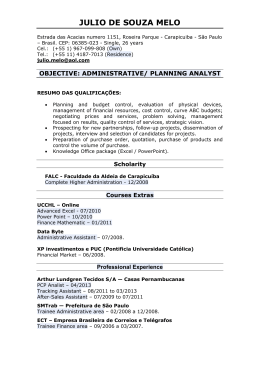
ISSN 0034-7280 Versão impressa Publicação bimestral Vol. 74 - nº 4 - Julho/Agosto 2015 REVISTA BRASILEIRA DE OFTALMOLOGIA JUL/AGO 2015 VOLUME 74 NÚMERO 4 P. 197-268 100 w Correlation of accommodation and asthenopia in hyperopic patients w Biomarkers and surrogate endpoints in glaucoma w Granuloma macular por tuberculose w Perda visual irreversível após uso de Paclitaxel 95 75 25 5 0 capa-JULHO-AGOSTO sexta-feira, 22 de maio de 2015 16:35:20 197 ISSN 0034-7280 Revista Brasileira de (Versão impressa) ISSN 1982-8551 (Versão eletrônica) Oftalmologia PUBLICAÇÃO OFICIAL: SOCIEDADE BRASILEIRA DE OFTALMOLOGIA SOCIEDADE BRASILEIRA DE CATARATA E IMPLANTES INTRAOCULARES SOCIEDADE BRASILEIRA DE CIRURGIA REFRATIVA Sociedade Brasileira de Oftalmologia Indexada nas bases de dados: LILACS Literatura Latino-americana em Ciências da Saúde SciELO Scientific Electronic Library OnLine WEB OF SCIENCE www.freemedicaljournals.com Disponível eletronicamente: www.sboportal.org.br Publicação bimestral Editor Chefe André Luis Freire Portes (RJ) Editor Executivo Arlindo José Freire Portes (RJ) Co-editores André Luiz Land Curi (RJ) Bruno Machado Fontes (RJ) Carlos Eduardo Leite Arieta (SP) Hamilton Moreira (PR) Liana Maria Vieira de Oliveira Ventura (PE) Marcony R. Santhiago (RJ) Mario Martins dos Santos Motta (RJ) Maurício Maia (SP) Newton Kara-Junior (SP) Niro Kasahara (SP) Renato Ambrósio Jr. (RJ) Ricardo Augusto Paletta Guedes (MG) Rodrigo Pessoa Cavalcanti Lira (PE) Silvana Artioli Schellini (SP) Walton Nosé (SP) Corpo Editorial Internacional Baruch D. Kuppermann - Califórnia - EUA Christopher Rapuano - Phyladelphia - EUA Curt Hartleben Martkin - Colina Roma - México Daniel Grigera - Olivos - Argentina Deepinder Kauer Dhaliwal - Pittsburg - EUA Felipe A. A. Medeiros - Califórnia - EUA Felix Gil Carrasco - México – México Fernando Arevalo - Riyadh - Arábia Saudita Francisco Rodríguez Alvira – Bogotá - Colombia Howard Fine - Eugene - EUA Jean Jacques De Laey - Ghent - Bélgica Kevin M. Miller - Califórnia - EUA Lawrence P. Chong - Califórnia - EUA Lihteh Wu – San José - Costa Rica Liliana Werner - Utah - EUA Miguel Burnier Jr. - Montreal - Canadá Pablo Cibils - Assunção - Paraguai Patricia Mitiko Santello Akaishi – Arábia Saudita Peter Laibson - Phyladelphia - EUA Steve Arshinoff - Toronto - Canadá Corpo Editorial Nacional Abelardo de Souza Couto - Rio de Janeiro- RJ Abrahão da Rocha Lucena - Fortaleza - CE Alexandre Augusto Cabral de Mello Ventura - Recife - PE Alexandre H. Principe de Oliveira – Salvador – BA Alexandre Seminoti Marcon – Porto Alegre - RS Ana Carolina Cabreira Vieira – Rio de Janeiro – RJ Ana Luisa Hofling de Lima - São Paulo - SP André Correa de Oliveira Romano – Americana - SP André Curi - Rio de Janeiro - RJ André Luis Freire Portes - Rio de Janeiro - RJ André Marcio Vieira Messias – Ribeirão Preto – SP Andrea Kara José Senra - São Paulo – SP Antonio Marcelo Barbante Casella - Londrina - PR Armando Stefano Crema- Rio de Janeiro- RJ Beatriz de Abreu Fiuza Gomes – Rio de Janeiro - RJ Bruna Vieira Ventura - Recife - PE Bruno Diniz – Goiânia - GO Coordenação de Aperfeiçoamento de Pessoal de Nível Superior http://www.capes.gov.br Rev Bras Oftalmol, v. 74, n. 4, p. 197-268, Jul./Ago. 2015 Carlos Augusto Moreira Jr.- Curitiba- PR Carlos Gabriel Figueiredo - São José do Rio Preto - SP Carlos Ramos de Souza Dias- São Paulo- SP Claudio do Carmo Chaves - Manaus - AM Cristiano Caixeta Umbelino - São Paulo - SP Daniel Lavinsky – Porto Alegre - RS David Leonardo Cruvinel Isaac – Goiania - GO Diego Tebaldi Q. Barbosa - São Paulo - SP Edmundo Frota De Almeida Sobrinho- Belém- PA Eduardo Buchele Rodrigues – Florianópolis - SC Eduardo Cunha de Souza – São Paulo - SP Eduardo Damasceno - Rio de Janeiro - RJ Eduardo Dib – Rio de Janeiro - RJ Eduardo Ferrari Marback- Salvador- BA Eliezer Benchimol - Rio de Janeiro - RJ Enzo Augusto Medeiros Fulco – Jundiaí - SP Eugenio Santana de Figueiredo – Juazeiro do Norte - CE Fábio Marquez Vaz – Ondina – BA Felipe Almeida - Ribeirão Preto - SP Fernando Cançado Trindade - Belo Horizonte- MG Fernando Marcondes Penha - Florianópolis - SC Fernando Oréfice- Belo Horizonte- MG Fernando Roberte Zanetti – Vitória - ES Flavio Rezende- Rio de Janeiro- RJ Francisco de Assis Cordeiro Barbosa - Recife - PE Frederico Valadares de Souza Pena – Rio de Janeiro - RJ Frederico Guerra - Niterói - RJ Giovanni N.U.I.Colombini- Rio de Janeiro- RJ Guilherme Herzog Neto- Rio de Janeiro- RJ Harley Biccas - Ribeirão Preto - SP Haroldo Vieira de Moraes Jr.- Rio de Janeiro- RJ Hélcio Bessa - Rio de Janeiro - RJ Helena Parente Solari - Niterói - RJ Heloisa Helena Abil Russ – Curitiba – PR Henderson Celestino de Almeida- Belo Horizonte- MG Hilton Arcoverde G. de Medeiros- Brasilia- DF Homero Gusmao de Almeida- Belo Horizonte- MG Italo Mundialino Marcon- Porto Alegre- RS Iuuki Takasaka – Santa Isabel - SP Ivan Maynart Tavares - São Paulo - SP Jaco Lavinsky - Porto Alegre - RS Jair Giampani Junior – Cuiabá - MT Jeffersons Augusto Santana Ribeiro - Ribeirão Preto - SP João Borges Fortes Filho- Porto Alegre- RS João Luiz Lobo Ferreira – Florianópolis – SC João Marcelo de Almeida G. Lyra - Maceió - AL João Orlando Ribeiro Goncalves- Teresina- PI Jorge Carlos Pessoa Rocha – Salvador – BA JorgeAlberto de Oliveira - Rio de Janeiro - RJ José Augusto Cardillo – Araraquara – SP José Beniz Neto - Goiania - GO José Ricardo Carvalho L. Rehder- São Paulo- SP Laurentino Biccas Neto- Vitória- ES Leonardo Akaishi - Brasília - DF Leonardo Provetti Cunha - SP Leticia Paccola - Ribeirão Preto - SP Liana Maria V. de O. Ventura- Recife- PE Luiz Alberto Molina - Rio de Janeiro - RJ Manuel Augusto Pereira Vilela- Porto Alegre- RS Marcelo Hatanaka – São Paulo – SP Marcelo Netto - São Paulo - SP Marcelo Palis Ventura- Niterói- RJ Marcio Bittar Nehemy - Belo Horizonte - MG Marco Antonio Bonini Filho - Campo Grande - MS Marco Antonio Guarino Tanure - Belo Horizonte - MG Marco Antonio Rey de Faria- Natal- RN Marcos Pereira de Ávila - Goiania - GO Maria de Lourdes Veronese Rodrigues- Ribeirão Preto- SP Maria Rosa Bet de Moraes Silva- Botucatu- SP Maria Vitória Moura Brasil - Rio de Janeiro - RJ Mário Genilhu Bomfim Pereira - Rio de Janeiro - RJ Mario Luiz Ribeiro Monteiro - São Paulo- SP Mário Martins dos Santos Motta- Rio de Janeiro- RJ Marlon Moraes Ibrahim – Franca - SP Mauricio Abujamra Nascimento – Campinas - SP Maurício Bastos Pereira - Rio de Janeiro - RJ Maurício Dela Paolera - São Paulo - SP Miguel Ângelo Padilha Velasco- Rio de Janeiro- RJ Miguel Hage Amaro - Belém - PA Milton Ruiz Alves- São Paulo- SP Moyses Eduardo Zadjdenweber - Rio de Janeiro - RJ Nassim da Silveira Calixto- Belo Horizonte- MG Nelson Alexandre Sabrosa - Rio de Janeiro – RJ Newton Kara-José - São Paulo - SP Newton Leitão de Andrade – Fortaleza – CE Núbia Vanessa dos Anjos Lima Henrique de Faria - Brasília-DF Octaviano Magalhães Júnior - Atibaia - SP Oswaldo Moura Brasil- Rio de Janeiro- RJ Otacílio de Oliveira Maia Júnior – Salvador - BA Patrick Frensel de Moraes Tzelikis – Brasília – DF Paulo Augusto de Arruda Mello Filho – São Paulo – SP Paulo Augusto de Arruda Mello- São Paulo- SP Paulo Schor - São Paulo - SP Pedro Carlos Carricondo – São Paulo – SP Pedro Duraes Serracarbassa – São Paulo – SP Priscilla de Almeida Jorge – Recife – PE Rafael Ernane Almeida Andrade - Itabuna – BA Raul N. G. Vianna - Niterói - RJ Remo Susanna Jr.- São Paulo- SP Renata Rezende - Rio de Janeiro - RJ Renato Ambrosio Jr.- Rio de Janeiro- RJ Renato Luiz Nahoum Curi- Niterói- RJ Richard Yudi Hida – São Paulo – SP Riuitiro Yamane - Niterói - RJ Roberto Lorens Marback - Salvador - BA Roberto Pinto Coelho – Ribeirão Preto – SP Rodrigo França de Espíndola – São Paulo – SP Rogerio Alves Costa- Araraquara- SP Rogerio de Almeida Torres - Curitiba - PR Rubens Belfort Neto – São Paulo – SP Rubens Camargo Siqueira- São José do Rio Preto- SP Sebastião Cronemberger So.- Belo Horizonte- MG Sérgio Henrique S. Meirelles- Rio de Janeiro- RJ Sérgio Kwitko - Porto Alegre - RS Sérgio Luis Gianotti Pimentel – São Paulo – SP Silvana Artioli Schellini - Botucatu- SP Suel Abujamra- São Paulo - SP Suzana Matayoshi - São Paulo - SP Tânia Mara Cunha Schaefer – Curitiba – PR Vitor Cerqueira - Rio de Janeiro - RJ Walter Yukihiko Takahashi – São Paulo – SP Walton Nose- São Paulo- SP Wener Passarinho Cella - Plano Piloto - DF Wesley Ribeiro Campos- Passos- MG Yoshifumi Yamane- Rio de Janeiro- RJ Redação: Rua São Salvador, 107 Laranjeiras - CEP 22231-170 Rio de Janeiro - RJ Tel: (0xx21) 3235-9220 Fax: (0xx21) 2205-2240 Tiragem: 5.000 exemplares Edição:Bimestral Secretaria: Marcelo Diniz Editoração Eletrônica: Sociedade Brasileira de Oftalmologia Responsável: Marco Antonio Pinto DG 25341RJ Publicidade: Sociedade Brasileira de Oftalmologia Responsável: João Diniz [email protected] Revisão: Eliana de Souza FENAJ-RP 15638/71/05 Normalização: Edna Terezinha Rother Assinatura Anual: R$420,00 ou US$280,00 Impressão: Gráfica Stamppa Associada a ABEC - Associação Brasileira de Editores Científicos 198 Revista Brasileira de Oftalmologia Rua São Salvador, 107 - Laranjeiras - CEP 22231-170 - Rio de Janeiro - RJ Tels: (0xx21) 3235-9220 - Fax: (0xx21) 2205-2240 - e-mail: [email protected] - www.sboportal.org.br Revista Brasileira de Oftalmologia, ISSN 0034-7280, é uma publicação bimestral da Sociedade Brasileira de Oftalmologia Diretoria da SBO 2015-2016 Presidente: João Alberto Holanda de Freitas (SP) Vice-presidentes: Armando Stefano Crema (RJ) Durval Moraes de Carvalho Jr. (SP) Francisco de Assis Cordeiro Barbosa (PE) Miguel Hage Amaro (PA) Sérgio Kwitko (RS) Secretário Geral: Arlindo José Freire Portes (RJ) 1º Secretário: Oswaldo Ferreira Moura Brasil (RJ) 2º Secretário: Jorge Carlos Pessoa Rocha (BA) Tesoureiro: Mário Martins dos Santos Motta (RJ) Diretor de Cursos: Gustavo Amorim Novais (RJ) Diretor de Publicações: André Luis Freire Portes (RJ) Diretor de Biblioteca: Evandro Gonçalves de Lucena Junior (RJ) Conselho Consultivo: Carlos Alexandre de Amorim Garcia (RN) Eduardo Henrique Morizot Leite (RJ) Marco Antonio Rey de Faria (RN) Conselho Fiscal: Efetivos: Jacqueline Coblentz (RJ) Marcelo Lima de Arruda (RJ) Ricardo Lima de Almeida Neves (RJ) Suplentes: Arnaldo Pacheco Cialdini (GO) Helcio José Fortuna Bessa (RJ) Silvana Maria Pereira Vianello (MG) SOCIEDADES FILIADAS À SOCIEDADE BRASILEIRA DE OFTALMOLOGIA Associação Brasileira de Banco de Olhos e Transplante de Córnea Presidente: Ari de Souza Pena Associação Maranhense de Oftalmologia Presidente: Romero Henrique Carvalho Bertand Associação Matogrossense de Oftalmologia Presidente: Jair Giampani Junior Associação Pan-Americana de Banco de Olhos Presidente: Alvio Isao Shiguematsu Associação Paranaense de Oftalmologia Presidente: Otavio Siqueira Bisneto Associação Rondoniense de Oftalmologia Presidente: Renata Campos Sales Associação Sul Matogrossense de Oftalmologia Presidente: Elson Yamasato Associação Sul-Mineira de Oftalmologia Presidente: Mansur Elias Ticly Junior Sociedade Alagoana de Oftalmologia Presidente: Mário Jorge Santos Sociedade Brasileira de Administração em Oftalmologia Presidente: Ronald Fonseca Cavalcanti Sociedade Brasileira de Catarata e Implantes Intraoculares Presidente: Carlos Gabriel de Figueiredo Sociedade Brasileira de Cirurgia Plástica Ocular Presidente: Guilherme Herzog Neto Sociedade Brasileira de Cirurgia Refrativa Presidente: Carlos Gabriel de Figueiredo Sociedade Brasileira de Ecografia em Oftalmologia Presidente: Leila Sueli Gouveia José Sociedade Brasileira Glaucoma Presidente: Francisco Eduardo Lopes Lima Sociedade Capixaba de Oftalmologia Presidente: Adriana Vieira Cardozo Sociedade Catarinense de Oftalmologia Presidente: Ayrton Roberto Bravo Ramos Sociedade Cearense de Oftalmologia Presidente: Newton Andrade Júnior Sociedade Goiana de Oftalmologia Presidente: José Eduardo Simarro Rios Sociedade Norte-Nordeste de Oftalmologia Presidente: Carlos Alexandre de Amorim Garcia Sociedade de Oftalmologia do Amazonas Presidente: Leonardo Bivar Sociedade de Oftalmologia da Bahia Presidente: André Hasler Príncipe de Oliveira Sociedade de Oftalmologia do Nordeste Mineiro Presidente: Mauro César Gobira Guimarães Sociedade de Oftalmologia de Pernambuco Presidente: Alexandre Augusto Cabral de Mello Ventura Sociedade de Oftalmologia do Rio Grande do Norte Presidente: Nelson Roberto Salustino Galvão Sociedade de Oftalmologia do Rio Grande do Sul Presidente: Afonso Reichel Pereira Sociedade de Oftalmologia do Sul de Minas Presidente: Mansur Elias Ticly Junior Sociedade Paraense de Oftalmologia Presidente: Frederico José Correia Lobato Sociedade Paraibana de Oftalmologia Presidente: Saulo Zanony Lemos Neiva Sociedade Piauiense de Oftalmologia Maria de Lourdes Cristina Alcântara Paz Carvalho do Nascimento Sociedade Sergipana de Oftalmologia Presidente: Carlos Barreto Barbosa Jr. 199 Revista Brasileira de ISSN 0034-7280 (Versão impressa) ISSN 1982-8551 (Versão eletrônica) Oftalmologia PUBLICAÇÃO OFICIAL: SOCIEDADE BRASILEIRA DE OFTALMOLOGIA SOCIEDADE BRASILEIRA DE CATARATA E IMPLANTES INTRAOCULARES SOCIEDADE BRASILEIRA DE CIRURGIA REFRATIVA Fundada em 01 de junho de 1942 CODEN: RBOFA9 Indexada nas bases de dados: SciELO Scientific Electronic Library OnLine WEB OF SCIENCE www.freemedicaljournals.com Disponível eletronicamente: www.sboportal.org.br LILACS Literatura Latino-americana em Ciências da Saúde Coordenação de Aperfeiçoamento de Pessoal de Nível Superior http://www.capes.gov.br Publicação bimestral Rev Bras Oftalmol, v. 74, n. 4, p. 197-268, Jul./Ago. 2015 Contents - Sumário Editorial 201 Triamcinolone for diabetic retinopathy Triancinolona no tratamento da retinopatia diabética Otacílio de Oliveira Maia Júnior Originals Articles 203 Prevalence of adenoviral conjunctivitis at the ophthalmologic clinic on municipality of Viçosa/MG Prevalência de conjuntivite adenoviral em clínica oftalmológica no município de Viçosa/MG Euldes Nei Rosado-Filho, Silvia Almeida Cardoso, Lorena Nacif Marçal, Eliziária Cardoso dos Santos, Eduardo de Almeida Marques da Silva, Sérgio Oliveira de Paula, Leandro Licursi de Oliveira 209 Life quality of low-vision elderly people: before and after hearing and speech intervention Qualidade de vida de idosos com baixa visão adquirida: pré e pós intervenção fonoaudiológica Mayla Myrina Bianchim Monteiro , Keila Miriam Monteiro de Carvalho 216 Health and vision related quality of life among patients with choroidal neovascular age related macular degeneration Qualidade de vida relacionada com a visão em doentes com degeneração macular relacionada à idade neovascular Maria Picoto, José Galveia, Sara Patrício, António Rodrigues, Fernanda Vaz 222 Chalazion and demographic characteristics of patients in a population sample Calázio e características demográficas dos portadores em uma amostra populacional Marjorie Fornazier do Nascimento, Ana Claudia Viana Wanzeler, Roberta Lilian Fernandes Sousa, Larissa Horikawa Satto, Carlos Roberto Padovani, Silvana