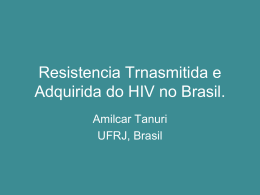
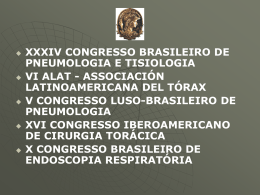
v. 3 n. 8 AWRJ - Abdominal Wall Repair Journal 1 O que você espera em um reparo de Hérnia Ventral Videolaparoscópica? Acesso com mínimo trauma. Facilidade intraoperatória. Fixação segura em qualquer ângulo.1, 2, 3 Endopatch XCEL® Bladeless Trocar Ethicon® Physiomesh Ethicon® Securestrap Visite nosso site: Ethicon.com Referências: 1. Yap, H. & Cardinale, M. Tack comparison surface area CAD, Ethicon internal document, CAD drawings ORN-50-3090 The Lineup, Rev 13. 2. Cardinale, M. et al. Comparison of acute holding strength of an absorbable strap fixation device in porcine flank at various implantation angles, Ethicon Internal Document. 3. Shnoda, P. 28-day mesh fixation study of the Orion device to evaluate mesh migration and tissue response using a swine model, Ethicon internal document, Study Report PSE accession Nº. 09-0132. 2 © Johnson & Johnson do Brasil Indústria e Comércio de Produtos para Saúde Ltda., 2015. Johnson & Johnson Medical Brasil, uma divisão de Johnson & Johnson do Brasil Indústria e Comércio de Produtos para Saúde Ltda. - Rua Gerivatiba, 207 - São Paulo, SP • CEP 05501-900 - Responsável técnico: Nancy Mesas do Rio - CRF-SP nº 10.965 Ethicon® Physiomesh - Registro ANVISA nº 80145901373 - Ethicon® Securestrap - Registro ANVISA nº 80145901386 - Trocartes cirúrgicos Endopatch XCEL® - Registro Anvisa nº 80145900744 AWRJ - Abdominal Wall Repair Journal v. 3 n. 8 Impresso em Março/2015 - Válido de Março/15 a Março/17 - BRMRETH5462. Volume 3 Número 8 Abril 2015 / Julho 2015 Realização: Editor–chefe • Editor-in-Chief SÉRGIO ROLL (SP – Brazil) Editores Associados • Associated Editors JAMES SKINOVSKY (PR – Brazil) JULIO CESAR BEITLER (RJ – Brazil) RIGOBERTO ÁLVAREZ (Mexico) Lapsurg International Institute of Endoscopic Surgery Av. Rep. Argentina, 665, Sl. 1202 Água Verde - Curitiba - PR - CEP 80.240-210 (55) (41) 3242-9257 www.lapsurg.com.br [email protected] Versão: Eletrônica Periodicidade: Quadrimestral ISSN 2317-5982 Apoio: conselho Editorial • Editorial Board ALEXANDER MORREL (SP) ARTUR SEABRA (RS) CRISTHIANO KLAUS (PR) EDUARDO TANAKA (SP) EDVALDO FAHEL (BA) FLÁVIO MALCHER (RJ) GUSTAVO CARVALHO (PE) LEANDRO TOTTI CAVAZOLLA (RS) MARCELO FURTADO (SP) MARCUS VINICIUS DANTAS DE CAMPOS MARTINS (RJ) MAURICIO CHIBATA (PR) MIGUEL NÁCUL (RS) PLÍNIO CARLOS BAÚ (RS) RENATO MIRANDA DE MELO (GO) RICARDO Z. ABDALLA (SP) conselho Editorial Internacional • International Editorial Board ADRIANA HERNANDEZ (Mexico) ALFREDO CARBONELL II (USA) ALFREDO MORENO EGEA (Spain) ANDREW DE BOAUX (United Kingdom) ARTHUR GILBERT (USA) B. TODD HENIFORD (USA) BRENT D. MATTHEWS (USA) DAVIDE LOMANTO (Singapore) EDUARDO PARRA-DAVILLA (USA) GIOVANI DAPRI (Belgium) JAN KUKLETA (Switzerland) JOHANNES JEEKE (Netherlands) JUAN CARLOS MAYAGOITIA GONZÁLES (Mexico) MARC MISEREZ (Belgium) Mariano Palermo (Argentina) Mario Morino (Italy) PARVIZ K. AMID (USA) SALVADOR MORALES-CONDE (Spain) v. 3 n. 8 AWRJ - Abdominal Wall Repair Journal 1 AWRJ - Abdominal Wall Repair Journal Copyright© 2015 by LapSurg Todos os direitos reservados a LapSurg International Institute of Endoscopic Surgery Produção: Primax Edições Projeto Gráfico: Marco Antonio Levandovski Editoração Eletrônica: Erik Ferreira Bibliotecária Responsável: Joelma Marques – CRB 9/1290 DadosInternacionais Internacionais de de Catalogação Catalogação na Dados naPublicação Publicação(CIP) (CIP) AWRJ –– Abdominal Wall Repair Journal [recurso eletrônico] / AWRJ LapSurg International International Institute Institute of of Endoscopic Endoscopic Surgery. Surgery. –– Ano 1, 3, n.1 n.8 LapSurg (abr. 2015/jul. Curitiba : Lap Surg International Institute (dez. 2012/mar.2015)2013)- .―.― Curitiba : LapSurg International of Endoscopic Surgery,Surgery, 2015- 2013. Institute of Endoscopic . Quadrimestral. Quadrimestral. Modo Modo de de acesso: acesso: <http://www.lapsurg.com.br/front/awrj/index> <http://www.lapsurg.com.br/front/awrj/index> ISSN 2317-5982 1. Hérnia – Periódicos. 2. Hérnia – Cirurgia. 3. Hérnia – Tratamento. I. Título. 1. Hérnia – Periódicos. 2. Hérnia – Cirurgia. 3. Hérnia – Tratamento. I. Título. CDD 617.557 CDU 616.34-007.43 CDD 617.557 CDU 616.34-007.43 2 AWRJ - Abdominal Wall Repair Journal v. 3 n. 8 sumário • Summary Conselho Editorial ........................................................................................................... 01 Editorial ............................................................................................................................. 04 Artigos Originais - Original Articles • Impact of Smoking on Ventral Hernia Repair: Analysis of Nsqip.......................... 07 Impacto do tabagismo sobre correção de hérnia ventral: Análise da NSQIP Ciara R. Huntington, Samuel W. Ross, Laurel Blair, Tanushree Prasad, Amy E. Lincourt, Ronald F. Sing, B. Todd Heniford, Vedra A. Augenstein • Extraperitoneal Space: Right Access For Endoscopic Hérnia Repair?..................... 17 Espaço extraperitoneal: Acesso correto para o reparo herniário endoscópico? Leandro Totti Cavazzola, Miguel Prestes Nácul, José Gustavo Olijnyk, João Vicente Machado Grossi Relatos de Casos - Cases Reports • Garangeot’s Hernia: A Case Report .............................................................................. 27 Hérnia Garangeot’s: Relato de caso James Skinovsky, Flávio Panegalli Filho, Fernanda Keiko Tsumanuma, Rômulo Augusto Andrade de Almeida, Alinne Vandramin Anexo High Tech Surgery - Appendix High Tech Surgery • Incidence of Gallbladder Stones after Bariatric Surgery............................................... 31 Incidência de cálculos da Vesícula Biliar após Cirurgia Bariátrica Ibarra Eliana, Pascowsky Maria, Souza Juan Manuel, Vega Emiliano, Pilar Quevedo, Marianela Aguirre Ackerman, Guillermo Duza, Edgardo Serra, Mariano Palermo • Eventos Tromboembólicos em Pacientes Submetidos à Cirurgia Abdominal a Céu Aberto e Cirurgias Videolaparoscópicas.............................................................. 35 Thromboembolic events in patients submitted open abdominal surgery and laparoscopic abdominal surgery James Skinovsky, Cristina Okamoto, Joseph Chenisz, Daniel Lacerda, Augusto Mozzaquatro, Stephan Saab, João Paulo Bacarin Artigo de Revisão High Tech Surgery - Review Article High Tech Surgery • Videocirurgia: De Onde Viemos e Para Onde Vamos?.............................................. 41 Videosurgery: Where we come and where are we going? James Skinovsky, Sérgio Roll v. 3 n. 8 AWRJ - Abdominal Wall Repair Journal 3 EDITORIAL CIRUGÍA LAPAROSCÓPICA POR PUERTO ÚNICA Y MINI-LAPAROSCOPÍA Desde el advenimiento de la cirugía laparoscópica, tanto los avances técnicos como de la industria han permitido que esta sea cada vez menos invasiva. En la búsqueda de menor trauma parietal se desarrollaron ciertas técnicas como la cirugía acuscópica, NOTES y cirugía laparoscópica por puerto único. La cirugía acuscópica desarrollada en los años noventa, siendo Michel Gagner quien la ha descripto, a caído en desuso dado que el instrumental utilizado no presentaba la rigidez suficiente para poder realizar los procedimientos resectivos con adecuada tensión en forma segura, siendo la tensión y triangulación la clave en la cirugía laparoscópica. La cirugía por orificios naturales (NOTES) desarrollada por Kaloo tuvo su auge alrededor del año 2006 para luego caer en desuso por sus dificultades técnicas y baja aceptación de los pacientes, no pudiéndose convertir en una técnica standart. Esta ultima técnica a quedado restringida para pacientes muy seleccionados dando paso al desarrollo de la cirugía laparoscópica por puerto único. Por lo tanto si hay alguna virtud que nos ha dejado el NOTES, es favorecer el desarrollo del puerto único. La cirugía por puerto único utiliza el ombligo como cicatriz natural para el acceso a la cavidad abdominal. Esta permite la realización de diversos procedimientos no dejando prácticamente cicatriz, con lo cual la agresión a la pared abdominal es mínima siendo sus potenciales beneficios un mejor resultado cosmético, menor dolor postoperatorio y mayor confort general del paciente. Para estas dos ultimas variables se siguen aguardando ensayos clínicos controlados aleatorizados. Las desventajas de esta técnica serian la disminución de la triangulación. También ofrece dificultades para la retracción de órganos y choque de instrumentos dado que los mismos ingresan muy próximos entre sí. Numerosas alternativas surgen para sortear estas dificultades como ser, la utilización de diferentes plataformas de acceso, instrumental curvo y/o articulado, y también la colocación de puntos externos para lograra una adecuada retracción de los órganos. Es así como se ha logrado desarrollar instrumental mini-laparoscópico fabricado con la misma rigidez que los instrumentos laparoscópicos convencionales lo cual permite la realización de diferentes procedimientos resectivos abdominales con mínima invasión parietal utilizando puertos de 2,7 a 2,9 mm. Esto permite la misma maniobrabilidad y triangulación de la laparoscopía convencional con la ventaja de menores incisiones y menor trauma parietal. Patologías pasibles de ser realizadas por estas técnicas son: apendicitis, litiasis vesicular y colecistitis, patología de pared abdominal, cirugía colónica, bariátrica y de otros órganos solidos. Por lo tanto creo que tanto la cirugía laparoscópica por puerto único como la mini-laparoscopia son dos opciones mini-invasivas, que presentan similares resultados en cuanto a las complicaciones cuando se la compara con la cirugía laparoscópica multi-puerto, pero con un plus muy 4 AWRJ - Abdominal Wall Repair Journal v. 3 n. 8 EDITORIAL grande como ser un mejor resultado cosmético por un menor trauma parietal, llevando esto a tener un grado de satisfacción muy elevado de los pacientes Dr. Mariano Palermo MAAC, FACS, (Hon)SCGP, (Hon)SBC, (Hon)SPCE Doctor en medicina (UBA). Docente Autorizado de Cirugía de la Universidad de Buenos Aires. Cirujano de Centro Cien – DIAGNOMED y Fundación DAICIM, Buenos Aires, Argentina. Presidente de ICYLS (International Club of Young Laparoscopic Surgeons). Vicepresidente de AIICE (Asociación Iberoamericana de Innovación en Cirugía Endoscópica) v. 3 n. 8 AWRJ - Abdominal Wall Repair Journal 5 Artigos Originais Original Articles 6 AWRJ - Abdominal Wall Repair Journal v. 3 n. 8 IMPACT OF SMOKING ON VENTRAL HERNIA REPAIR: ANALYSIS OF NSQIP Impacto do tabagismo sobre correção de hérnia ventral: Análise da NSQIP Ciara R. Huntington, MD, Samuel W. Ross, MD, MPH, Laurel Blair, MD, Tanushree Prasad MA, Amy E. Lincourt, PhD, MBA, Ronald F. Sing, DO, FACS, B. Todd Heniford, MD, FACS, Vedra A. Augenstein, MD, FACS* Carolinas Medical Center Department of General Surgery Division of Gastrointestinal and Minimally Invasive Surgery Carolinas Medical Center Charlotte, North Carolina Author Contributions Study design: Huntington, Ross, Sing, Heniford, Augenstein Data Acquisition/Analysis: Ross, Huntington, Lincourt, Prasad, Sing, Heniford, Augenstein Manuscript draft: Huntington, Ross, Blair, Sing, Heniford, Augenstein Critical review: All authors Disclosure statement Dr. Heniford holds a patent for CeDARTM, a free mobile application designed to predict the rate and cost of wound complications after ventral hernia repair; he does not receive financial gain from this app. Drs. Heniford and Augenstein have previously been awarded surgical research and education grants from W.L. Gore and Associates, Ethicon, Novadaq, Bard/Davol, and LifeCell Inc. All other authors confirm they have no financial and personal relationships with other people or organizations that could potentially and inappropriately influence this work and its conclusions. *Corresponding Author: Vedra A. Augenstein, MD, FACS, Carolinas Medical Center, 1025 Morehead Medical Drive, Suite 300, Charlotte, North Carolina 28204 Office: (704) 355-8787, Fax: (704) 355-4117, [email protected] Accepted for oral presentation at the Academic Surgical Congress, Las Vegas, NV, February 2015 and presented at the North Carolina Chapter of American College Surgeons Meeting July 2014. Abstract Introduction: Although smoking is known to increase complications following surgery, elective operations on smokers are common, and there is no consensus among surgeons regarding preoperative smoking cessation. This study quantifies the effect of smoking on ventral hernia repair (VHR) using national outcomes data. Methods: The NSQIP database was queried for all elective laparoscopic VHR (LVHR) and open VHR (OVHR) from 2005-2013. Standard statistical tests, v. 3 n. 8 including multivariate regression (MVR) controlling for age, sex, BMI, diabetes, Charlson Comorbidity Index(CCI), recurrent and incarcerated hernia, were performed. Results: There were 162,037, VHRs identified: 30,110 LVHR and 131,927 OVHR. In LVHR, smokers were similar to nonsmokers by rates of recurrent hernia, gender, and mean CCI(p>0.05) but had decreased age, BMI, and diabetes rates and increased rate of incarceration(p<0.05). In OVHR, smokers were more often female with increased rates of recurrent and incarcerated hernias(p<0.05) while non-smokers had increased mean age, BMI, and decreased AWRJ - Abdominal Wall Repair Journal 7 Augenstein et al. Artigo Original CCI(p<0.05). Results of MVR found higher odds for all postoperative complications examined in smokers undergoing OVHR, including wound and other morbidity, reoperation, readmission, and mortality(p<0.05). Likelihood of major complication was increased in smokers undergoing LVHR(p<0.05), but wound complication and mortality were similar(p>0.05). Conclusions: Smoking increases morbidity in LVHR and OVHR, but also carries increased risk of death after OVHR. Preoperative smoking cessation should be goal for all repairs, but if repair must be performed, LVHR is associated with fewer complications than OVHR in a smoker. Keywords: Hernia, Impact of Smoking, Surgery. INTRODUction Smoking is the leading cause of preventable death in the United States with over 480,000 deaths from tobacco-related illnesses annually1. Currently, over 42.1 million Americans smoke cigarettes (18% of the US population). While the smoking rate has decreased slightly in the United States over the past decade, it remains one of the preeminent public health concerns both in this country and across the globe1. Smokers have increased perioperative risks compared to non-smokers. In a recent meta-analysis of 107 studies, smokers had 52% increased rate of overall morbidity2. Specifically, their relative risk of wound complications doubled, with a 54% increase in postoperative infections, and a 73% increase in pulmonary complications2. In another study comparing matched groups of smokers and non-smokers undergoing surgery from the American College of Surgeons National Surgical Quality Improvement Program (NSQIP), smokers had increased rates of unplanned intubation, respiratory failure, pneumonia, and were 1.38 times more likely to die in the month following surgery compared to nonsmokers3. Despite increased risks to their health and cost to the healthcare system, 10 million smokers undergo surgery each year. Ventral hernia repair (VHR) is one of the most common operations performed by surgeons in the United States, with over 350,000 operations performed annually; the majority of which are elective4. Previous studies have confirmed the detrimental effects of current tobacco use in ventral hernia patients; Bencini et al found an association between smoking and increased rate of recurrence in 146 pa- 8 tients undergoing laparoscopic VHR (LVHR). They noted a 58% smoking rate in recurrent hernia group compared to 23% smokers in the non-recurrent hernia cohort, p=0.015. In a study of 1505 patients undergoing VHR at twelve Veteran’s Affairs (VA) hospitals, smoking was associated with 1.5 times greater chance of wound infections compared to non-smokers; it was the only modifiable risk factor for wound complications after VHR identified by the study6. Smokers are much more likely to develop surgical site infections than non-smokers after ventral hernia repair, and smoking remains a predictor of readmission in VHR7. We have previously demonstrated that wound complications in OVHR cost an additional $27,000 in the hospital and an additional $20,000 over a year as an outpatient; mesh infections cost more than $80,0008. Though smoking has persistently been associated with postoperative complications, there has not been a quantification of the effect of smoking on VHR on a national level nor the cumulative effect of years of smoking on outcomes in VHR. Furthermore, studies have examined laparoscopic and open approaches, but the risks that tobacco use might lend to each approach has not been delineated. Therefore, the purpose of this study was to examine national outcomes in VHR in smokers and to quantify the effect of smoking on patient outcomes. The authors hypothesized that, similar to previous literature, smoking would independently be associated with adverse outcomes. Additionally, a secondary goal was to determine the difference in outcomes between LVHR and OVHR in an active smoker. methods DATA SOURCE This is a retrospective cohort study examining smoking impact on patients following VHR utilizing data from the American College of Surgeons National Surgical Quality Improvement Program (NSQIP) database. Demographic information, comorbidities, procedural data, and postoperative complications within 30 days are collected by trained data abstractors, supplemented as necessary with additional questions addressed to treating physicians and follow up calls to patients. Over 400 centers currently participate in this program9. NSQIP VARIABLES AND OUTCOMES NSQIP records over 30 patient comorbidities but does AWRJ - Abdominal Wall Repair Journal v. 3 n. 8 Impact of Smoking on Ventral Hernia Repair: Analysis of NSQIP Abril 2015 / Julho 2015 not include a global comorbidity scale on which to rate patients such as the Charlson Comorbidity Index (CCI)10. The CCI is one such scoring system that has been extensively validated in surgery patients11-13. Age group and major comorbidities are ranked from one to six points. Points are then summated to provide a total patient score that correlates with ten year survival rate14. The authors used available NSQIP data to create a NSQIP Charlson Comorbidity Index which has previously published15, where comorbidities are scored as points according to the original CCI. Previous studies have verified that CCI adapted to large administrative databases have had similar sensitivity in stratifying mortality16,17, and this strategy has been used in NSQIP in previous studies18,19. Primary outcomes of interest for this study were death, and wound-related, major, and minor complications. Additional outcomes of interest were operative time and hospital length of stay (LOS). NSQIP has over 25 complications variables. To facilitate multivariate analysis and comparison between groups, the authors classified complications into wound complications wound disruption, superficial and deep surgical site infections (SSI), minor complications superficial SSI, wound disruption, renal insufficiency, urinary tract infection, bleeding requiring