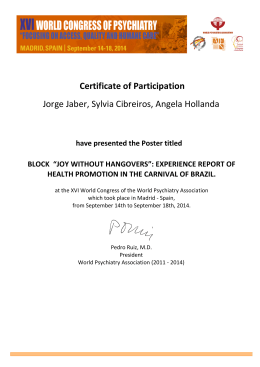
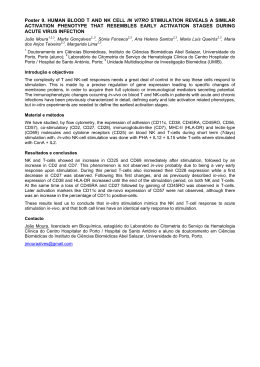
ARTICLE IN PRESS CORRESPONDENCE Remission of Major Depression Under Deep Brain Stimulation of the Lateral Habenula in a Therapy-Refractory Patient To the Editor: epression is a severe, common psychiatric illness with limited therapeutic options. Only approximately twothirds of patients treated respond to standard antidepressants. Even with electroconvulsive therapy (ECT), a significant fraction remains therapy refractory. For such cases deep brain stimulation (DBS) is currently under investigation: DBS of the subcallosal cingulate was successful in 7 of 20 patients after 6 months (1). Stimulating the ventral capsule/ ventral striatum resulted in 3 of 15 remitted patients (2). A possible novel target is suggested by anatomical implications of the long-standing monoamine hypothesis of depression (3): the serotonergic, noradrenergic, and dopaminergic system each have strong interactions and direct efferents from the lateral habenula (LHb) (to dorsal raphe nuclei, locus coeruleus, and ventral tegmental area) that in turn receives limbic and cortical inputs (4). During learned helplessness, an animal model of depression and anxiety (5), susceptible rats (6) showed striking LHb hypermetabolism (7). In humans, this area covaries with dorsal raphe nuclei activity during the induction of depression through tryptophan depletion (8,9), and shows selective volume reductions in brains of patients with depression (10). Recent primate work implicated the LHb in controlling reward through the ventral tegmental area, constituting a “circuit of disappointment” (11). In summary, convergent evidence indicates that overactivity in the LHb is present during depressed states, where it could drive the changes in midbrain activity linked to depression (12,13). This suggests that the LHb might prove to be a promising novel target for DBS in cases of intractable major affective disorder. We report here the results on the first patient with treatmentresistant major depression undergoing bilateral DBS of the major afferent bundle (i.e., stria medullaris thalami) of the LHb. D Patient and Method. Our female patient with major depressive disorder (DSM-IV) was 64 years old at the time of DBS surgery (July 2008). She suffered from major depressive episodes (MDE) beginning at age 18 without any hypomanic or manic episodes. No additional psychiatric diagnoses were made. At age 55, the first severe depressive episode with psychotic features was described. Appropriate pharmacotherapeutic trials involving antidepressants and augmentation with lithium, valproate, and various antipsychotic medications could not control the illness. At age 59, after two suicide attempts, she received ECT. Although remission was achieved after seven sessions, it could not be maintained. The patient unfailingly experienced early relapse despite maximal pharmacotherapy (at least one antidepressant, one antipsychotic and lithium), necessitating repeat ECT. We therefore started maintenance ECT (mECT), 2.5 years before surgery. However, we were unable to prolong ECT intervals to a period of 2 weeks or longer without relapse, despite concurrent medication including sertraline, mirtazepine, and risperidone in the last year. During mECTs, the patient experienced four severe relapses, rapidly developing over 2 days–3 days, reaching Hamilton Depression Scale (HAMD21) ratings of approximately 45, with severe psychotic features (delusions of guilt), mutism, and pronounced anxiety. With deteriorating quality of life and increasing side effects from ECT and pharmacotherapy, we suggested DBS surgery. 