Artioli Schellini 200 225 Correlation between the use of the accommodation and symptoms of asthenopia in hyperopic patients Correlação entre o uso da acomodação e sintomas de astenopia em pacientes hipermétropes Juan Carlos Luna da Costa , Ian Beltrão de Sá Martins, Larissa Tavares Albuquerque Nóbrega, Maria Odília Navarro Medeiros, Luciana Maria Palitot, Marília Bezerra Cavalcanti Dias, Tarcízio José Dias 231 Eyelid disorders: frequency of occurrence and profile of carriers in a Brazilian population sample Alterações palpebrais: frequência de ocorrência e perfil dos portadores em amostra populacional brasileira Ana Cláudia Viana Wanzeler, Marjorie Fornazier do Nascimento, Roberta Lilian Fernandes Sousa, Carlos Roberto Padovani, Silvana Artioli Schellini 235 Patient’s perception on glaucoma and different types of treatment (medical versus surgical treatment) Percepção dos pacientes portadores de glaucoma sobre sua doença e os diferentes tipos de tratamento (clínico versus cirúrgico) Augusto Alves Pinho Vieira, Ricardo Augusto Paletta Guedes, Rita de Cássia Padula Alves Vieira, Vanessa Maria Paletta Guedes Case Report 241 X-linked juvenile retinoschisis Retinosquise juvenil ligada ao X Cesar Gomes da Silveira, Gabriela Hertz Soares, Jacqueline Provenzano 244 Atypical presentation of Graves’ ophthalmopathy Apresentação atípica da oftalmopatia de Graves Flávia Marques Rodrigues, Nilson Lopes da Fonseca Junior, José Ricardo Carvalho Lima Rehder , Celso Lopez Fernandez, Debora Mayumi Sugano 248 Retro-orbital tumor suggestive of optic nerve sheath meningocele Tumoração retroorbitária sugestiva de meningocele da bainha do nervo óptico Michelle Rodrigues Gonçalves Dias Chaves, Isabella Bezerra Wanderley de Queiroga, Mario Augusto Pereira Dias Chaves, Fernando Melo Gadelha, Debora Apolônio Vieira 251 Macular granuloma due to tuberculosis without pulmonary symptoms Granuloma macular por tuberculose sem manifestação pulmonar Albert Costa Rebello, João Helio Leonardo de Sousa, José Gilberto de Sá, Karime Kalif de Sousa Rebello 254 Irreversible visual loss after use of Paclitaxel Perda visual irreversível após uso de Paclitaxel Maria Helena Lopes Amigo, Paulo Falabella, Ângela Bettarello, Wagner Ghirelli Review Article 257 Biomarkers and surrogate endpoints in the glaucomatous optic neuropathy: new developments and a review Biomarcadores e desfechos substitutos na neuropatia óptica glaucomatosa: novos desenvolvimentos e uma revisão Niro Kasahara Instruções aos autores 266 Normas para publicação de artigos na RBO EDITORIAL 201 Triamcinolone for diabetic retinopathy Triancinolona no tratamento da retinopatia diabética T he current therapeutic approach to diabetic retinopathy, based on the high level of scientific evidence, includes drugs administered via intraocular injection into the vitreous cavity associated or not to laser photocoagulation of the retina, besides a multidisciplinary approach for systemic metabolic control. The treatment is indicated in the proliferative form of the disease and/or diabetic macular edema (the main cause of visual loss). The ETDRS - Early Treatment Diabetic Retinopathy Study – has defined the laser treatment strategies in the diabetic retinopathy according to the classification, assessing the effects of panphotocoagulation at earlier stages and macular photocoagulation for macular edema1,2. As for drugs, we have some available for exclusive use in the eye (ranibizumab and aflibercept) and the ones used in an “off label” way with extensive global experience as for the effectiveness (triamcinolone and bevacizumab). Invariably, patients are involved in the discussion about the choice of drug, convenience, power, cost and side effects. Among them, an important factor for access to treatment is the cost, being it the great competitive advantage of the “off label” drugs. The triamcinolone approach in this editorial is due to our view that it is an excellent treatment choice for selected patients due to the properties it has regarding the pathophysiology of diabetic retinopathy, in addition to the low cost of application. It is believed that the mechanism of action of triamcinolone in diabetic retinopathy produces an antiinflammatory effect not only by reducing cellular mediators of inflammation, but also by stabilizing the blood-retinal barrier3,4. On the other hand, the diabetic macular edema is thought to be a multifactorial disease with the action of inflammatory and VEGF (Vascular Endothelial Growth Factor) factors. Studies have shown the superiority of anti-VEGF vs Laser, and currently there is pharmacological treatment indication of the diabetic macular edema in patients with an edema involving the center of the macula, defined as the central subfield thickness e” 250 microns and as visual acuity as Snellen equivalent of 20/32 to 20/3205. However, evidence has shown that interleukin 8 (IL-8) may play an important role in cases refractory to anti-VEGF, and that triamcinolone could be an option for said cases. The presence of IL-8 supports the hypothesis that non-responsive patients to anti-VEGF seem to have the preponderance of inflammatory effects in the genesis of the macular edema. Joen et al. showed low levels of VEGF in the aqueous humor at the moment of injection of triamcinolone, inferring that only the reduction of VEGF was not enough to cure the macular edema6. The DRCR net group in a phase 3 study did not observe any difference in the visual acuity between intravitreal triamcinolone plus laser treatment (n=203) and laser monotherapy (n=186) after one year. However, the subgroup of pseudophakic eyes treated with triamcinolone and laser showed better results in the visual acuity compared to only laser7. Another study in this group showed a similar effect of triamcinolone and ranibizumab in pseudophakic patients or with minimal change of crystalline8. Thus, triamcinolone can be considered the drug of first choice in patients with pseudophakic diabetic macular edema and who did not present ocular hypertension and/or glaucoma9. Pioneering studies showed a favorable effect of intravitreal triamcinolone as an adjuvant to the laser treatment in patients with proliferative diabetic retinopathy and macular edema in relation to those treated only with laser therapy10,11. This finding was confirmed in a multicenter study of DRCR net, and currently the triamcinolone may be an option in patients with proliferative diabetic retinopathy and macular edema undergoing laser treatment12. Recently, it was demonstrated that not only triamcinolone raises the intraocular pressure (IOP). Continuous treatment with ranibizumab may increase the risk of raising the IOP or the need for an ocular hypotensive13. We must be judicious regardless of the drug chosen and conduct a closer post operative evaluation. While most of these complications are transient and/or treatable, the retinologist must consider them when assessing the risks and benefits of the treatment, and it is important to report to the patients the possibility of adverse effects of these medications. Therefore, the use of triamcinolone in diabetic retinopathy can be considered in selected patients, and a careful analysis of cost-effectiveness is imperative for adhesion to the treatment. It gives a more universal access to the drug benefits in the treatment of this multifactorial disease. Otacílio de Oliveira Maia Júnior Assistant at São Rafael Hospital – Monte Tabor Foundation, Salvador – BA. Rev Bras Oftalmol. 2015; 74 (4): 201-2 202 Maia Júnior OO REFERENCES 1. Treatment techniques and clinical guidelines for photocoagulation of diabetic macular edema. Early Treatment Diabetic Retinopathy Study Report Number Early Treatment Diabetic Retinopathy Study Research Group. Ophthalmology. 1987;94(7):761-74. 2. Techniques for scatter and local photocoagulation treatment of diabetic retinopathy: Early Treatment Diabetic Retinopathy Study Report no. 3. The EarlyTreatment Diabetic Retinopathy Study Research Group. Int Ophthalmol Clin. 1987;27(4):254-64. 3.Wilson CA, Berkowitz BA, Sato Y, Ando N, Handa JT, de Juan E Jr. Treatment with intravitreal steroid reduces blood-retinal barrier breakdown due to retinal photocoagulation. Arch Ophthalmol. 1992;110(8):1155-9. 4. Funatsu H, Noma H, Mimura T, Eguchi S, Hori S. Association of vitreous inflammatory factors with diabetic macular edema. Ophthalmology. 2009;116(1):73-9. 5. Wells JA, Glassman AR, Ayala AR, et al; Diabetic Retinopathy Clinical Research Network. Aflibercept, bevacizumab, or ranibizumab for diabetic macular edema. N Engl J Med. 2015;372(13):1193-203. 6. Jeon S, Lee WK. Effect of intravitreal triamcinolone in diabetic macular edema unresponsive to intravitreal bevacizumab. Retina. 2014;34(8):1606-11. 7. Diabetic Retinopathy Clinical Research Network, Elman MJ, Aiello LP, Beck RW, Bressler NM, Bressler SB, Edwards AR, Ferris FL 3rd, Friedman SM, Glassman AR, Miller KM, Scott IU, Stockdale CR, Sun JK. Randomized trial evaluating ranibizumab plus prompt or deferred laser or triamcinolone plus prompt laser for diabetic macular edema. Ophthalmology. 2010 Jun;117(6):1064-1077.e35. 8. Elman MJ, Bressler NM, Qin H, Beck RW, Ferris FL 3rd, Friedman SM, GlassmanAR, Scott IU, Stockdale CR, Sun JK; Diabetic Retinopathy Clinical Research Network. Expanded 2-year follow-up of ranibizumab plus prompt or deferred laser or triamcinolone plus prompt laser for diabetic macular edema. Ophthalmology. 2011;118(4):609-14. 9. Dewan V, Lambert D, Edler J, Kymes S, Apte RS. Cost-effectiveness analysis of ranibizumab plus prompt or deferred laser or triamcinolone plus prompt laser for diabetic macular edema. Ophthalmology. 2012;119(8):1679-84. 10. Bandello F, Polito A, Pognuz DR, Monaco P, Dimastrogiovanni A, Paissios J. Triamcinolone as adjunctive treatment to laser panretinal photocoagulation for proliferative diabetic retinopathy. Arch Ophthalmol. 2006;124(5):643-50. 11. Maia OO Jr, Takahashi BS, Costa RA, Scott IU, Takahashi WY. Combined laser and intravitreal triamcinolone for proliferative diabetic retinopathy and macular edema: one-year results of a randomized clinical trial. Am J Ophthalmol. 2009;147(2):291-7 e2. 12. Diabetic Retinopathy Clinical Research Network, Googe J, Brucker AJ, Bressler NM, Qin H, Aiello LP, Antoszyk A, Beck RW, Bressler SB, Ferris FL 3rd, Glassman AR, Marcus D, Stockdale CR. Randomized trial evaluating short-term effects of intravitreal ranibizumab or triamcinolone acetonide on macular edema afterfocal/grid laser for diabetic macular edema in eyes also receiving panretina photocoagulation. Retina. 2011 Jun;31(6):1009-27. 13. Bressler SB, Almukhtar T, Bhorade A, Bressler NM, Glassman AR, Huang SS, Jampol LM, Kim JE, Melia M; for the Diabetic Retinopathy Clinical Research Network Investigators. Repeated intravitreous ranibizumab injections for diabetic macular edema and the risk of sustained elevation of intraocular pressure or the need for ocular hypotensive treatment. JAMA Ophthalmol. 2015 Feb 26. doi:10.1001/ jamaophthalmol.2015.186. [Epub ahead of print] Rev Bras Oftalmol. 2015; 74 (4): 201-2 ORIGINAL ARTICLE 203 Prevalence of adenoviral conjunctivitis at the ophthalmologic clinic on municipality of Viçosa/MG Prevalência de conjuntivite adenoviral em clínica oftalmológica no município de Viçosa/MG Euldes Nei Rosado-Filho1, Silvia Almeida Cardoso2, Lorena Nacif Marçal3, Eliziária Cardoso dos Santos3, Eduardo de Almeida Marques da Silva4, Sérgio Oliveira de Paula4, Leandro Licursi de Oliveira4, ABSTRACT Objective: The aim of this study was to evaluate the prevalence of Adenovirus as a etiologic agent of conjunctivitis on a ophthalmic clinic in Viçosa, Minas Gerais, Brazil. Methods: Samples of conjunctival secretion from 91 patients clinically diagnosed with conjunctivitis were subjected to polymerase chain reaction (PCR) using degenerate primers targeted to the gene encoding the structural protein II. Positive samples were subsequently subjected to sequencing and genotyping. Results: PCR results showed 36.3% prevalence of Adenovirus. No differences between the sexes and was found to be higher in the age group 26-65 years with 60.60% of the positive cases. Sequencing of positive cases showed the presence of Adenovirus serotypes 3, 4, 7, 8, and 34 circulating in the region. Conclusion: In Viçosa two in five cases of conjunctivitis has Adenovirus as etiologic agent. Keywords: Virology; Adenovirus/epidemiology; Conjunctivitis viral/etiology; Conjunctivitis viral/diagnosis; Polimerase chain reaction RESUMO Objetivo: O objetivo deste estudo foi avaliar a prevalência de Adenovirus como agente etiológico da conjuntivite, em clínica médica oftalmológica especializada, em Viçosa, Minas Gerais, Brasil. Métodos: Amostras da secreção conjuntival de 91 pacientes clinicamente diagnosticados com conjuntivite foram submetidas à reação em cadeia da polimerase (PCR) utilizando primers degenerados para a região codificadora do gene da proteína estrutural II. Posteriormente as amostras positivas foram submetidas a sequenciamento e genotipagem. Resultados: A análise dos resultados de PCR revelou prevalência de 36,3% de Adenovirus. Não havendo distinção entre os sexos e com maior prevalência na faixa etária de 26 a 65 anos com 60,60% dos casos positivos. O sequenciamento dos casos positivos por Adenovirus revelaram a presença dos sorotipos 3, 4, 7, 8 e 34 circulante na região. Conclusão: No município de Viçosa, dois em cada cinco casos de conjuntivite são de etiologia adenoviral. Descritores: Virologia; Adenovirus/epidemiologia; Conjuntivite viral/etiologia; Conjuntivite viral/diagnóstico; Reção em cadeia da polimerase 1 2 3 4 Department of General Biology, Federal University of Viçosa – UFV – Viçosa (MG), Brazil. Department of General Biology Department of General Biology, Federal University of Viçosa – UFV – Viçosa (MG), Brazil. Department of General Biology, Federal University of Viçosa – UFV – Viçosa (MG), Brazil. Department of General Biology Associate Professor, Federal University of Viçosa – UFV – Viçosa (MG), Brazil. Department of General Biology Study conducted at the Federal University of Viçosa – UFV – Viçosa (MG), Brazil. The authors declare no conflists of interest Received for publication 29/10/2012 - Accepted for publication 28/01/2013 Rev Bras Oftalmol. 