ,000 ,065 ,000 ,065 ,000 ,065 ,000 10 ,000 ,182 ,000 ,129 ,000 ,179 ,000 8 ,000 ,113 ,000 ,080 ,000 ,112 ,000 ,083 ,000 ,116 ,000 8 ,000 ,117 ,000 4 ,000 ,100 ,000 ,071 ,000 ,100 ,000 ,062 ,000 ,087 ,000 ,019 ,000 ,019 ,000 4 ,000 ,087 ,000 2 ,000 ,019 ,000 ix Annex Annex 16 Results of Chi‐square independence test and association measures Place of death 1 1 2 3 Pearson Chi‐Square Value Cause of death: Infectious and parasitic 91,9 6,0 2,0 17562,5872 diseases 74,8 22,2 3,0 Malignant neoplasms Colon, rectum and 74,9 22,3 2,8 anus 72,1 22,6 5,3 Female breast 83,3 12,9 3,9 Cervix uteri 61,9 31,2 7,0 Diabetes mellitus 53,7 35,8 10,4 Alcohol abuse Ischemic heart 51,7 39,2 9,1 diseases 51,3 40,5 8,3 Stroke Diseases of the 76,8 18,9 4,3 respiratory system Diseases of the 88,6 9,5 1,8 digestive system Diseases of the 81,3 16,7 2,0 musculoskeletal system/connective tissue Diseases of the 83,4 13,3 3,3 genitourinary system Symptoms, signs, 25,5 51,8 22,7 abnormal findings, ill‐ defined causes External causes of 46,2 19,5 34,4 injury and poisoning Note 1: Modalities for the variable Place of death: 1 – Hospital/Clinic 2 – At home 3 ‐ Elsewhere Note 2: 0 cells (,0%) have expected count less than 5. Phi Cramer's V df Asymp. Sig. (2‐ sided) Value App. Sig. 28 ,000 ,444 ,000 Value App. Sig. Contingency Coeff. Value App. Sig. ,314 ,000 ,406 Application for the 2010 SCML Award x ,000 Annex Annex 17 Number of hospitalizations, hospitalization deaths and intra‐hospital lethality rate, by place of residence (NUT III) 2000 Variation 2000‐2008 (%) Let. Let. Let. Hosp. Death Hosp. Death Hosp. Death (%) (%) (%) 762038 41365 5,4 862204 46450 5,4 32,6 24,8 ‐5,3 2004 2008 Hosp. Death. 650444 37224 Let. (%) 5,7 10421 643 6,2 12098 676 5,6 13592 848 6,2 30,4 31,9 1,1 5909 392 6,6 5265 403 7,7 8968 563 6,3 51,8 43,6 ‐5,4 Algarve 21649 1535 7,1 27953 1746 6,2 33549 2417 7,2 55,0 57,5 1,6 Alto Alentejo Alto Trás‐os‐ Montes Ave 9025 640 7,1 10200 727 7,1 10593 828 7,8 17,4 29,4 10,2 20273 945 4,7 22393 1163 5,2 23930 1206 5,0 18,0 27,6 8,1 26436 1304 4,9 31773 1430 4,5 36629 1719 4,7 38,6 31,8 ‐4,9 Baixo Alentejo 9013 660 7,3 8992 627 7,0 10956 626 5,7 21,6 ‐5,2 ‐22,0 Baixo Mondego 28733 1519 5,3 34729 1670 4,8 37596 1758 4,7 30,8 15,7 ‐11,5 Baixo Vouga Beira Interior Norte Beira Interior Sul Cávado 27013 1342 5,0 32006 1521 4,8 36874 1789 4,9 36,5 33,3 ‐2,3 8655 539 6,2 10271 537 5,2 10269 584 5,7 18,6 8,3 ‐8,7 8097 427 5,3 8232 446 5,4 7606 512 6,7 ‐6,1 19,9 27,6 17381 980 5,6 20840 1118 5,4 23652 1222 5,2 36,1 24,7 ‐8,4 Cova da Beira 10789 545 5,1 11737 510 4,3 12661 623 4,9 17,4 14,3 ‐2,6 Dão‐Lafões 19796 1141 5,8 24354 1328 5,5 27531 1467 5,3 39,1 28,6 ‐7,6 Douro Entre Douro e Vouga Grande Lisboa 15360 760 4,9 17823 938 5,3 21085 1151 5,5 37,3 51,4 10,3 15515 694 4,5 19465 640 3,3 21695 746 3,4 39,8 7,5 ‐23,1 137724 8641 6,3 150041 9323 6,2 159763 9477 5,9 16,0 9,7 ‐5,5 Grande Porto 64466 3529 5,5 85919 3931 4,6 108983 4665 4,3 69,1 32,2 ‐21,8 Lezíria do Tejo 17839 1175 6,6 20896 1408 6,7 23465 1643 7,0 31,5 39,8 6,3 Médio Tejo 13995 987 7,1 18352 1063 5,8 20796 1183 5,7 48,6 19,9 ‐19,3 Minho‐Lima 13864 770 5,6 16237 867 5,3 22228 1036 4,7 60,3 34,5 ‐16,1 Oeste Península de Setúbal Pinhal Interior Norte Pinhal Interior Sul Pinhal Litoral 21675 1331 6,1 25392 1590 6,3 30311 1781 5,9 39,8 33,8 ‐4,3 41896 2649 6,3 48697 3029 6,2 54220 3626 6,7 29,4 36,9 5,8 9280 497 5,4 12135 696 5,7 