transfusion, and deep vein thrombosis (DVT)/thrombophlebitis, and major complications deep SSI, graft or flap failure, pneumonia, unplanned intubation, respiratory failure, pulmonary embolism, acute renal failure (ARF), cerebrovascular accident (CVA), myocardial infarction, sepsis and septic shock, similar to previously published work15 STUDY DESIGN The NSQIP database was queried for all elective LVHR from 2009-2013 and OVHR from 2005-2013 as determined by current procedural terminology (CPT) codes; CPT codes for laparoscopy were introduced in 2009. The following CPT codes were utilized for LVHR: 49652, 49653, 49654, 49655, 49656, and 49657. The following CPT codes were used for OVHR: 49560, 49561, 49565, 49566, 49570, 49572, 49585, and 49587. Patients under age 18 and cases coded as “emergent” were excluded for primary analysis. Variables are clearly described in the ACS NSQIP data dictionary; smokers are defined as patients who have smoked cigarettes in the year prior to admission for surgery (NSQIP Data Dictionary, acsnsqip.org). Patients who smoke cigars or pipes or use chewing tobacco were excluded. v. 3 n. 8 STATISTICAL ANALYSIS Descriptive statistics were reported as means with corresponding standard deviations for continuous variables and percentages for categorical variables. Bivariate analyses were performed to evaluate patient demographics, comorbidities, operative details, and outcomes with respect to effects of smoking status within each operative approach strata (OVHR and LVHR). Categorical variables were evaluated using Pearson’s Chi-squared and Fisher’s exact test where appropriate. Continuous and ordinal variables were evaluated using two-sample t-tests for normally distributed data or Wilcoxon two-samples test for non-normally distributed data. Multivariate logistic regression (MVR) and Analysis of Covariance (ANCOVA) for adverse patient outcomes were then performed within surgical approach strata controlling for age, sex, BMI, diabetes, CCI, recurrent and incarcerated hernia. Odds ratios with corresponding 95% confidence intervals and ANCOVA adjusted means were used to report the results of the multivariate regression models. Statistical significance was set at p≤0.05, and all reported p values are two-tailed. All data were analyzed using Statistical Analysis Software, version 9.4 (SAS Institute, Inc., Cary, NC). RESULTS PATIENT CHARACTERISTICS There were 162,037 VHRs in the study period: 30,110 LVHR and 131,927 OVHR. General patient characteristics by operative approach are displayed in Table 1. Notably, there were 5,603 smokers in the LVHR strata (18.6%) and 26,310 smokers underwent OVHR (19.9%). Operative details were collected for LVHR and OVHR (Table 2): inpatient admission (41.3% vs. 48.6%), recurrent hernias (14.7% vs. 17.5%), incarcerated hernias (30.0% vs. 24.7%), with most operative fields classified as “clean” (85.3% vs. 79.0%). The average operative times were 97.0 ± 63.6 minutes in LVHR and 100.8 ± 90.9 minutes in OVHR. The mean size of the hernia defect or mesh used is not recorded in this data set. AWRJ - Abdominal Wall Repair Journal 9 Artigo Original Augenstein et al. Table 1 – Patient characteristics 10 AWRJ - Abdominal Wall Repair Journal v. 3 n. 8 Impact of Smoking on Ventral Hernia Repair: Analysis of NSQIP Abril 2015 / Julho 2015 Table 2 – Operative details PATIENT CHARACTERISTICS BY SMOKING STATUS The patient characteristics for LVHR and OVHR groups stratified by smoking status are displayed in Table 3. In LVHR, smokers were similar to nonsmokers by rates of recurrent hernia, gender and mean CCI (p>0.05); however, they had decreased age, BMI, and rates of diabetes, and increased rate of incarcerated hernias (p<0.05). When compared to non-smokers, smokers who underwent OVHR were younger with decreased rates of diabetes, lower mean BMI, and increased average CCI (p<0.05). They were more often female with increased rates of recurrent and incarcerated hernias compared to non-smokers (p<0.05). Table 3 – Patient characteristics by smoking status v. 3 n. 8 AWRJ - Abdominal Wall Repair Journal 11 Augenstein et al. Artigo Original PATIENT OUTCOMES BY SMOKING STATUS Comparisons for each operative approach stratified by smoking status are displayed in Table 4. Analysis of smokers versus nonsmokers in LVHR found no significant difference (p>0.05) for wound complications, minor complications, length of stay (LOS), readmission, reoperation, and mortality, but had increased rates of major complications compared to non-smokers, 2.6% vs. 2.0% (p=0.005). In OVHR, smokers had higher rates of wound complications, minor complications, major complications, mean LOS, reoperation, and readmission (p<0.05). Thirty-day mortality rate was similar in smokers and nonsmokers (p>0.05). Table 4 – Postoperative Outcomes by Smoking Status MULTIVARIATE ANALYSIS BY SMOKING STATUS To control for confounding factors between smokers and nonsmokers, multivariate regression analysis was performed; results are displayed in the Table 5. In OVHR, smokers had a higher odds ratio for all complications examined including 60% increased odds of wound complications (OR 1.6, 95% CI 1.4-1.7, p<0.0001), 30% increased odds of major complications (OR 1.3, 95% CI 1.2-1.4, p<0.0001), and nearly 12 twice the likelihood of 30-day mortality (OR 1.9, 95% CI 1.5-2.5, p<0.0001). In multivariate analysis of LVHR patients, major complications were increased by 70% in smokers compared to non-smokers (OR 1.7, 95%CI 1.3-2.4, p<0.0006). There was no difference in wound complications, minor complications, reoperation, readmission, or 30-day mortality (p>0.05). Paradoxically, adjusted LOS was shorter in the smokers undergoing LVHR compared to non-smokers (mean 1.9 vs. 2.3 days, p<0.0064). AWRJ - Abdominal Wall Repair Journal v. 3 n. 8 Impact of Smoking on Ventral Hernia Repair: Analysis of NSQIP Abril 2015 / Julho 2015 Table 5 – Operative details Discussion This study of over 162,000 elective ventral hernia repairs from a national surgical outcomes database demonstrates that smokers not only have an increased risk of major complications and prolonged hospitalization after VHR, but that operative approach can magnify or mitigate the risks of this elective operation. Cigarette smoking was found to be a substantial independent risk factor for major complications following LVHR and a multitude of postoperative complications after OVHR including wound infection and disruption, major complications, minor complications, reoperation, readmission, and increased risk of post-operative death. While major complication rates are increased in both open and laparoscopic approaches, OVHR carried higher rates of wound complications, reoperation, readmission, and death, even after controlling for confounding factors. Wound infections in VHR have been extensively studied, and reported rates in ventral hernia repair have ranged from 8%-50%20,21. A study designed to find predictive factors of increased wound infection or prolonged length of stay examined 25,172 VHRs using national outcomes data and found that smokers had 1.46 times greater risk of wound infections compav. 3 n. 8 red to non-smokers (95% CI 1.13–1-84, p=0.003)22. Wound healing in tobacco users is impaired at the molecular and cellular levels23,24. Nicotine in tobacco products is a vasoconstrictor which restricts flow to the wound and interferes with angiogenesis25. Additionally, nicotine inhibits proliferation of cells necessary for wound-healing and blocks prostaglandin production, which in turn increases platelet adhesiveness, leading to microscopic thrombosis and tissue ischemia26. Wound complications may lead to mesh infections, hernia recurrences and may progress to reoperation, administration of long term antibiotics, and, potentially, mesh explantation. Wound complications have been shown to be directly-related to recurrence or predict recurrence in several studies27-29. The current study demonstrates that smokers are more likely to develop a wound-related problem in 6.9% of OVHR (compared to 4.7% in non-smokers, p<0.0001) and 1.3% in LVHR (compared to 1.0%, p=0.051). Laparoscopy has previously been associated with fewer infections in VHR than open repair6, and this study confirms that if an operation must be pursued, LVHR may be the safer choice to avoid wound-related complications in smokers. Given the above information, it may also result in fewer recurrences, but this has not been proven in this patient category. Surgical site infections and wound complications in- AWRJ - Abdominal Wall Repair Journal 13 Artigo Original Augenstein et al. crease the risk of hernia recurrence by at least 3-fold, and management of these complications can cost from $25,000 to $50,000 per occurrence30,31. A study presented at the American College of Surgeons in 2013 revealed the expansive cost of these infections; the average cost of a wound complication was $40,000 and mesh infection was $80,0008. Beyond financial consequences, wound infections directly impact patients’ quality of life. Patients with wound complications have increased pain, mesh sensation, and movement limitation at one month postoperatively; even when controlling for confounding factors, VHR patients with wound complications have a significantly poorer quality of life at six months post-operatively compared to those without wound complications32. A predictive model for the development of wound infection after OVHR and its estimated costs was presented at the 2012 American College of Surgeons; along with obesity and uncontrolled diabetes, smoking is one of the most important modifiable comorbidities in the algorithm8. A free version of this algorithm for clinical use is now widely available as the downloadable CeDAR appTM for mobile devices (http://www.carolinashealthcare.org/ download-the-app)8. This mobile app may be useful in preoperative counseling of patients with preventable comorbidities such as tobacco use33. The app is based on 500 patients who underwent VHR at our institution and includes over a million data points. Patients are able to see how smoking cessation among other significant data points changes their risk of wound infections and hospital and follow up charges. Further studies are on the way to validate the efficacy of this recently developed medical app. In this study, more than 26,000 smokers underwent elective OVHR across the US. Univariate analysis demonstrated no difference in the incidence of mortality, but when controlling for confounders, smoking increased the incidence of death within 30 days of the operation compared to non-smokers. While the overall incidence of post-operative mortality was quite low (0.4%), this was a significant finding. Increased mortality in smokers after cardiac and non-cardiac surgery has been demonstrated in some studies, including elective colorectal surgery34-36; however a recent Cochrane analysis failed to demonstrate overall increased postoperative mortality in smokers2. The risk of death was not increased in smokers versus non-smokers undergoing LVHR in univariate or multivariate analysis. In an era where insurance company are tiering surgeons with a new push toward outcomes based reimbursement37-39, there has been considerable debate about 14 whether smokers should be refused elective surgery. Given the increased risk to the patients, smoking cessation should be strongly encouraged40; permanent abstinence from tobacco is possible but rare, but even brief interventions for smoking cessation can be effective41-43. However, smoking cessation at least three weeks prior to surgery can reduce the risks of surgery considerably41,42,44. In one randomized, controlled trial of smoking cessation 6-8 weeks prior to surgery, complications decreased from 52% to 18% in the smoking intervention group with significant improvement in wound-related complications (5% vs. 31%, p=0.001), cardiovascular complications (0% vs. 10%, p=0.08), and reoperation (4% vs. 15%, p=0.07)41. Though 75% of patients who smoke preoperatively endorse a desire to quit, only 5% will be successful in permanent abstinence45. Though some patients are successful in short term smoking cessation, 25% of patients continue to smoke through the perioperative period46. A Cochrane review of 13 trials on preoperative smoking cessation reported that preoperative counseling and nicotine replacement therapy (such as nicotine patches or gum) improved rates of short-term smoking cessation and in some cases, improved postoperative morbidity47. From multiple, albeit small trials, the best evidence to reduce complications and achieve long-term abstinence supports intervention starting 4-8 weeks before surgery including weekly counseling sessions and nicotine replacement47. Active smokers are at increased risk of complications if they undergo VHR. Preoperative optimization of high risk patients should be achieved prior to elective surgery for medical, ethical, and economic reasons8,45,48. Patients with preventable comorbidities such as morbid obesity, uncontrolled diabetes, and active smoking, will see postoperative benefit from targeted preoperative interventions prior to undergoing VHR8. A goal for surgeons should be to counsel patients to make necessary medical and lifestyle changes such as smoking cessation. It is controversial as to whether to ensure adherence with recommendations in ways such as checking cotinine levels prior to surgery (a breakdown product of nicotine found in the urine and blood49). Given the increased rates of morbidity and in some cases, small but increased odds of death, all smokers should be encouraged to quit smoking. When smokers require ventral hernia repair, surgeons might consider LVHR as a way to mitigate smoking-induced complications. This study utilizes national data to provide important insight into the care of ventral hernia in patients who smoke, but it does have several limitations. As NSQIP AWRJ - Abdominal Wall Repair Journal v. 3 n. 8 Impact of Smoking on Ventral Hernia Repair: Analysis of NSQIP Abril 2015 / Julho 2015 is not a hernia specific database, the study unfortunately does not have detailed information on the hernia defect size, location for placement of mesh, type of mesh, technique, or hernia recurrence rates. Thus the multivariate model cannot account for additional technical factors such as surgical technique, use and location of mesh, or defect size. Smokers in NSQIP are self-reported and broadly defined as active smokers if they used cigarettes within the last year, and no other tobacco products are counted40. Patients who stopped smoking either permanently or temporarily in the weeks or months prior to surgery could affect the results of this study. Despite these limitations inherent to the data sources, over 162,000 VHRs are in the dataset, and a considerable proportion of patients undergoing elective surgery across the country are represented. conclusion Smokers who undergo elective OVHR have increased wound, minor, and major complications, increased rates of reoperation, and 30-day readmission. Despite a low overall mortality rate for this operation, smokers have increased odds of peri-operative death compared to non-smokers in OVHR. LVHR performed in active smokers is associated with increased major complications. Smoking cessation prior to surgery should be encouraged, and if a repair is performed, a laparoscopic approach should be considered when appropriate. Further analysis is necessary to stratify adequate length of smoking cessation. Physicians of all specialties need to recognize smoking as a significant risk in surgical patients. Prospective trials are needed, similar to those for perioperative antibiotics and deep venous thrombosis prophylaxis; these trials should focus on guidelines to help ensure smoking cessation pre-operatively and post-operatively and measure improved surgical outcomes. ACKNOWLEDGEMENTS The authors would like to thank Tiffany Cox, M.D., and Bindhu Oommen, M.D., M.P.H., for their assistance with this manuscript. REFERENCES 1. National Center for Chronic Disease Prevention and Health Promotion (US) Office on Smoking and Health. The health consequences of smoking – 50 years of progress: a report of the surgeon v. 3 n. 8 general. Atlanta (GA): Centers for Disease Control and Prevention (US); 2014. 2. Grønkjær M, Eliasen M, Skov-Ettrup LS, Tolstrup JS, Christiansen AH, Mikkelsen SS, Becker U, Flensborg-Madsen T. Preoperative smoking status and postoperative complications: a systematic review and meta-analysis. Ann Surg. 2014 Jan;259(1):52-71 3. Turan A, Mascha EJ, Roberman D, Turner PL, You J, Kurz A, Sessler DI, Saager L. Smoking and perioperative outcomes. Anesthesiology. 2011 Apr;114(4):837-46. 4. Poulose BK, Shelton J, Phillips S, Moore D, Nealon W, Penson D, Beck W, Holzman MD. Epidemiology and cost of ventral hernia repair: making the case for hernia research. Hernia. 2012 Apr;16(2):179-83. 5. Bencini L, Sanchez LJ, Bernini M, Miranda E, Farsi M, Boffi B, Moretti R. Predictors of recurrence after laparoscopic ventral hernia repair. Surg Laparosc Endosc Percutan Tech. 2009 Apr;19(2):128-32. 6. Finan KR, Vick CC, Kiefe CI, Neumayer L, Hawn MT. Predictors of wound infection in ventral hernia repair. Am J Surg. 2005 Nov;190(5):676-81. 7. Lovecchio F, Farmer R, Souza J, Khavanin N, Dumanian GA, Kim JY. Risk factors for 30-day readmission in patients undergoing ventral hernia repair. Surgery. 2014 Apr;155(4):702-10. 8. Colavita PD. Zemlyak AY, Burton PV, Dacey KT, Walters AL, Lincourt AE, Tsirline VE, Kercher KW, Heniford BT. The expansive cost of wound Complications After Ventral Hernia Repair. In: American College of Surgeons, Washington DC; 2013. 9. User Guide for the Participant Use of Data File: American College of Surgeons National Quality Improvement Program; 2007 [Nov 2014]; Available from: https://www.facs.org/~/media/files/ quality%20programs/nsqip/ug06.ashx. 10. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373-83. 11. Birim O, Maat AP, Kappetein AP, van Meerbeeck JP, Damhuis RA, Bogers AJ. Validation of the Charlson comorbidity index in patients with operated primary non-small cell lung cancer. Eur J Cardiothorac Surg, 2003. 23(1): p. 30-4. Eur J Cardiothorac Surg. 2003 Jan;23(1):30-4. 12. Abdollah F, Sun M, Schmitges J, Thuret R, Djahangirian O, Jeldres C, Tian Z, Shariat SF, Perrotte P, Montorsi F, Karakiewicz PI.Development and validation of a reference table for prediction of postoperative mortality rate in patients treated with radical cystectomy: a population-based study. Ann Surg Oncol. 2012 Jan;19(1):309-17 13. Schroeder RA, Marroquin CE, Bute BP, Khuri S, Henderson WG, Kuo PC. Predictive Indices of Morbidity and Mortality After Liver Resection. Annals of Surgery. 2006;243(3):373-379. 14. Charlson M, Szatrowski TP, Peterson J, Gold J. Validation of a combined comorbidity index. J Clin Epidemiol. 1994 nov;47(11):1245-51. 15. Ross SW, Oommen B, Kim M, Walters AL, Green JM, Heniford BT, Augenstein VA. A little slower, but just as good: postgraduate year resident versus attending outcomes in laparoscopic ventral hernia repair. Surg Endosc. 2014 nov;28(11):3092-100. 16. Sundararajan V, et al. New ICD-10 version of the Charlson comorbidity index predicted in-hospital mortality. J Clin Epidemiol. 