2015; 74 (4): 203-8 204 Rosado-Filho EN, Cardoso SA, Marçal LN, Santos EC, Silva EAM, Paula SO, Oliveira LL INTRODUCTION METHODS onjunctivitis is considered one of the most common disorders of ophthalmic emergency worldwide (1). It has viruses and bacteria as its main etiologic agents, is highly contagious and can occur in outbreaks(2,3). The viral conjunctivitis has in most cases the adenovirus (AdVs) as the causative agent, which are viruses with double-stranded DNA, non-enveloped, lytic and with icosahedral morphology. There are more than 55 AdVs serotypes already identified. They are classified into seven distinct groups (AdV A-F), based on their biological phytochemical, and genetic characteristics(4). Adenoviral conjunctivitis cases are caused most often by AdV3 (AdV-B), AdV -4 (AdV-E), AdV -8, -19a, -37, -53, and -54 (AdV-D) (4, 5). Conjunctivitis can also be caused by other viruses such as Herpes Virus, Coxsackievirus, Rhinovirus, Echovirus, Enterovirus, Molluscum Contagiosum Virus, among others. The Enterovirus 70 and Coxsackievirus A4 are both related to the hemorrhagic form of viral conjunctivitis(6). Most eye disorders secondary to the infection with Adenovirus are presented in the form of simple follicular conjunctivitis, faringoconjuntival fever and epidemic keratoconjunctivitis. Simple follicular conjunctivitis is usually selflimited, transitory and non-associated to systemic dysfunctions(7). The serotypes 1 to 11 and 19 are the primary cause of nonspecific follicular conjunctivitis(8-10). Faringoconjuntival fever, most commonly caused by serotypes 3, 4, 5 and 7 of the Adenovirus, is characterized by fever, headache, pharyngitis, follicular conjunctivitis, and preauricular adenopathy. In some isolated cases, the systemic signs can mimic an infection caused by the influenza virus(11,12). The epidemic keratoconjunctivitis is often caused by serotypes 8, 19 and 37 of group AdV-D, with significant involvement of the cornea. In most patients it is presented in the bilateral form, preceded by upper respiratory tract infection(13). The assessment of systemic signs associated with precise molecular biology techniques is key for the clinical diagnosis and prevention of epidemics during the acute phase of adenoviral conjunctivitis (3) . Some of the most important conventional techniques for the clinical diagnosis of viral conjunctivitis include, among others, cytological investigation of the conjunctiva, assessment of the cytopathic effect in susceptible cell lines, detection of antigens in the cells of conjunctiva by direct fluorescence or detection of antibodies. Despite the sensitivity of detection of the same, these techniques are time consuming and costly from an economic point of view, what becomes a challenge for detection and a rapid diagnosis of AdV as caused by conjunctivitis. Other important, relatively simple, fast, highly sensitive and low cost diagnostic method which has been used a lot in the last decade is the polymerase chain reaction (PCR)(13-16). Considering the importance of accuracy of early diagnosis and specific treatment of adenoviral conjunctivitis, the objective of the present study is to evaluate the frequency of Adenovirus in the conjunctival secretion of the patients assisted in eye clinic located in the municipality of Viçosa, Minas Gerais, Brazil, in the period from May 2009 to January 2011, using PCR as the technique. This is a cross-sectional study on patients assisted in a specialized eye clinic located in the municipality of Viçosa-MG, in the period from May 2009 to January 2011. A total of 91 patients of both genders aged between 1 and 74 years with symptoms indicative of viral conjunctivitis (hyperemic eyes, watery discharge and discomfort) underwent ocular inspection followed by thorough ophthalmologic assessment. After assessment, patients with diffuse conjunctival hyperemia presenting ocular discomfort, palpebral edema and tearing with watery secretion, follicular reaction in the tarsal conjunctiva, satellite lymphadenopathy and keratitis with multiple sub-epithelial infiltrates were considered as possible cases of conjunctivitis of adenoviral etiology. After the diagnosis confirmation, the patients were informed about the possibility of Adenovirus prevalence as the causative agent of the disease, and were invited to participate in a clinical research for the detection of the same. The 91 patients who volunteered signed a written consent to participate in the study after being aware of the clinical implications of the same. The principles of Bioethics were guaranteed to all participants, according to regulation 196/96 of the National Health Council determining the ethical aspects necessary for conducting research in humans (CEPH-167741). Subsequently, a conjunctival secretion was collected from the anterior eyeball of each patient with aid of a sterile rayon swab soaked in solution of 0.9% sodium chloride, using slit lamp (Topcon 3E). The material obtained was placed in sterile 1.5 ml polypropylene tubes previously identified and containing phosphate buffered saline solution (PBS), and freezed for subsequent viral DNA extraction, PCR and gene sequence analysis for the identification of the serotype responsible for the infection. The viral DNA of all samples of conjunctival secretion supposedly infected by Adenovirus have been extracted using a specific kit for viral RNA and DNA extraction (QIAamp UltraSens Virus-Quiagen). The extraction was carried out according to the manufacturer’s instructions. Then, 500mL of sample were treated with 500mL of buffer AR and 20mL of proteinase K, and incubated at 40°C for 10 min. Later 300mL of buffer AB were added and the material was applied to a QIAamp affinity column, washed and eluted with 30mL of buffer AVE. The eluted material was used for the PCR reactions; samples of patients with a healthy conjunctiva and with no sign of infection were used as negative control. The total DNA extracted was then subjected to PCR using degenerate primers hex1deg (5’-GCC (C,G)CA (AG)TG G(G,T)C (A,T)TA CAT GCA CAT C-3’) with 25 nucleotides and hex2deg (5’-CAG CAC (C,G)CC (A,T,C,G)GG (A,G)AT GTC AAA-3’) with 21 nucleotides(17). The primers generate an amplicon between position 21 and 322 of the coding region of the structural gene II protein, which is sensitive to multiple serotypes of Adenovirus to amplify a fragment of approximately 301 bp of DNA. The PCR reaction was processed in a thermocycler (Mastercycler, Eppendorf) using the following parameters: 1 cycle at 94°C for 2 min. (denaturing) followed by 30 cycles of 94°C for 30 seconds (denaturing), 55°C for 30 seconds (annealing) and 72°C for 30 seconds (synthesis) and 1 cycle of 72°C for 10 minutes (extension). The PCR reaction product was subjected to electrophoresis on 1.5% agarose gel containing 1.0 µg/mL of red gel (Uniscience) using Read-load 100pb DNA C Rev Bras Oftalmol. 2015; 74 (4): 203-8 Prevalence of adenoviral conjunctivitis at the ophthalmologic clinic on municipality of Viçosa/MG Ladder as a standard molecular marker (Invitrogen, LT) with 60 mV for approximately 1.5 hours as sieving parameters. After the electrophoresis sieving the gel was visualized under a UV irradiation chamber and with digital photo documentation. The bands of the positive samples confirmed by electrophoresis were cut out of the gels and subjected to sequencing for confirmation of identity of the viral isolate. Sequencing was performed on ABI Prism 377 DNA Sequencer device according to the Protocol described in the kits used (Templiphi DNA amplification, Amersham Biosciences; Big DyeTM Terminator Cycle Sequencing Ready Reaction, PE Applied Biosystems). The nucleotide sequences obtained were aligned with the aid of the program CAP 3 to obtain the final consensus sequence of viral DNA. The identity was analyzed using the Blast program of the ‘National Center for Biotechnology Information’ (NCBI) (http://www.ncbi.nlm.nih.gov). The alignment of the consensus sequences was performed by the program Multalin (INRA) (http://prodes.toulouse.inra.fr/multalin/multalin.html). 205 60.60% of cases confirmed (Figure 2B). There was a high incidence of confirmed cases by Adenovirus in children under two years of age (75%). RESULTS Of the 91 patients clinically diagnosed with conjunctivitis and who had the conjunctival secretion collected for analysis, 36.3% (33) of the cases were confirmed as having conjunctivitis from adenoviral source. The distribution of positive cases in the PCR analysis during the study was more prevalent between May and June 2009, a period in which there was an outbreak of the disease in the city. The presence of Adenovirus in the secretions collected from patients was also found considerable in the months of February, November, December 2010, and in a lesser proportion in January 2011 (Figure 1). Figure 2: Prevalence of conjunctivitis cases according to sex (A) and age (B). Figure 1: Distribution of conjunctivitis cases from May 2009 to January 2011. The samples were tested by PCR for positive or negative reaction to the detection of Adenovirus in conjunctival swabs. The prevalence of adenoviral conjunctivitis, when compared between genders in the period of the study, was a little different, and the percentage of women and men with the disease confirmed represented 55.17% and 45.83% respectively (Figure 2A). Regarding the distribution of conjunctivitis cases by age group, a higher prevalence among individuals in the economically active age group (26 to 65 years) was observed, accounting for Regaring the different serotypes of Adenovirus as causative of conjunctivitis in the municipality, serotypes 3, 4, 7, 8 and 34 were identified in the samples from confirmed cases (Figure 3A). Of these, serotype 8 proved to be more prevalent with approximately 33.33% of the cases evaluated, followed by serotype 4 with 25%, serotype 7 presented 17% and serotypes 3 and 34 presented less than 10% of cases. Other unidentified serotypes in the sequencing (8.33%) were also detected in the period of the study (Figure 3A). Regarding the group of Adenovirus as causative of conjunctivitis, groups B and D presented 33.33% of cases each, followed by group E with 25% of cases; groups A, C and F were not found in the present study, and 8.33% of non-identified Adenovirus were group NI (Figure 3B). The signs and symptoms presented by patients during the detailed ophthalmic assessment before the collection and analysis of conjunctival secretion were used to supplement the laboratory detection diagnosis of Adenovirus in the secretions analyzed (table 1). All patients assessed (91 cases) had ocular hyperemia and tearing, common signs of conjunctivitis. When the signs and symptoms strongly related to adenoviral conjunctivitis were analysed, it was found that patients with satellite lymphadenopathy 66.67% (22 cases), conjunctival chemosis 81.82% (27 cases) and nummular keratitis 75.76% (25 cases) were more expressive in the cases confirmed of adenoviral conjunctivitis. Rev Bras Oftalmol. 2015; 74 (4): 203-8 206 Rosado-Filho EN, Cardoso SA, Marçal LN, Santos EC, Silva EAM, Paula SO, Oliveira LL Figure 3: Identification of the etiological agent causative of adenoviral conjunctivitis. Serotypes identified by sequencing (A). Prevalence of conjunctivitis causative groups (B). Table 1 Evaluation of frequency of conjunctivitis symptoms Non-adenoviral conjunctivitis Signs and symptoms Ocular hyperemia Tearing Serous secretion Purulent secretion Satellite lymphadenopathy Conjunctival chemosis Conjunctival membrane Subconjunctival haemorrhage Discomfort Moderate pain Severe pain Corneal wound Nummular keratitis Fever General malaise Nº cases (n=58) % Nº cases (n=33) 58 58 51 3 12 21 3 3 35 18 0 1 7 7 22 100.00 100.00 87.93 5.17 20.69 36.21 5.17 5.17 60.34 31.03 0.00 1.72 12.07 12.07 37.93 33 33 32 1 22 27 7 7 15 11 7 4 25 6 16 DISCUSSION It is established in the scientific literature that Adenovirus is responsible for epidemic outbreaks of conjunctivitis worldwide, affecting all age groups in varied chronology and in different orders of gravity (18-20). The early diagnosis and efficacy in controlling the infection is a key process to minimize the incidence of the disease(17,20). One of the methods considered as gold standard to detect Adenovirus is the qPCR and the real-time PCR due to the fast analysis, high sensitivity and precision on molecular identification of the different serotypes involved in ocular disease (20-22). According to Allard et al. degenerate primers for the coding region of the structural protein gene II of Adenovirus has been shown to be effective in highlighting different serotypes of AdVs in epidemiological studies(17). Considering these findings, the PCR reaction using these primers was the method used to analyze the frequency and detect different serotypes causative of adenoviral Rev Bras Oftalmol. 2015; 74 (4): 203-8 Adenoviral conjunctivitis % ‘100.00 100.00 96.97 3.03 66.67 81.82 21.21 21.21 45.45 33.33 21.21 12.12 75.76 18.18 48.48 conjunctivitis in the municipality of Viçosa/MG in the period from May 2009 to January 2011 without the need of culture of viral isolation. The prevalence of positive samples analyzed for adenoviral conjunctivitis was 36.3% in the present study. Previous studies have demonstrated prevalence ranging from 15%(23), 70%(24), and 82%(20). Different environmental factors may be related to these discrepancies. Scientific literature has reported differences in the seasonality for the emergence of Adenovirus as a causative agent of conjunctivitis worldwide. According to Matsui et al. in a study conducted in Japan, Adenovirus keeps a low frequency throughout the year; however an outbreak was reported in September(20). Another study by Maranhão et al. in Brazil which was related to the seasonal distribution of eye infections by AdV in the years from 2004 to 2007 showed the occurence of only one outbreak in April 2004, with no constancy over the years of study(3). The present study presented the differences in relation Prevalence of adenoviral conjunctivitis at the ophthalmologic clinic on municipality of Viçosa/MG to this seasonal distribution, and AdV was more frequent in the months of May and June, a period of disease outbreak in the city. A possible explanation for said differences may be related to weather conditions, because a higher prevalence of cases has occurred in early winter. Allard et al. analyzed secretion samples from 40 patients with clinical symptoms of conjunctivitis caused by AdV considering the age of the patients, and they found a very heterogeneous distribution, with a frequency ranging from 9 months to 74 years of age(17). This finding is in agreement with our approach, despite the higher frequency of cases in this study has occurred in the age group between 26 and 65 years. In order to determine the serotypes present in the samples confirmed of adenoviral conjunctivitis, the PCR products were characterized by sequencing(17). There was a predominance of serotype 8 (33.33%), followed by 4 (25%) associated to keratitis, as well as in the study of Jin et al. in Hanoi, Vietnam(25). The presence of serotype 7 (17%) brought particular concern, since this serotype has been associated to more severe cases of infection by Adenovirus, such as pneumonia and myocarditis, with a possible adverse development to respiratory and cardiovascular failure(5). The main clinical symptoms presented by the patients with conjunctivitis were ocular hyperemia, serous secretion and tearing. Patients with adenoviral conjunctivitis showed a greater frequency of satellite lymphadenopathy, conjunctival chemosis and nummular keratitis. Keratitis usually appear on the 5th day after the onset of conjunctivitis, followed by the rise of corneal nummular opacity on day 7, as it is reported by various authors (26,27). 