13112 767 5,8 41,3 54,3 9,2 3416 246 7,2 3993 266 6,7 4185 308 7,4 22,5 25,2 2,2 18340 920 5,0 23116 1075 4,7 27242 1217 4,5 48,5 32,3 ‐10,9 Total NUT II – place of residence: Alentejo Central Alentejo Litoral Serra da Estrela 4608 245 5,3 5610 267 4,8 5207 313 6,0 13,0 27,8 13,1 Tâmega 24298 1084 4,5 32085 1285 4,0 39205 1654 4,2 61,4 52,6 ‐5,4 Unknown 24978 1084 4,3 21434 1085 5,1 16301 721 4,4 ‐34,7 ‐33,5 1,9 Application for the 2010 SCML Award xi Annex Annex 18 Number of hospitalizations, hospitalization deaths and intra‐hospital lethality rate due to Ischemic heart disease, by place of residence (NUT III) 2000 Total NUT II – place of residence: Alentejo Central Alentejo Litoral Algarve Alto Alentejo Alto Trás‐os‐ Montes Ave Baixo Alentejo Baixo Mondego Baixo Vouga Beira Interior Norte Beira Interior Sul Cávado Cova da Beira Dão‐Lafões Douro Entre Douro e Vouga Grande Lisboa Grande Porto Lezíria do Tejo Médio Tejo Minho‐Lima Oeste Península de Setúbal Pinhal Interior Norte Pinhal Interior Sul Pinhal Litoral Serra da Estrela Tâmega Unknown 2004 Hosp. Death 1753 Let. (%) 6,0 30096 668 45 338 1093 455 2008 Variation 2000‐2008 (%) Let. Hosp. Death (%) ‐4,3 ‐6,3 ‐2,1 Hosp. Death 2012 Let. (%) 6,7 28036 1642 Let. (%) 5,9 6,7 676 45 6,7 655 42 6,4 ‐1,9 ‐6,7 ‐4,8 14 76 24 4,1 7,0 5,3 249 1249 446 17 82 31 6,8 6,6 7,0 535 1429 472 23 83 33 4,3 5,8 7,0 58,3 30,7 3,7 64,3 9,2 37,5 3,8 ‐16,5 32,5 600 32 5,3 656 40 6,1 655 24 3,7 9,2 ‐25,0 ‐31,3 1080 496 744 805 50 20 49 33 4,6 4,0 6,6 4,1 885 545 1033 847 56 32 54 42 6,3 5,9 5,2 5,0 924 494 1006 846 42 18 49 50 4,5 3,6 4,9 5,9 ‐14,4 ‐0,4 35,2 5,1 ‐16,0 ‐10,0 0,0 51,5 ‐1,8 ‐9,6 ‐26,0 44,2 316 29 9,2 415 18 4,3 309 20 6,5 ‐2,2 ‐31,0 ‐29,5 253 20 7,9 408 28 6,9 269 27 10,0 6,3 35,0 27,0 606 444 553 425 22 13 31 29 3,6 2,9 5,6 6,8 564 518 661 417 39 24 47 35 6,9 4,6 7,1 8,4 521 577 709 528 19 22 36 24 3,6 3,8 5,1 4,5 ‐14,0 30,0 28,2 24,2 ‐13,6 69,2 16,1 ‐17,2 0,5 30,2 ‐9,4 ‐33,4 412 28 6,8 476 30 6,3 379 24 6,3 ‐8,0 ‐14,3 ‐6,8 8876 3093 789 417 589 1041 616 191 30 32 23 66 6,9 6,2 3,8 7,7 3,9 6,3 8434 3253 894 653 675 1052 670 204 57 37 45 92 7,9 6,3 6,4 5,7 6,7 8,7 6549 3097 1089 760 548 1049 475 196 46 38 31 59 7,3 6,3 4,2 5,0 5,7 5,6 ‐26,2 0,1 38,0 82,3 ‐7,0 0,8 ‐22,9 2,6 53,3 18,8 34,8 ‐10,6 4,5 2,5 11,1 ‐34,8 44,9 ‐11,3 2654 136 5,1 2664 162 6,1 2248 136 6,0 ‐15,3 0,0 18,1 203 16 7,9 335 20 6,0 366 23 6,3 80,3 43,8 ‐20,3 102 12 11,8 109 9 8,3 124 9 7,3 21,6 ‐25,0 ‐38,3 646 98 877 33 7 44 5,1 7,1 5,0 523 168 932 20 10 50 3,8 6,0 5,4 462 108 920 21 8 46 4,5 7,4 5,0 ‐28,5 10,2 4,9 ‐36,4 14,3 4,5 ‐11,0 3,7 ‐0,3 636 32 5,0 408 18 4,4 408 18 4,4 ‐35,8 ‐43,8 ‐12,3 Hosp. Death. 29309 Application for the 2010 SCML Award xii Annex Annex 19 Number of hospitalizations, hospitalization deaths and intra‐hospital lethality rate due to stroke, by place of residence (NUT III) 4204 Let. (%) 15,0 Variation 2000‐2008 (%) Let. Hosp. Death (%) 15,4 3,9 ‐10,0 585 257 434 323 86 37 81 70 14,7 14,4 18,7 21,7 ‐5,3 ‐25,3 ‐57,8 ‐23,3 19,4 ‐26,0 ‐55,7 ‐20,5 26,2 ‐0,9 4,8 3,7 19,1 734 121 16,5 ‐5,2 ‐6,9 ‐1,9 154 104 173 134 10,8 18,0 17,1 11,9 1399 442 931 1124 177 78 196 197 12,7 17,6 21,1 17,5 6,2 ‐2,2 ‐7,9 3,7 ‐6,3 16,4 10,7 22,4 ‐11,8 19,1 20,2 18,0 457 112 24,5 410 105 25,6 15,5 19,3 3,3 20,2 15,8 9,6 14,9 14,7 330 835 397 1032 713 57 142 45 169 124 17,3 17,0 11,3 16,4 17,4 283 738 225 1101 687 68 111 32 196 115 24,0 15,0 14,2 17,8 