2004 Dec;57(12):1288-94. 17. D’Hoore W, Bouckaert A, Tilquin C. Practical considerations on the use of the Charlson comorbidity index with administrative data bases. J Clin Epidemiol, 1996; 49(12):1429-33. 18. Ehlert BA, Durham CA, Parker FM, Bogey WM, Powell CS, AWRJ - Abdominal Wall Repair Journal 15 Artigo Original Augenstein et al. Stoner MC. Impact of operative indication and surgical complexity on outcomes after thoracic endovascular aortic repair at National Surgical Quality Improvement Program Centers. J Vasc Surg, 2011; 54(6):1629-36. 19. Bergman S, Martelli V, Monette M, Sourial N, Deban M, Hamadani F, Teasdale D, Holcroft C, Zakrzewski H, Fraser S. Identification of quality of care deficiencies in elderly surgical patients by measuring adherence to process-based quality indicators. J Am Coll Surg, 2013; 217(5):858-66. 20. Kanters AE, Krpata DM, Blatnik JA, Novitsky YM, Rosen MJ. Modified hernia grading scale to stratify surgical site occurrence after open ventral hernia repairs. J Am Coll Surg, 2012; 215(6):78793. 21. Martindale RG, Deveney CW. Preoperative risk reduction: strategies to optimize outcomes. Surg Clin North Am, 2013; 93(5): 1041-55. 22. Kaoutzanis C, Leichtle SW, Mouawad NJ, Welch KB, Lampman RM, Wahl WL, Cleary RK. Risk factors for postoperative wound infections and prolonged hospitalization after ventral/incisional hernia repair. Hernia. 2015 Feb;19(1):113-23. 23. Jorgensen LN, Kallehave F, Christensen E, Siana JE, Gottrup F. Less collagen production in smokers. Surgery, 1998;123(4): 450-5. 24. Jonsson K, Jensen JA, Goodson WH, Scheuenstuhl H, West J, Hopf HW, Hunt TK. Tissue oxygenation, anemia, and perfusion in relation to wound healing in surgical patients. Ann Surg. 1991; 214(5):605-13. 25. Nolan J, Jenkins RA, Kurihara K, Schultz RC. The acute effects of cigarette smoke exposure on experimental skin flaps. Plast Reconstr Surg. 1985; 75: 544-9. 26. Silverstein P. Smoking and Wound Healing. Am J Med. 1992 Jul 15;93(1A):22S-24S. 27. Luijendijk RW, Hop WC, van den Tol MP, de Lange DC, Braaksma MM, IJzermans JN, Boelhouwer RU, de Vries BC, Salu MK, Wereldsma JC, Bruijninckx CM, Jeekel J. A comparison of suture repair with mesh repair for incisional hernia. N Engl J Med. 2000 Aug 10;343(6):392-8. 28. Cobb WS, Warren JA, Ewing JA, Burnikel A, Merchant M, Carbonell AM. Open retromuscular mesh repair of complex incisional hernia: predictors of wound events and recurrence. In: Southern Surgical Association. 2014. Palm Beach, Florida. 29. Todd TB, Williams KB, Bradley JF, Wormer BA, Belyansky I, Walters AL, Lincourt AE, Dacey KT, Kercher KW, Augenstein VA. Ventral and incisional hernia repair with preperitoneal mesh placement: an analysis of technique with long-term follow-up. In: Southern Surgical Association. 2013; Hot Springs, Virgina. 30. Colavita PD, Zemlyak AY, Tsirline VB, Burton PV, Dacey KT, Walters AL, Lincourt AE, Augenstein VA, Kercher KW, FACS, Heniford BT. The expansive cost of wound complcations following ventral hernia repair. In: The American College of Surgeons Annual Clinical Congress; 2013. 31. Scott RD. The direct medical costs of healthcare-associated infections in U.S. hospitals and benefits of prevention. 2009. March 2009 cited 2013; Available from: http://www.cdc.gov/HAI/pdfs/ hai/Scott_CostPaper.pdf. 32. Colavita PD, Tsirline VB, Belyansky I, Walters AL, Lincourt AE, Sing RF, Heniford BT. Prospective, long-term comparison of quality of life in laparoscopic versus open ventral hernia repair. Ann 16 Surg. 2012; 256(5):714-22. 33. Frangou C. New app predicts complications, costs of ventral hernia repair: tool for preoperative discussions with patients. In: General Surgery News; 2014. 34. Singh JA, et al. Mediation of smoking-associated postoperative mortality by perioperative complications in veterans undergoing elective surgery: data from Veterans Affairs Surgical Quality Improvement Program (VASQIP)--a cohort study. BMJ Open. 2013;3(4). 35. Gajdos C, Hawn MT, Campagna EJ, Henderson WG, Singh JA, Houston T. Adverse effects of smoking on postoperative outcomes in cancer patients. Ann Surg Oncol. 2012; 19(5):1430-8. 36. Sharma A, Deeb AP, Iannuzzi JC, Rickles AS, Monson JR, Fleming FJ. Tobacco smoking and postoperative outcomes after colorectal surgery. Ann Surg. 2013; 258(2):296-300. 37. Unicare. Physician Tiering FAQ. 2012 July 1, 2012. cited Nov 2014; Available from: https://www.unicares Sharma A1, Deeb AP, Iannuzzi JC, Rickles AS, Monson JR, Fleming FJ. tateplan.com/ pdf/physicianTieringFAQ.pdf. 38. Wadgaonkar AD. Schneider EC. Bhattacharyya T. Physician tiering by health plans in Massachusetts. J Bone Joint Surg Am. 2010; 92(12):2204-9. 39. Hong CS, et al. Relationship between patient panel characteristics and primary care physician clinical performance rankings. JAMA. 2010; 304(10): 1107-13. 40. Shi Y, Warner DO. Surgery as a teachable moment for smoking cessation. Anesthesiology. 2010;112: 102-7. 41. Møller AM, Villebro N, Pedersen T, Tønnesen H. Effect of preoperative smoking intervention on postoperative complications: a randomised clinical trial. Lancet. 2002; 359(9301): 114-7. 42. Nåsell H, Adami J, Samnegård E, Tønnesen H, Ponzer S. Effect of smoking cessation intervention on results of acute fracture surgery: a randomized controlled trial. J Bone Joint Surg Am. 2010 Jun;92(6):1335-42. 43. Lee SM, Landry J, Jones PM, Buhrmann O, Morley-Forster P. The effectiveness of a perioperative smoking cessation program: a randomized clinical trial. Anesth Analg. 2013;117(3): 605-13. 44. Warner M. Divertie MB, Tinker JH. Preoperative smoking cessation in cabg patients. Anesthesiology. 1984; 60: 380-3. 45. Fiore MC, Cohen SJ, et. al. Treating Tobacco Use and Dependence. Clinical Practice Guideline., 2000, US Department of Health and Human Services: Rockville, MD. 46. Theadom A, Cropley M. Effects of preoperative smoking cessation on the incidence and risk of intraoperative and postoperative complications in adult smokers: a systematic review. Tob Control. 2006 Oct;15(5):352-8. 47. Thomsen T, Villebro N, Møller AM. Interventions for preoperative smoking cessation. Cochrane Database Syst Rev. 2010 Jul 7;(7):CD002294. 48. Snowden CP, Anderson H.Preoperative optimization: rationale and process: is it economic sense? Curr Opin Anaesthesiol. 2012 Apr;25(2):210-6. 49. Moyer TP, Charlson JR, Enger RJ, Dale LC, Ebbert JO, Schroeder DR, Hurt RD. Simultaneous analysis of nicotine, nicotine metabolites, and tobacco alkaloids in serum or urine by tandem mass spectrometry, with clinically relevant metabolic profiles. Clin Chem. 2002 Sep;48(9):1460-71. AWRJ - Abdominal Wall Repair Journal v. 3 n. 8 EXTRAPERITONEAL SPACE: RIGHT AcCESS FOR ENDOSCOPIC HÉRNIA REPAIR? Espaço extraperitoneal: Acesso correto para o reparo herniário endoscópico? Leandro Totti Cavazzola, 2Miguel Prestes Nácul, 3 José Gustavo Olijnyk, 4João Vicente Machado Grossi 1 Universidade Federal do Rio Grande do Sul, Faculdade de Medicina, Programa de Pós-Graduação em Medicina - Ciências Cirúrgicas, Porto Alegre, Brasil 1-4 ABSTRACT The correction of inguinal hernias is one of the most performed surgeries in the world today. Although this procedure is considered safe, simple and have satisfactory results, there is no consensus regarding the best technique to use. Today, the inguinal hernia repair can be accomplished by open or endoscopic video techniques. Although open techniques dispend am lower cost, video-endoscopic techniques are considered more cost-effective in reducing the time of postoperative recovery causing a positive socioeconomic impact. Currently the transabdominal preperitoneal (TAPP) and totally extraperitoneal (TEP) are the most widely used endoscopic video. The TEP has lower cost per dispense with the use of clamps and allow better postoperative recovery. However, the TEP is more difficult to perform, because it has a lower visual field that may be partially offset by performing a good dissection of the extraperitoneal space. For this reason, the use of a balloon dissector is critical. This review about the methods for accessing the extraperitoneal space in video endoscopic inguinal hernia repair by totally extraperitoneal technique includes the advantages and disadvantages of different techniques to access the extraperitoneal space such as closed and open with finger dissection with optica (“telescóptica”) and balloon. Keywords: TEP. Inguinal hernia. Balloon. Hérnia repair. BACKGROUND New technologies and innovations in surgical approaches need to demonstrate an improvement in patient care especially in regard to their safety, satisfaction, ease of use and cost-effectiveness1,2 relationship. The great v. 3 n. 8 success of laparoscopic cholecystectomy encouraged surgeons to seek other indications for the method, eg, the treatment of hernias of the inguinal3 region. Inguinal hernias of the region represent 75% of all abdominal wall hernias, one of the most common ailments of adults and can lead to complaints such as pain and discomfort4. The risk of a man developing a hernia in the groin during your life is 27%, nine times higher than in women5. Surgical treatment of a hernia in this region is the procedure most often performed abdominal surgery and the most commonly performed by general surgeons in the United States. In this country, approximately 700,000 surgeries are performed each year, making up 15% of all surgeries according to data from the National Center for Health Statistics5. 20 million repairs are performed annually worldwide6. The data in Brazil are not as well known. According to the Brazilian Institute of Geography and Statistics (IBGE), approximately 5.4 million people suffer from hernia in Brazil7 Abdominal wall hernias were responsible for about 500 000 surgeries performed between 1993 and 1996 by general surgeons SUS (Unified Health System), ranking second among the procedures hired, costing the state coffers about 100 million dollars at the time8. Data from DATASUL regarding hospitalizations for the treatment of abdominal wall hernias SUS express the reality of the public health system, which in 2012 represented 74.9% of the population who did not have additional9 health plan. These data show that in Brazil the percentage of inguinal hernioplasty performed by video-endoscopy is very low. From 2008 to 2012 162 008 cholecystectomies were performed by laparoscopic inguinal hernioplasty but only 3982 were made by this method in this period10. From January to October 2013, 94150 and 11858 hernioplasty unilateral inguinal bilateral inguinal hernioplasty were performed by SUS. Only 657 of these were made by endoscopic techniques10. AWRJ - Abdominal Wall Repair Journal 17 Artigo Original Cavazzola et al. The treatment of inguinal hernias region has been an area of controversy in surgical practice from the moment he was conceived. Although the procedure is considered safe and relatively simple, with satisfactory results, patients may experience a prolonged postoperative recovery, with a delay in returning to normal work activities and recurrence. Thus, the inguinal hernia region not only affect the individual patient, but also have great socioeconomic importance and significant impact on employment, disability and costs to the health system with a recurrence rate of 5% to 10% and a cost of over 28 billion dollars in the United States11. Throughout history, many techniques have been proposed and innovations for their treatment. These innovations were adopted through a combination of subjective processes and application of scientific method12. During the past 25 years, the treatment of inguinal hernias region has undergone a dramatic change. Clearly, the force responsible for this change was the desire to reduce the length of hospital stay, the patient’s disability and recurrence rates13. The advent of laparoscopy with successful laparoscopic cholecystectomy, the acceptance of the use of prostheses and the effectiveness of extraperitoneal repairs enabled the development of video-endoscopic techniques for repair of inguinal hernias crus13,14. Many of the early attempts use of laparoscopy for the treatment of inguinal hernia region of non-adherence to technical principles learned with open surgery, probably due to technological deficiency. Subsequent technological advances have allowed a return to the principles established15 In 1992 Arregui and colleagues16 and Dion and Morin17 reported a posterior preperitoneal trans-abdominal laparoscopic approach, now known as technical pre-trans-abdominal peritoneal (TAPP) using a large prosthesis to completely cover the hole miopectin Fruchaud of overlapping. The prosthesis was fixed superiorly and inferiorly in the abdominal transverse arch ligament of Cooper with a stapling device. Inguinal hernia surgery endoscopic TAPP was accompanied by several surgeons including Corbitt18. In these early years of video-endoscopic era, TAPP repair using a polypropylene mesh, expanded PTFE or polyester was the predominant method for the treatment of inguinal hernias by laparoscopic15. However, both the TAPP repair as obviously required repair IPOM entry into the peritoneal cavity. Dulucq19 was the first surgeon to perform a direct extraperitoneal approach without entering the abdominal cavity an inguinal hernia crural region to repair, Ferzli in 199220 and McKernan and Laws22 later popularized technique 18 Dulucq preferring the term “totally extraperitoneal” (TEP). Using an open access, dissection was performed directly in the extraperitoneal space without any access to the peritoneal cavity. In 1993 Phillips and colleagues23 Arregui et al24 reported a technique in which separate the extraperitoneal space initial dissection was performed under direct vision through a video endoscopic optical introduced into the peritoneal cavity. The optics was later relocated to the extraperitoneal space and the procedure completed as a endoscopic inguinal hernia repair (TEP). The first video endoscopic inguinal hernia surgery in Brazil was held in October 1991 by the surgeon of São Paulo Sergio Roll which published its first series of 58 patients in 199325. Never interest in inguinal hernia repair was so intense and this is due to the advent of video-endoscopic techniques that have evolved in parallel with the experience and technology11. Currently, the two video endoscopic techniques used for the treatment of inguinal hernias crus are trans-abdominal preperitoneal (TAPP) and totally extraperitoneal (TEP) using a polypropylene mesh. The video-endoscopic repairs continue to develop its place in the surgical armamentarium for the treatment of inguinal hernias crus. Endoscopic techniques used today achieve excellent long-term results with a low rate of recurrence, but the prevention of chronic inguinal pain remains difficult4,25. The lack of consensus in the literature about the best repair technique or how ideal to ensure a durable result in long-term prosthesis is also amazing4,25. INGUINAL HERNIA REPAIR TECHNIQUE FOR TOTALLY EXTRAPERITONEAL ENDOSCOPIC (TEP) CONCEPTS The description of endoscopic TEP inguinal hernia repair by Dulucq19 in the early 1990s in Europe can be considered as a logical further development of the TAPP technique26. The TEP technique has gained popularity in recent years and has been considered by some authors as the TAPP preferred because it is less invasive and prevent entry into the peritoneal cavity4,27 The video endoscopic inguinal hernia repair TEP synergy advantages of minimal access to the a tension-free repair using prosthesis28. The video endoscopic inguinal region of vision by the posterior approach allows the surgeon a magnified panoramic exhibition of three possible hernia defects (defect direct, indirect and femoral besides the shutter) contributing to the AWRJ - Abdominal Wall Repair Journal v. 3 n. 8 Extraperitoneal Space: Right Access for Endoscopic Hérnia Repair? Abril 2015 / Julho 2015 understanding of the occult hernias or recurrences. The extraperitoneal space is logical for prosthesis implantation site. This anatomical space, the prosthesis far from the subcutaneous tissue is relatively avascular, and suffers the action of intra-abdominal keeps it in place by pushing it against the anterior abdominal wall pressure. This also allows non prosthesis fixation by avoiding the use of staples which is costly and may be associated with postoperative pain4,25. Clearly if the surgical procedure is performed in the extraperitoneal space, access it directly would be preferable. The video endoscopic inguinal hernia repair TEP will involve a peritoneal access, avoiding possible injury or visceral adhesions. In addition, it incorporates more easily using instrumental 3 millimeters (mm) with the inherent advantages of minilaparoscopy as the expansion of visual space and field of work, decreased incidence of peritoneal injury and esthetical result29. The TEP for inguinal hernia repair is a complex procedure mainly be held in a restricted virtual space, the extraperitoneal space, which has to be accessed and developed during surgery. Therefore, dissection of the extraperitoneal space is fundamental step in the surgical procedure. Therefore, some concepts on anatomical spaces should be established. ANATOMICAL SPACES The advent of endoscopic surgery, several potential anatomical spaces have attracted the interest of surgeons as true “secret passages”30,31. Anatomical space can be defined as a cavity or compartment. Have potential space is one that is not apparent until distention or created by dissection. In 1991, Haines32 defined a space true potential as that to be created does not alter the structural and functional integrity of tissue offers a mesothelial lining which is covered with small amount of serous fluid and can be repeatedly created and obliterated without causing tissue damage or require repair. With connective tissue planes a thin layer of loose areolar tissue connects adjacent surfaces. The separation of these surfaces determines, even minimal tissue damage. A surgical procedure in this kind of space tends to injure areolar tissue and adhesions may form, hindering or even preventing the repeated access to this space. Most anatomical areas covered by video-endoscopic techniques, including the extraperitoneal space, cannot be considered “true potential spaces” because it does not meet the criteria of Haines30,31. In a surgical procedure, spaces or anatomical planes need to be opened by an active physical process such as dissection in order to separate the adjacent tissues v. 3 n. 8 previously in contact so that its shape and extension can be configured and operated. The blunt dissection can be, even with the use of hand or finger only. For video endoscopic procedures, this pre-dissection prior to the introduction of gas or liquid. It is necessary to develop and refine methods to create, develop and explore anatomical spaces through natural or surgically created pathways30,31. EXTRAPERITONEAL SPACE Using the concept of Haines32, the extraperitoneal space is not a true “potential space”, even though its surface can be easily separated. However, since dissected anatomic changes in the characteristics of the space depending on scar formation occurs, and may be even more significant if a