4. 5. 6. 7. 8. 9. 10. 11. 12. CONCLUSION 13. The present study revealed that in Viçosa two out of five cases of conjunctivitis are of adenoviral etiology. Considering the possibility of adenoviral conjunctivitis outbreaks throughout the year, and the different serotypes that can lead to eye disease, the study highlights the importance of conducting rapid diagnostic tests such as PCR for the recognition of the serotype and specific treatment as a potential measure to reduce the virus and consequently the potential for transmission. 14. ACKNOWLEDGEMENTS The funding agencies: the State of Minas Gerais Research Support Foundation (FAPEMIG) and the National Council of Scientific and Technological Development (CNPq). 15. 16. 17. 18. 19. REFERENCES 1. 2. 3. Adlhoch C, Schöneberg I, Fell G, Brandau D, Benzler J. Increasing case numbers of adenovirus conjunctivitis in Germany, 2010. Euro Surveill. 2010;15(45):pii: 19707. González-Sotero J, Rojas-Álvarez E, Correa-Rojas O, IviricuTielves R. Resistencia antimicrobiana en oftalmología. Rev Mex Oftalmol. 2011;85(3):148-55. Maranhão AG, Soares CC, Albuquerque MC, Santos N. Molecular epidemiology of adenovirus conjunctivitis in Rio de Janeiro, 20. 21. 22. 207 Brazil, between 2004 and 2007. Rev Inst Med Trop Sao Paulo. 2009;51(4):227-9. Aoki K, Kaneko H, Kitaichi N, Ohguchi T, Tagawa Y, Ohno S. Clinical features of adenoviral conjunctivitis at the early stage of infection. Jpn J Ophthalmol. 2011;55(1):11-5. Robinson CM, Shariati F, Zaitshik J, Gillaspy AF, Dyer DW, Chodosh J. Human adenovirus type 19: genomic and bioinformatics analysis of a keratoconjunctivitis isolate. Virus Res. 2009;139(1):122-6. Flint SJ, Enquist LW, Racaniello VR, Skalka AM. Principles of virology: molecular biology, pathogenesis, and control of animal viruses. 2nd ed. Washington: ASM Press; 2003. Weber CM, Eichenbaum JW. Acute red eye. Differentiating viral conjunctivitis from other, less common causes. Postgrad Med. 1997;101(5):185-6, 189-92, 195-6. Comment in Postgrad Med. 1997;102(3):63-4. Takeuchi S, Itoh N, Uchio E, Aoki K, Ohno S. Serotyping of adenoviruses on conjunctival scrapings by PCR and sequence analysis. J Clin Microbiol. 1999;37(6):1839-45. Weiss A, Brinser JH, Nazar-Stewart V. Acute conjunctivitis in childhood. J Pediatr. 1993;122(1):10-4. Wood SR, Sharp IR, Caul EO, Paul I, Bailey AS, Hawkins M, et al. Rapid detection and serotyping of adenovirus by direct immunofluorescence. J Med Virol. 1997;51(3):198-201. Bell JA, Rowe WP, Engler JI, Parrott RH, Huebner RJ. Pharyngoconjunctival fever; epidemiological studies of a recently recognized disease entity. J Am Med Assoc. 1955;157(13):1083-92. Weiss A. Acute conjunctivitis in childhood. Curr Probl Pediatr. 1994;24(1):4-11. Review. Elnifro EM, Cooper RJ, Klapper PE, Bailey AS, Tullo AB. Diagnosis of viral and chlamydial keratoconjunctivitis: which laboratory test? Br J Ophthalmol. 1999;83(5):622-7. Review. Allard A, Girones R, Juto P, Wadell G. Polymerase chain reaction for detection of adenoviruses in stool samples. J Clin Microbiol. 1990;28(12):2659-67. Erratum in J Clin Microbiol. 1991;29(11):2683. Pring-Akerblom P, Adrian T. Type- and group-specific polymerase chain reaction for adenovirus detection. Res Virol. 1994;145(1):25-35. Van Rij G, Klepper L, Peperkamp E, Schaap GJ. Immune electron microscopy and a cultural test in the diagnosis of adenovirus ocular infection. Br J Ophthalmol. 1982;66(5):317-9. Allard A, Albinsson B, Wadell G. Rapid typing of human adenoviruses by a general PCR combined with restriction endonuclease analysis. J Clin Microbiol. 2001;39(2):498-505. Cheung D, Bremner J,Chan JT. Epidemic keratoconjunctivitis—do outbreaks have to be epidemic? Eye (Lond). 2003;17(3):356-63. Matsui K, Saha S, Saitoh M, Mizuki N, Itoh N, Okada E, et al. Isolation and identification of adenovirus from conjunctival scrapings over a two-year period (between 2001 and 2003) in Yokohama, Japan. J Med Virol. 2007;79(2):200-5. Matsui K, Shimizu H, Yoshida A, Nagaoka E, Nishio O, Okuda K. Monitoring of adenovirus from conjunctival scrapings in Japan during 2005—2006. J Med Virol. 2008;80(6):997-1003. Cooper RJ, Yeo AC, Bailey AS, Tullo AB. Adenovirus polymerase chain reaction assay for rapid diagnosis of conjunctivitis. Invest Ophthalmol Vis Sci. 1999;40(1):90-5. Heim A, Ebnet C, Harste G, Pring-Akerblom P. Rapid and quantitative detection of human adenovirus DNA by real-time PCR. Rev Bras Oftalmol. 2015; 74 (4): 203-8 208 Rosado-Filho EN, Cardoso SA, Marçal LN, Santos EC, Silva EAM, Paula SO, Oliveira LL J Med Virol. 2003;70(2):228-39. Erratum in J Med Virol. 2003;71(2):320. 23. Aoki K, Tagawa Y. A twenty-one year surveillance of adenoviral conjunctivitis in Sapporo, Japan. Int Ophthalmol Clin. 2002;42(1):49-54. 24. Mejía-López H, Matías-Florentino M, Vélez-Montoya R. [Identification of adenovirus associated with conjunctivitis by molecular methodology]. Arch Soc Esp Oftalmol. 2006;81(7):37582. Spanish. 25. Jin XH, Ishiko H, Nguyen TH, Ohguchi T, Akanuma M, Aoki K, et al. Molecular epidemiology of adenoviral conjunctivitis in Hanoi, Vietnam. Am J Ophthalmol. 2006;142(6):1064-6. Rev Bras Oftalmol. 2015; 74 (4): 203-8 26. Durand M, Weber DJ, Rutala WA. Nosocomial ocular infections. In: Mayhall CG,editor. Hospital epidemiology and infection control. 3rd ed. Baltimore: Lippincott, Williams & Wilkins; 2004. 27. Melendez CP, Florentino MM, Martinez IL, Lopez HM. Outbreak of epidemic keratoconjunctivitis caused by adenovirus in medical residents. Mol Vis. 2009;15:557-62. Corresponding author Leandro Licursi de Oliveira Av. PH Rolfs, s/n Campus Universitário ZIP Code: 36570-000-Viçosa (MG), Brazil. E-mail: [email protected] ORIGINAL ARTICLE 209 Life quality of low-vision elderly people: before and after hearing and speech intervention Qualidade de vida de idosos com baixa visão adquirida: pré e pós intervenção fonoaudiológica Mayla Myrina Bianchim Monteiro1 , Keila Miriam Monteiro de Carvalho 2 ABSTRACT Aim: To evaluate life quality of elderly people with acquired low vision before and after hearing and speech intervention. Methods: This was a descriptive cross-sectional study. The study was made with 52 elderly people with acquired low vision. Two questionnaires that measures life quality were used in this study. The first was ‘Low Quality of Life Vision (LVQOL)’ and the second the ‘National Eye Institute Visual Function Questionnaire (NEIVFQ-25)’. The study included people with more than 60 years with acquired low vision and who accepted to participate signing the consent form. The hearing and speech therapy were made into three months, one meeting a week. The questionnaires were applied in the first and last day of the intervention. Results: The age ranged between 60 and 91 years. The macular disorder (38%), such as age-related macular degeneration, macular hole and high myopia were the main causes of visual loss. Although the tests show superior performance after the intervention, there was no statistically significant difference. On the question about difficulties seeing in general, 17 participants answered that they had much more difficulty before the intervention and only 5 participants have reported having much difficulty after the intervention. Conclusion: The intervention trended to positive results, and after the meetings, participants showed improvements in aspects of the two questionnaires used in the study, decreasing the degree of difficulty in performing activities. Keywords: Quality of life; Low vision; Elderly; Questionnaire; Rehabilitation RESUMO Objetivo: Avaliar a qualidade de vida de idosos com baixa visão adquirida antes e depois de intervenção fonoaudiológica. Métodos: Foi realizado um estudo descritivo e transversal. A população do estudo foi constituída por 52 idosos com baixa visão adquirida. Dois questionários que mensuram qualidade de vida foram aplicados neste estudo. O primeiro foi “Low Quality of Life Vision” (LVQOL) e o segundo the “National Eye Institute Visual Function Questionnaire” (NEIVFQ-25). Foram incluídos na pesquisa sujeitos com mais de 60 anos, portadores de baixa visão adquirida e que assinaram o Termo de Consentimento Livre e Esclarecido. A intervenção fonoaudiológica tinha duração de três encontros, um por mês. Os questionários foram aplicados no primeiro e no ultimo dia da Intervenção. Resultados: A idade variou entre 60 e 91 anos. A alteração macular (38%), como degeneração macular relacionada à idade, buraco macular e alta miopia foram as principais causas da perda visual. Apesar dos testes mostrarem um desempenho superior após a intervenção, não houve diferença estatisticamente significativa. Na questão sobre dificuldades de ver em geral, 17 sujeitos responderam que tinham muita dificuldade antes da intervenção, e após a intervenção somente 5 sujeitos relataram ter muita dificuldade. Conclusão: A intervenção tendenciou à resultados positivos, e após os três encontros, os idosos apresentaram melhoras em aspectos avaliados nos dois questionários usados no estudo, diminuindo o grau de dificuldade na realização de atividades. Descritores: Qualidade de vida; Baixa visão; Idoso; Questionário; Reabilitação 1 2 Faculdade de Ciências Médicas, Universidade Estadual de Campinas, Campinas, SP, Brazil. Departament of Oftalmology, Faculdade de Ciências Médicas, Universidade Estadual de Campinas, Campinas, SP, Brazil. Study carried out at Subnormal Vison Ambulatory, Departament of Oftalmology, Hospital de Clinicas, Universidade Estadual de Campinas Campinas, SP, Brasil. The authors declare no conflicts of interest Received for publication 19/03/2013 - Aceito para publicação em 08/01/2014 Rev Bras Oftalmol. 2015; 74 (4): 209-15 210 Monteiro MMB , Carvalho KMM INTRODUCTION I n the last decade, life quality related to health has become an important issue and also the need of researches regarding this issue. Investigations of the conditions that allow life quality in old age and also the variations that the best age provides is getting great scientific and social importance and attention. Attempting to answer the apparent contradiction that exists between old age and wellbeing, or even the association between old age and diseases, researches may contribute towards understanding the aging process and the limits and attainability of human development. In addition to this, such investigations will give the possibility of creating alternatives for interventions aimed at promoting wellbeing at the best age(1). According to the World Health Organization (WHO) (2), health is a state of complete physical, mental and social wellbeing and not merely the absence of disease. The term “quality of life” (QOL) is the subjective perception of wellbeing and wholeness. It is a broad concept affected in a complex way by a person’s physical health, psychological state, level of independence, social relationships, and his or her relationship to the salient features of his or her environment(3). There is a need on measure the results of low-vision rehabilitation to be able to discuss the case of low-vision assessment within manage care plans, to improve services offered, and to secure and enhance funding for low-vision services(4,5). Several questionnaires were developed to measure the life quality of people with visual impairments(6). There are non disease-specific vision-related QOL instruments that include: the National Eye Institute Visual Function Questionnaires (NEIVFQ and NEIVFQ25) and the Low Vision Quality of Life (LVQOL) described by Wolffsohn and Cochrane(7). Most of the instruments contain measures that capture a combination of visual symptoms, visual physical function, performance and participation of the low vision elderly in daily activities. In vision rehabilitation, an instrument to specifically address restriction of participation (handicap) is necessary to add to measures of impairment such as visual acuity and subjective or objective measures of activity limitation (8). Patient-reported outcomes (PROs) are the measurement of patients’ perception of the impact of a disease and its treatment(s), which are typically reported by questionnaire. PROs are increasingly being accepted as the primary endpoints of clinical trials in health research. Therefore, it is critical that data collected by PROs are accurate and reliable, which is only possible when patients are able to understand the questions asked and select response categories that represent their status. Poorly understood questions, or underutilized rating scale categories can seriously impair the accuracy and reliability of PRO measurements(9,10). The role of speech therapy in the rehabilitation of visually impaired elderly aims to maintain communication, both oral and written, in full use. Some studies related that there is a decrease of written communication between the effects of visual impairment. The aim of this study was to evaluate life quality of lowvision elderly before and after Hearing and Speech Intervention. Rev Bras Oftalmol. 