16,7 ‐1,4 ‐8,0 ‐34,2 ‐1,9 ‐7,0 17,2 ‐12,6 ‐3,0 17,4 5,5 18,9 ‐5,0 47,4 19,6 13,5 77 14,9 460 64 13,9 529 88 16,6 2,5 14,3 11,5 5667 2772 787 731 914 994 768 383 149 99 105 136 13,6 13,8 18,9 13,5 11,5 13,7 3619 2420 856 735 812 1001 592 359 177 104 105 134 16,4 14,8 20,7 14,1 12,9 13,4 3643 2304 962 640 879 1112 607 379 146 117 129 134 16,7 16,4 15,2 18,3 14,7 12,1 ‐35,7 ‐16,9 22,2 ‐12,4 ‐3,8 11,9 ‐21,0 22,9 ‐1,0 19,1 ‐2,0 ‐19,8 18,2 35,0 22,9 27,7 ‐1,5 ‐11,9 1863 321 17,2 1783 280 15,7 1512 254 16,8 ‐18,8 ‐20,9 ‐2,5 417 58 13,9 447 71 15,9 362 58 16,0 ‐13,2 0,0 15,2 195 736 171 1381 45 123 34 168 23,1 16,7 19,9 12,2 189 738 175 1466 37 97 18 196 19,6 13,1 10,3 13,4 174 771 171 1413 50 134 34 211 28,7 17,4 19,9 14,9 ‐10,8 4,8 0,0 2,3 11,1 8,9 0,0 25,6 24,5 4,0 0,0 22,8 195 37 19,0 153 25 16,3 249 39 15,7 27,7 5,4 ‐17,5 2000 Total NUT II – place of residence: Alentejo Central Alentejo Litoral Algarve Alto Alentejo Alto Trás‐os‐ Montes Ave Baixo Alentejo Baixo Mondego Baixo Vouga Beira Interior Norte Beira Interior Sul Cávado Cova da Beira Dão‐Lafões Douro Entre Douro e Vouga Grande Lisboa Grande Porto Lezíria do Tejo Médio Tejo Minho‐Lima Oeste Península de Setúbal Pinhal Interior Norte Pinhal Interior Sul Pinhal Litoral Serra da Estrela Tâmega Unknown 2004 Hosp. Death 4048 Let. (%) 16,6 25221 618 344 1028 421 72 50 183 88 11,7 14,5 17,8 20,9 774 130 1317 452 1011 1084 2008 Hosp. Death 3909 Let. (%) 15,5 28089 566 283 461 353 69 49 95 72 12,2 17,3 20,6 20,4 16,8 792 151 189 67 177 161 14,4 14,8 17,5 14,9 1430 578 1011 1129 355 88 24,8 287 802 342 1122 739 58 127 33 167 109 516 Hosp. Death. 24340 Application for the 2010 SCML Award xiii Annex Annex 20 Number of hospitalizations, hospitalization deaths and intra‐hospital lethality rate due to female breast cancer, by place of residence (NUT III) 2000 2004 5353 464 8,7 1131 64 Let. (%) 5,7 NUT II – place of residence: Alentejo Central Alentejo Litoral Algarve Alto Alentejo Alto Trás‐os‐ Montes Ave Baixo Alentejo Baixo Mondego Baixo Vouga Beira Interior Norte Beira Interior Sul Cávado Cova da Beira Dão‐Lafões Douro Entre Douro e Vouga Grande Lisboa Grande Porto Lezíria do Tejo Médio Tejo Minho‐Lima Oeste Península de Setúbal Pinhal Interior Norte Pinhal Interior Sul Pinhal Litoral Serra da Estrela Tâmega 107 9 8,4 126 48 192 69 9 17 8 18,8 8,9 11,6 79 7 142 77 261 187 Unknown Variation 2000‐2008 (%) 7112 373 Let. (%) 5,2 7 5,6 127 10 7,9 18,7 11,1 ‐6,4 41 241 90 3 11 11 7,3 4,6 12,2 69 314 100 2 16 9 2,9 5,1 9,0 43,8 63,5 44,9 ‐77,8 ‐5,9 12,5 ‐84,5 ‐42,5 ‐22,4 8,9 74 6 8,1 115 7 6,1 45,6 0,0 ‐31,3 9 10 18 9 6,3 13,0 6,9 4,8 180 102 319 269 8 2 22 12 4,4 2,0 6,9 4,5 277 80 288 212 17 7 16 10 6,1 8,8 5,6 4,7 95,1 3,9 10,3 13,4 88,9 ‐30,0 ‐11,1 11,1 ‐3,2 ‐32,6 ‐19,4 ‐2,0 50 4 8,0 60 5 8,3 57 5 8,8 14,0 25,0 9,6 63 4 6,3 51 6 11,8 38 4 10,5 ‐39,7 0,0 65,8 153 65 134 67 12 10 9 8 7,8 15,4 6,7 11,9 150 74 183 65 6 8 17 4 4,0 10,8 9,3 6,2 215 66 172 105 6 10 7 4 2,8 15,2 4,1 3,8 40,5 1,5 28,4 56,7 ‐50,0 0,0 ‐22,2 ‐50,0 ‐64,4 ‐1,5 ‐39,4 ‐68,1 49 4 8,2 70 3 4,3 164 3 1,8 234,7 ‐25,0 ‐77,6 1184 358 145 153 98 194 138 12 13 16 8 16 11,7 3,4 9,0 10,5 8,2 8,2 1275 448 180 147 101 203 111 18 12 11 5 17 8,7 4,0 6,7 7,5 5,0 8,4 1512 808 214 173 164 264 89 26 13 12 3 18 5,9 3,2 6,1 6,9 1,8 6,8 27,7 125,7 47,6 13,1 67,3 36,1 ‐35,5 116,7 0,0 ‐25,0 ‐62,5 12,5 ‐49,5 ‐4,0 ‐32,2 ‐33,7 ‐77,6 ‐17,3 404 35 8,7 437 26 5,9 490 30 6,1 