prosthesis or other biomedical material has been placed. The repetition of the dissection in a second moment becomes complicated and even contraindicated. Despite the increased interest in the surgical community, only relatively few centers worldwide have adopted the extraperitoneal video-endoscopic access as standard. Lack of space, difficulty in spatial orientation and anatomical identification are the problems most frequently encountered by the surgeon33,34. Either way, video-endoscopic surgical procedures of the extraperitoneal space including the retroperitoneum, are considered safe and feasible with various techniques described in the literature35 However, it is essential to understand these anatomical and surgical concepts in inguinal hernia repair for video-endoscopic TEP, the correct plan is accessed and dissected36. The extraperitoneal space involves all portions of the abdomen that are located outside the serous membrane known as the peritoneum that covers part or all of abdominal organs37. The retroperitoneum is a part of the abdominal cavity located between the posterior parietal peritoneum and the posterior abdominal wall. Its upper part extends to the peritoneal reflection liver (with an upper limit diaphragm) and its bottom goes to the extraperitoneal pelvic region, and bounded below by the pelvic diaphragm38. As Lange et al36, the pre-peritoneal space is located between two components of the preperitoneal fascia complex: a lap component known as posterior lamina of the dorsal fascia transversalis and component known as preperitoneal fascia. It is difficult to look for the correct line of cleavage in this space in the posterior layer of the transversalis fascia. Furthermore, the position of the arcuate line is variable. The ventral (posterior layer of the transversalis fascia) would AWRJ - Abdominal Wall Repair Journal 19 Artigo Original Cavazzola et al. be suspended between the arcuate line and the pubis. This component serves as a cover of the actual preperitoneal space and must be opened so that it is accessed. Already dorsal component of preperitoneal fascia is inserted in the bladder probably preventing spontaneous cleavage of that structure together with the peritoneum during dissection. Both components originate in the posterior fascia of the rectus abdominis muscle. Katkhouda and colleagues28 argued that access to the preperitoneal space was performed at the level of the arcuate line to this space really was not accessed and the posterior fascia of the rectus abdominal inferior epigastric vessels where they are. The correct dissection plane find themselves between the rectus abdominis muscle and the posterior lamina of the transversalis fascia. This fascia must be incised so that it is in the correct space. If this fascia is left intact dorsally, the lower epigastric vessels tend to stand out from the rectus abdominis muscle without the support of the ventral component, getting in a “clothesline”, obstructing the view and sometimes needing to be connected. Lange and colleagues36 reinforced this concept that an inguinal hernia surgery video-endoscopic technique for TEP, the floor of the procedure should be made by the peritoneum covered by the dorsal component of the pre-peritoneal fascia and preperitoneal fat. The anatomical adequate workspace can only be accessed after the cleavage of the ventral component of the two layers preperitoneal fascia, also known as the posterior layer of the transversalis fascia complex. Moreno-Egea et al39 have discussed the term “pre-peritoneal space,” suggesting that if using only the term “extraperitoneal space.” Also suggested that this concept also applies to the retroperitoneal space. For the authors, the term pre-peritoneal fascia should be common to all its regional meanings (urogenital fascia, umbilical-prevesical fascia, lumbar fascia, sacrum-genital-rectal fascia, etc.). The authors description the fascia transversalis separately, even if folded back to hold the inferior epigastric vessels, with the call back layer is considered the pre-peritoneal fascia. In 1858, Retzius described the homonymous lateral to the bladder (bladder pre-space), separated by prevesical umbilical fascia space, anterior and situated. The space of Retzius is also displayed on a video endoscopic inguinal hernioplasty PET, but should avoid any operation on this medial zone (Cooper ligament below) to not cause injury to the bladder or venous plexus40. Bogros (1786-1825) described a triangular space in the iliac re- 20 gion between the iliac fascia, transversalis fascia and parietal peritoneum. The space Bogros lies between the peritoneum and the posterior lamina of the transversalis fascia separated by internal spermatic fascia41 and is correct to be accessed and developed in a video endoscopic inguinal hernia repair TEP space. Like Lange, Moreno-Egea and colleagues39 found that the variety of terms used to describe the fascial elements involved in a video endoscopic inguinal hernia repair TEP make complex understanding of the workspace this technique to surgeons unaccustomed to this approach, hindering spreading technique. Conclude that it is necessary to create a consensus on the terminology for the wider dissemination of the TEP repair. Understanding this knowledge should encourage the spread of this video-endoscopic repair. EXTRAPERITONEAL SPACE ACCESS Endoscopic access to the extraperitoneal space began with a focus on addressing the retroperitoneal organs, mainly for urological procedures. In 1969, well before the blossoming of laparoscopy, Bartel42 performed the first endoscopic visualization of the retroperitoneal space with a mediastinoscopy, using an open access technique without gas. In 1978, Wickham was the first to perform an air insufflation of the retroperitoneal space for the realization of a ureterolithotomy33. In 1980, Hald and Rasmussen43 described the first dissection video-endoscopic retroperitoneal also with the help of a mediastinoscopy. The authors, however, found very limited due to the use of only a gas for performing dissection. The historical description of Clayman laparoscopic nephrectomy for a transperitoneal approach in 199144 created a worldwide interest in video endoscopic surgery of the retroperitoneal organs. A year later, Clayman described the first nephrectomy using a retroperitoneal approach. However, discouraged by inadequate workspace and retroperitoneal air suboptimal due to the limitation of the initial dissection of the retroperitoneal space, the authors chose the transperitoneal approach in its subsequent cases-. The retroperitoneal organs are usually addressed by extraperitoneal route in open procedures. Thus, the video-endoscopic surgery, the retroperitoneal route would be the logical choice technique for exploration of the retroperitoneum. However, the presence of dense fibrous trabeculae and retroperitoneal adipose tissue do not allow the creation of a satisfactory air retroperitoneum without the use of disruptive force. The shortage of space for surgical manipulation due to unsatisfactory retroperitoneal air was mainly res- AWRJ - Abdominal Wall Repair Journal v. 3 n. 8 Extraperitoneal Space: Right Access for Endoscopic Hérnia Repair? Abril 2015 / Julho 2015 ponsible for the poor results of this method in the past and its limited dissemination46 the revival of retroperitonealscopy reason was due to the pioneering work of Indian urologist Mumbai, Durga Gaur that opened the retroperitoneal and extraperitoneal routes for surgeons. In 1992, Gaur published their experience with the use of a handmade balloon dissection to develop the extraperitoneal space47. The balloon dissector allowed rapid dissection of fibro-fatty tissue of the retroperitoneum, creating adequate space for performing endoscopic surgical procedures. Through this seminal article considered, all retroperitonealscopy evolved (Figure 1). Figure 1 – Balloon original of Durga Gaur 1992 The first publications in the early 1990s describing inguinal hernia surgery video-endoscopic TEP did not use any type of balloon dissector in accessing the extraperitoneal space, but direct dissection with the help of finger48 or optical video-endoscopic, call for “telescoping dissection”49. Later, the use of a dissector, or processed artisan flask was proposed. The introduction of the balloon dissector has made access to the extraperitoneal space to be simplified. THE TECHNIQUES OF ACCESS EXTRAPERITONEAL SPACE The most important step in conducting an endoscopy surgical procedure in the extraperitoneal space is to obtain satisfactory access. The video extraperitoneal laparoscopic approach provides secure and minimally invasive procedures to a variety of approach. This technique has a learning curve and requires a thorough knowledge of the anatomy of the extraperitoneal space49. Wickmam33 and Clayman45 published the first v. 3 n. 8 descriptions of access techniques for urological retroperitoneal endoscopic video. Wickmam described an open technique in which plans for after opening the abdominal wall to access the retroperitoneal space, an initial digital dissection followed by dissection with optical video-endoscopic (telescopic dissection) and carbon dioxide gas itself (CO2) was performed. Clayman already described a closed technique in which one needle puncture was performed in Veres extraperitoneal space. After insufflation to about 10 to 15 millimeters of mercury (mmHg) was positioned one trocar puncture “blind” in the retroperitoneum. As the pre-space achieved with this technique was still limited, was also required additional telescopic dissection with the use of gas (CO2). The problem with these techniques is not determined that an initial air in retroperitoneum satisfactory. Dissection in this way can be difficult, time consuming and even frustrating, because the initial view does not permit the identification of anatomical landmarks and even simple endoscopic spatial orientation50. These access techniques to the retroperitoneum were reproduced for access to the extraperitoneal space for the realization of a video endoscopic inguinal hernia repair TEP. The basic principle is to create an anatomical space through which the miopectin hole can be visualized49. THE CLOSED TECHNIQUE Dulucq27 first published a technique of closed access to the extraperitoneal space for the realization of a video endoscopic inguinal hernia repair TEP. A Veres needle was positioned in the space of Retzius through a puncture in the suprapubic region. Then proceeded with CO2 insufflation and placement of a trocar directly “blindly” into the extraperitoneal space. In this method, it is difficult to accurately place a Veres needle in the correct anatomical space. Furthermore, the workspace is initially narrow4. Access via the transperitoneal visualization is an alternative (Grade D - MBE)4. This technique starts with the creation of a pneumoperitoneum and placement of a trocar into the peritoneal cavity. The initial dissection of the extraperitoneal space is held with forceps endoscopic video of 3 or 5 mm into the extraperitoneal space positioned under transperitoneal view with the aid of CO2. Although relatively simple and cost-effective not to use any material single use, this technique may present some potential complications inherent to the peritoneal access as visceral injury or herniated portal. Furthermore, the presence of pneumoperitoneum can compromise the extraperitoneal space29. AWRJ - Abdominal Wall Repair Journal 21 Artigo Original Cavazzola et al. Another way of achieving access to the extraperitoneal space enclosed by technique described in Patent US 5271380 of 1993 Siegfried Riek et al51 US 5334150 and Steven Kaali 199452 who invented the “optical trocar.” Unlike a conventional trocar in the tissue penetration is performed blindly optical display trocars to allow tissue penetration when the trocar is advanced through the abdominal wall. An optical trocar consists of a rigid tube with a transparent window in the distal portion of acute penetrating format. A rigid optic endoscopic video miniature camera and coupled to a light source positioned within the optical trocar allows the visualization of the tissues at the tip of the tube through the transparent penetrating window. These patents have generated two products to market: the Visiport® produced by ©Covidien (Mansfield, USA) and the Xcel Endopath Bladeless® Company © Johnson & Johnson (Cincinnati, USA). In 2008, Tai and co-workers53 describe a technique for access to the closed space for an extraperitoneal endoscopic video inguinal hernia repair with the use of PET Visiport® (©Covidien). The goal would be to simplify and accelerate the installation of extraperitoneal working space. The use of the optical trocar caused a decrease in access time and less loss of gas during the procedure. One of the problems of the technique was the extra cost of the optical trocar. The use of an optical trocar for developing the extraperitoneal space has not spread. This type of trocar is currently used primarily to access to the cavity, the peritoneal cavity especially in situations involving risk of puncture accident, especially in patients with previous surgery. THE OPEN TECHNIQUE Initially described by Ferzli et al20 and McKernan and Laws21, the open space for access to the extraperitoneal endoscopic video inguinal hernioplasty TEP technique, is carried out in most cases with a trocar type Hasson. Through a umbilical skin incision for median-(the side of the hernia) transverse 1-2cm long, the anterior fascia of the rectus abdominis muscle is addressed. Originally, the fascia was incised was made longitudinally on the midline. However, cross the midline increases the risk of peritoneal opening. Therefore, the technique was modified to a transverse incision along the anterior sheath of the rectus abdominis muscle49. After opening the fascia, the muscle is retracted laterally (or trans-rectal access done) and the space between the rectus abdominis muscle and its posterior sheath is accessed under direct vision. More recently, Daes54 described a variation of the open technique. 22 Access was obtained in a well-lateralized position in cranial and abdominal wall on the side of the hernia. After reaching the extraperitoneal space, Daes used a balloon dissector and held the section of the semilunar line with video-endoscopic visualization. A modification of the technique aimed to facilitate anatomical understanding, working in an area with more space, allowing the TEP repair even the most complex cases and in large hernias, prior prostatectomy, incarcerated hernias, patients who have a small distance between the navel and the pubis and obese. The skin incision open technique should be larger than the size of the trocar around 12-15mm to allow adequate visualization of the anatomical planes and allow the insertion of a finger, the trocar device or a balloon dissector43. The dissection of the anatomic structures through a small incision is especially difficult in obese patients. If you choose to extend this incision, access is facilitated, but increases the chance of gas leakage around the trocar, which interferes with the maintenance of an adequate air pre-peritoneum55. When an open access is performed to dissect the extraperitoneal space can be initiated using one of the following techniques49: a) The digital dissection In this technique, one uses the blunt tip of a finger. A gentle sweeping motion across the midline of the pubic symphysis is first employed. This dissection with the finger should be tangential to the rectus muscle. Once this is done, the Linea Alba is hooked with your finger and pulled the cephalic direction, causing it to rupture. With experience, the digital dissection offers a fast, effective, safe and less costly alternative technique49. However, this approach requires an incision large enough to accept the surgeon’s finger size. Depending on the size of the incision, higher gas leak can occur, making it difficult to maintain the extraperitoneal space. In addition, an extended scar is not desired56. b)Dissection with optical (“Telescopic”) The telescopic blunt dissection under direct vision with an optical endoscopic was described by Ferzli and colleagues20 using a 10mm trocar with a working channel of 5mm, and McKernan and Laws21 is a method often used in many centers around the world25. It is initiated by placing a 10mm trocar into the extraperitoneal space. Using the very perspective of 10mm (preferably zero degrees in order to have a front view), the dissection is carried medially until first the retropubic space of Retzius and then continues laterally into AWRJ - Abdominal Wall Repair Journal v. 3 n. 8 Extraperitoneal Space: Right Access for Endoscopic Hérnia Repair? Abril 2015 / Julho 2015 the space Bogros and fascia ileos-psoas. The dissection remains in the midline in a plane parallel to the rectus abdominis muscle to stop any bleeding or peritoneal injury and should be carried out later through the posterior lamina of the inner portion of the transversalis fascia as described by Cooper49. The anatomical delineation and development of the extraperitoneal working space in a video endoscopic inguinal hernia repair TEP is also satisfactory with both the digital dissection how to telescopic. However, both techniques are more time consuming, may cause more bleeding and the initial anatomical identification is more complex25. Because of the limitations of the techniques described above, the use of a balloon dissector has been proposed. c) The Balloon Dissector After the initial access to the extraperitoneal space in open surgery, the balloon dissector is introduced along the posterior part of the abdominal rectus muscle toward the pubis and positioned in the extraperitoneal space. The balloon is inflated with liquid or gas separating adjacent tissue layers and create the desired space49. After the completion of the initial creation of anatomical space, the balloon must be kept inflated for approximately 5 to 7 minutes for hemostasis56. After the balloon is removed, the primary and secondary portal are established and the video endoscopic inguinal hernia repair performed TEP. When the introduction of optical endoscopic should first assess the quality of dissection with the balloon, trying to detect any peritoneal injury, vascular or visceral and whether there are any fragments of the balloon. If the initial dissection balloon is not satisfactory for either its quality or its extension, additional fascial barriers can be broken with the finger or the tip of the optical or even repeated with the dissection balloon57. REFERENCES 1. Skinovsky J, Roll S. Cirurgia por acesso mínimo e novas tecnologias cirúrgicas. In: Cirurgia por acesso mínimo. Rio de Janeiro: Revinter; 2011. p. 1-3. 2. Satava RM. Emerging technologies for surgery in the 21st century. Arch Surg.1999 Nov;134(11):1197-202. 3. Melo MC. Mudanças: conceitos e resistências. In: Melo MC, editor. A reconfiguração da cirurgia. Recife, PE: Editora Prazer de Ler; 2010. p. 21-39. 4. Simons MP, Aufenacker T, Bay-Nielsen M, Bouillot JL, Campanelli G, Conze J, et al. European Hernia Society guidelines on the treatment of inguinal hernia in adult patients. Hernia. 