0006-3223/09/$36.00 Figure 1. Clinical time course. This figure demonstrates three relapses of our patient, quantified with the Hamilton depression scale (HAMD21). The first relapse was treated with six electroconvulsive therapy sessions. Later on, during full remission at week 0, deep brain stimulation (DBS) surgery was performed. As shown in red, early stimulation was done with 5 V, and the patient consecutively relapsed again. Stimulation was stepwise increased to 10.5 , and finally the patient reached full and stable remission (HAMD21 ⫽ 3). The third relapse occurred a couple of days after the DBS unit was switched off due to an incidental bicycle accident. Again the patient reached remission (HAMD21 ⫽ 0) after 12 weeks of high-voltage DBS. After two independent psychiatrists evaluated the patient and supported this course of action, we obtained informed consent from the patient (during a phase of remission), her husband, and her son for this off-label-use treatment option. After a severe relapse 3 weeks later, another ECT course, and full remission she received bilateral DBS surgery. The complete time course is demonstrated in Figure 1 (see also Supplement 1). We measured brain glucose metabolism with fluorodeoxyglucose positron emission tomography (FDG-PET) before DBS surgery (T1) to exclude causes of organic mood disorder and followed up with a study at week 24 (T2) during high-parameter stimulation. At each time point the patient was clinically remitted. To localize changes over time, we co-registered the PET T1 and T2 images and calculated a difference image (T2 ⫺ T1). To localize anatomical regions as well as the position of the electrode tips, the post-operation CT image was co-registered to a high-resolution T1 (1 mm ⫻ 1 mm ⫻ 1 mm) magnetic resonance tomography (MRT) scan of the patient and the PET difference images to the T1 MRT scan with the same transformation parameters. All processing steps used SPM5 (Wellcome Trust Center for Neuroimaging, London, United Kingdom; http:// www.fil.ion.ucl.ac.uk/spm). A strong bilateral increase of metabolism was found bilaterally at the electrode tips in the afferent bundles (Figure 2). Discussion. The DBS procedure resulted in a sustained full remission of depressive symptoms in a patient who was therapyresistant to all standard treatments for at least 9 years and suffered from severe major depressive disorder for 46 years. Placebo effects, which are extremely uncommon in this patient population (14), could be further excluded by a severe relapse when stimulation was briefly accidentally discontinued. We did not observe an acute antidepressive effect of DBS. After switching to high stimulation, the interval to remission of BIOL PSYCHIATRY 2009;xx:xxx © 2009 Society of Biological Psychiatry ARTICLE IN PRESS e2 BIOL PSYCHIATRY 2009;xx:xxx Correspondence Supplementary material cited in this article is available online. Alexander Sartorius Department of Psychiatry and Psychotherapy Central Institute of Mental Health J5, D-68159 Mannheim, Germany [email protected] Karl L. Kiening Department of Neurosurgery Division of Stereotactic Neurosurgery University Hospital Heidelberg Heidelberg, Germany Peter Kirsch Department of Psychiatry and Psychotherapy Central Institute of Mental Health Mannheim, Germany Carl C. von Gall Uwe Haberkorn Department of Nuclear Medicine University of Heidelberg Heidelberg, Germany Figure 2. Fluorodeoxyglucose positron emission tomography (FDG-PET) imaging of metabolic effects of deep brain stimulation treatment. Cerebral standardized uptake values (SUVs) are shown. (A) The FDG-PET image at time point T2 (post-surgery, full stimulation, full remission, week 24 in Figure 1), showing marked metabolic increase at electrode tip sides. (B) Sagittal view shows coincidence of left electrode tip position (marked in green) with maximum metabolic increase with a difference of approximately 6 SUVs between T2 and T1 (post-surgery–pre-surgery). Thresholded positive difference images overlayed on the magnetic resonance tomography scan are shown. (C and D) Transversal and coronal view as indicated by yellow line in (B). Andreas W. Unterberg Department of Neurosurgery University Hospital Heidelberg Heidelberg, Germany Fritz A. Henn Brookhaven National Laboratory Life Sciences Long Island, New York Andreas Meyer-Lindenberg approximately 4 months corresponds to the mean time span reported in other DBS patients stimulated at the ventral capsule/ ventral striatum or subcallosal cingulate (1,2). This convergent experience, which is in marked contrast with the immediate effects that DBS has in many neurological conditions, points to induced neural plasticity in mood-regulatory circuits in recovery from depression. With FDG-PET, we could verify a localized metabolic increase at the stimulation sites, as intended. Because local brain energy consumption is driven by both inhibitory and excitatory synaptic activity (15), the functional consequences of this afferent stimulation on the LHb cannot be directly inferred from PET but are expected to be inhibitory as discussed in the preceding text. No changes in LHb metabolism were detected or expected, because convergent prior data showed a state-dependency of LHb hyperactivity, and our patient was in full remission during both procedures. In conclusion, we report the first successful treatment of a severe treatment-resistant depression with verified functional modulation of the major afferent bundle of the LHb. Our data support a critical role of this structure, at the juncture of brainstem monoaminergic systems and limbic regulatory cortex, in depression. Our experience should prompt a clinical trial of this approach. We would like to acknowledge the excellent clinical support of Dr. Eva Grips and Dr. Michael Fritzinger. The authors AS and KLK are joint first authors. The authors reported no biomedical financial interests or potential conflicts of interest. www.sobp.org/journal Department of Psychiatry and Psychotherapy Central Institute of Mental Health Mannheim, Germany 1. Lozano AM, Mayberg HS, Giacobbe P, Hamani C, Craddock RC, Kennedy SH (2008): Subcallosal cingulate gyrus deep brain stimulation for treatment-resistant depression. Biol Psychiatry 64:461– 467. 2. Malone DA Jr, Dougherty DD, Rezai AR, Carpenter LL, Friehs GM, Eskandar EN, et al. (2009): Deep brain stimulation of the ventral capsule/ventral striatum for treatment-resistant depression. Biol Psychiatry 65:267–275. 3. Schildkraut JJ, Kety SS (1967): Biogenic amines and emotion. Science 156:21–37. 4. Geisler S, Trimble M (2008): The lateral habenula: No longer neglected. CNS Spectr 13:484 – 489. 5. Seligman ME, Maier SF, Geer JH (1968): Alleviation of learned helplessness in the dog. J Abnorm Psychol 73:256 –262. 6. Henn FA, Vollmayr B (2005): Stress models of depression: Forming genetically vulnerable strains. Neurosci Biobehav Rev 29:799 – 804. 7. Shumake J, Edwards E, Gonzalez-Lima F (2003): Opposite metabolic changes in the habenula and ventral tegmental area of a genetic model of helpless behavior. Brain Res 963:274 –281. 8. Morris JS, Smith KA, Cowen PJ, Friston KJ, Dolan RJ (1999): Covariation of activity in habenula and dorsal raphe nuclei following tryptophan depletion. Neuroimage 10:163–172. 9. Roiser JP, Levy J, Fromm SJ, Nugent AC, Talagala SL, Hasler G, et al. (2009): The effects of tryptophan depletion on neural responses to emotional words in remitted depression. Biol Psychiatry 66:441– 450. 10. Ranft K, Dobrowolny H, Krell D, Bielau H, Bogerts B, Bernstein HG (2009): Evidence for structural abnormalities of the human habenular complex in affective disorders but not in schizophrenia. Psychol Med 12:1–11. ARTICLE IN PRESS Correspondence 11. Matsumoto M, Hikosaka O (2007): Lateral habenula as a source of negative reward signals in dopamine neurons. Nature 447:1111– 1115. 12. Sartorius A, Henn FA (2007): Deep brain stimulation of the lateral habenula in treatment resistant major depression. Med Hypotheses 69:1305–1308. 13. Hikosaka O, Sesack SR, Lecourtier L, Shepard PD (2008): Habenula: Crossroad between the basal ganglia and the limbic system. J Neurosci 28:11825–11829. BIOL PSYCHIATRY 2009;xx:xxx e3 14. Mayberg HS, Lozano AM, Voon V, McNeely HE, Seminowicz D, Hamani C, et al. (2005): Deep brain stimulation for treatment-resistant depression. Neuron 45:651– 660. 15. Waldvogel D, van Gelderen P, Muellbacher W, Ziemann U, Immisch I, Hallett M (2000): The relative metabolic demand of inhibition and excitation. Nature 406:995–998. doi:10.1016/j.biopsych.2009.08.027 www.sobp.org/journal
Baixar