21,3 ‐14,3 ‐29,3 90 6 6,7 103 8 7,8 101 6 5,9 12,2 0,0 ‐10,9 24 1 4,2 21 6 28,6 27 1 3,7 12,5 0,0 ‐11,1 153 19 89 8 0 4 5,2 0,0 4,5 172 41 72 15 1 2 8,7 2,4 2,8 138 45 233 6 4 7 4,3 8,9 3,0 ‐9,8 136,8 161,8 ‐25,0 ‐ 75,0 ‐16,8 ‐ ‐33,2 699 60 8,6 6426 427 6,6 544 25 4,6 ‐22,2 ‐58,3 ‐46,5 Hosp. Death. Let. (%) Hosp. Death Total 2008 Hosp. Death Hosp. Death Let. (%) 32,9 ‐19,6 ‐39,5 Application for the 2010 SCML Award xiv Annex Annex 21 Number of hospitalizations, hospitalization deaths and intra‐hospital lethality rate due to colo‐rectal cancer, by place of residence (NUT III) 2000 7811 1004 Let. (%) 12,9 NUT II – place of residence: Alentejo Central Alentejo Litoral Algarve Alto Alentejo Alto Trás‐os‐ Montes Ave Baixo Alentejo Baixo Mondego Baixo Vouga Beira Interior Norte Beira Interior Sul Cávado Cova da Beira Dão‐Lafões Douro Entre Douro e Vouga Grande Lisboa Grande Porto Lezíria do Tejo Médio Tejo Minho‐Lima Oeste Península de Setúbal Pinhal Interior Norte Pinhal Interior Sul Pinhal Litoral Serra da Estrela Tâmega 151 Unknown 2008 8741 1181 Let. (%) 13,5 20 13,2 199 101 270 157 11 34 27 10,9 12,6 17,2 164 15 309 152 337 325 Variation 2000‐2008 (%) Let. Hosp. Death (%) 17,0 36,8 16,9 9137 1373 Let. (%) 15,0 37 18,6 163 35 21,5 7,9 75,0 62,1 111 336 128 9 42 23 8,1 12,5 18,0 93 368 142 13 56 25 14,0 15,2 17,6 ‐7,9 36,3 ‐9,6 18,2 64,7 ‐7,4 28,3 20,8 2,4 9,1 247 35 14,2 309 43 13,9 88,4 186,7 52,1 44 26 44 45 14,2 17,1 13,1 13,8 286 145 337 346 31 24 48 46 10,8 16,6 14,2 13,3 372 136 373 328 35 25 59 44 9,4 18,4 15,8 13,4 20,4 ‐10,5 10,7 0,9 ‐20,5 ‐33,9 ‐3,8 7,5 34,1 21,1 ‐2,2 ‐3,1 116 17 14,7 132 11 8,3 154 25 16,2 32,8 47,1 10,8 160 19 11,9 137 20 14,6 106 13 12,3 ‐33,8 ‐31,6 3,3 206 178 235 161 34 27 21 10 16,5 15,2 8,9 6,2 162 175 281 171 18 24 37 17 11,1 13,7 13,2 9,9 238 178 268 175 24 30 39 19 10,1 16,9 14,6 10,9 15,5 0,0 14,0 8,7 ‐29,4 ‐38,9 11,1 11,1 85,7 62,8 90,0 74,8 96 11 11,5 123 13 10,6 178 27 15,2 85,4 145,5 32,4 1611 612 242 195 138 267 253 49 38 27 16 30 15,7 8,0 15,7 13,8 11,6 11,2 1760 773 235 232 137 330 276 89 41 40 17 55 15,7 11,5 17,4 17,2 12,4 16,7 1879 931 286 242 191 348 301 104 67 46 31 61 16,0 11,2 23,4 19,0 16,2 17,5 16,6 52,1 18,2 24,1 38,4 30,3 19,0 112,2 76,3 70,4 93,8 103,3 2,0 39,5 49,2 37,3 40,0 56,0 546 73 13,4 619 86 13,9 650 95 14,6 19,0 30,1 9,3 102 13 12,7 173 19 11,0 137 23 16,8 34,3 76,9 31,7 58 4 6,9 59 10 16,9 42 8 19,0 ‐27,6 100,0 176,2 243 62 148 23 4 15 9,5 6,5 10,1 287 64 199 26 6 17 9,1 9,4 8,5 252 61 297 37 9 41 14,7 14,8 13,8 3,7 60,9 55,1 ‐1,6 125,0 128,7 100,7 173,3 36,2 469 54 11,5 557 64 11,5 240 38 15,8 ‐48,8 Hosp. Death. Total 2004 Hosp. Death Hosp. Death ‐29,6 Application for the 2010 SCML Award xv 37,5 Annex Annex 22 Number of hospitalizations, hospitalization deaths and intra‐hospital lethality rate due to Tracheal, Bronchus and Lung, by place of residence (NUT III) 2000 2004 Hosp. Death. Total 4483 1153 Let. (%) 25,7 78 NUT II – place of residence: Alentejo Central Alentejo Litoral Algarve Alto Alentejo Alto Trás‐os‐ Montes Ave Baixo Alentejo Baixo Mondego Baixo Vouga Beira Interior Norte Beira Interior Sul Cávado Cova da Beira Dão‐Lafões Douro Entre Douro e Vouga Grande Lisboa Grande Porto Lezíria do Tejo Médio Tejo Minho‐Lima Oeste Península de Setúbal Pinhal Interior Norte Pinhal Interior Sul Pinhal Litoral Serra da Estrela Tâmega Unknown 2008 4639 1414 Let. (%) 30,5 18 23,1 89 39 179 66 9 