2009 Aug;13(4):343-403. v. 3 n. 8 5. Primatesta P, Goldacre MJ. Inguinal hernia repair: incidence of elective and emergency surgery, readmission and mortality. Int J Epidemiol. 1996 Aug;25(4):835-9. 6. Cavazzola LT, Rosen MJ. Laparoscopic versus open inguinal hernia repair. Surg Clin North Am. 2013 Oct;93(5):1269-79. 7. Ministério do Planejamento, Orçamento e Gestão. Instituto Brasileiro de Geografia e Estatística (IBGE) [homepage na internet]. Censo Demográfico 1960, 1970, 1980, 1991, 2000 e 2010. 2014 mar 13. Disponível em: http://www.censo2010.ibge.gov.br/sinopse/index.php?dados=8. 8. Lopes AG, Souza JCL, Bienik TS, Velozo TS, Nader PA, Cardoso JR. Tratamento da hérnia inguinal com anestesia local. ABCD Arq Bras Cir Dig. 2004; 17(1): 26-8. 9. Ministério da Saúde. Agencia Nacional de Saúde Suplementar (ANS) [homepage na internet]. FOCO Saúde Suplementar. 2012 dez. Disponível em: http://www.ans.gov.br/images/stories/Materiais_para_pesquisa/Perfil_setor/Foco/20130124_foco_dezembro_web_2012.pdf. 10. Ministério da Saúde. DATASUS [homepage na internet]. Procedimentos hospitalares do SUS por local de internação. 2014 mar 13. Disponível em: http://tabnet.datasus.gov.br/cgi/deftohtm. exe?sih/cnv/qiuf.def. 11. Nathan JD, Pappas TN. Inguinal hernia: an old condition with new solutions. Ann Surg. 2003 Dec; 238(6 Suppl):S148-57. 12. Chowbey PK, Khullar R, Sharma A, Soni V, Baijal M. Totally extraperitoneal repair of inguinal hernia: Sir Ganga Ram Hospital technique. J Minim Access Surg.2006 Sep;2(3):160-4. 13. Bowne WB, Morgenthal CB, Castro AE, Shah P, Ferzli GS. The role of endoscopic extraperitoneal herniorrhaphy: where do we stand in 2005? Surg Endosc. 2007 May;21(5):707-12. 14. Lau WY. History of treatment of groin hernia. World J Surg. 2002 Jun;26(6):748-59. 15. Kingsnorth NA. General Introduction and History of Hernia Surgery. In: Kingsnorth, NA, LeBlanc KA, editor. Management of Abdominal Hernias. 4th ed. London: Springer; 2013. p. 1-23 16. Arregui ME, Davis CJ, Yucel O, Nagan RF. Laparoscopic mesh repair of inguinal hernia using a preperitoneal approach: a preliminary report. Surg Laparosc Endosc. 1992 Mar;2(1):53-8. 17. Dion YM, Morin J. Laparoscopic inguinal herniorrhaphy. Can J Surg. 1992 Apr;35(2):209-12. 18. Corbitt JD Jr. Transabdominal preperitoneal herniorrhaphy. Surg Laparosc Endosc. 1993 Aug;3(4):328-32. 19. Dulucq JL.Treatment of inguinal hernia by insertion of a subperitoneal patch under pre-peritoneoscopy. Chirurgie. 1992;118(12):83-5. 20. Ferzli GS, Massad A, Albert P. Extraperitoneal endoscopic inguinal hernia repair. J Laparoendosc Surg. 1992;2(6):281-6. 21. McKernan JB, Laws HL. Laparoscopic repair of inguinal hernias using a totally extraperitoneal prosthetic approach. Surg Endosc. 1993 Jan-Feb;7(1):26-8. 22. Phillips EH, Carroll BJ, Fallas MJ. Laparoscopic preperitoneal inguinal hérnia repair without peritoneal incision. Technique and early clinical results. Surg Endosc. 1993 May-Jun;7(3):159-62. 23. Arregui ME, Navarrete J, Davis CJ, Castro D, Nagan RF. Laparoscopic inguinal herniorrhaphy. Techniques and controversies. Surg Clin North Am. 1993 Jun;73(3):513-27. 24. Roll S, Campos FG, Szego T. Herniorrafia inguinal por via laparoscópica. In: Creuz O, editor. Cirurgia vídeo-Endoscópica. Rio de Janeiro: Revinter; 1993. p. 303-10. 25. Bittner R, Arregui ME, Bisgaard T, Dudai M, Ferzli GS, Fitzgibbons RJ, et al. Guidelines for laparoscopic (TAPP) and endoscopic (TEP) treatment of inguinal herniaInternational Endohernia Soci- AWRJ - Abdominal Wall Repair Journal 23 Artigo Original Cavazzola et al. ety (IEHS). Surg Endosc. 2011 Sep;25(9):2773-843. 26. Meyer A, Blanc P, Balique JG, Kitamura M, Juan RT, Delacoste F, Atger J. Laparoscopic totally extraperitoneal inguinal hernia repair: twenty-seven serious complications after 4565 consecutive operations. Rev Col Bras Cir. 2013 Jan-Feb;40(1):32-6. 27. Dulucq JL, Wintringer P, Mahajna A. Laparoscopic totally extraperitoneal inguinal hernia repair: lessons learned from 3,100 hernia repairs over 15 years. Surg Endosc. 2009 Mar;23(3):482-6. 28. Katkhouda N, Campos GM, Mavor E, Trussler A, Khalil M, Stoppa R. Laparoscopic extraperitoneal inguinal hernia repair. A safe approach based on the understanding of rectus sheath anatomy. Surg Endosc. 1999 Dec;13(12):1243-6. 29. Carvalho GL, Loureiro MP, Bonin EA, Claus CP, Silva FW, Cury AM, Fernandes FA Jr. Minilaparoscopic technique for inguinal hernia repair combining transabdominal pre-peritoneal and totally extraperitoneal approaches. JSLS. 2012 Oct-Dec;16(4):569-75. 30. Newell RL. Anatomical Spaces. In: Farinon AM, Rulli F, editors. Endoscopic Surgery of the potential anatomical spaces. Dordrecht: Springer; 2005. p. 1-8. 31. Farinon F. Surgical endoscopic Access to potential anatomical spaces: a multidisciplinary issue. In: Farinon AM, Rulli F, editors. Endoscopic Surgery of the potential anatomical spaces. Dordrecht: Springer; 2005. p. 35-8. 32. Newell RL. Anatomical spaces: a review. Clin Anat. 1999;12(1):66-9. 33. Gill IS, Munch LC, Lucas BA, Das S. Initial experience with retroperitoneoscopic nephroureterectomy: use of a double-balloon technique. Urology. 1995 Nov;46(5):747-50. 34. Gill IS, Clayman RV, Albala DM, Aso Y, Chiu AW, Das S, Donovan JF, et al.Retroperitoneal and pelvic extraperitoneal laparoscopy: an international perspective. Urology. 1998 Oct;52(4):56671. 35. Micali F, Forte F. Video-assisted approach to the retroperitoneum. In: Farinon AM, Rulli F, editors. Endoscopic Surgery of the potential anatomical spaces. Dordrecht: Springer; 2005. p. 83-98. 36. Lange JF, Rooijens PP, Koppert S, Kleinrensink GJ. The preperitoneal tissue dilemma in totally extraperitoneal (TEP) laparoscopic hernia repair: an anatomo-surgical study. Surg Endosc. 2002 Jun;16(6):927-30. 37. Arregui, ME, Castro D, Nagan RF. Anatomy of the peritoneum, preperitoneal fascia and posterior lamina of the transversalis fascia in the inguinal área. In: Arregui ME, Nagan RF, editors. Inguinal Hernia. Advances or controversies. Nova York: Radcliffe Medical Press; 1994. p. 23-34. 38. Oliveira VFO, Cavazzola LTC, Ambrosini L, Rocha HP, Chedid MF. Região Retroperitoneal. In: Oliveira VFO, Chedid MF, Girardi FM, editores. Anatomia Clínica e Cirúrgica do Abdome. Porto Alegre: Editora da Universidade Federal do Rio Grande do Sul; 2005.p. 337-345 39. Moreno-Egea A, Martínez JA, Girela E, de la Calle MC, Albasini JL. Anatomicaland surgical study of totally extraperitoneal laparoscopic hernioplasty. Med Sci Monit. 2005 Mar;11(3):CR127-31. 40. Mirilas P, Colborn GL, McClusky DA 3rd, Skandalakis LJ, Skandalakis PN Skandalakis JE. The history of anatomy and surgery of the preperitoneal space. Arch Surg. 2005 Jan;140(1):90-4. 41. Fölscher DJ, Leroy J, Jamali FR, Marescaux J: Totally extrafascial endoscopic preperitoneal hernia repair: a merger of anatomy and surgery. The exact description to endoscopically dissect the spermatic fascia. Hernia, 2000 dec; 4 (4): 223-27. 42. Gaur. A simple device for making a glove balloon for retroperitoneal dissection. Minim Invasive Ther Allied Technol. 2003 Mar;12(1):65-8. 24 43. Hald T, Rasmussen F. Extraperitoneal pelvioscopy: a new aid in staging of lower urinary tract tumors. A preliminary report. J Urol. 1980 Aug;124(2):245-8. 44. Clayman RV, Kavoussi LR, Soper NJ, Dierks SM, Meretyk S, Darcy MD, et al. Laparoscopic nephrectomy: initial case report.J Urol. 1991 Aug;146(2):278-82. 45. Clayman RV, Kavoussi LR, McDougall EM, Soper NJ, Figenshau RS, Chandhoke PS, Albala DM. Laparoscopic nephrectomy: a review of 16 cases. Surg Laparosc Endosc. 1992 Mar;2(1):29-34. 46. Gaur DD, Rathi SS, Ravandale AV, Gopichand M. A single-centre experience of retroperitoneoscopy using the balloon technique. BJU Int. 2001 May;87(7):602-6. 47. Gaur DD. Laparoscopic operative retroperitoneoscopy: use of a new device. J Urol. 1992 Oct;148(4):1137-9. 48. Ferzli G, Kiel T. Evolving techniques in endoscopic extraperitoneal herniorrhaphy. Surg Endosc. 1995 Aug;9(8):928-30. 49. Sayad P, Ferzli G. The extraperitoneal approach and its utility. Surg Endosc. 1999 Nov;13(11):1168-9. 50. Gaur DD. Retroperitoneal Access Techniques. In: Gaur DD, editor. Retroperitoneal laparoscopic urology. Nova Deli, IND: Oxford University Press; 1997. p. 31-47. 51. Riek S, Bachmann KH, Gaiselmann T, inventores; Penetration instrument. United States patent US 5271380. 1993 Dez 21. 52. Kaali SG, inventor; Visually directed trocar for laparoscopic surgical procedures and method of using same. United States patent US 5334150. 1994 Aug 2. 53. Tai HC, Lai MK, Chueh SC, Chen SC, Hsieh MH, Yu HJ. An alternative access technique under direct vision for preperitoneoscopic pelvic surgery: easier for the beginners. Ann Surg Oncol. 2008 Sep;15(9):2589-93. 54. Daes J. Reparo laparoscópico de la hernia inguinal : presentación de la técnica totalmente extraperitoneal con vista extendida. Rev. Colomb. Cir. 2011;26(2):89-92. 55. LeBlanc KA , Allain Jr BW, Streetman WC. Laparoscopic Inguinal Hernia Repair In: Kingsnorth, NA, LeBlanc KA, editors. Management of Abdominal Hernias. 4th ed. Londres: Springer; 2013. p. 271-283 56. Gaur DD. Retroperitoneal laparoscopic urology. Nova Deli, IND: Oxford University Press; 1997. p. 24-30. 57. Gaur DD. Retroperitoneal laparoscopic urology. Nova Deli, IND: Oxford University Press; 1997. p. 56-60. 58. Fogarty TJ, Scott JS, Torre Rde L, Denes BS, Hermann GD. Selected applications of balloon dissection. Surg Technol Int. 1994;3:45-52. 59. Kieturakis MJ, Nguyen DT, Vargas H, Fogarty TJ, Klein SR. Balloon dissection facilitated laparoscopic extraperitoneal hernioplasty. Am J Surg. 1994 Dec;168(6):603-7; discussion 607-8. 60. Gaur DD. Retroperitoneal laparoscopic urology. Nova Deli, IND: Oxford University Press; 1997. p. 48-55 61. Bringman S, Ek A, Haglind E, Heikkinen T, Kald A, Kylberg F, et al. Is a dissection balloon beneficial in totally extraperitoneal endoscopic hernioplasty (TEP)? A randomized prospective multicenter study. Surg Endosc. 2001 Mar;15(3):266-70. 62. Ferzli G, Kiel T. Evolving techniques in endoscopic extraperitoneal herniorrhaphy. Surg Endosc. 1995 Aug;9(8):928-30. 63. Dulucq JL.Treatment of inguinal hernia by insertion of a subperitoneal patch under pre-peritoneoscopy. Chirurgie. 1992;118(12):83-5. 64.Sherson N. An aid to laparoscopic hernioplasty--balloon dissection. Med J Aust. 1993 Feb 1;158(3):213-4. 65. Cable RL, Gilling PJ, Jones WO. Laparoscopic extraperitoneal inguinal hérnia repair using a balloon dissection technique. Aust N AWRJ - Abdominal Wall Repair Journal v. 3 n. 8 Extraperitoneal Space: Right Access for Endoscopic Hérnia Repair? Abril 2015 / Julho 2015 Z J Surg. 1994 Jun;64(6):431-3. 66. Wishart GC, Wright D, O’Dwyer PJ. Use of a Foley catheter to dissect the preperitoneal space for extraperitoneal endoscopic hernia repair. J Laparoendosc Surg. 1995 Feb;5(1):27-9. 67. Ullah MZ, Bhargava A, Jamal-Hanjani M, Jacob S. Totally extraperitoneal repair of inguinal hernia by a glove-balloon: technical innovation. Surgeon. 2007 Aug;5(4):245-7. 68. Golash V. A handy balloon for total extraperitoneal repair of inguinal hernia. Journal of minimal access surgery. 2008 Jan;4(2):54-6. 69. Misra MC, Kumar S, Bansal VK. Total extraperitoneal (TEP) mesh repair of inguinal hernia in the developing world: comparison of low-cost indigenous balloon dissection versus direct telescopic dissection: a prospective randomized controlled study. Surg Endosc. 2008 Sep;22(9):1947-58. 70. Kumar S. A new balloon dissector for totally extraperitoneal hernia repair. Journal of minimal access surgery. 2009 Jan;5(1):22-4. 71. Gaur DD, Agarwal DK, Purohit KC, Darshane AS. Laparoscopic condom dissection: new technique of retroperitoneoscopy. J Endourol. 1994 Apr;8(2):149-51. 72. Gaur DD. Retroperitoneal laparoscopic urology. Nova Deli, IND: Oxford University Press; 1997. p. 10-17. 73. Kieturakis MJ, Nguyen DT, Vargas H, Fogarty TJ, Klein SR. Balloon dissection facilitated laparoscopic extraperitoneal hernioplasty. Am J Surg. 1994 Dec;168(6):603-7; discussion 607-8. 74. Moll FH, Gresl Jr C, Chin A, Hopper PK inventores; Origin Medsystems Inc., cessionário. Retraction Methods using endoscopic inflatable retraction devices. United States patent US 5309896. 1994 May 10. 75. Moll FH, Chin AK. Balloon Assisted Extraperitoneal Laparoscopic Approaches. J Am Assoc Gynecol Laparosc. 1994 Aug;1(4, Part 2):S23. 76. Hirsch IH, Moreno JG, Lotfi MA, Gomella LG. Controlled balloon dilatation of the extraperitoneal space for laparoscopic urologic surgery. J Laparoendosc Surg. 1994 Aug;4(4):247-51. 77. Sierocuk TJ, Garrison WA, Michetti AR, inventores; Ethicon Endo Surgery Inc., cessionário. Surgical Dissector. United States patent US 5607441. 1997 Mar 4. 78. Echevery JM, Fernandez LM, Jervis JE, Robinson JC, Tanaka S, Voss LK, inventors; General Surgical Innovations Inc., assignee. Apparatus and method for developing na anatomic space for laparoscopic procedures. United States patent US 6015421. 2000 Jan 18. 79. Peartree KA, Palermo TJ, Tanaka S, Powell FT, inventors; General Surgical Innovations Inc., assignee. Balloon dissector appara- v. 3 n. 8 tus. United States patent US 6592602. 2003 Jul 15. 80. Criscuolo C, Creston B, Aranyi E, Geiste R, inventors; Tyco Healthcare Group Inc., assignee. Balloon dissector with cannula. United States patent US 7300448. 2007 Nov 27. 81. Heikkinen TJ, Haukipuro K, Koivukangas P, Hulkko A. A prospective randomized outcome and cost comparison of totally extraperitoneal endoscopic hernioplasty versus Lichtenstein hernia operation among employed patients. Surg Laparosc Endosc. 1998 Oct;8(5):338-44. 82. Wellwood J, Sculpher MJ, Stoker D, Nicholls GJ, Geddes C, Whitehead A, Singh R, Spiegelhalter D. Randomised controlled trial of laparoscopic versus open mesh repair for inguinal hernia: outcome and cost. BMJ. 1998 Jul 11;317(7151):103-10. Erratum in: BMJ 1998 Sep 5;317(7159):631. 83. Ferzli G, Sayad P, Huie F, Hallak A, Usal H. Endoscopic extraperitoneal herniorrhaphy. A 5-year experience. Surg Endosc. 1998 Nov;12(11):1311-3. 84. Spitz JD, Arregui ME. Sutureless laparoscopic extraperitoneal inguinal herniorrhaphy using reusable instruments: two hundred three repairs without recurrence. Surg Laparosc Endosc Percutan Tech. 2000 Feb;10(1):24-9. 85. Schurz JW, Arregui ME, Hammond JC. Open vs laparoscopic hernia repair. Analysis of costs, charges, and outcomes. Surg Endosc. 1995 Dec;9(12):1311-7. 86. Farinas LP, Griffen FD. Cost containment and totally extraperitoneal laparoscopic herniorrhaphy. Surg Endosc. 2000 Jan;14(1):3740. 87. Bringman S, Ek A, Haglind E, Heikkinen TJ, Kald A, Kylberg F, et al.Is a dissection balloon beneficial in bilateral, totally extraperitoneal,endoscopic hernioplasty? A randomized, prospective, multicenter study. Surg Laparosc Endosc Percutan Tech. 2001 Oct;11(5):322-6. 88. Basu S, Chandran S, Somers SS, Toh SK. Cost-effective laparoscopic TEP inguinal hernia repair: the Portsmouth technique. Hernia. 2005 Dec;9(4):363-7. 89. Kuthe A. Invited comment to the paper of S. Basu: Cost-effective laparoscopic TEP inguinal hernia repair: the Portsmouth Technique. Hernia. 2006 Mar;10(1):102. 90. Loureiro MP. hernioplastia endoscópica extraperitoneal: custos, alternativas e benefícios. Rev bras videocir 2006;4(3):135-138. 91. Chiang DT-W, Bohmer R. Cutting the cost: Laparoscopic inguinal hernia repair by totally extraperitoneal approach without disposable instruments. Surg PractInternet. 2006 Nov ;10(4):154-8. AWRJ - Abdominal Wall Repair Journal 25 Relato de Caso Case Report 26 AWRJ - Abdominal Wall Repair Journal v. 3 n. 8 GARANGEOT’S HERNIA: A CASE REPORT Hérnia Garangeot’s: Relato de caso James Skinovsky1, Flávio Panegalli Filho2, Fernanda Keiko Tsumanuma3, Rômulo Augusto Andrade de Almeida4, Alinne Vandramin4 PhD – Chairman Surgery Department, Positivo University, Red Cross University Hospital – Curitiba-Brazil 2 MD – Surgery Staff – Red Cross University Hospital – Curitiba-Brazil 3 MD – Assistant Professor – Positivo University, Red Cross University Hospital – Curitiba-Brazil 4 Academic Medicine Course – Positivo University – Curitiba-Brazil 1 BACKGROUND Femoral hernias occur below the inguinal ligament when the abdominal contents passes through the inguinal canal1. In about 0.8-1% of femoral hernias, the appendix is included within the hernia sac2,3,4. The average age of presentation is 554. The presence of appendicitis is even more unusual1. This was first described by the French surgeon Rene Jacques Croissant de Garengeot in 17315.6. To date, few cases have been reported in the literature5. It affects more women than men at a ratio of 13:16. Many times diagnosis is incidental during hernia repair surgery7,8. Garengeot`s hernia can remain for years without presenting imprisonment or inflammatory symptoms. There is a report of a case where the patient remained with this type of hernia for 30 years until symptoms such as increasing the size and touch increased sensitivity appeared7. Among the reported symptoms, there is: local inflammatory signs, abdominal distension, nausea and vomiting, periumbilical pain, fever1,6,7. The abnormal anatomical position of the appendix in the pelvis and a large mobile cecum are factors attributed appendix entry into the inguinal canal6. In cases of appendicitis, confuse the diagnosis with femoral hernia incarcerated9. In addition, the presence of pus, from extra-hernia ruptured appendix, the hernia sac can also lead to similar symptoms9. One of the articles found reports a Richter hernia case associated with herniated Garengeot6. The gold standard for diagnosis is computed tomography, however, the use of ultrasound can also provide an accurate diagnosis, being cheap and affordable and without ionizing radiation1. MRI can also be used in cases where CT is contraindicated as in cases of allergy to contrast4. laparoscopy, and therapy can also be used as a diagnostic method10. v. 3 n. 8 It is important to know the anatomy of the femoral triangle to accurately diagnose this hernia on imaging studies. The triangle is formed medially by the adductor longus muscle, laterally by the sartorius and superiorly by the inguinal ligament, while the iliopsoas, adductor longus pectineus and form your floor. The femoral channel is the medial femoral vein. This channel is relatively narrow, which causes more chences to choke than in inguinal hernias. The goal of imaging is to find a dead end pipe in the right iliac fossa. The resonance characteristics suggesting a normal appendix is detecting a high signal on T2 within the lumen and the presence artifacts that show the presence of air in the Appendix. In case of appendicitis, an inflammatory fluid around the appendix appear in T2 hyper-radiation. Appendix size calculation can also help in the diagnosis of appendicitis. There is a need in contrast radiography examination4. Abdominal x-ray does not help in the diagnosis of hernia8. Its treatment is appendectomy and hernia repair, however, there isn’t a standard procedure because of its rarity7. Some authors showed that appendectomy via the hernia sac is appropriate, however, in cases of perforation and abscess formation, the transabdominal route is preferable11. It was suggested that in cases where no appendicitis, it is not necessary