2015; 74 (4): 209-15 METHODS The research was conducted through longitudinal study. The study was approved by the Committee of Ethics in Research of the Faculty of Medical Sciences, State University of Campinas under the protocol number 1041/2010. The study was made with 52 elderly participants. The inclusion criteria were: participants over 60 years, according to the World Health Organization - WHO; acquired low vision (visual acuity equal or less than 6/18 (0.3), according to WHO); attended at Outpatient Low Vision/HC/UNICAMP (VSN-HCUNICAMP); with no other associated disabilities and/or mental illness; subjects who participated in three meetings called Hearing and Speech´ Intervention consecutively; participants who answered both questionnaires before and after Hearing and Speech´ Intervention; Inclusion voluntary, by signing Consent Form for the period from February 2011 to June 2012 (16 months). Two questionnaires that deal with quality of life were chosen for use in this study. The first questionnaires was the ‘Low Quality of Life Vision’ (LVQOL) which contains 25 questions specifically for low vision, and evaluated sub-items for each point analyzed, for instance, the basic aspects, mobility, adaptation, reading and working. In this study, it was used a Portuguese version, which is a result of the thesis entitled “Low Vision Elderly: Causes, Functional Status, Perceptions of Constraints and Visual Rehabilitation Unit at University Hospital” by Prof. Dr. Keila M. M. de Carvalho (11), obtained in 2007. The questionnaire consists of 23 questions. Some items from life quality questionnaire addressed to the topic of low vision, LVQOL, Low Vision Quality of Life as described by Wolffsohn and Cochrane(7), translated and subjected to changes given the local reality, were used to prepare this instrument. The second questionnaire, the VFQ-25 is a version that reliable and valid 25-item National Eye Institute. The National Eye Institute (NEI) sponsored the development of the VFQ-25 in order to create a survey that would measure the dimensions of self-reported health of vision that are most important for people who have chronic eye diseases. Based on this goal, the study measures the influence of visual disability and visual symptoms on generic health domains such as welfare and social and emotional functioning, as well as oriented tasks related to the daily visual operation (12). Simon et al investigated its reliability and validity in a group of Brazilian patients with different eye conditions in Minas Gerais. The version used in the 2008 study, was also used in this research (13). When one participant arrived at the Outpatient Low Vision/ HC/UNICAMP (VSN-HC-UNICAMP), he/she was invited to participate on the study. Once agreed, two questionnaires were applied and the three meetings were scheduled. At the end of the third meeting, both questionnaires were reapplied for comparison of responses. The questionnaires were applied by the researcher. The reading of the questionnaire was made reliably for both questionnaires. Intervention Speech was accomplished through three meetings, monthly. The meetings were conducted in groups, lasting 50 minutes. - 1st meeting: The theme was activities of daily living. Perform activities of daily living with facilitators. In this meeting, Life quality of low-vision elderly people: before and after hearing and speech intervention the researcher stressed the need of the use of communication in routine tasks like grocery shopping, taking a bus, leave a note or ask someone for some information on the street. All these activities require the use of communication, both oral and written; - 2nd meeting: The theme was the optical and non-optical aids. If the participant had the need of prescription use, frequency of use and improved vision. The optical aids had been previously prescribed by the ophthalmologist for the subjects during the consultation at the outpatient Low Vision. However, to date the intervention, some subjects had still not managed to get the aid, or saw no need to use it. Optical aids are generally used in closely activities, especially for reading. Thus at this meeting, was necessary the use of an optical aid to perform readings. - 3rd meeting: The theme of the meeting was reading and writing. The use, frequency, difficulty, use of optical and non optical aids to carry out the activities, the importance of continuing these activities. This meeting covered an important area of the Hearing and Speech Pathology. Reading and writing not only refers to writing code or decipher them, we must interpret and use them socially. During the meetings, the researcher offered new options for participants conduct their daily activities, as well answered questions regarding optical and non-optical aids and reading and writing. Patients were encouraged to discuss on the issues and also share their own experiences. Life quality was measured after the intervention to verify if it had an impact on the visual function and life quality by comparing the results obtained by the two quizzes. VEM-test was performed for question 7 and 18 and descriptive analyses was used for other data for questionnaire 1 (LVQOL). 211 For questionnaire 2 (VFQ-25) the average SCORE for each sub domain was calculated and the t-test was performed to observe if the treatment lead to an improvement of visual function and the communication. The difference between the measures before versus after the treatment were compared and values with interval equal to or greater than zero, were considered a confidence level of 95%. The choice of t-test was due to paired terms. The same test was applied to the check difference between the VEM before versus the intervention. RESULTS Seventy-one subjects were selected to participate on the study, but only fifty-two subjects participated in all phases. The participants’ age was from 60 to 91 years. Most participants were retired, and among them, 70% were retired due to visual problems. The educational level of the participants is low: 81% have primary education. The results involving issues of Q1 - LVQOL are presented below. The q7 sought to examine the degree of difficulty in performing some activities. Table 1 (q7) presents the comparison for conducting such activities before and after the intervention. The statistical test showed no significant improvement after the intervention, however, by observing the table above it is possible to infer that the VEM value to each question is a little different, there was a tendency to improvement. Despite the statistics have shown that there was no significant difference before and after the intervention, it was possible to observe an Table 1 Comparison of pre and post intervention speech: degree of difficulty performing activities of daily living (Questionnaire 1) Before Intervention Difficulty in some activities NONE (1) After Intervention A LOT (4) MEDIA FEW (2) VEM A LOT (PRE) (4) 1. To see generally? 17 26 9 0 3.2 5 2. To use vision for 22 22 8 0 3.3 23 16 14 0 3.2 MEDIA FEW (2) NONE (1) VEM (POST) 31 10 3 2.8 9 30 7 3 2.9 12 28 6 3 3.0 long time? 3. To use the night vision at home? 4. To see with glare? 17 25 10 0 3.1 16 23 7 3 3.1 5. To see street signs? 24 18 10 0 3.3 15 26 5 3 3.1 6. To watch TV? 18 23 11 0 3.1 8 31 7 3 2.9 7. Seeing objects that move? 20 23 9 0 3.2 23 18 5 3 3.2 22 11 0 3.3 24 17 5 3 3.3 25 18 9 0 3.3 26 16 4 3 3.3 24 18 10 0 3.3 23 19 4 3 3.3 26 17 9 0 3.3 25 17 4 3 3.3 8. To calculate the distance between you and an object? 29 9. To see steps or holes in the sidewalk ? 10. To walk on the neighborhood ? 11. To cross the street with traffic? Rev Bras Oftalmol. 2015; 74 (4): 209-15 212 Monteiro MMB , Carvalho KMM improvement in the items 1-5 that the VEM decreased after speech therapy and in items 7-11, the results of VEM remained the same, showing no improvement or worsening after the intervention. In the question about difficulty seen in general (item 1), 17 subjects reported that they had much more difficulty before the intervention, whereas after the intervention only 5 subjects still reported such problem. The q8 questions are about use and types of optical aids used, before and after Intervention. For better visualization, the responses to q8 are divided into two tables presented below: table 2 and table 3. Note that not all participants in the study to make use of optical aids both pre and post intervention. Table 3 Comparison of before and after intervention speech: types of optical aids used (Questionnaire 1) Table 2 Yes No Total Before Intervention 37 15 52 Before Intervention Glasses Magnifying glasses Others Do not use Total 27 10 4 15 52 After Intervention 52% 19% 8% 39% 100% 31 18 5 7 52 60% 35% 10% 14% 100% *Multiple Answers Comparison of before and after intervention speech: using optical aids (Questionnaire 1) Use of optical aids (N=52) Types of optical aids (N=52) 61% 39% 100% Q12 is questioned on the purpose of using the optical feature. The answers are manifold, because the subjects were free to choose more than one answer. On this issue there was also an increase of the activities for which the subjects are using their optical devices (Table 4). For Q18 and Q19 also statistical test was used VEM. The two questions sought to know the great difficulty performing certain activities using optical aids (Table 5). After Intervention 45 7 52 86% 14% 100% Table 4 Comparison of before and after intervention speech: intended use of the optical feature (Questionnaire 1) Intended use of the optical feature Before Intervention (N=37) To read close, yes or no? To read To watch tv, yes or no? To write, yes or no? To do manual work, yes or no? To walk on the street, yes or no? After Intervention (N=45) YES NO YES NO YES NO YES NO 27 14 15 20 19 15 10 23 31 17 18 22 73% 38% 33% 54% 51% 41% 27% 62% 67% 46% 49% 59% 36 12 15 34 30 18 9 33 31 11 15 27 80% 27% 33% 76% 67% 40% 20% 73% 67% 24% 33% 60% Table 5 Comparison of before and after intervention speech: difficulty with activities performed with optical aids (Questionnaire 1) Before Intervention Using optical aids, the degree of difficulty you have to (n=52) To read large letters in newspaper? To read text of journal or book? To read labels for medicines? To read letters? To thread the needle? To cut with scissors? To write? To read what you write? To do housework? A LOT MEDIA FEW 8 11 12 12 16 16 11 11 11 13 15 15 14 10 10 10 11 11 NONE VEM(PRE) A LOT MEDIA FEW NONE VEM (PRE) 12 8 7 8 8 8 11 12 8 For Q2 - VFQ-25 was also performed a comparison before and after the intervention. For a confidence level of 95% using the t test concluded that there is no difference in the results of the responses given by patients after treatment (p-value> 0.05). Rev Bras Oftalmol. 2015; 74 (4): 209-15 After Intervention 4 3 3 3 3 3 5 3 7 2.68 2.92 2.97 2.95 3.05 3.05 2.73 2.81 2.70 4 7 25 23 26 26 13 11 6 26 26 10 12 8 8 20 22 23 11 8 7 7 8 7 9 9 11 4 4 3 3 3 3 3 3 3 2.67 2.80 3.27 3.22 3.27 3.30 2.96 2.91 2.71 But there was a tendency to improvement, post intervention, the sub domain related to: vision (q20), psychological aspects (q3, q21, q22, q25), difficulties everyday (q17, q18), dependence (q20, q23, q24), peripheral vision (q10) (Table 6). Life quality of low-vision elderly people: before and after hearing and speech intervention 213 Table 6 Comparison of pre and post intervention speech: medium SCORE for sub domain of questionnaire 2 Sub domains VFQ (N=52) Before intervention (average) After intervention (average) 46 61 61 46 42 39 53 56 54 0 50 44 46 58 62 48 43 42 50 48 50 0 52 42 Geral health Vision Ocular pain Closer activities Far activities Social aspects Psychological aspects Daily life activities Dependency Ability to drive motor Color vision Peripheral vision The statistical analysis of the overall VFQ-25 in this study is not presented statistical variation between subdomains. Five subdomains showed statistical improvement after the intervention, and five did not. Two subdomains showed no differences before and after the intervention. DISCUSSION The purpose of this study was to know if there was an improvement on life quality of those people who attended the research, after hearing and speech intervention. The impact of the eyesight loss has adverse individual and collective consequences, giving rise to psychological, social and economic problems, because implies loss of self-esteem, status in occupational restrictions and consequent income decrease (14,15). Low-vision rehabilitation maximizes a person’s residual vision, with the use of visual aids and adaptive skills, improving their ability to perform specific tasks that were previously considered difficult (16). Macular disease (38%) such as age-related macular degeneration, macular hole and high myopia syndrome, were the related causes regarding visual loss. Similar data were found in others studies about low vision in the elderly (17). Visual rehabilitation aims to enhance an individual’s functional ability and independence, as well as maximize their use of any residual vision. Approximately 90% of visually impaired patients have sufficient residual vision to allow them to benefit from low-vision rehabilitation. At the present, there is no literature available to demonstrate which strategies are the most effective for low-vision rehabilitation. Part of the difficulty in collecting such information lies in the numerous forms of lowvision rehabilitation strategies available. Low-vision rehabilitation is becoming increasingly important in the wider community, once visual impairment affects approximately 314 million people worldwide. The number is about to rise with increased life expectancy and, therefore, more age-related visual problems are appearing. (18,19). Recognizing that the Hearing and Speech therapist is a professional who works in the habilitation and rehabilitation of Difference pre x post 0 -3 1 2 1 3 -3 -7 -5 0 2 -2 Itens num 1 1 2 3 3 2 4 2 3 2 1 1 Questions 1 2 4,19 5,6,7 8,9,14 11,13 3,21,22,25 17,18 20,23,24 15,16 12 10 communication between people, their participation in this process for people with low vision is extremely important, considering that subjects with visual impairment need to use different means from those used for effective communication, thus enabling the continuity of social relationships, so important to life quality (20). The difficulties presented by the elderly involves both activities near and far, showed that the visual impairment brought involvement in various activities of the daily life. This whole impact of impairment in vision entails a greater reliance of the elderly. Such dependence is closely linked to poorer mental health in the elderly with low vision or blind, as well as the loss of social life, relationships with friends and family. The visual impairment influences not only the near vision and also as far peripheral vision, leading the elderly has greater insecurity to get around or run errands. All these findings demonstrate the great impact that the visual impairment brings to life of the elderly, as well as its consequences interact, causing a vicious cycle (21). The number of participants using optical aids increased after the intervention. As this was one of the topics discussed during the intervention, it was expected that this number actually increased and that more seniors begin to make use of the aids (17, 20). During the appointment the help was rewritten, perhaps because the participants had no questions about the help that only arise with their use. It is important that local professionals and the elderly people are able to train using their aids, since this helps in better quantitative and qualitative vision. Without doing the training, it is possible that the elderly gives up from using the aids and then becomes unused. Moreover, during the intervention was enhanced the explanation about the use of optical aids. The researcher demonstrated how to use each aid, and stressed that training is necessary to use them correctly. Activities with reading and writing were conducted with the participants to show its effectiveness in carrying out this activity. Question 12 asks the surveyed to consider in which activities the optical aids are used, and also a comparison of the use of optical aids before and after the intervention. For closer reading activities, write and walk down the street, the use of aids was increased after the intervention. As for the reading activities of posters, watching television and crafts, the use of optical aids has decreased. Rev Bras Oftalmol. 