58 19 23,1 32,4 28,8 86 20 222 60 139 121 Variation 2000‐2008 (%) Let. Hosp. Death (%) 17 36,8 16,9 4964 1618 Let. (%) 32,6 31 34,8 76 39 51,3 7,9 75 62,1 47 191 86 14 59 28 29,8 30,9 32,6 38 211 46 12 81 18 31,6 38,4 39,1 ‐7,9 36,3 ‐9,6 18,2 64,7 ‐7,4 28,3 20,8 2,4 23,3 89 15 16,9 82 16 19,5 88,4 186,7 52,1 41 22 31 30 18,5 36,7 22,3 24,8 189 68 157 163 40 24 41 33 21,2 35,3 26,1 20,2 257 67 211 145 66 30 49 40 25,7 44,8 23,2 27,6 20,4 ‐10,5 10,7 0,9 ‐20,5 ‐3,8 34,1 ‐2,2 ‐33,9 7,5 21,1 ‐3,1 60 11 18,3 87 17 19,5 54 10 18,5 32,8 47,1 10,8 56 9 16,1 54 7 13,0 28 6 21,4 ‐33,8 ‐31,6 3,3 175 63 152 105 50 13 26 14 28,6 20,6 17,1 13,3 165 115 129 83 51 20 37 15 30,9 17,4 28,7 18,1 131 112 165 87 46 20 47 23 35,1 17,9 28,5 26,4 15,5 0 14 8,7 ‐29,4 11,1 85,7 90 ‐38,9 11,1 62,8 74,8 62 22 35,5 48 14 29,2 76 30 39,5 85,4 145,5 32,4 1013 562 132 82 101 102 326 137 28 18 23 16 32,2 24,4 21,2 22,0 22,8 15,7 1007 585 116 63 63 123 379 167 32 20 15 39 37,6 28,5 27,6 31,7 23,8 31,7 1161 655 112 91 86 181 404 225 35 27 21 54 34,8 34,4 31,3 29,7 24,4 29,8 16,6 52,1 18,2 24,1 38,4 30,3 19 112,2 76,3 70,4 93,8 103,3 2 39,5 49,2 37,3 40 56 299 78 26,1 342 137 40,1 361 161 44,6 19 30,1 9,3 68 16 23,5 50 11 22,0 82 24 29,3 34,3 76,9 31,7 20 3 15,0 12 4 33,3 15 3 20,0 ‐27,6 100 176,2 45 26 148 17 1 32 37,8 3,8 21,6 77 29 127 22 6 28 28,6 20,7 22,0 90 27 168 27 3 47 30,0 11,1 28,0 3,7 ‐1,6 100,7 60,9 55,1 125 128,7 173,3 36,2 222 65 29,3 285 108 37,9 149 54 36,2 ‐48,8 ‐29,6 Hosp. Death Hosp. Death Application for the 2010 SCML Award xvi 37,5 Annex Annex 23 Service Strategy for TIP Medicine Surgery Services Intensive care Not identified Services N % N % N % 4 10,5 9 23 N % Total 14 36,8 11 28,9 Never/Rarely 12 86 9 81,8 3 75,0 6 66,6 Sometimes/ Frequently 2 14 1 9,10 1 25,0 2 22,2 Doesn’t know / not applic. ‐ ‐ 1 9,10 ‐ ‐ 1 11,1 Never/Rarely 10 90,9 7 77,8 2 50,0 6 66,7 Sometimes/ Frequently 1 9,1 2 22,2 1 25,0 ‐ ‐ Doesn’t know / not applic. ‐ ‐ ‐ ‐ 1 25,0 3 33,3 There is a reserved room for No 11 78,6 4 36,4 2 50,0 5 55,6 Yes 3 21,4 7 63,6 2 50,0 2 22,2 Doesn’t know / not applic. ‐ ‐ ‐ ‐ ‐ ‐ 2 36,8 Guidelines for accompanying No 2 14,3 3 30,0 ‐ ‐ 5 55,6 Yes 12 85,7 7 70,0 4 100 3 33,3 Doesn’t know / not applic. ‐ ‐ ‐ ‐ ‐ ‐ 1 100 The service never transfers TIP Transfer for another hospital TIP TIP There is a written protocol for n=12 Transfer to room / space n=7 n=4 n=3 1 8,3 ‐ ‐ 1 25 1 33,3 Pain control 1 8,3 1 14,3 3 75 ‐ ‐ Possibility of family presence 3 25 2 28,6 3 75 2 66,6 Psychological Support 2 16,7 2 28,6 2 50 1 33,3 Spiritual and religious care 4 33,3 3 42,9 3 75 2 66,6 Language support 3 25 2 28,6 3 75 1 33,3 Medical discharge if the 2 16,7 1 14,3 ‐ ‐ 1 33,3 isolated patient wishes The service has medical providers with specific training in this area No 8 57,1 10 90,9 3 75,0 6 62,5 Yes 4 28,6 ‐ ‐ 1 25,0 ‐ ‐ Doesn’t know / not applic. 2 14,3 1 9,1 ‐ ‐ 3 37,5 3 33,3 When they are integrated into service medical providers receive specific training No 6 42,9 Application for the 2010 SCML Award 4 36,4 2 50,0 xvii Annex Yes 3 21,4 ‐ ‐ 1 25,0 1 11,1 Doesn’t know / not applic. / 5 35,7 7 63,3 1 25,0 5 55,6 unanswered The service has nurses with specific training in this area No 7 50,0 7 60,0 2 50,0 4 44,4 Yes 4 28,6 2 20,0 2 50,0 4 44,4 Doesn’t know / not applic. / 3 21,4 2 20,0 ‐ ‐ 1 11,4 unanswered When they are integrated into service nurses receive specific training No 