appendectomy3.12. Both open surgery and laparoscopic the via13 can be used. Retrograde appendectomy is an option in cases of appendicitis, in order to prevent peritoneal contamination12. The hernia repair is preferably to place a mesh11 except in cases of infection, where the screen contamination of chance makes it preferable to use the Cooper’s ligament for herniária correction7. The most common complication of Garengeot De hernia repair is a wound infection at a rate reaching 29%. Some cases of necrotizing fasciitis and even death have been reported, probably related to delay in diagnosis and older age of patients8. AWRJ - Abdominal Wall Repair Journal 27 Artigo Original Skinovsky et al. CASE REPORT A 62-year-old male paciente was admitted in the emergency room with pain in the right inguinal region in the last 3 days and progressive worsening. Denied bowel habit changes, denied nausea and vomiting, fever or any other symptoms. The patient reported that he had never noticed any changes in the groin before the onset of pain. He denied any co-morbidity in treatment or previous surgeries. On physical examination, it was noticed not reducible bulging in the inguinal region, with intense pain on palpation, but no local inflammatory signs without pain and signs of peritoneal irritation. Laboratory tests were performed, the result of which showed no changes: blood count, coagulation tests, renal function, blood glucose and normal electrolytes. It was chosen by the non-operation of imaging due to intense pain of the patient and clinical diagnosis already performed examining the patient. It was performed a right inguinotomy of about 10 to 12 centimeters, with the patient under general anesthesia, but anesthetic block of ilioinguinal nerve. When performing the opening of the abdominal wall plans and dissection of the area was observable the cecal apêndix with no inflammation insinuating themselves imprisoned by the inguinal canal, indirectly, requiring local dissection with partial opening of the channel to release the appendix and part of cecum (Figure 1). Appendectomy via sac and reduction of remaining content, correction of inguinal canal with 3.0 Prolene yarn was made. The correction occurred by technique without tension, using heavyweight polypropylene mesh, attached to the cooper ligament inferiorly and Figure 1 – Hernia content after release of the inguinal canal – Garangeot’s Hernia superiorly to the joint area with nonabsorbable sutures. The patient had good postoperative evolution, reporting only little local nuisance, which resolved with the use of simple analgesics. The patient was discharged on postoperative second and returned with 1 week, 3 weeks, 1 month and 6 months postoperatively, without evidence of any surgical complication or hérnia recurrence. DISCUSSION The history and physical examination of the patient have proven completely sufficient for the diagnosis of incarcerated hernia, but the diagnosis of Garangeot Hernia only appeared in the perioperative period. This diagnosis could have been made preoperatively by a CT scan, but it was decided to perform surgery without it because the intensity of the patient’s pain. Because of the rarity of cases like this there is not an established surgical technique in the literature. In this case appendectomy was performed via hernia sac, but according to the literature presented in the introduction, there would be conversion to transabdominal technique if there were cecal appendix with signs of inflammation or other difficulties. The hernia defect repair was carried out without tension polypropylene mesh, which determines a lower rate of post-operative complications and especially recurrence. FINAL CONSIDERATIONS The case presented is shown of great importance to reporting because of their rarity, not only by the presence appendix of the inguinal canal, but also because it occurred in a man (more commonly occurs in women). Compared to cases such as this must be done a surgical precise, excluding the possibility of bottlenecks or acute appendicitis inside the hernia and the treatment should be conducted according to the case, where possible without performing the tension-free correction of the hernia as recommended nowadays REFERENCES 1. Shah A, Janardhan HS. De Garengeot hernia: a case report and review of literature. Indian J Surg. 2013 Jun; 75(Suppl 1): 439–441. 2. Ahmed, K. et al. Appendicitis in De Garengeot’s hernia presenting as a nontender inguinal mass: case report and review of the literature. Case Rep Surg. 2014; 2014: p.1-3. . 3. Brown N, Moesbergen T, Steinke K. The French and their her- 28 AWRJ - Abdominal Wall Repair Journal v. 3 n. 8 Garangeot’s Hernia: A Case Report Abril 2015 / Julho 2015 nias: prospective radiological differentiation of the Garengeot from other groin hernias. J Radiol Case Rep. 2013 Apr; 7(4):16-21. 4. Halpenny D, Barrett R, O’Callaghan K, Eltayeb O, Torreggiani WC. The MRI findings of a de Garengeot hernia. Br J Radiol. 2012 Mar;85(1011):e59-61. 5. Talini C, Oliveira LO, Araújo AC, Netto FA, Westphalen AP. De Garengeot hernia: case report and review. Int J Surg Case Rep. 2015;8C:35-7. 6. Le HD, Odom SR, Hsu A, Gupta A, Hauser CJ. A combined Richter’s and De Garengeot’s hernia. Int J Surg Case Rep. 2014; 5(10): 662–664. 7. Schäfer HM, Holzen U, Nebiker C. Swelling of the right thigh for over 30 years: the rare finding of a De Garengeot hernia. Int J Surg Case Rep. 2014;5(12):1120-2. 8. Piperos T, Kalles V, Al Ahwal Y, Konstantinou E, Skarpas G, Mariolis-Sapsakos T. Clinical significance of de Garengeot’s hernia: A case of acute appendicitis and review of the literature. International Journal of Surgery Case Reports. 2012;3(3):116-117. v. 3 n. 8 doi:10.1016/j.ijscr.2011.12.003. 9. Hsiao T, Chou, Y. Appendiceal pus in hernia sac simulating strangulated femoral hernia: a case report. Int J Gen Med. 2011 Mar 23;4:235-7. 10. Thomas B, Thomas M, McVay B, Chivate J. De Garengeot Hernia. JSLS : Journal of the Society of Laparoendoscopic Surgeons. 2009;13(3):455-457. 11. Ebisawa K, Yamazaki S, Kimura Y, et al. Acute Appendicitis in an Incarcerated Femoral Hernia: A Case of De Garengeot Hernia. Case Reports in Gastroenterology. 2009;3(3):313-317. 12. Hussain A, Slesser AAP, Monib S, Maalo J, Soskin M, Arbuckle J. A De Garengeot Hernia masquerading as a strangulated femoral hernia. International Journal of Surgery Case Reports. 2014;5(10):656-658. 13. Comman A, Gaetzschmann P, Hanner T, Behrend M. DeGarengeot Hernia: Transabdominal Preperitoneal Hernia Repair and Appendectomy. JSLS : Journal of the Society of Laparoendoscopic Surgeons. 2007;11(4):496-501. AWRJ - Abdominal Wall Repair Journal 29 Anexo High Tech Surgery Appendix High Tech Surgery 30 AWRJ - Abdominal Wall Repair Journal v. 3 n. 8 INCIDENCE OF GALLBLADDER STONES AFTER BARIATRIC SURGERY Incidência de cálculos da Vesícula Biliar após Cirurgia Bariátrica Ibarra Eliana, Pascowsky Maria, Souza Juan Manuel, Vega Emiliano, Pilar Quevedo, Marianela Aguirre Ackerman, Guillermo Duza MAAC, Edgardo Serra MAAC, Mariano Palermo MD PhD MAAC FACS Bariatric and Metabolic Surgery Division. Centro Cien-DIAGNOMED Afiliated Institution to the University of Buenos Aires ABSTRACT Objectives: To compare the incidence of gallstones formation post bariatric surgery according to techniques, Roux en Y Gastric bypass ans gastric sleeve. Material y methods: We made a literature search through Medline database of prospective and retrospective work type. The search criteria focused on obese patients referred for bariatric surgery that were included in treatment protocols using surgical techniques Roux en-Y gastric bypass and gastric sleeve, and monitoring plans designed to detect the development of gallblader disease. Results: During the follow up, 134 patients (37%) developed gallbladder disease after Roux en Y gastric bypass. In detail, 66 (49,25%) cases of cholelithiasis occurred in the first year post surgery, 38 (57,5%) of which were developed specifically in the first 6 months; 23 patients ( 17.16% ) during the second year of follow-up, while only 5 patients ( 3.73 % ) made it beyond the second year.On the other hand, during the follow-up 21 patients (10%) developed gallbladder disease after gastric sleeve. In this case, only one of the works included in this revision clarifies the periods development of disease patients, specifying a time interval of 18.4 +/- 10.7 months. Conclusion: Our results are showing that the incidence of cholelithiasis is higher after Roux en Y gastric bypass than after gastric sleeve. We understand that this result is conditioned because of the poor number of patients that underwent gastric sleeve, and also because two of the works about gastric sleeve were aimed only to detect cases of symptomatic or complicated illness , leaving out the diagnosis of asymptomatic patients. So we could said that in reality, the incidence of galldblader diseade would be similar if we could compare all patients , both symptomatic and asymptomatic. All v. 3 n. 8 of the works make it clear that the only predictor of gallbladder disease post- bariatric surgery is the rapid weight loss , especially in the first six months, which is when most cases of stone disease develops. So, the choice of technique would not impact on the incidence of post bariatric gallbladder disease , although the small number of studies about gastric sleeve require new items to make a conclusion based on a more significant sample. Keywords: Gallbladder, Obesity, Bariatric Surgery. INTRODUCTION Morbid obesity is a chronic multifactorial disease associated with significant physical and psychological complications that contribute to worsen the quality of patients life and reduce their life expectancy. The treatment of this disease with lifestyle modifications and drug, fails, in most cases, to loose sufficient weight to appropiate control of the comorbidities. So far, bariatric surgery is the only treatment that is able to reach these long-term expectations. Bariatric surgery is a therapeutic tool that requiring for indications an strict selection criteria that refer to the magnitude of obesity, the existence of complications and failure of conventional treatments previously applied . Obese patients becomes in candidates for bariatric surgery when they have a BMI ≥ 40 kg/m2 or ≥ 35 kg/m2 with 2 or more comorbidities that requiring weight loss treatment, including Miellitus Diabetes, arterial hypertension, dyslipidemia, heart coronary. The different surgical techniques can be classified into restrictive, malabsorptive and mixed. Within which, at present, the Gold Standard is the gastric bypass. In Latin America it reported that between 5 and 15 % AWRJ - Abdominal Wall Repair Journal 31 Anexo – High Tech Surgery Palermo et al. of people have gallstones, and there are populations and ethnic groups with the highest prevalence, such as Caucasian, Hispanic or Native Americans. Countries like the United States, Chile, Bolivia are among the highest number of people affected by this disease1. Following bariatric surgery, especially Roux-en-Y gastric bypass (RYGB), the frequency of gallstone formation increases as compared to the normal population due to rapid weight loss3,4. Hepatic supersaturation of bile with cholesterol, gallbladder stasis, and increased concentration of mucin within bile are possible causes5 The management of gallstone disease in these patients is still controversial. Protocols coexist of conventional prophylactic surgery (cholecystectomy simultaneously with gastric bypass to all patients, whether or not gallstones), elective (cholecystectomy simultaneously with gastric bypass to asymptomatic carriers of gallstones) and conventional (cholecystectomy only in the presence of gallstones and symptoms). MATERIALS AND METHODS We made a literature search through Medline database of prospective and retrospective work type. The search criteria focused on obese patients referred for bariatric surgery that were included in treatment protocols using surgical techniques Roux en-Y gastric bypass and gastric sleeve, and monitoring plans designed to detect the development of gallblader disease. The terms used for the search were “morbid obesity” “gastric bypass” “sleeve gastrectomy” “gallbladder disease” “gallstones “ “ Roux en-Y gastric bypass “ “ prospective” “ cholectystectomy”. They were included for this review a total of 7 works, governed by the aforementioned criteria. Of these, 2 are such prospective jobs while the rest are retrospective. Only two of these items the study population is subject only to the surgical technique of gastric sleeve, and in turn these two items have the distinction of being evaluated in monitoring the development of symptomatic cholelithiasis and not of those who develop asymptomatically. Moreover of the 5 remaining works, 4 refer to the use of gastric bypass with Roux-Y reconstruction and the only remaining, meanwhile, compared both techniques. In all the items patients were included in protocols for monitoring including a preoperative abdominal ultrasound to rule out pre vesicular disease. Thus, were excluded from the final sample all those patients with previous cholecystectomy, gallstones preoperative 32 including both the finding of gallstones and biliary sludge, and those patients that could not be followed strictly. Those in which vesicular disease identified preoperatively underwent concomitant cholecystectomy with bariatric surgery. The post- surgical follow-up of all patients was performed at diferents periods of time at, between 6 months and 2 years. This included clinical evaluation (weight, BMI, percentage calculation weight loss, development of symptoms compatible with vesicular disease) and laboratory analysis, fundamentally, total cholesterol, and triglyceride fractions. We had a sample of 845 patients, of which 536 (63.4%) underwent Roux-Y gastric bypass, while the remaining 309 (36.5%) underwent gastric sleeve. From 536 patients undergoing Roux-Y-gastric bypas, 176 (32.8%) were excluded. In detail exclusions were due to previous cholecystectomy in 78 patients (13.61%); gallbladder disease preoperatively detected in 89 patients (16.6%); lost to follow up in 9 (1.67%) and doubtful ultrasound 5 (0.93%) . Having been excluded those already named , a cohort of 360 (67.16%) patients without gallbladder disease patients was finally obtained. Moreover, of the 309 patients undergoing gastric sleeve , the excluded were 99 patients (32.03%). The reasons for these exclusions were prior cholecystectomy in 40 patients (12.94%) ; previous disease in 38 patients (12.29%) and lost to follow up in 21 patients (6.79%). Thus, we obtained a final sample of 210 patients (67,9%) without gallbladder disease. RESULTS From data collected from the different items we had a sample of patients without gallbladder disease and strictly monitored of 360 patients who underwent Roux-en Y- gastric bypass was obtained , and 210 patients underwent gastric sleeve surgery During the follow up, 134 patients (37%) developed gallbladder disease after Roux en Y gastric bypass. In detail, 66 (49,25%) cases of cholelithiasis occurred in the first year post surgery, 38 (57,5%) of which were developed specifically in the first 6 months; 23 patients (17.16%) during the second year of follow-up, while only 5 patients (3.73 %) made it beyond the second year. On the other hand, during the follow-up 21 patients (10%) developed gallbladder disease after gastric sleeve. In this case, only one of the works included in this AWRJ - Abdominal Wall Repair Journal v. 3 n. 8 Incidence of Gallbladder Stones after Bariatric Surgery Abril 2015 / Julho 2015 revision clarifies the periods development of disease patients, specifying a time interval of 18.4 +/- 10.7 months. DISCUSSION While in this review, are presents results that include two techniques of bariatric surgery, it should be noted that while the literature that include the cases treated with the technique of Bypass is abundant, the available regarding the incidence of gallstones post- Manga gastric is scarce. This difference is explained by the BY PASS is generally the most used technique. Compared with the general population, obesity is associated with high serum cholesterol levels, determining a higher incidence of lithiasis, which further increases in the population of patients undergoing different techniques of bariatric surgery. The latter is linked to several factors, including the severe weight loss (especially in the first six months post surgery), which in turn favors a significant mobilization of cholesterol from adipose tissue stores and lower production of bile salts and phospholipids into the gallbladder lumen. Furthermore, after bariatric surgery, the motility vesicular decreased, and an increase in mucin secretion to the bladder favoring that nucleation occurs .This predominant component of cholesterol on phospholipids and bile salts in bile promotes the formation of gallstones in post-bariatric patients. Other factors stimulated the formation of gallstones post-surgery, as the decrease in motility by altering the vagal nerve derived from the surgical process are present in some cases but are not constant in the different series. However, rapid weight loss (more than 25% of initial weight in 6 months), is the only predictor of vesicular disease present in all the series. Adding the total of the studies analyzed, the sample of patients undergoing bariatric surgery free of vesicular disease reached 494 cases, of which 360 correspond to surgical technique of Gastric Bypass and 210 to Gastric Sleeve. It should be noted that all patients treated with the latter technique, only in 43 patients the follow up post-surgical included clinical features and ultrasound, while the remaining 167 only the appearance of symptoms was evaluated, both gallstones and complicated stones With respect to patients treated with Gastric Bypass, of 360 undergoing this technique, 134 have developed vesicular disease, that constitutes 37%. This percenv. 3 n. 8 tage is in line with others previous works, where they obtained values of between 25% and 50 % : Amaral and Thompson (28%), Schmidt et al. (40%), Shiffman et al. (47%) , Surgeman (32%). Regarding the series of cases treated with the technique of Sleeve Gastrectomy, if we consider the one of Coupaye et. Al, which is the only one that have the strictly follow-up raised in this review, 12 of the 43 cases developed vesicular disease, proven by clinical signs and/or data obtained in the post-surgery scans. This represents a 27.9% of vesicular disease after Sleeve Gastrectomy, with a value that is in tune with Gastric Bypass treated series. This value drops significantly when we include the other two sets of Sleeve Gastrectomy analyzed, but this is based that in these work were aimed only to detect cases of symptomatic or complicated illness, leaving out the diagnosis of asymptomatic patients detected by ultrasound, which are the most cases of vesicular disease post- surgery. CONCLUSION Our results are showing that the incidence of cholelithiasis is higher after Roux en Y gastric bypass than after gastric sleeve. We understand that this result is conditioned because of the poor number of patients that underwent gastric sleeve, and also because two of the works about gastric sleeve were aimed only to detect cases of symptomatic or complicated illness, leaving out the diagnosis of symptomatic patients. So we could said that in reality, the incidence of galldblader diseade would be similar if we could compare all patients, both symptomatic and asymptomatic. On the other hand, all of the works make it clear that the only predictor of gallbladder disease post-bariatric surgery is the rapid weight loss, especially in the first six months, which is when most cases of stone disease develops. So, the choice of technique would not impact on the incidence of post bariatric gallbladder disease, although the small number of studies about gastric sleeve require new items to make a conclusion based on a more significant sample. REFERENCES 1. Li VK, Pulido N, Martinez-Suartez P, Fajnwaks P, Jin HY, Szomstein S, Rosenthal RJ. Symptomatic gallstones after sleeve gastrectomy. Surg Endosc. 