2015; 74 (4): 209-15 214 Monteiro MMB , Carvalho KMM Relate to the use of optical aids, participants have reported that the degree of difficulty in relation to read large print in a newspaper, read a text book or newspaper, write, read what you write and do housework, has decreased. Related on how to read labels of remedies, threading the needle and cut with scissors, there was no change in the degree of difficulty after the intervention. As those activities requires more accurace of vision, then are considered more difficult to realize. The “VFQ” evaluates both quality of life and visual function. For this reason, the option was use “VFQ” as an instrument for evaluation of elderly life quality; moreover, this questionnaire was already validated for utilization with the Brazilian population (22). In relation to overall health, there was no significant difference before and after intervention. As for vision, psychological, everyday difficulties, dependence and peripheral vision significantly improved after the intervention. Analyzing the answers, it was expected that the vision (with the increased use and time of optical aids using), the vision has improved and everyday life difficulties had decreased. One of the intervention goals was to introduce strategies to improve visual functionality during daily tasks so could continue to be performed by the elderly without help (17). A dependency is a factor directly proportional. The lower the difficulty in performing activities, the less dependency is expected. The psychological aspects showed up as a surprise satisfactory, since it is known psychological impairment of people with visual impairment acquired (23). In the sub domains of ocular pain, near and distance activities, color vision has improved after intervention, although were not significant. The VFQ-25 has three relevant items to mobility of people with low vision. As this issue was not addressed during the intervention, it won´t be discussed in this study. It is understood the importance of orientation mobility and to improve the life quality of elderly visually impaired, and it is known that these aspects influences its independence and autonomy (12). The majority aspects of the two questionnaires used in the study tendency to improvement after intervention. There was no statistically significant overall improvement. We believe that this is due to the short time intervention (three sessions). But we believe that if the intervention lasted a little longer, we would have less surveyed interested to participate in the entire study. Other professionals participated in the evaluation and prescription of optical aids, they were ophthalmologists and educator, who were in the subjects appointment at the Low Vision Clinic of UNICAMP. The subjects passing by this appointment are referred to the Visual Rehabilitation Group in another center within the UNICAMP own. There is an interdisciplinary team for Visual Rehabilitation in this center, consisting of a social worker, educator, occupational therapist, psychologist, computer science and orientation and mobility professor. Some subjects who participated in this study has also participated in Visual Rehabilitation Groups previously, others don´t. We should also take into consideration the participation of other professionals, previously consulted, in improving the quality of life of participants in this study. Rev Bras Oftalmol. 2015; 74 (4): 209-15 CONCLUSION After three meetings of Hearing and Speech Intervention, the communication and life quality of elderly with acquired low vision had improvements in the aspects regarding the questioned items in the two questionnaires used for this research: LVQOL and VFQ-25. AUTHORS CONTRIBUTIONS Both, the authors Mayla Myrina Bianchim Monteiro and Keila Miriam Monteiro de Carvalho participated in the design, analysis of results, and contributed effectively in the realization of this manuscript. REFERENCES 1. Chachamovich E, Fleck MP, Trentini C, Power M. Brazilian WHOQOL-OLD Module version: a Rasch analysis of a new instrument. Rev Saúde Pública. 2008;42(2):308-16. 2. World Health Organization. Global data on blindness: an update [internet]; 1995. Geneva: Switzerland [cited 2013 Oct 15] Available from: www.who.int/ncd/.../WHO_PBL_94.38.pdfý 3. Lamoureux EL, Pallant JF, Pesudovs K, Hassell JB, Keeffe JE. The Impact of Vision Impairment Questionnaire: an evaluation of its measurement properties using Rasch analysis. Invest Ophthalmol Vis Sci. 2006;47(11):4732-41. 4. Avis M, Bond M, Arthur A. Questioning patient satisfaction: an empirical investigation in two out-patients clinics. Soc Sci Med. 1997;44(1):85-93. 5. Nobre MI, Temporini ER, Montilha RC, Gasparetto ME, KaraJosé N. [Low vision and rehabilitation: knowledge of ophthalmology residents]. Medicina (Ribeirão Preto). 2006;39(2):253-9. Portuguese. 6. Khadka J, McAlinden C, Gothwal VK, Lamoureux EL, Pesudovs K. The importance of rating scale design in the measurement of patient-reported outcomes using questionnaires or item banks. Invest Ophthalmol Vis Sci. 2012;53(7):4042-54. 7. Wolffsohn JS, Cochrane AL. Design of the low vision quality-oflife questionnaire (LVQOL) and measuring the outcome of lowvision rehabilitation. Am J Ophthalmol. 2000;130(6):793-802. 8. Wright SE, McCarty CA, Burgess M, Keeffe JE. Vision impairment and handicap: The RVIB Employment Survey. The Steering Committee for the RVIB Employment Survey. Aust N Z J Ophthalmol. 1999;27(3-4):204-7. 9. Varma R, Richman EA, Ferris FL 3rd, Bressler NM. Use of patient-reported outcomes in medical product development: a report from the 2009 NEI/FDA Clinical Trial Endpoints Symposium. Invest Ophthalmol Vis Sci. 2010;51(12):6095-103. 10. Fayers PM, Sprangers MA. Understanding self-rated health. Lancet. 2002;359(9302):187-8. 11. Carvalho KM. Baixa visão em idosos: causas, estado funcional, percepções de limitações e reabilitação visual em unidade hospitalar universitária. Campinas. [tese Livre-Docência em Ciências Médicas]. Campinas: Universidade Estadual de Campinas; 2007. 12. Mangione CM, Lee PP, Gutierrez PR, Spritzer K, Berry S, Hays RD; National Eye Institute Visual Function Questionnaire Field Test Investigators. Development of the 25-item National Eye Institute Visual Function Questionnaire. Arch Ophthalmol. 2001;119(7):1050-8. 215 Life quality of low-vision elderly people: before and after hearing and speech intervention 13. Simão LM, Lana-Peixoto MA, Araújo CR, Moreira MA, Teixeira AL. The Brazilian version of the 25-Item National Eye Institute Visual Function Questionnaire: translation, reliability and validity. Arq Bras Oftalmol. 2008;71(4):540-6. 14. Bravo Filho VT, Ventura RU, Brandt CT, Sarteschi C, Ventura MC. [Visual impairment impact on the quality of life of the elderly population that uses the public health care system from the western countryside of Pernambuco State, Brazil]. Arq Bras Oftalmol. 2012;75(3):161-5. Portuguese. 15. Chia EM, Wang JJ, Rochtchina E, Smith W, Cumming RR, Mitchell P. Impact of bilateral visual impairment on health-related quality of life: the Blue Mountains Eye Study. Invest Ophthalmol Vis Sci. 2004;45(1):71-6. 16. Wang BZ, Pesudovs K, Keane MC, Daly A, Chen CS. Evaluating the effectiveness of multidisciplinary low-vision rehabilitation. Optom Vis Sci. 2012;89(9):1399-408. 17. Carvalho KM, Monteiro GB, Isaac CR, Shiroma LO, Amaral MS. Causes of low vision and use of optical aids in the elderly. Rev Hosp Clin Fac Med São Paulo. 2004;59(4):157-60. 18. Stelmack J. Quality of life of low-vision patients and outcomes of low-vision rehabilitation. Optom Vis Sci. 2001;78(5):335-42. Review. 19. Hinds A, Sinclair A, Park J, Suttie A, Paterson H, Macdonald M. Impact of an interdisciplinary low vision service on the quality of life of low vision patients. Br J Ophthalmol. 2003;87(11):1391-6. 20. Monteiro MM, Montilha RC, Gasparetto ME. [Speech and language pathology therapy and the reading and writing of a person with visual disabilitie: exploratory study]. Rev Bras Ed Espec. 2011;17(1):121-36. Portuguese. 21. Trauzettel-Klosinski S, Hahn GA. Support for patients loosing sight. Dev Ophthalmol. 2003;37:199-214. Review. 22. Ferraz EV, Lima CA, Cella W, Arieta CE. [Adjustment of a quality of life evaluation questionnaire to aplication in cataract patients]. Arq Bras Oftalmol. 2002;65(3):293-8. Portuguese. 23. Mello PR, Roma AC, Moraes Junior HV. [Analysis of the life quality of infectious and non-infectious patients with uveitis using the NEI-VFQ-25 questionnaire]. Arq Bras Oftalmol. 2008;71(6):847-54. Portuguese. Corresponding author: Mayla M. B. Monteiro Rua Renato Portioli, 509 Jardim Itapema, Mogi Mirim, SP Zip code: 138010-036; Brazil Fax: 19 3862-1839 E-mail: [email protected] Rev Bras Oftalmol. 2015; 74 (4): 209-15 ORIGINAL ARTICLE 216 Health and vision related quality of life among patients with choroidal neovascular age related macular degeneration Qualidade de vida relacionada com a visão em doentes com degeneração macular relacionada à idade neovascular Maria Picoto1, José Galveia1, Sara Patrício1, António Rodrigues1, Fernanda Vaz2 ABSTRACT Purpose: To describe the impact of aged-related macular degeneration (AMD) on vision-related quality of life (QOL) on a sample of portuguese patients and explore the association with vision, Central Foveal Thickness (CFT) and demographic variables in a Portuguese population. Methods: Observational, interview study of 68 patients with clinical diagnosis of NV AMD seen between January and April 2011 at the Ophthalmology Department of Centro Hospitalar de Lisboa Ocidental. Health-related quality of life (HRQL) was measured with a Portuguese version of the 25-item National Eye Institute Visual Function Questionnaire (NEI VFQ-25). Scores were analysed and correlated with age, gender, laterality of the disease, initial and final visual acuity (VA), CFT and duration of follow-up. Results: Worst eye VA had predictive value in the following scores: global, distance activities, color vision, peripheral vision, role difficulties, social functioning and mental health (p<0.05). In a multivariable model with inclusion of all the parameters studied, the analysed variables explained 60% of the variability of the Global Score, with a predictive value of 0.08 (R2 0.57, p=0.088). Conclusion: NV AMD is associated with impairment in reported vision related QOL in our group of patients. The VA of the worst eye has a predictive value in NEI VFQ-25 scores. Keywords: Quality of life; Macular degeneration; Visual acuity; Mental health; Questionnaires; Chronic disease RESUMO Objetivo: Avaliar o impacto da degeneração macular relacionada à idade (DMRI) na qualidade de vida relacionada com a visão (QVRV) numa amostra de pacientes portugueses. Métodos: Estudo observacional em corte transversal, não comparativo no qual foram incluídos 68 pacientes seguidos no Departamento de Retina Médica do Serviço de Oftalmologia do Centro Hospitalar de Lisboa Ocidental, entre Janeiro e Abril de 2011. A QVRV foi avaliada por meio do questionário National Eye Institute Visual Functioning Questionnaire (NEI-VFQ-25), traduzido para português. Os scores obtidos foram analisados e correlacionados com os seguintes parâmetros idade, sexo, lateralidade da doença, tempo de follow-up, acuidade visual (AV) e EFC iniciais e finais do melhor (MO) e pior olho (PO). Resultados: A AV do PO apresentou valor preditivo nos scores global, atividade para longe, visão cromática, visão periférica, desempenho, função social e saúde mental (p<0,05). Num modelo de multivariáveis com inclusão de todos os parâmetros clínicos analisados, as variáveis estudadas explicaram 60% da variância do score global (SG) com um valor preditivo de 0,08 (R2 0,57, p=0,088). Conclusões: A DMRI NV está associada a uma diminuição da QVRV. A AV do PO tem valor preditivo nos scores do NEI-VFQ-25. Descritores: Qualidade de vida; Degeneração macular; Acuidade visual; Saúde mental; Questionário; Doença crônica 1 2 Egas Moniz Hospital, West Lisbon Hospital, Lisbon, Portugal. Department of Medical Retina, Egas Moniz Hospital, West Lisbon Hospital, Lisbon, Portugal. The authors declare no conflists of interest Received for publication 19/05/2013 - Accepted for publication 29/09/2013 Rev Bras Oftalmol. 2015; 74 (4): 216-21 Health and vision related quality of life among patients with choroidal neovascular age related macular degeneration INTRODUCTION A ge-related macular degeneration (AMD) is the leading cause of severe vision loss in people older than 65 years1,2. Its incidence increases exponentially with age. The Framingham study3 showed an incidence of 11% in people aged between 65 and 74 years, and 30% between 75 and 85 years old. Although only 10 to 20% of AMD cases are identified as exudatively, it accounts for 80-90% of cases of blindness in this pathology3. This disease shows a progressive loss of central vision with a measurable impact on the quality of life of the patient4. When evaluating the impact of a disease, four categories of markers are considered. The physiological markers (eg: glycosylated Hb in Diabetes Mellitus), clinical markers (eg: VA measurement), markers reported by the clinician from their perception of the impact of the disease, and at last the markers reported by the patient. The objective clinical measurement of the visual function in a patient such as VA provides quantitative data5. However, this analysis does not reflect the impact of the visual impairment (VI) in the daily activities (DA) of the patient.6. The quantification of vision-related quality of life (VRQL) provides extra information on the impact of a disease in the function, particularly in the DA. This measurement is important in patients with AMD, because in addition to having high propensity to depressive disorder 7, they show a VI that compromises DA and mobility, which according to Williams et al. is higher in patients of the same age and comparable to patients with chronic disease4. The impact of VRQL on health professionals and community members is low8. Brown et al., Stein et al., Hart et al. found that these groups, including ophthalmologists, underestimate the impact of mild, moderate and severe AMD in VRQL9,10,11. The primary objective of this study was to determine the impact of AMD NV in the vision-related quality of life (VRQL) in a sample of Portuguese patients. The secondary objectives were to understand the impact of some variables in the VRQL, namely the presence of unilateral versus bilateral diseases, the value of VA of the best and worst eye (BE and WE) and the EFC of the BE and WE. And finally, interpret a global model of interaction of the variables studied. METHODS An observational study of 68 patients followed in a retinal consultation by AMD NV between January and April 2011 in the West Lisbon Hospital. The inclusion criteria were: signing an informed consent for participation in the study; age greater than or equal to 50 years old; clinical diagnosis of AMD NV. The exclusion criteria were: follow-up of less than 6m; history of eye disease besides AMD which might compromise the VA (i.e., amblyopia, uncontrolled glaucoma with IOP > 30 mmHg, ischemic optic neuropathy, diabetic macular edema clinically meaningful, significant diabetic retinopathy, active uveitis, clinical signs of myopic choroiditis or refraction > -8D in the current prescription; clinical evidence of thinning of the sclera. 