7 50,0 6 54,6 ‐ ‐ 2 22,2 Yes 4 28,6 1 9,1 4 100 3 33,3 Doesn’t know / not applic. / 3 21,4 1 9,1 ‐ ‐ 4 44,5 unanswered The service has available for TIP the support from the others professionals No ‐ ‐ 1 9,1 ‐ ‐ 1 12,5 Yes 14 100 1 90,9 4 100 5 50,0 Doesn’t know / not applic. / ‐ ‐ ‐ ‐ ‐ ‐ 3 37,5 unanswered The TIP usually participates in the decision on the following alternatives Medical treatment 6 42,9 5 45,5 2 50 2 22,2 Strategies for pain control 6 42,9 9 81,8 2 50 2 22,2 Chance to go home 8 57,1 11 100 3 75 4 44,4 Doesn’t know / not applic. 6 42,9 ‐ ‐ 1 25 2 22,2 The service provides domiciliary care scheme No 12 85,7 9 81,8 4 100 8 88,9 Yes 1 7,1 2 18,2 ‐ ‐ ‐ ‐ Doesn’t know / not applic. / 1 7,1 ‐ ‐ ‐ ‐ 1 11.1 unanswered The TIP to which the Service provides care at domiciliary scheme is reported to the assistants’ practitioners/Family practitioners No 2 14,3 1 9,1 1 25 1 11,1 Yes 3 21,4 2 18,2 ‐ ‐ 1 11,1 Doesn’t know / not applic. / 9 64,3 2 18,2 3 75,0 7 77,8 unanswered Application for the 2010 SCML Award xviii Annex Annex 24 Parte3. Strategy to support families Medicine Surgery Services Intensive care Not identified Services N % N % N % 36,8 11 10,5 9 23 N % Total 14 28,9 4 The family can to follow the Tip 24 hour per day 9 64,3 7 63,6 2 50 5 55,6 Only during the day 4 28,6 3 27,3 2 50,0 2 22,2 Only in visit hour ‐ ‐ ‐ ‐ ‐ ‐ ‐ Doesn’t know / not 1 7,1 1 9,1 ‐ ‐ 2 22,2 ‐ applic. / unanswered The family is frequently informed about the cares to provide Sometimes 2 14,3 1 9,1 1 25,0 3 37,5 Frequently 12 85,7 10 90,9 3 75,0 6 62,5 Unanswered ‐ ‐ ‐ ‐ ‐ ‐ ‐ ‐ Guidelines for communicating with family in case of imminent death No 3 21,4 3 27,3 ‐ ‐ 1 11,1 Yes 10 71,4 6 54,5 4 100 5 55,6 Doesn’t know / not 1 7,1 2 18,2 ‐ ‐ 2 22,2 applic. / unanswered The service has guidelines about communicating with family, when patient´s family wasn´t present at death moment No ‐ ‐ 2 18,2 ‐ ‐ 1 11,1 Yes 11 78,6 6 54,5 4 100 5 55,6 Doesn’t know / not 3 21,4 3 27,3 ‐ ‐ 3 33,3 applic. / unanswered When the family isn´t present at death moment, usually the news is given by Personally 10 71,4 5 45,4 4 100 5 55,6 By phone 11 78,6 9 81,8 2 50 5 55,6 Doesn’t know / ‐ ‐ ‐ ‐ ‐ ‐ 1 11,1 unanswered Usually the news is given by A doctors 10 71,4 9 81,8 4 100 6 62,5 A nurse 10 71,4 8 72,8 3 75 4 44,4 Doesn’t know / ‐ ‐ ‐ ‐ ‐ ‐ 1 11,1 unanswered The news of death is frequently reported to Assistant Practitioners/ Family practitioners Never/Rarelly 8 57,1 6 Application for the 2010 SCML Award 54,6 1 25,0 3 33,3 xix Annex Sometimes/ Frequently 5 35,7 4 36,4 2 50,0 5 55,6 Doesn’t know / not 1 7,1 1 91, 1 25,0 1 11,1 applic. Annex 25 Characterization of sample Doctors Nurses N Total 41 100,0 176 100,0 Health Region Norte 9 22,0 56 31,8 Centro 4 LVT 23 56,1 89 50,6 Alentejo 2 4,9 8 4,5 Algarve 1 2,4 2 1,1 Unanswered 2 4,9 4 2,3 Gender M 20 48,8 31 17,6 F 21 51,2 145 82,4 Age groups % 9,8 0,0 N 17 % 9,7 7 4,0 < 25 years 0 25 a 34 years 6 14,6 95 54,0 35 a 44 years 5 12,2 36 20,5 45 a 54 years 12 29,3 34 19,3 55 a 64 years 17 41,5 2 1,1 Unanswered 2 1,1 1 2,4 Application for the 2010 SCML Award xx Annex Annex 26 Characterization of health professionals by professional specialty Total Speciality 1: Doctors N % 41 18,9 Gastroenterology 16 39,0 Internal Medicine 12 29,3 General Surgery 3 7,3 Pediatrics 2 4,9 Infectious disease Internal Medicine ‐ Oncology 1 2,4 1 2,4 Internal Medicine (IC) 