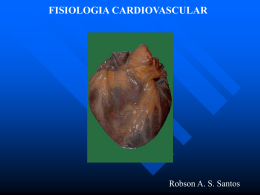
ARTICLE IN PRESS International Journal of Surgery (2006) www.int-journal-surgery.com SHORT REPORT RO OF Cardiac bullet embolus after thoracic vena cava penetrating injury causing tricuspid valve insufficiency DP ~o Ettinger, Carlos Hohlenwerger, Paulo Vicente*, Ricardo Eloi, Joa Leandro Leite, Paulo Amaral, Edvaldo Fahel TE Maranha~o Street, #206, Apartment 102, Pituba, 41830260 Salvador, Bahia, Brazil KEYWORDS EC Bullet; Embolus; Heart RR Introduction CO Emboli of foreign bodies to the heart, although unusual, have been reported with increasing frequency since 1834 when Davis published the first case report of a bullet embolus.1 Although bullets are one of the more common foreign body emboli to the heart and beyond, a cardiac ballistic embolus is a very rare situation.2 In the literature very few reports were found, so far this is a unique case, because the patient had a very dangerous lesion which is the vena cava wound associated with a cardiac embolus causing tricuspid valve insufficiency. Case report UN 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 -, -e- A 25-year-old patient was admitted with a history of armed robbery, having been shot with a 38* Corresponding author. Tel.: þ55 71 33450887. E-mail address: [email protected] (P. Vicente). caliber revolver and presenting a gunshot wound in the right hemithorax. He entered the emergence room (ER) and physical examination revealed pervious airways with spontaneous breathing, stable hemodynamically, neurologically normal, with a penetrating injury above the right clavicle. No wound exit was noted. The PA and lateral chest X-ray showed a small hemothorax and a 38-mm special projectile (low velocity bullet) in the projection of the heart (Fig. 4) After that, a chest drain was placed and the patient suddenly developed a continuous bleeding via thoracostomy tube and was taken immediately to the operation room (OR) to be submitted to a right thoracotomy, which showed a hemothorax and a bullet entrance orifice in the superior vena cava. The bullet was not found and there was not an exit orifice for the projectile, the injury was treated with a 3-0 polypropylene running suture and closed thoracic drainage. Later, the patient was stabilized and immediately taken to the intensive care unit (ICU). 1743-9191/$ - see front matter ª 2006 Surgical Associates Ltd. Published by Elsevier Ltd. All rights reserved. doi:10.1016/j.ijsu.2006.04.008 IJSU126_proof 16 May 2006 1/3 57 58 59 60 61 62 63 64 65 66 67 68 69 70 71 72 73 74 75 76 77 78 79 80 81 82 83 84 85 86 87 88 89 90 91 92 93 94 95 96 97 98 99 100 101 102 103 104 105 106 107 108 109 110 111 112 ARTICLE IN PRESS 2 RO right atriotomy incision was performed and the missile was successfully removed from the trabeculae of the right ventricle (Figs. 1 and 2). There was no evidence of injury to the internal structures of the heart. The postoperative course was without complications, and the patient was discharged on the 5th postoperative day (Fig. 3). Discussion TE After clinical improvement, the surgical and intensive care team looked for the projectile and the image of the bullet was found in the topography of the heart. The lateral chest X-ray showed a defocused bullet (characteristic of a cardiac embolus) so the team agreed that the bullet was moving because it was inside the cardiac chamber. A systolic murmur was also found, an echocardiography was preceded and the cardiologist found it normal; a radioscopy was done and the missile was found moving together with the heart so another echocardiogram was performed by the same cardiologist and at that time a tricuspid valve insufficiency and an image suggestive of a projectile inside the right ventricle were found. The surgical team discussed the possibility of percutaneous transvenous retrieval of the projectile, and the cardiothoracic team discarded this possibility because of the probable difficulty in assessing the bullet surrounded by the trabeculae of the right ventricle. The patient was prepared and submitted to a cardiac surgery; a median sternotomy with cardiopulmonary bypass and bicaval cannulation. A Figure 3 Patient at the ICU after the operation for the bullet retrieve. DP Figure 1 The 38 special bullet trapped in the chordae tendineae of the right ventricle, the uninjured tricuspid valve is also seen after the atriotomy with cardiopulmonary bypass. OF Area of bullet entry The diagnosis of bullet emboli to the heart is usually not difficult when proper roentgenograms are obtained. The presence of a wound of entry, the lack of a wound of exit, and the absence of the bullet in the wounded part raise the index of suspicious.2 It is important