217 The study participants received a questionnaire VFQ-25 translated into Portuguese during the routine consultation. The revised parameters were as follows: age; sex; number of anti-VEGF injections performed; laterality of the disease; initial VA determined in the appointment before the treatment by the Snellen chart and by the same orthotics technician; final visual acuity assessed at the last follow-up appointment by the Snellen chart and by the same orthotics technician; EFC determined by TD OCT (Stratus, Carl Zeiss Meditec, Inc.) in two occasions. Measurement of EFC EFC (average thickness in 1000ìm of the core diameter) was determined using the TD OCT (Stratus, Carl Zeiss Meditec, Inc) and by a single experienced operator in the two stages. Only the scans of sufficient amount were accepted (signal strength e” 8, cuts without areas with absent or reduced signal, core cuts in the macula and correct segmentation limits). Participants were in an iatrogenic mydriasis (pupil diameter e” 6mm) using tropicamide 0.5%, and were instructed to establish an internal fixation target. After the focus adjustment was made and a good central fixation was acquired, the process started. The thickness maps were calculated from the analysis software of the appliance. Questionnaire VFQ-25 The patients rated themselves in 12 dimensions: (1) general health; (2) overview; (3) nearsightedness; (4) activities related to farsightedness; (5) eye pain; (6) social function related to vision; (7) performance related to vision; (8) mental health related to vision; (9) dependence related to vision; (10) difficulties in driving; (11) color vision and (12) peripheral vision. The total score ranges from 0 (worst possible function) and 100 (best possible function). For the statistical analysis of the results we determined: - Average age, standard deviation and distribution by age groups; - Number of female and male patients; - Number of patients with unilateral and bilateral disease; - Average time of follow-up and standard deviation; - Mean initial and final visual acuity and the respective standard deviation; -Mean injections and standard deviation; - Mean baseline scores for each dimension studied of the questionnaire VFQ-25 and the respective standard deviation; - Impact of VA factors, laterality, age, sex and EFC independently in the scores of the questionnaire VFQ-25 (analysis of variance - ANOVA); - Impact of the factors mentioned in line 8) along with the scores of questionnaire VFQ-25 (analysis of variance - ANOVA). RESULTS Sixty-eight patients with AMD participated in the study conducted in medical routine appointments in the West Lisbon Hospital. The average age was 79.2 years, with 75% of the sample aged over 75 years. All patients were caucasian. Most were women (n=44). The final average VA of BE was 0.55 ± 0.27 and WE of 0.22 ± 0.22. The final VA of BE was e” to 0.5 in 42 patients (62%), and the final VA of WE was < 0.1 in 34 patients (50%). The distribution of VA of BE and WE are listed in table 1. Rev Bras Oftalmol. 2015; 74 (4): 216-21 218 Picoto M, Galveia J, Patrício S, Rodrigues A, Vaz F Table 1 Table 3 Distribution of VA of BE and WE by subgroups Analysis of variance (p-value) of the scores of VRQL (NEI-VFQ 25) according to the VA of BE and WE ≥ 0.1 e < 0.25 ≥ 0.25 e <0.5 ≥ 0.5 AV <0.1 BE Final 3 (4%) 8 (12%) 15 (22%) 42 (62%) WE Final 34 (50%) 12 (18%) 10 (15%) 12 (18%) VA: visual acuity; BE: best eye; WE: worst eye Regarding the laterality of the disease, 44 patients (68%) had one eye disease and 21 (32%) had bilateral disease. The average time of follow-up was 22.63 ± 13.11. The mean number of anti-VEGF injections per patient was 3.73 ± 3.06. The scores obtained in each domain of the questionnaire VFQ-25 are described in table 2. Table 2 Scores of VRQL of NEI-VFQ 25 Score NEI-VFQ-25 n Mean (%) General health Overview Eye pain Farsightedness Nearsightedness Social function Mental health Performance Dependence Driving Color vision Peripheral vision Total score 68 68 68 68 68 67 68 68 68 25 65 66 68 27 43 76 51 53 66 47 45 77 54 75 64 57.4 R2 General health 0.16 Overview 0.15 Eye pain 0.1 Farsightedness 0.25 Nearsightedness 0.34 Social function 0.51 Mental health 0.42 Performance 0.45 Dependence 0.27 Driving 0.25 Color vision 0.22 Peripheral vision 0.49 Total score 0.44 BW (p) 0.18 0.96 0.86 0.42 0.81 0.41 0.75 0.79 0.96 0.81 0.42 0.76 0.90 WE (p) 0.996 0.19 0.35 0.22 0.02 0.01 0.01 0.01 0.06 0,998 0.0463 0.0024 0.0092 Interaction (p) 0.61 0.0071 0.70 0.39 0.17 0.04 0.62 0.16 0.28 0.32 0.41 0.05 0.02 SD (%) 20 19 26 26 32 36 26 36 28 36 38 35 23 Except for the score of driving, the response rate was close to 100%. The highest mean values were observed in the scores of dependence (77%), eye pain (76%) and color vision (75%). The lower mean scores were of general health (27%), overview (43%), performance related to vision (45%), mental health (47%) and farsighted activities (53%). Table 3 shows the p-values for the impact of the VA of BE and WE independently. The results of ANOVA are presented for each one of the dimensions studied. The VA of BE and WE explained more than 40% of the variance observed in the following scores of NEI-VFQ 25: social function related to vision (51%), peripheral vision (49%), performance related to vision (45%) total score (44%) and mental health (42%). In relation to the specific effect of VA of each eye in the dimensions studied, the p-values had a statistically significant value (p<0.05) for the impact of the WE in the following dimensions: peripheral vision (p=0.002), total score (chart 1, p=0.009), performance related to vision (p=0.01), mental health (p=0.01), social function related to vision (p=0.01), nearsighted activities (p=0.02) and color vision (p=0.046). The impact of BE in the scores analyzed showed no statistical significance. Rev Bras Oftalmol. 2015; 74 (4): 216-21 Score NEI-VFQ-25 Chart 1 Impact of VA of WE in the total score (p=0.0092) A significant interaction between the VA of BE and WE was observed in the following dimensions: overview (p=0.007), social function related to vision (p=0.04), peripheral vision (p=0.05) and total score (p=0.02). Regarding the laterality of the disease, patients with bilateral disease had worse results in scores except for the dimension of driving, as described in chart 2. However, the difference in value between the scores was not statistically significant. See table 4. Regarding the study on the impact of the variable sex in the results of the scores, there was no statistically significant difference between the two sexes in the dimensions studied. Stratifying the sample by 4 age groups (group 1: < 65 years; group 2: 65-74 years; group 3: 75-84 years; group 4: 85-91 years) there was no statistically significant difference for the dimensions studied (Chart 3). Health and vision related quality of life among patients with choroidal neovascular age related macular degeneration 219 Chart 2 Table 4 VRQL Scores of NEI-VFQ 25 according to the laterality of the disease Analysis of variance (p-value) of the scores of VRQL (NEI-VFQ 25) according to the laterality of the disease Chart 3 Analysis of variance of the total score by age groups Score NEI- VFQ-25 n Unilateral disease Bilateral Unilateral disease /bilateral disease (p-value, T (student) General health 68 25% 30% 0.37 Overview 68 43% 43% 0.92 Eye pain 68 76% 79% 0.68 Farsightedness 68 55% 44% 0.18 Nearsightedness 68 56% 48% 0.32 Social function 67 70% 58% 0.24 Mental health 68 49% 44% 0.54 Performance 68 51% 35% 0.102 Dependence 68 78% 75% 0.64 Driving 25 65% 33% 0.11 Color vision 65 76% 73% 0.73 Peripheral vision 66 67% 58% 0.39 Total score 68 59% 54% 0.42 Analyzing the final EFC for BE and WE, a statistically significant predictive value of final EFC for WE was seen in the dimensions performance related to vision (p=0.03) and peripheral vision (p=0.03). Finally, by means of the analysis of variance we assessed the impact of the variables studied in each one of the scores of VRQL. We found that the variables studied explain more than 40% of the variance of scores (Table 5). Table 5 Analysis of variance (ANOVA) of the scores of VRQL, NEI-VFQ25 according to the variables studied Score NEI - VFQ-25 n R2 Age (p) Initial VA of Initial VA of Final VA of Final VA of BE(p) WE(p) BE(p) WE(p) Initial EFC of Initial EFC of Final Final No de Follow EFC of EFC of Injections - up BE(p) WE(p) BE(p) WE(p) General health 68 0.61 0.51 0.66 0.03 0.95 0.26 0.24 0.60 0.31 0.0085 0.26 0.0085 Overview 68 0.66 0.3 0.02 0.92 0.11 0.41 0.33 0.15 0.18 0.89 0.64 0.64 Eye pain 68 0.4 0.54 0.59 0.33 0.14 0.09 0.19 0.57 0.18 0.4 0.67 0.35 Farsightedness 68 0.63 0.3 0.0063 0.66 0.42 0.87 0.33 0.07 0.36 0.57 0.39 0.33 Nearsightedness 68 0.63 0.28 0.00 0.61 0.14 0.31 0.03 0.93 0.03 0.04 0.87 0.067 Social function 67 0.53 0.46 0.04 0.76 0.07 0.27 0.45 0.24 0.24 0.34 0.71 0.11 Mental health 68 0.4 0.56 0.09 0.99 0.64 0.6 0.16 0.71 0.12 0.47 0.82 0.28 Performance 68 0.46 0.57 0.15 0.96 0.11 0.83 0.52 0.9 0.27 0.87 0.34 0.87 Dependence 68 0.67 0.16 0.0032 0.3194 0.9771 0.0069 0.116 0.72 0.08 0.445 0.850 0.011 Color vision 65 0.38 0.14 0.15 0.84 0.78 0.84 0.18 0.78 0.11 0.96 0.57 0.95 Peripheral vision 65 0.58 0.4 0.11 0.17 0.1 0.2 0.41 0.2 0.15 0.26 0.57 0.09 Total score 68 0.6 0.37 0.0076 0.71 0.27 0.3 0.16 0.21 0.09 0.36 0.86 0.37 Rev Bras Oftalmol. 2015; 74 (4): 216-21 220 Picoto M, Galveia J, Patrício S, Rodrigues A, Vaz F This model built from the analysis of multivariate variance explains 60% of the variance of the total score, with a predictive value of 0.08 (Chart 4). Chart 4 Analysis of variance of the total score (total score= 0.773 + 0.0076 age + 0.0076 No. inj + 0.625 VA BE + 0.032 VA WE + 0.271 VA BE – 0.287 VA WE – 0.001 EFCi BE + 0.001 EFCi WE + 0.0016 EFC BE + 0.003 EFC WE) DISCUSSION The demographic characteristics of the sample, 75% of patients over 75 years old and predominance of females, are in accordance with the normal distribution of a population of patients with AMD12. The results of the study clearly show that the VA has a greater impact on VRQL, a finding already documented in other studies7,8. Regarding the use of the questionnaire NEI-VFQ 25 as a way of measuring the VRQL, to date several researchers have consistently found associations between low VA and low VRQL using this assessment tool5,13. This effect is particularly important in QOL in elderly patients, to the extent that it leads to dependence, disability, anxiety and depression. Some areas were more affected than others by the VA. The impact was virtually non-existent in eye pain (R2=0.1) and in general health (R2=0.15), unlike the domains of social function related to vision (R2=0.51), peripheral vision (R2=0.49), performance related to vision (R2=0.45), total score (R2=0.44) and mental health (R2=0.42), in which the impact was pretty strong. This result is consistent with previous studies 4. The symptomatic profile of the disease, in which there is a progressive loss of the central vision, explains the changes reported by the patients in activities that rely on it, including reading labels of medicines and daily shopping at the supermarket. The low scores on mental health, social function and performance related to vision show the insulating effect of this disease and reflect the loss of independence and increased anxiety. It was observed that the VA of the WE had a higher predictive value than the VA of the BE in the following scores on the questionnaire: peripheral vision, total score, performance related to vision, mental health, social function, nearsighted activities and color vision. This finding is supported by several studies described in the literature. Rev Bras Oftalmol. 2015; 74 (4): 216-21 In the study of Berdeaux8 et al., the VA of the WE had a measurable impact on mental health, dependence, color vision and farsightedness. In the Los Angeles Latino Eye Study14, patients with VA in the WE < 20/200 had worse scores in all dimensions, except for general health and eye pain. According to the study by Azen et al. 15 both eyes contribute independently to the VRQL, and the preservation of a minimal VA in the WE may contribute to the VRQL. Moreover, patients with worse views, even if only in one of the eyes and without reflection on binocular vision, had higher rates of depression, which has an impact on the VRQL, as reported by several researchers4,7. The findings in the aforementioned studies confirm previous publications on the influence of VA of the WE on the VRQL in ophthalmic diseases. The final impact of VA of the WE was initially demonstrated in articles about the benefits of cataract surgery in the second eye14. Subsequent articles have confirmed these results to other ophthalmic pathologies characterized by chronic loss of visual function, particularly gaucoma, AMD and uveitis. The impact of VA of the WE can be explained by the phenomenon of visual inhibition, where binocular vision is worse than the vision of the BE in 1 or more lines. The Los Angeles latino Eye Study 14 demonstrated that a high proportion of individuals may be affected by this phenomenon. Thus the evaluation of binocular vision should be a primary measure in the study of vision difficulties, since it reflects the usual mode of operation. In this study, it was observed that the impact of unilateral and bilateral disease in VRQL was comparable. That is, in spite of the VRQL scores in patients with bilateral disease are lower than in patients with unilateral disease, there was no difference between these two groups, both having similar effects on the VRQL. This finding has several implications. Given the current economic situation, sometimes the treatment of AMD NV in a second eye has to be considered, especially when the VA if it is very low and worse than the 1st eye treated. The decision may be not treating the 2nd eye if the greatest improvement of VA and VRQL occurs after the treatment of the first eye. In this study, since it was observed that the unilateral disease has an impact similar to the bilateral disease and that the VA of the WE has a greater impact on the VRQL, treating the second eye may be recommended, even though it has a VA worse than the first eye treated. These findings were also described by Varma et al.5, and Javitt et al.16,17 regarding other ocular pathology, cataracts. From the multivariable model with inclusion of all clinical parameters analyzed, it was found that the variables studied explain 60% of the variance of the global score (GS) with a predictive value of 0.08 (R2 0.57, p 0.088). However, individually basis the variables age and sex don’t explain the variance of scores, such as the EFC for most scores. These results are important, given that age and sex are often factors that confuse the analysis of QOL, which was not the case in our sample. Regarding the EFC, this is an anatomical measurement and that often has no correlation with the functional aspects, particularly when a psychosocial functional dimension is assessed. Furthermore, despite the AMD the value of EFC can be high or low in patients with low VA, either by intraretinal edema or by atrophy of the retinal layers. Currently, the treatment of AMD tends to preserve mostly the vision and entails heavy financial burden. The cost-benefit Health and vision related quality of life among patients with choroidal neovascular age related macular degeneration analysis is essential in the decision to treat a patient with NV. The evaluation of VRQL may be an extra tool in the decision-making for both the beginning as for the maintenance of the therapy in case this translates into an improved VRQL. This study has several limitations, including the sample size and the age of the patients, which may put some bias in the application of a questionnaire. In addition, the sample was not controlled for the degree of differentiation. The VRQL of patients with NV, assessed by NEI-VFQ 25, reveals an association to the VA of the patient. Unilateral and bilateral diseases have similar impact on the VRQL. The preservation of the VA in the WE is important in maintaining the VRQL. This study suggests that the WE should be treated for maintaining a good long-term VRQL. The assessment of the VRQL should be included in future studies aimed at a better understanding of the impact of this disease on patients’ lives and a better assessment of the effect of the treatment of this disease. REFERENCES 1. 