2009 Nov;23(11):2488-92. AWRJ - Abdominal Wall Repair Journal 33 Anexo – High Tech Surgery Palermo et al. 2. Taha MIA; Freitas Jr WR; Puglia CR; Lacombe A; Malheiros CA. Fatores preditivos de colelitíase em obesos mórbidos após astroplastia em Y de Roux. Rev. Assoc. Med. Bras. Rev Assoc Med Bras 2006; 52(6): 430-4 3. Nagem RG, Lázaro AS, Oliveira RM, Morato VG. Gallstone-related complications after Roux-en-Y gastric bypass: a prospective study. Hepatobiliary Pancreat Dis Int. 2012 Dec 15;11(6):630-5 4. Teivelis MP, Faintuch J, Ishida R, Sakai P, Bresser A, Gama-Rodrigues J. Endoscopic and ultrasonographic evaluation before and after roux-en-y gastric bypass for morbid obesity. Arq Gastroenterol. 2007 Jan-Mar;44(1):8-13. 5. Karadeniz M, Görgün M, Cemal K. The evaluation of gallstone formation in patients undergoing Roux-en-Y gastric bypass due to 34 morbid obesity. Ulus Cerrahi Derg. 2014; 30(2): 76-79. 6. Sioka E, Zacharoulis D, Zachari E, Papamargaritis D, Pinaka O, Katsogridaki G, Tzovaras G. Complicated Gallstones after Laparoscopic Sleeve Gastrectomy. J Obes. 2014; 2014. 7. Moon RC, Teixeira AF, DuCoin C, Varnadore S, Jawad MA. Comparison of cholecystectomy cases after Roux-en-Y gastric bypass, sleeve gastrectomy, and gastric banding. Surg Obes Relat Dis. 2014 Jan-Feb;10(1):64-8. 8. Palermo M, Berkowski DE, Córdoba JP, Verde JM, Giménez ME. Prevalence of cholelithiasis in Buenos Aires, Argentina. Acta Gastroenterol Latinoam. 2013; 43(2):98-105. 9. Carbonell CLA, Prado YA, González TP, Ferro YP, Hernández ZH. Clinical and epidemiological diagnosis of bladder stone. Rev. Cienc Med Pinar Rio. 2012; 16(1): 200-214. AWRJ - Abdominal Wall Repair Journal v. 3 n. 8 EVENTOS TROMBOEMBÓLICOS EM PACIENTES SUBMETIDOS a CIRURGIA ABDOMINAL A CÉU ABERTO E CIRURGIAS ViDEOLAPAROSCÓPICAS Thromboembolic events in patients submitted open abdominal surgery and laparoscopic abdominal surgery James Skinovsky¹, Cristina Okamoto², Joseph Chenisz³, Daniel Lacerda³, Augusto Mozzaquatro³, Stephan Saab³, João Paulo Bacarin³ Doutor em Cirurgia. Professor Titular do Curso de Medicina da Universidade Positivo – Curitiba-PR. Coordenador das Residências Médicas em Cirurgia Geral e Cirurgia do Aparelho Digestivo do Hospital da Cruz Vermelha – Universidade Positivo – Curitiba-PR. 2 Doutora em Pediatria e Neonatologia, Especialização em Neonatologia na Universidade Estadual de Osaka-Japão, Professora da Graduação do Curso de Medicina da Universidade Positivo. 3 Doutorandos do quinto ano de Medicina da Universidade Positivo. 1 resumo Objetivo: Avaliar a presença de eventos tromboembólicos (tromboembolismo pulmonar e trombose venosa profunda) em pacientes submetidos a cirurgia abdominal a céu aberto, e cirurgias videolaparoscópicas, assim como o perfil epidemiológico desses pacientes. Método: Trata-se de uma análise observacional descritivo transversal, com coleta retrospectiva de pacientes submetidos a cirurgia abdominal a céu aberto e videolaparoscópica no período de 1 ano (01/01/2013 31/12/2013) no Hospital da Cruz Vermelha. A amostra é composta por 498 pacientes, sendo 242 cirurgias a céu aberto e 256 videolaparoscópicas. Foram pesquisados fatores clínicos, medicamentosos e cirúrgicos para eventos tromboembólicos em todos os pacientes incluídos no estudo através de critérios previamente estabelecidos. Resultados: De toda amostra, 7 (1,4%) dos pacientes apresentaram evento tromboembólico, sendo 4 trombose venosa profunda (TVP) e 4 tromboembolismo pulmonar (TEP). Assim, um mesmo paciente apresentou tanto TVP como TEP. Considerando apenas cirurgias a céu aberto o evento tromboembólico foi encontrado em 5 pacientes, sendo 2 casos de TVP e 3 TEP. A cirurgia de maior prevalência dentre as abertas foi a apendicectomia, seguida da laparotomia exploratória. A taxa de incidência para cirurgia aberta foi de 2,1%, com intervalo de confiança de 95%, de 0,3% a 3,9%. Em cirurgias videolaparoscópicas, foram enconv. 3 n. 8 trados 2 casos de TVP e 1 TEP. A cirurgia de maior prevalência entre as cirurgias por vídeo foi a colecistectomia, seguida da apendicectomia. A taxa de incidência foi de 0,8%, com intervalo de confiança de 95%, de 0% a 1,9%. Conclusão: O pós-operatório de cirurgia a céu aberto representa um maior risco de desenvolvimento para evento tromboembólico em relação ao pós-operatório de uma cirurgia videolaparascópica, isso se deve também aos fatores que motivaram a via a céu aberto serem determinantes de maior gravidade. Palavras-chave: Cirurgia laparoscópica. Cirurgia abdominal. Eventos tromboembólicos. Keywords: Laparoscopic surgery. Abdominal surgery. Thromboembolic events. INTRODUÇÃO Os eventos tromboembólicos (ETE) estão entre as principais causas de morbimortalidade no Brasil e no mundo. Estima-se que cerca de 50 a 100 mil pessoas morram anualmente nos EUA por algum tipo de ETE. Os ETE são caracterizados por Tromboembolismo Pulmonar (TEP) e Trombose Venosa Profunda (TVP). Diversos fatores de risco contribuem para essas entidades, dentre eles destacamos: estado de hipercoagulabilidade, estase venosa e lesão endotelial (Triade AWRJ - Abdominal Wall Repair Journal 35 Anexo – High Tech Surgery Skinovsky et al. de Virchow). Outros fatores de risco que devem ser destacados são: diminuição da atividade fibrinolítica, imobilização prolongada, pacientes submetidos a cirurgia, vítimas de trauma, presença de doenças malignas, idade avançada, falência cardíaca, episódio prévio de TVP, obesidade, varizes, doenças intestinais inflamatórias, sepse, infarto agudo do miocárdio e reposição hormonal1,2. O TEP isoladamente é responsável por cerca de 100 mil mortes por ano nos Estados Unidos e cerca de 10% deles ocorrem na primeira hora de sua evolução. Além disso, segundo o Centers for Disease Control and Prevention (CDC), o número de casos de Trombose Venosa Profunda gira em torno de 300.000 a 600.000 mil casos por ano. No Canadá, os números giram em torno de 45.000 casos por ano2. Nos países ocidentais, estima-se uma incidência de 48 casos de TVP e de 23 casos de TEP por ano para cada 100.000 habitantes. Embora sejam apresentações distintas da mesma doença, o risco de morte no TEP é de 5 a 17 vezes maior do que na TVP3. Um estudo realizado em Worcester, Massachusetts, verificou que mais da metade dos pacientes com a doença não recebeu profilaxia correta para tromboembolismos venosos3. Estima-se que 10% dos óbitos hospitalares ocorram devido a TEP, embora estudos de autópsia revelem o TEP como fator contribuinte ocorrendo em 29% a 37% dos casos de óbito4. Este trabalho revisou retrospectivamente os prontuários de 498 pacientes selecionados aleatoriamente, submetidos a cirurgia abdominal a céu aberto (242) e a cirurgias videolaparoscópicas (256), no serviço de cirurgia do Hospital da Cruz Vermelha no período de 01/01/2013 a 31/12/2013. Abordaremos a seguir os métodos de coleta dos dados com as variáveis analisadas. Posteriormente, com os resultados obtidos da pesquisa, demonstraremos a relação do tipo de cirurgia e pós-operatório com eventos tromboembólicos. MÉTODOs O estudo trata-se de uma análise observacional descritivo transversal, com coleta retrospectiva, tendo como população paciente submetido à cirurgia abdominal a céu aberto e por via videolaparoscópica. A pesquisa revisou prontuários no período de 01/01/2013 a 31/12/2013 no Hospital da Cruz Vermelha. O projeto foi conduzido com a aprovação do protoco- 36 lo pelo Comitê de Ética da Universidade Positivo, com a permissão da direção do hospital e sem a assinatura do termo de consentimento livre e esclarecido pelos pacientes. A amostra foi composta de 498 prontuários, sendo 242 de cirurgias abertas e outras 256 cirurgias videolaparoscópicas. Os critérios de inclusão foram: todos os pacientes submetidos a cirurgia abdominal aberta ou via videolaparoscópica durante todo o ano de 2013. Os critérios de exclusão foram: prontuários incompletos ou com informações inadequadas. Os dados coletados foram organizados em planilha Excel (Microsoft®) e a análise estatística foi feita com o auxílio do programa Prism 4.0. Os testes de Fisher e qui quadrado foram aplicados para o estudo de associação de variáveis nominais e os testes de Mann, Whitney e teste T para variáveis numéricas. A significância adotada foi de 5%. Foram pesquisados fatores clínicos, medicamentosos e cirúrgicos para ETE em todos os pacientes incluídos no estudo através de critérios previamente estabelecidos. RESULTADOS Foram coletados 498 prontuários de pacientes submetidos a cirurgia abdominal no ano de 2013. Desse número, 242 realizaram cirurgia a céu aberto e 256 realizaram cirurgia videolaparoscópica. Em relação ao gênero encontramos 278 (55,82%) pacientes do sexo feminino e 220 (44,18%) do sexo masculino. A média de idade encontrada foi 47,03 anos, sendo que os extremos de idade foram 14 e 89 anos. A cirurgia de maior prevalência foi a colecistectomia, com 37,34%, seguida da apendicectomia e da laparotomia exploratória, com respectivamente 22,48% e 11,04%. De toda amostra, 7 (1,4%) dos pacientes apresentaram evento tromboembólico, sendo 4 TVP e 4 TEP. Assim, um mesmo paciente apresentou tanto Trombose Venosa Profunda como Tromboembolismo Pulmonar. Do total da amostra, 84 (16,86%) pacientes apresentavam comorbidades, 210 (42,16%) doenças prévias e apenas 35 (7,02%) foram submetidos a algum tipo de profilaxia. Considerando apenas cirurgias abertas encontramos 111 (45,86%) pacientes do sexo feminino e 131 (54,14%) do sexo masculino. A cirurgia de maior prevalência foi a apendicectomia, seguida da laparotomia exploratória e da herniorrafia inguinal unilateral AWRJ - Abdominal Wall Repair Journal v. 3 n. 8 Eventos Tromboembólicos em Pacientes Submetidos à Cirurgia Abdominal a Céu Aberto e Cirurgias Vídeolaparoscópicas Abril 2015 / Julho 2015 ou bilateral com, respectivamente, 36,36%, 21,48% e 6,61%. O evento tromboembólico foi encontrado em 5 pacientes, sendo 2 casos de TVP e 3 TEP. Dentre todos os pacientes submetidos a cirurgia aberta, 42 (17,35%) apresentavam algum tipo de comorbidade, 105 (43,38) alguma doença prévia e apenas 17 (7,02%) foram submetidos a algum tipo de profilaxia. A taxa de incidência para cirurgia aberta foi de 2,1%, com intervalo de confiança de 95%, de 0,3% a 3,9%. Entre os casos de TEP, em pacientes submetidos a cirurgias a céu aberto, 1 (33,33%) era do sexo feminino e 2 (66,67%) eram do sexo masculino. Destes pacientes, 66,67% apresentavam algum tipo de comorbidade, nenhum apresentava doença prévia e apenas um foi submetido a um tipo de profilaxia. Os casos de TVP, em cirurgias a céu aberto, foram observados em apenas 2 pacientes, sendo estes do sexo feminino. Destes 2 pacientes, 1 apresentava algum tipo de comorbidade, todos tinham histórico de doença prévia e todos foram submetidos a profilaxia. Considerando, agora, apenas cirurgias videolaparoscópicas, encontramos 167 (65,23%) pacientes do sexo feminino e 89 do sexo masculino (34,77%). A cirurgia de maior prevalência foi a colecistectomia, seguida da apendicectomia e da gastrofundoplicatura a Nissen com, respectivamente, 67,57%, 8,98% e 5,85%. O evento tromboembólico foi encontrado em 2 pacientes sendo 2 casos de TVP e 1 de TEP. Assim, um mesmo paciente apresentou tanto Trombose Venosa Profunda como Tromboembolismo Pulmonar. Dentre todos os pacientes submetidos a cirurgia por vídeo, 39 (15,23%) apresentavam algum tipo de comorbidade, 115 (44,92%) alguma doença prévia e apenas 18 (7,03%) foram submetidos a algum tipo de profilaxia. A taxa de incidência foi de 0,8%, com intervalo de confiança de 95%, de 0% a 1,9%. Nesse trabalho, apenas um paciente submetido a cirurgia videolaparoscópica evoluiu para TEP. Esse paciente era do sexo feminino, não apresentava nenhuma comorbidade, possuía doença prévia e não recebeu nenhuma profilaxia. A TVP, na cirurgia videolaparoscópica, foi observada em 2 pacientes, estes do sexo feminino. Esses não apresentavam nenhuma comorbidade, um apresentava doença prévia e apenas um recebeu algum tipo de profilaxia. MÉTODOs É fato que quando discorremos sobre complicações no pós-operatório, os eventos tromboembólicos (TEP e v. 3 n. 8 TVP) representam um importante fator com relação à morbidade e mortalidade dos pacientes. Principalmente quando uma dessas complicações é o TEP, o qual é responsável por 100 mil mortes anos nos EUA. Além disso, 74% dos pacientes acometidos de Trombose Venosa Profunda não procuram auxílio médico, podendo assim elevar os índices já citados, pois um terço dos pacientes vítimas de TVP evoluem com TEP1,2,3. Os eventos tromboembólicos podem evoluir para óbito, acredita-se que a embolia pulmonar, por exemplo, seja a terceira causa de morte intra-hospitalar5. Ademais, segundo a União Europeia, no ano de 2007, o número de óbitos após um evento tromboembólico, foi em torno de 370 mil pacientes6. Diversos fatores de risco podem levar ao desenvolvimento de ETE. O ato cirúrgico por si só pode levar a um estado de hipercoagulabilidade, o qual culminará com trombose. A imobilidade no período pós-cirúrgico contribui de forma importante para tais patologias, sendo fatores de risco: doenças malignas, idade avançada, falência cardíaca, episódio prévio de TVP, imobilização prolongada, obesidade, varizes, doenças intestinais inflamatórias, sepses, infarto do miocárdio, puerpério, uso de hormônios femininos e viagens longas1,2,3. Outro estudo demostra que os 3 principais fatores de risco são: idade acima de 70 anos, imobilização recente, historia prévia de trombose venosa profunda ou embolia pulmonar e câncer7. No que se refere ao fato etário, diversos estudos comprovam que a incidência de eventos tromboembólicos aumenta exponencialmente com o aumento de idade, sendo que a incidência aumenta de forma dramática após os 60 anos. Estudo publicado na Cleveland Clinic, coloca como fator de risco idade maior que 75 anos. Outros estudos colocam 70 anos associado com aumento de incidência, mostrando a associação positiva entre aumento da idade com TEP e TVP5. Nossos índices com relação à idade demonstraram que dos sete pacientes acometidos de eventos tromboembólicos, dois estavam abaixo de 40 anos (28,58%), 2 entre 40 e 60 anos (28,58%), 3 estavam acima de 60 anos (42,84%)3,8. Considerando o gênero, nas mulheres, mesmo que o uso de contraceptivos e reposição hormonal predisponha a casos de eventos tromboembólicos, ocorre uma disparidade quanto à prevalência entre os sexos. Contudo, alguns acreditam não haver disparidade significativa3. Estudo publicado na Arch Surg em Dezembro de 2011 contou com a análise do prontuário de 2189 AWRJ - Abdominal Wall Repair Journal 37 Anexo – High Tech Surgery Skinovsky et al. pacientes submetidos a cirurgia em um hospital universitário. Destes, 1,6% desenvolveram evento tromboembólico no pós-operatório, sendo 22 homens e 13 mulheres9. Porém nossos resultados demonstraram o contrário, sendo que 5 dos 7 pacientes acometidos, eram mulheres, como pode ser verificado em diversos estudos mais atuais10. Das comorbidades encontradas nos pacientes que desenvolveram ETE7, 3 pacientes eram obesos, sendo que um deles também era tabagista. O tabagismo mostrou o aumento do risco relativo de trombose de 3,3 vezes para pacientes que fumavam mais de 35 cigarros/dia e de 1,9 vezes para os que fumavam entre 24 e 35 cigarros/dia, na Nurse Health Study, um estudo de coorte realizado entre 1976 e 199211. As doenças prévias encontradas nos pacientes que desenvolveram eventos tromboembólicos foram Câncer, Hipertensão Arterial Sistêmica, Dislipidemia, Diabetes Mellitus tipo 2, Insuficiência Cardíaca Congestiva, Bloqueio Atrioventricular e Trombose Venosa Profunda prévia. Na nossa amostra, dos 7 pacientes que apresentaram evento tromboembólico, 3 possuíam alguma doença prévia. Um deles apresentava concomitantemente Câncer de Sigmoide, Hipertensão Arterial Sistêmica, Insuficiência Cardíaca Congestiva e Bloqueio Atrioventricular. Outro paciente apresentava Câncer de Pâncreas, Hipertensão Arterial Sistêmica e Dislipidemia. Enquanto isso, o terceiro paciente apresentava obesidade, Hipertensão Arterial Sistêmica e TVP prévia. A incidência de evento tromboembólico é duas vezes maior em pacientes acometidos por Câncer. Em relação ao tipo de Câncer, o mais envolvido com essa complicação é o Carcinoma de Cabeça de Pâncreas, encontrado em um de nossos pacientes12. O tempo de internamento implica em aumento da incidência de TVP e TEP. Nesse estudo observou-se que o tempo de internamento dos pacientes com evento tromboembólico foi em média 12 dias, sendo que o maior tempo de internamento foi de 32 dias e o menor de 4 dias. Apesar de diversos protocolos para a prevenção de TVP já estarem disponíveis, encontramos um índice de profilaxia de apenas 7,02% no número global da amostra. Assim como neste trabalho, a literatura demonstra que a adoção de medidas profiláticas em hospitais gerais ainda é insatisfatória. Além disso, muitas vezes quando realizada é de maneira ineficaz13,14,15. O ponto principal desse estudo foi analisar o perfil dos pacientes que evoluíram com um evento tromboem- 38 bólico em relação a cirurgias abdominais via videolaparoscópicas e a céu aberto. Como demonstrado nos resultados, os pacientes submetidos a cirurgia aberta tiveram um maior índice de eventos tromboembólicos (2,06%) em relação a pacientes submetidos por cirurgia videolaparoscópica (0,78%). Notavelmente os pacientes submetidos a cirurgia aberta tinham mais comorbidades e fatores de risco, quando comparados a pacientes submetidos a cirurgia videolaparoscópica. Além disso, a profilaxia foi escassa em ambos os grupos, tanto cirurgias abertas quanto por vídeo. A profilaxia está muito relacionada à presença de eventos tromboembólicos em pacientes cirúrgicos segundo diversos estudos. Os números parecem aumentar quanto maior o índice de comorbidades e fatores de risco, tais como: Câncer, idade maior que 40 anos, Evento Tromboembólico prévio. Os números indicam que pacientes cirúrgicos sem profilaxia, com essas características tem o seguinte risco: 40 a 80% aumentado para TVP distal, 10 a 20% para TVP proximal, e 0,2 a 5% para embolia pulmonar fatal3,16. Considerando outro estudo específico de cirurgias abdominais abertas verificou-se que 4 de 83 (5%) pacientes tiveram algum evento tromboembólico, no caso a TVP, demonstrando um índice mais elevado do que o encontrado neste devido estudo12. Os índices apurados neste trabalho demonstram que apesar do ETE ser uma complicação não tão prevalente, é a terceira maior causa de morte intra-hospitalar, portanto, deve-se tomar as melhores medidas de prevenção com esses pacientes, dentre elas a profilaxia. Por fim, fica claro que pacientes com fatores de risco, maior tempo de internamento, doenças malignas, cirurgias de grande porte, principalmente por via céu aberto, têm mais chance de desenvolver uma TVP ou mesmo um TEP. CONCLUSÃO Após a análise do perfil epidemiológico de uma parcela de pacientes submetidos a cirurgia abdominal via videolaparascópica e a céu aberto, observou-se que, de fato, o pós-operatório de cirurgia a céu aberto representa um maior risco de desenvolvimento para evento tromboembólico em relação ao pós-operatório de uma cirurgia videolaparascópica. Considerando o perfil dos pacientes que foram submetidos a cirurgia a céu aberto, fica evidente que as doenças prévias que motivaram este procedimento detinham uma maior gravidade. Dessa forma, apresenta- AWRJ - Abdominal Wall Repair Journal v. 3 n. 8 Eventos Tromboembólicos em Pacientes Submetidos à Cirurgia Abdominal a Céu Aberto e Cirurgias Vídeolaparoscópicas Abril 2015 / Julho 2015 vam um maior tempo de internamento, corroborando para o desenvolvimento tromboembólico. REFERÊNCIAS 1. Orra HA. Trombose venosa profunda. Disponível em: <http:// www.clinicadrhussein.com.br/pdf/trombose.pdf>. Acesso em: 15/02/2015. 