the attention while analyzing the Chest radiograph and observe the position of the projectile. If the bullet is blurred (defocused), it indicates the missile is moving together with the cardiac motion, and can lead to diagnose a cardiac embolus (Fig. 4A). Extremely critical patients requiring operative intervention prior to any X-Rays may have the diagnosis missed initially, but subsequent films will result in the discovery of the embolized missile,2 as happened in this case. It is imperative to make an echocardiography to document bullet localization in the right ventricular cavity prior to surgical removal.3 The classical indications for the surgical removal of cardiac foreign bodies include preventing embolus of the foreign body to more dangerous sites, reducing the danger of bacterial endocarditis, preventing recurrent pericardial effusions, preventing erosion of cardiac wall and diminishing the incidence of myocardial damage.4 The presence of lead missiles in the cardiovascular system also may lead to lead toxicity (plumbism).5 Management of bullet embolization to heart can be treated conservatively in some patients. In this EC RR CO UN 113 114 115 116 117 118 119 120 121 122 123 124 125 126 127 128 129 130 131 132 133 134 135 136 137 138 139 140 141 142 143 144 145 146 147 148 149 150 151 152 153 154 155 156 157 158 159 160 161 162 163 164 165 166 167 168 J. Ettinger et al. Figure 2 Retrieve of the projectile. IJSU126_proof 16 May 2006 2/3 169 170 171 172 173 174 175 176 177 178 179 180 181 182 183 184 185 186 187 188 189 190 191 192 193 194 195 196 197 198 199 200 201 202 203 204 205 206 207 208 209 210 211 212 213 214 215 216 217 218 219 220 221 222 223 224 ARTICLE IN PRESS Cardiac bullet embolus causing tricuspid valve insufficiency Bullet thoracic entry Superior vena cava injury Drain Right ventricule OF Right atrium RO Tricuspid valve DP A Bullet B Figure 4 (A) Postero-anterior chest X-ray showing blurred bullet in the projection of the right ventricle. (B) Bullet trajectory. evaluation and treatment are essential in these cases. TE case, we decided to retrieve the bullet due to the classical indications and because it was causing tricuspid insufficiency as shown by the echocardiogram (probably the bullet was pulling the chordae tendinae and causing this dysfunction). Missiles that are embedded in the subvalvar apparatus may require open excision to prevent systemic thromboembolism or chronic valvular dysfunction.6 Another issue to be considered is the possibility of the patient developing psychological problems related to the awareness that the bullet is inside the heart, causing ‘‘cardiac neurosis’’.7 There are in medical literature references of successful percutaneous retrieve of bullet embolus localized in the right ventricle, however, in our case this was not possible due to the probable difficulty in assessing the bullet surrounded by the trabeculae of the right ventricle and due to the indication of mandatory retrieve previously cited. We conclude that a superior vena cava injury due to gunshot wound associated with a cardiac embolus is a challenging injury and the specialized References EC RR CO UN 225 226 227 228 229 230 231 232 233 234 235 236 237 238 239 240 241 242 243 244 245 246 247 248 249 250 251 252 253 254 255 256 257 258 259 260 261 262 263 264 265 266 267 268 269 270 271 272 273 274 275 276 277 278 279 280 281 3 1. Barret NR. Foreign bodies in the cardiovascular system. Br J Surg 1960;37:416e45. 2. Bartlett H, Anderson CB, Steinhoff N. Bullet embolism to the heart. J Trauma 1973;13:476. 3. Amsel BJ, Van der Mast M, De Bock L, van Haasen R, Beeckman C. The importance of two-dimensional echocardiography in the location of a bullet embolus to the right ventricle. Ann Thorac Surg 1988 Jul;46(1):102e3. 4. Harken DE, Zoll PM. Foreign bodies in and in relation to the thoracic blood vessels and heart. III. Indications for the removal of intracardiac foreign bodies and the behavior of the heart during manipulation. Am Heart J 1946;32:1e19. 5. Schmelzer V, Mendez-Picon G, Gervin AS. Case report: transthoracic retrograde venous bullet embolization. J Trauma 1989 Apr;29(4):525e7. 6. Corbertt H, Paulsen EK, Smith S, Carman C. Paradoxical bullet embolus from the vena cava: a case report. J Trauma 2003 Nov;55(5):979e81. 7. Shannon FL, McCroskey BL, Moore EE, Moore FA. Venous bullet embolism: rationale for mandatory extraction. J Trauma 1987 Oct;27(10):1118e22. IJSU126_proof 16 May 2006 3/3 282 283 284 285 286 287 288 289 290 291 292 293 294 295 296 297 298 299 300 301 302 303 304 305 306 307 308 309 310 311 312 313 314 315 316 317 318 319 320 321 322 323 324 325 326 327 328 329 330 331 332 333 334 335 336 337 338
Baixar