1 2,4 Trauma and orthopedic 1 2,4 1 2,4 1 1 1 2,4 2,4 2,4 ‐‐‐‐‐ ‐‐‐ ‐‐‐ ‐‐‐ Speciality 2: ‐‐‐ ‐‐‐ Cardiology 1 2,4 Intensive medicine 1 2,4 Nefrology 1 2,4 Oncology Medicine Oncology 1 1 2,4 2,4 Unanswered 36 87,8 ‐‐‐‐ ‐‐‐ ‐‐ ‐‐‐‐ ‐‐ ‐‐‐ ‐‐‐ ‐‐‐ ‐‐‐ Ears, nouse and throat Pneumology Urology Unanswered Speciality 1: Surgery‐Medicine Nursing Pediatrics and Child Nursing Reahabilitation Nursing Psychiatric and Mental Health Nursing Neurosurgery Maternal Health and Obstetrics Nursing Nursing Adminitrations Services Adult and Elderly with chronic disease Nursing Communitary Nursing Gastroenterology Palliative Care Reumathology Geriatric and elderly health Unanswered Speciality 2: Nursing Administrations and management Services Person at risk of life Communication in health Palliative Care Hemodialysis Master in Nursing Science Neurosurgery Geriatric Pos‐ graduation Unanswered Nurses N 176 % 81,1 13 7,4 11 6,3 11 6,3 7 4,0 6 3,4 2 1,1 1 0,6 1 0,6 1 0,6 1 1 1 0,6 0,6 0,6 1 0,6 119 67,6 2 1,1 1 0,6 1 0,6 1 1 0,6 0,6 1 0,6 1 0,6 1 0,6 167 94,9 Application for the 2010 SCML Award xxi Annex Annex 27 Distribution of Health Professionals by number of years after education Total Doctors Nurses N % N % 41 100,0 176 100,0 N.º of years since the education 0 a 4 years 5 a 10 years 11 a 20 years 21 a 30 years > 30 years Unanswered 2 4 5 14 16 0 4,9 9,8 12,2 34,1 39,0 0,0 47 66 38 14 1 10 26,7 37,5 21,6 8,0 0,6 5,7 Annex 28 Identification of the Institution / Organization responsible for training after education Doctors N (8) (100%) Centro de Formação do Hospital Egas Moniz Faculdade de Medicina de Lisboa Hospital Geral de Santo António Instituto de Ciências Biomédicas Abel Salazar Sociedade Portuguesa de Cuidados Intensivos Unidade de Missão para os Cuidados Continuados Integrados Universidade Católica Portuguesa Nurses N (66) (100%) Associação Portuguesa de Cuidados Paliativos Centro de Formação do Hospital de Santa Maria Centro de Formação do Hospital Egas Moniz Centro Hospitalar Lisboa Norte CESPU Escola Superior de Enfermagem da Universidade do Minho Escola Superior de Enfermagem de Calouste Gulbenkian Escola Superior de Enfermagem de Coimbra Escola Superior de Enfermagem do Porto Escola Superior de Enfermagem S. Vicente de Paulo Escola Superior de Saúde Cruz Vermelha Portuguesa Escola Superior de Saúde de Santarém Escola Superior de Saúde de Viana do Castelo ESESFM Faculdade de Medicina da Universidade do Porto/Departamento de Bioética Faculdade de Medicina de Lisboa Faculdade de Medicina do Porto Hospital do Litoral Alentejano Hospital do Visconde de Salreu ‐ Estarreja Hospital Fernando Fonseca Hospital Garcia de Orta Hospital Geral de Santo António Instituto de Ciências Biomédicas Abel Salazar Instituto de Formação em Enfermagem Instituto Português de Oncologia Ordem dos Enfermeiros Sociedade Portuguesa de Cuidados Intensivos Unidade de Missão para os Cuidados Continuados Integrados Unidade Local de Saúde de Matosinhos Universidade Católica Portuguesa Universidade do Algarve Application for the 2010 SCML Award xxii Annex Annex 29 Specific training Doctors N % 41 100 Total Specific pre‐graduate training No Yes Specific pos‐graduating training No Yes Unanswered Total10 Kind of specific training Pós‐Graduation Seminars/Workshops Another11 39 2 95,1 4,9 33 8 0 80,5 19,5 0,0 8 100,0 3 5 2 37,5 62,5 25,0 Nurses N % 176 100 86 90 109 66 1 66 26 35 20 48,9 51,1 61,9 37,5 