2. Engelhom AL, Garcia AC, et al.Profilaxia da trombose venosa profunda: estudo epidemiológico em um hospital escola. J Vasc Br 2002;1(2):97-102. 3. White RH. The epidemiology of venous thromboembolism. Circulation. 2003 Jun 17;107(23 Suppl 1):I4-8. 4. Spencer FA1, Emery C, Lessard D, Anderson F, Emani S, Aragam J, Becker RC, Goldberg RJ. The Worcester Venous Thromboembolism study: a population-based study of the clinical epidemiology of venous thromboembolism. J Gen Intern Med. 2006 Jul;21(7):722-7. 5. Ozaki A, Bartholomew JR. Venous Thromboembolism (Deep Venous Thrombosis & Pulmonary Embolism). Cleveland Clinic, December 2012. 6. Cohen AT, Agnelli G, et al. Venous thromboembolism (VTE) in Europe: the number of VTE events and associated morbidity and mortality. Thromb Haemost. 2007 Oct;98(4):756-64. 7. Motykie GD1, Caprini JA. Risk factor assessment in the management of patients with suspected deep venous thrombosis. Int Angiol. 2000 Mar;19(1):47-51. 8. Scottish Intercollegiate Guidelines Network (SIGN). Prevention and management of venous thromboembolism. A national clinical v. 3 n. 8 guideline. Edinburgh (Scotland): Scottish Intercollegiate Guidelines Network (SIGN); 2010 dec. 101 p. 9. Smith BR, Dinis S, Stamos M,Nguyen NT. Deep venous thrombosis after general surgical operations at a university hospital: two-year data from the ACS NSQIP. Arch Surg. 2011 Dec;146(12):1424-7. 10. Deitelzweig SB1, Johnson BH, Lin J, Schulman KL. Prevalence of clinical venous thromboembolism in the USA: current trends and future projections. Am J Hematol. 2011 Feb;86(2):217-20. 11. Goldhaber SZ, Grodstein F, Stampfer MJ et al. A prospective study of risk factors for pulmonary embolism in women. JAMA. 1997; 277:642(5). 12. Stein PD, Beemath A, Meyers FA, Skaf E, Sanchez J, Olson RE. Incidence of venous thromboembolism in patients hospitalized with cancer. Am J Med. 2006 Jan;119(1):60-8 13. Arnold DM, Kahn SR, Shrier I. Missed opportunities for prevention of venous thromboembolism: an evaluation of the use of thromboprophylaxis guidelines. Chest. 2001;120:1964-71. 14. Maffei FHA, Caiafa JS, Ramacciotti E, Castro. Normas de orientação clínica para prevenção, diagnóstico e tratamento da trombose venosa profunda (revisão 2005). Salvador: SBACV; 2005. Disponível em: http://www.sbacv-nac.org.br. Acesso em: 15/02/2015. 15. Caiafa JS, Bastos M. Programa de profilaxia do tromboembolismo venoso do Hospital Naval Marcílio Dias: um modelo de educação continuada. J Vasc Bras. 2002;1:103-12. 16. Sakon M, Maehara Y, Yoshikawa H, Akaza H. Incidence of venous thromboembolism following major abdominal surgery: a multi-center, prospective epidemiological study in Japan. J Thromb Haemost. 2006 Mar;4(3):581-6. 17. Muleledhu AL, Galukande M et al. Deep venous thrombosis after major abdominal surgery in a Ugandan hospital: a prospective study. Int J Emerg Med. 2013 Nov 28;6(1):43. AWRJ - Abdominal Wall Repair Journal 39 ARTIGO de revisão High Tech Surgery review Article High Tech Surgery 40 AWRJ - Abdominal Wall Repair Journal v. 3 n. 8 VIDEOCIRURGIA: DE ONDE VIEMOS E PARA ONDE VAMOS? Videosurgery: Where we come and where are we going? James Skinovsky1, Sérgio Roll2 1 Doutor em Cirurgia. Professor Titular do Curso de Medicina da Universidade Positivo – Curitiba-PR. Coordenador das Residências Médicas em Cirurgia Geral e Cirurgia do Aparelho Digestivo do Hospital da Cruz Vermelha – Universidade Positivo – Curitiba-PR. 2 Doutor em Cirurgia. Ex-Presidente da America’s Hernia Society. “Surgery is the first and the highest division of the healing art, pure in itself, perpetual in its applicability, a working product of heaven and sure of fame on earth” Sushruta (400 B.C.) HISTÓRICO Figura 1 – Em 1901, a cavidade abdominal de uma grávida foi examinada por Dimitri von Ott, que empregou um espéculo introduzido via colpotomia Fonte: http//eleboo.e-bookshelf.de/products/reading-epub/product A primeira tentativa de visualização de um órgão humano interno foi efetivada por Philipp Bozzini, em Frankfurt, no ano de 1806, quando inspecionou a uretra com uma cânula de duplo lúmen; um lúmen transmitia a luz emitida por uma vela e o outro servia para observação. A cirurgia laparoscópica foi inicialmente introduzida, no início do século passado, por Dimitri von Ott, Georg Kelling e Hans Christian Jacobaeus. Von Ott, ginecologista russo, inspecionou a cavidade abdominal de uma grávida em 1901, usando um espelho frontal como fonte luminosa e inserindo um espéculo vaginal através da parede abdominal, para observação interna (Figura 1). No mesmo ano Jacobaeus publicou seu primeiro relato da chamada “laparotoracoscopia” (Figura 2). Ainda em 1901 Kelling, cirurgião alemão de Dresden, descreveu a celioscopia, técnica pela qual enchia o abdômen de cão vivo com ar e inseria um cistoscópio de Nitze para inspecionar as vísceras (Figura 3). Nos anos seguintes vários autores na Europa e Estados Unidos realizaram laparoscopias para fins diagnósticos. Em 1910, Jacobaeus publicou estudo de laparoscopias realizadas em doentes, descrevendo lesões hepáticas e peritonite tuberculosa. Foi somente com a introdução dos sistemas ópticos e da iluminação por fibras de luz fria que o procedimento tornou-se mais popular, especialmente nos serviços ginecológicos1-10. Figura 2 – Hans Christian Jacobaeus, sueco, creditado como tendo realizado a primeira toracoscopia, em 1901, utilizando um cistoscópio Fonte: http://archsurg.jamanetwork.com/article.aspx?articleid=396242 Figura 3 – Georg Kelling, cirurgião alemão, geralmente creditado como tendo realizado a primeira laparoscopia, em 1901 Fonte: http//eleboo.e-bookshelf.de/products/ reading-epub/product v. 3 n. 8 AWRJ - Abdominal Wall Repair Journal 41 Skinovsky et al. Anexo – High Tech Surgery Em 1929, a introdução de lentes de visão oblíqua por Kalk tornou a laparoscopia amplamente aceita como meio diagnóstico. Em 1938, na Hungria, Janus Veress inventou uma agulha para induzir pneumotórax em tuberculosos, na área pré-antibióticos. Na década de 1950, na Inglaterra, Hopkins e Kapany introduziram a tecnologia das fibras ópticas na endoscopia, ampliando ainda mais o uso da laparoscopia diagnóstica. A laparoscopia no campo da cirurgia geral era somente utilizada, em geral, para diagnóstico de doenças hepáticas e trauma abdominal, até que Lukichev em 1983 e Muhe em 1985 divulgaram suas técnicas para a realização de colecistectomia laparoscópica em humanos. Suas técnicas, em certa forma rudimentares, não receberam atenção adequada na época. Kurt Semm, ginecologista, foi o primeiro a realizar apendicectomia laparoscópica em 1981(Figura 4). Este cirurgião e engenheiro alemão desenvolveu um aparelho de insuflação automática, para monitorar a pressão intra-abdominal e o fluxo de gás. Até hoje, diversos instrumentos e técnicas inventadas por Semm são amplamente utilizadas, como a eletrocoagulação, tesouras em gancho, morceladores, instrumental para irrigação e aspiração, aplicadores de clipes e outros11-20. em seguida realizou diversas destas cirurgias, porém o principal responsável pela divulgação meteórica do método nos Estados Unidos e mundo foi Jacques Perissat (Figura 6), de Bordeaux , que realizou a cirurgia poucos dias após os primeiros e que publicou a primeira grande série de casos desta cirurgia. Perissat confidenciou que tentou, em vão, espaço para demonstrar a técnica no Congresso SAGES americano em 1989. Conseguiu então um videocassete emprestado, acoplou-o a uma televisão e deixou o vídeo correndo em um dos corredores da conferência; logo dezenas de cirurgiões assistiam boquiabertos aquela espetacular demonstração. Figura 5 – Philippe Mouret – realizador da primeira colecistectomia videolaparoscópica Fonte: http://www.huliq.com/32578/ honda-foundation Figura 4 – Kurt Semm, cirurgião alemão pioneiro da videocirurgia Figura 6 – Professor Jacques Perissat (centro) – pioneiro da videocirurgia, com Professores James Skinovsky (à direita daquele) e Mauricio Chibata (à esquerda) Fonte: html http://www.repromedizin.de/dgrm-informationen/geschichte. Erich Muhe realizou colecistectomia laparoscópica em 1985, porém seu procedimento foi limitado ao acesso à cavidade peritoneal através de um trocarte de grande diâmetro. No ano de 1987, mais precisamente no dia 17 de março daquele ano, em Lyon na França, Philippe Mouret (Figura 5) realizou a primeira colecistectomia laparoscópica completada pelo método. Francois Dubois 42 Em poucas semanas a notícia de uma técnica que fez o aforisma “grandes cirurgiões, grandes incisões” cair inapelavelmente ao chão espalhou-se como rastilho de pólvora aos principais centros cirúrgicos do mundo. Logo formadores de opinião se deram conta que estavam diante de um método capaz de rivalizar com grandes revoluções médicas mundiais, como a antissepsia de Sammelweiss, a anestesia de Horace Wells e Tho- AWRJ - Abdominal Wall Repair Journal v. 3 n. 8 Videocirurgia: De onde viemos e para onde vamos? Abril 2015 / Julho 2015 mas Morton, a descoberta da microflora de Thomas Cock, os antibióticos de Fleming e outros. Em 4 de Outubro de 1990, a European Association for Endoscopic Surgery (EAES) foi fundada em Paris. Noventa e quatro cirurgiões de 10 países estavam presentes21-30. Desde então, um consórcio informal formado por cirurgiões e a indústria desenvolveram, em velocidade assustadora, novos e melhores equipamentos para a realização das então chamadas videocirurgias, especialmente sistemas ópticos, monitores especializados, fontes de luz fria e insufladores mais potentes. Novas fontes de energia igualmente apareceram e se desenvolveram, como o bisturi ultrassônico, ao largo de lançamentos de instrumentos e grampeadores especializados e inovadores. Devido a isto, novas e mais complexas cirurgias foram sendo realizadas por esta abordagem. Contraindicações iniciais como doenças com processos inflamatórios importantes e cirurgias oncológicas foram caindo uma a uma e hoje praticamente todas as cirurgias abdominais, respeitados os limites patológicos individuais, podem ser realizadas pelo método visualizado pelo pioneiros de 1901, mais de um século atrás. diminuindo a necessidade do aprendizado de ética discutível em pacientes e animais de experimentação. Agora podemos treinar o quanto quisermos, pelo tempo que tivermos disponível. Novas tecnologias estão a nossa porta, como a surpreendente cirurgia guiada por imagem, onde imagens escaneadas do corpo do próprio paciente serão projetadas, guiando o cirurgião pela anatomia real. A telecirurgia promete cirurgias a distância, acessíveis para aqueles que necessitarem nos locais mais ermos, como em estações espaciais e marinheiros no vasto oceano. A nanotecnologia permitirá para breve que pequenos robôs passeiem pelo nosso corpo, diagnosticando doenças, desobstruindo vasos, fazendo biópsias e cauterizando sangramentos. Utopia? Possivelmente Bozzini, aquele que inspecionou a uretra em 1806, também achava. Bem-vindos ao admirável mundo da Cirurgia Minimamente Invasiva! NOVAS TECNOLOGIAS, ABORDAGENS E O ENSINO DA VIDEOCIRURGIA 1. Utterback JM. Mastering the dynamics of innovation. Boston: Harvard Business School Press; 1994. 2. Christensen CM. The innovator’s dilemma: the revolutionary book that will change the way you do business. New York: HarperCollins; 1997:15-16. 3. Roberts EB. Innovation: driving product, process, and market change. San Francisco: Jossey-Bass; 2002. 4. Cosgrove DM. The innovation imperative. J Thorac Cardiovasc Surg. 2000 Nov;120(5):839-42. 5. The American Heritage Dictionary of the English Language, 4th ed. Houghton Mifflin; 2004. 6. Jones JW, McCullough LB, Richman BW. Ethics of surgical innovation to treat rare diseases. J Vasc Surg. 2004 Apr;39(4):918-9. 7. History of Technology. Encyclopaedia Britannica; 2004. 8. Gorden A. The history and development of endoscopic surgery. London: Saunders; 1993. 9. Gotz F, et al. The history of laparoscopy. In: Color atlas of laparoscopic Surgery. New York; 1993. 10. Modlin IM, Kidd M, Lye KD. From the lumen to the laparoscope. Arch Surg. 2004;139:1110-1126. 11. Lau WY, Leow CK, Li AK. History of endoscopic and laparoscopic surgery. World J Surg. 1997;21:444-453. 12. Litynski GS. Endoscopic surgery: the history, the pioneers. World J Surg. 1999;23:745-753. 13. Rosin D. History. In: Minimal Access Medicine and Surgery. Oxford: Radcliffe Medical; 1993:1-9. 14. Desormeaux A.J. De l’endoscopie, instrument proper a éclairer certaines cavités intérieures de l’économie. In: Compte rendu des séances de l’academie des sciences. Paris: Bachelier; 1855. 15. Desormeaux AJ. De l’endoscope et de ses applications au diagnostic et au traitement des affections de l’urèthre et de la vessie. Paris: Balliere; 1865. Paralelamente ao desenvolvimento da videocirurgia, novas tecnologias e abordagens surgiram e vêm despontando como a Minilaparoscopia, NOTES – Natural Orifices Translumenal Endoscopic Surgery, LESS - Laparoendoscopic Single-Site Surgery e a Cirurgia Robótica31-43. A capacidade de registro em vídeo de todas as cirurgias facilitou enormemente a difusão e o ensino da abordagem videocirúrgica. Cirurgiões são agora capazes de revisar suas próprias cirurgias, aprender com seus erros e ensinar de maneira didática seus pares em desenvolvimento técnico. A internet rápida facilita a comunicação em tempo real, a transmissão de cirurgias ao vivo, a troca de experiências em sites especializados e chats, bem como cursos didáticos pela web e transmissões de eventos científicos, permitindo acesso ao conhecimento fácil e barato, sem limite de distância. Em breve aplicativos para dispositivos móveis como telefones celulares e tablets incrementarão o desenvolvimento científico na área. A realidade virtual deixou de ser exclusivamente utilizada no treinamento de pilotos na área da aviação e invadiu o campo do treinamento da videocirurgia, v. 3 n. 8 REFERÊNCIAS AWRJ - Abdominal Wall Repair Journal 43 Anexo – High Tech Surgery Skinovsky et al. 16. Desormeaux AJ. The endoscope and its application to the diagnosis and treatment of affections of the genitourinary passages. Chicago Med J. 1867;24:177-194. 17. Bevan L. The oesophagoscope. Lancet. 1868;1:470. 18. Pantaleoni, D.C. On endoscopic examination of the cavity of the womb. Medical Press Circular. 1869;8:26-27. 19. Kelling G. Die tamponade der bauchhohle mit luft zur stillung lebensgefahrlicher intestinalblutungen. Med Wochenschr. 1901;48:1480. 20. Shah J. Endoscopy through the ages. Br J Urol Int. 2002;89:645. 21. Treuting R. Minimally invasive orthopedic surgery: arthroscopy. Ochsner J. 2000;2:158-163. 22. Mancuso S. Endoscopy in gynecology. Rays. 1998;23:603-604. 23. Paolucci B, Schaeff B, Stuttgart G. Gasless laparoscopy in general surgery and gynecology: diagnostic and operative procedures; 1996. 24. Spaner SJ, Warnock GL. A brief history of endoscopy, laparoscopy, and laparoscopic surgery. J Laparoendosc Adv Surg Tech. 1997;7:369-373. 25. Clark K, Wheelwright S. Organizing and leading heavyweight development teams. Calif Manage Rev. 1992;34:9-28. 26. Smith PG, Reinertsen DG. Developing Products in Half the Time. New York: Van Nostrand Reinhold; 1991. 27. Von Hippel E. Lead users: a source of novel product concepts. Manage Sci. 1986;32:791-805. 28. Drucker P. Innovation and entrepreneurship. New York: Harper & Row; 1985. 29. Schon DA. The reflective practitioner: how professionals think in action. New York: Basic Books; 1983. 30. Denis JL, Hebert Y, Langley A, et al. Explaining diffusion patterns for complex health care innovations. Health Care Manage Rev. 2002;27:60-73. 31. Greer AL. Scientific knowledge and social consensus. Controlled Clin Trials. 1994;15:431-36. 32. David TE. Innovation in surgery. J Thorac Cardiovasc Surg. 2000;119(suppl):38-41. 44 33. Shah J. Endoscopy through the ages. Br J Urol Int. 2002;89:645. 34. Darwin C. On the Origin of Species by Means of Natural Selection, or the Preservation of Favoured Races in the Struggle for Life. London: John Murray; 1859. 35. Lister J. On the antiseptic principle of the practice of surgery. Lancet. 1867;2. 36. Picard JF. American patronage and French Medicine: from the Rockefeller philanthropy to INSERM. In: John Shaw Billings Society for the History of Medicine; 1995. 37. Kalbasi H, Moddaressi Y. History and development of laparoscopic surgery. J Assoc Iranian Endosc Surgeons. 2001;1:1. 38. Sircus W. Milestones in the evolution of endoscopy: a short history. J R Coll Physicians (Edinb). 2003;33:124-134. 39. Nezhat C. Videolaseroscopy and laser laparoscopy in gynaecology. Br J Hosp Med. 1987;38:219-224. 40. Dubois FP, Berthelot G. Coelioscopic cholecystectomy: preliminary report of 36 cases. Ann Surg. 1990;211:60-62. 41. Dubois F, Berthelot G, Levard H. Laparoscopic cholecystectomy: historic perspective and personal experience. Surg Laparosc Endosc. 1991;1:52-57. 42. Christensen CM, Bohmer R, Kenagy J. Will disruptive innovations cure health care? Harvard Business Rev. 2000;78:102-112. 43. Filipi CJ, Fitzgibbons RJ, Salerno GM. Historical review: diagnostic laparoscopy to laparoscopic cholecystectomy and beyond. Surg Laparosc. 1991;3:21. 44. Clarke HC. History of endoscopic and laparoscopic surgery. World J Surg. 2001;25:967-968. 45. Stirrat G, Ramsay B. Surgical innovation under scrutiny. Lancet. 1993;342:187-188. 46. Stirratt G, et al. The challenge of evaluating surgical procedures. Ann R Coll Surg Engl. 1992;74:80-84. 47. Banta HD. Minimally Invasive Therapy (MIT). In: Five European Countries. Amsterdam: Elsevier; 1993. 48. Skinovsky J, Brawerman A, Alberti J, Chibata M. Videosurgery learning and the internet: how to keep yourself up-to-date accessing the virtual world. Bras. J. Video Sur. 2011; 4(2):96-100. AWRJ - Abdominal Wall Repair Journal v. 3 n. 8 v. 3 n. 8 AWRJ - Abdominal Wall Repair Journal 45 46 AWRJ - Abdominal Wall Repair Journal v. 3 n. 8
Baixar