0,6 100,0 39,4 53,0 30,3 Annex 30 Incentives for training by the service and specific training when the professionals integrated the service. Doctors N % Total Incentive training No Yes Don´t Know Unanswered Training when the provider was integrated in the service No Yes Don´t Know Unanswered 41 100 21 10 9 1 51,2 24,4 22,0 2,4 37 2 1 1 90,2 4,9 2,4 2,4 Nurses N % 176 62 75 37 2 149 20 4 3 100 35,2 42,6 21,0 1,1 84,7 11,4 2,3 1,7 Annex 31 Frequency who follow the TIP Total Doctors Nurses N % N % 41 100 176 100 Frequency who follow the TIP Never Less than 10 patients by year 10 or more patients by year Don´t Know 0 10 30 1 0,0 24,4 73,2 2,4 2 35 133 6 1,1 19,9 75,6 3,4 10 Total equals the number of health professionals who answered yes to the above question 11 Note: the sum is greater than the total because it can be selected more than one alternative. Another types of training cited: In‐service Training in Continuing Care, Master of Palliative Care. Application for the 2010 SCML Award xxiii Annex Annex 32 Team talk about the possibility to be followed at home TIP Total Team talk about the possibility to be followed at home TIP Never Rarely Sometimes Frequently Doesn’t know Not applicable Unanswered Doctors Nurses N % N 100% 41 100 176 100 2 4,9 20 11,4 2 4,9 20 11,4 5 12,2 32 18,2 11 26,8 25 14,2 0 0,0 1 0,6 9 22,0 41 23,3 12 29,3 37 21,0 Annex 33 The family is informed about the cares to provide Doctors Nurses N % N % Total 41 100 176 100 The family is informed about the cares to provide 5 12,2 9 5,1 Never 6 14,6 28 15,9 Rarelly 10 24,4 67 38,1 Sometimes 16 39,0 47 26,7 Frequently 3 7,3 19 10,8 Don´t applied 1 2,4 6 3,4 Unanswered Annex 34 Psychological therapy to family members during the terminal process and after death Total Psychological therapy to family members during the terminal process Never Rarelly Sometimes Frequently Don´t applied Unanswered Psychological therapy to family members after death Never Rarelly Sometimes Frequently Don´t applied Unanswered Never Doctors Nurses N % N % 41 100 176 100 8 9 12 12 0 0 19,5 22,0 29,3 29,3 0,0 0,0 14 17 7 3 0 0 0 34,1 41,5 17,1 7,3 0,0 0,0 0,0 36 34 47 49 7 3 67 44 26 24 1 10 4 20,5 19,3 26,7 27,8 4,0 1,7 38,1 25,0 14,8 13,6 0,6 5,7 2,3 Application for the 2010 SCML Award xxiv Annex Annex 35 Social support to family members during the terminal process Doctors Nurses N % N % 41 100 176 100 Total Social support to family members during the terminal process Never Rarelly Sometimes Frequently Don´t applied Unanswered Social support to family members after the died Never Rarelly Sometimes Frequently Don´t know Don´t applied Unanswered 2 6 10 23 0 0 4,9 14,6 24,4 56,1 0,0 0,0 16 11 10 2 1 0 1 39,0 26,8 24,4 4,9 2,4 0,0 2,4 14 21 49 82 7 3 74 50 23 9 5 11 4 8,0 11,9 27,8 46,6 4,0 1,7 42,0 28,4 13,1 5,1 2,8 6,3 2,3 Annex 36 Strategies to follow the TIP with a multidisciplinary team Doctors Nurses N N Total 41 100 176 100 Multidisciplinary team to follow the Tip Never Rarelly Sometimes Frequently Don´t applied Unanswered Never 7 2 8 17 5 1 1 % 17,1 4,9 19,5 41,5 12,2 2,4 2,4 21 35 34 71 5 9 1 % 11,9 19,9 19,3 40,3 2,8 5,1 0,6 Application for the 2010 SCML Award xxv
Baixar
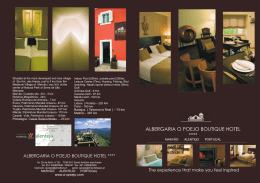


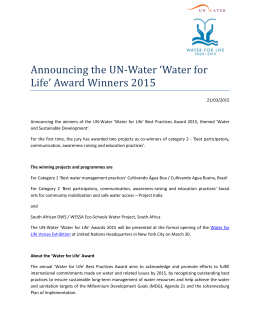


![ÁREA TEMÁTICA: [Classes, desigualdades e políticas públicas]](http://s1.livrozilla.com/store/data/000648442_1-768482465a7b071cc38e0cc23ba02cf6-260x520.png)