2. 3. 4. 5. 6. Klein R, Klein BE, Linton KL. Prevalence of age-related maculopathy. The Beaver Dam Eye Study. Ophthalmology. 1992;99(6):933-43. Vingerling JR, Dielemans I, Hofman A, Grobbee DE, Hijmering M, Kramer CF, et al. The prevalence of age-related maculopathy in the Rotterdam Study. Ophthalmology. 1995;102(2):205-10. Leibowitz HM, Krueger DE, Maunder LR, Milton RC, Kini MM, Kahn HA, Nickerson RJ, Pool J, Colton TL, Ganley JP, Loewenstein JI, Dawber TR. The Framingham Eye Study monograph: An ophthalmological and epidemiological study of cataract, glaucoma, diabetic retinopathy, macular degeneration, and visual acuity in a general population of 2631 adults, 1973-1975. Surv Ophthalmol. 1980;24(Suppl):335-610. Williams RA, Brody BL, Thomas RG, Kaplan RM, Brown SI. The psychosocial impact of macular degeneration. Arch Ophthalmol. 1998;116(4):514-20. Varma R, Wu J, Chong K, Azen SP, Hays RD; Los Angeles Latino Eye Study Group. Impact of severity and bilaterality of visual impairment on health-related quality of life. Ophthalmology. 2006;113(10):1846-53. Margolis MK, Coyne K, Kennedy-Martin T, Baker T, Schein O, Revicki DA. Vision-specific instruments for the assessment of health-related quality of life and visual functioning: a literature review. Pharmacoeconomics. 2002;20(12):791-812. Review. 7. 8. 9. 10. 11. 12. 13. 14. 15. 16. 17. 221 Brody BL, Gamst AC, Williams RA, Smith AR, Lau PW, Dolnak D, et al. Depression, visual acuity, comorbidity, and disability associated with age-related macular degeneration. Ophthalmology. 2001;108(10):1893-900; discussion 1900-1. Berdeuax GH, Nordmann JP, Colin E, Arnould B. Vision-related quality of life in patients suffering from age-related macular degeneration. Am J Ophthalmol. 2005;139(2):271-9. Brown GC, Brown MM, Sharma S. Difference between ophthalmologists’ and patients’ perceptions of quality of life associated with age-related macular degeneration. Can J Ophthalmol. 2000;35(3):127-33. Stein JD, Brown MM, Brown GC, Hollands H, Sharma S. Quality of life with macular degeneration: perceptions of patients, clinicians, and community members. Br J Ophthalmol. 2003;87(1):8-12. Hart PM, Chakravarthy U, Stevenson MR. Questionnaire-based survey on the importance of quality of life measures in ophthalmic practice. Eye (Lond). 1998;12(Pt 1):124-6. Delcourt C. Epidemiology of AMD. In: Silva R., coordinator. AMD Age-related macular degeneration. GER Group; 2010. p.11-20. Cahill MT, Banks AD, Stinnett SS, Toth CA. Vision-related quality of life in patients with bilateral severe age-related macular degeneration. Ophthalmology. 2005;112(1):152-8. Globe DR, Wu J, Azen SP, Varma R; Los Angeles Latino Eye Study Group. The impact of visual impairment on self-reported visual functioning in Latinos: The Los Angeles Latino Eye Study. Ophthalmology. 2004;111(6):1141-9. Azen SP, Varma R, Preston-Martin S, Ying-Lai M, Globe D, Hahn S. Binocular visual acuity summation and inhibition in an ocular epidemiological study: the Los Angeles Latino Eye Study. Invest Ophthalmol Vis Sci. 2002;43(6):1742-8. Javitt JC, Steinberg EP, Sharkey P, Schein OD, Tielsch JM, Diener M, Cataract surgery in one eye or both. A billion dollar per year issue, Ophthalmology. 1995;102(11):1583-92 Javitt JC, Brenner MH, Curbow B, Legro MW, Street DA, Outcomes of cataract surgery. Improvement in visual acuity and subjective visual function after surgery in the first, second, and both eyes, Arch Ophthalmol. 1993;111(5):686-91. Corresponding author: Maria Picoto Rua: Silva e Albuquerque, 15, rc dto, Zip Code: 1700-360, Lisbon, Portugal. E-mail: [email protected], Rev Bras Oftalmol. 2015; 74 (4): 216-21 ORIGINAL ARTICLE 222 Chalazion and demographic characteristics of patients in a population sample Calázio e características demográficas dos portadores em uma amostra populacional Marjorie Fornazier do Nascimento1, Ana Claudia Viana Wanzeler1, Roberta Lilian Fernandes Sousa1, Larissa Horikawa Satto1, Carlos Roberto Padovani 2, Silvana Artioli Schellini1 ABSTRACT Purpose: To show the frequency of occurrence of chalazion in a population sample, as well as the characteristics of patients. Methods: A cross-sectional study using randomized population sample was carried out during 2004/2005, in the Midwest region of the state of São Paulo. Participants were evaluated according to demographic variables and ocular examination. Results: The frequency of occurrence of chalazion was 1.56‰, more common in women, people with astigmatism or low hyperopia, with wide variation in age of onset. It was necessary to prescribe optical correction and surgery in a significant number of cases. Conclusion: The chalazion has low frequency of occurrence in the general population. It occurs predominantly in women and there is a significant association with refractive error. Keywords: Chalazion/epidemiology; Hordeolum; Eyelid/injuries; Refractive errors RESUMO Objetivo: Apresentar a frequência de ocorrência do calázio em uma amostra populacional, assim como as características de seus portadores. Métodos: Estudo transversal utilizando amostra populacional aleatorizada, realizado nos anos 2004/2005, na região centro-oeste do estado de São Paulo. Os participantes foram avaliados segundo variáveis demográficas e exame oftalmológico. Resultados: A frequência de ocorrência do calázio foi de 1,56‰, sendo mais frequente em mulheres, portadores de astigmatismo ou hipermetropia de pequenos graus, com grande variação de idade de acometimento. Foi necessária prescrição de correção óptica e cirurgia em número expressivo de casos. Conclusão: O calázio tem baixa frequência de ocorrência na população geral. Ocorre predominantemente em mulheres e há associação importante com ametropia. Descritores: Calázio/epidemiologia; Terçol; Pálpebra/lesões; Erros de refração 1 2 Department of Ophthalmology of the Medicine College of Botucatu, São Paulo State University “Júlio de Mesquita Filho”, Botucatu, SP, Brazil. Department of Biostatistics of the Biosciences Institute of Botucatu, São Paulo State University “Júlio de Mesquita Filho”, Botucatu, SP, Brazil. Study conducted at the Medicine College of Botucatu, São Paulo State University “Júlio de Mesquita Filho” Botucatu, SP, Brazil The authors declare no conflicts of interest Received for publication 08/03/2014 - Accepted for publication 23/10/2014 Rev Bras Oftalmol. 2015; 74 (4): 222-4 223 Chalazion and demographic characteristics of patients in a population sample INTRODUCTION RESULTS he chalazion is the most common inflammatory lesion of the eyelid, and is a granulomatous reaction caused by the retention of the secretion from the Meibomian glands due to chronic inflammation resulting from an internal hordeolum or meibomitis.1 It is commonly caused by Staphylococcus sp and may be treated with medical therapy; but when there is no resolution and there chronicity of the process, it may require surgery.2-5 After the removal, a histological examination is needed, particularly in the case of recurrent injuries due to the possibility of a malignant tumor, such as sebaceous cell carcinoma.6-8 Although it is common in eye care services, there are no studies on the distribution of chalazion in the general population, which motivated this study aimed at observing the frequency of occurrence of chalazion in a given population and describing the demographic profile of carriers. Twelve cases of chalazion were found in the general population in the Midwest of São Paulo, resulting in 1.56% of frequency of occurrence of the disease. Analyzing the characteristics of the patients, 11 (91.7%) were female, with a wide range of age of occurrence, which was between 31 and 77 years. Nine (75%) cases were observed on the right side. The main complaint was a foreign body sensation, reported by 33%. There was no link between chalazion and systemic or local diseases. The visual acuity (VA) presented (uncorrected) was > 0.7 in 25%, from 0.3 to 0.7 in 66.7% and < 0.05 in 8.3% of cases. When the corrected VA was assessed, 91.7% showed AV > 0.7 and 8.3% from 0.3 to 0.05 (Fig. 1). The refraction test showed that 58.3% of patients with chalazion were emmetropic, 33% were hyperopic (ranging from +1 to +3.75), and 41.7% were astigmatic (ranging from -0.50 to -2.00). The treatment was the prescription of optical correction to 41.7% of patientes, and 75% were referred for surgical treatment (Fig. 2). T METHODS The analysis of patients with chalazion was based on data from a cross-section, observational study made with a randomized population sample conducted between March 2004 and June 2005. The study was conducted in nine cities of the Midwest region in the state of São Paulo, for which the reference center is the city of Botucatu. The research protocol was reviewed and approved by the Research Ethics Committee of the Medicine College of Botucatu - UNESP. Participants were sorted taking into account the place of residence according to the IBGE census tract (Census, 2000). The sample size of 8,010 individuals was stablished, of which 7,654 people were examined. The sample size was based on the total number of inhabitants of the study area and on the prevalence of blindness and low vision in the population studied. The subjects were invited to participate and an appointment was scheduled. The study population was approached by a Mobile Ophthalmic Unit, registering the identification data, clinical history, and ocular and systemic background of the participants. Then an eye examination was performed with the assessment of visual acuity (VA) by means of the Snellen chart for the illiterate placed 5 meters away and with good lighting conditions, with and without optical correction. The external ocular exam was performed with a hand-held flashlight. The static and dynamic refractometry values were recorded using an auto-refractor (Topcon KR-7000, Japan) and a phoropter (Topcon VT10, Japan). The biomicroscopy assessment was performed using a slit lamp (Shin-Nippon, Japan), and the indirect fundoscopy was performed using 90D Volk lens (Mentor, USA). In individuals aged below 40 years, cycloplegia was obtained by instilling a droplet of cyclopentolate eyedrops (Cicloplégico, Allergan, São Paulo-Brazil), with examination after 30 minutes. Individuals with a spherical component between -0.50 and +0.50 were considered emmetropic, hyperopic with a degree greater than +0.50, and astigmatic with a degree lower than -0.50. All data obtained was categorized and transferred to an Excel table, being statistically treated for the frequency analysis of occurrence of the phenomena observed. Figure 1: Distribution of visual acuity (VA) uncorrected and with the best optical correction in patients with chalazion. Figure 2: Distribution of patients with chalazion regarding the refractive error and the treatment adopted. Rev Bras Oftalmol. 2015; 74 (4): 222-4 224 Nascimento MF, Wanzeler ACV, Sousa RLF, Satto LH, Padovani CR, Schellini SA DISCUSSION The main value of the present study was to randomly assess participants, which helped identify the frequency of occurrence of chalazion in the general population. This injury is very common in optometrists’ offices, and when it is searched in a sample that is not the convenient one, it shows a low prevalence. The lesion was predominant in females, as described by others.9,10 There was a wide variation in the age of the carrier, predominantly in the elderly, which was surprising, since the chalazion is an infection that occurs more frequently in youngsters.9,10 There was no relation between the presence of chalazion and ocular or systemic background, although the association with conditions such as blepharitis, acne rosacea and seborrheic keratosis is known.3,9,11 The uncorrected visual acuity was greater than 0.3 for 91.7% of patients with chalazion. With the best optical correction, there was an improvement of the VA, which was above 0.7 in 91.7% of individuals. The association between chalazion and refractive errors of low degree is classic. When it comes to recurrent lesions, ametropia is often associated. The present study confirms this association, with astigmatism and hyperopia being often observed in association with the presence of chalazion, including requiring optical correction. In addition, astigmatism can be induced chalazion, particularly when located on the upper eyelid, due to causing corneal flattening and deformity.12,13 Although some cases had shown improvement with conservative measures as warm and moist compresses3,4,5,14, the clinical treatment is only effective in the acute inflammatory phase, i.e., in the styes. In the chronic phase, when the granulomatous process is already installed, only small chalazions may cure spontaneously. In our sample, there was indication for surgical excision for most of the cases, and no indication of removal for small lesions carriers. REFERENCES 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. Onesti MG, Troccola A, Maruccia M, Conversi A, Scuderi G. Suspected spinocellular carcinoma of the inferior eyelid resulted multiple chalazion. Ann Ital Chir. 2013;23:84(ePub). pii: S2239253X13019592. Matayoshi S, Forno EA, Moura EM. Manual de cirurgia plástica ocular. São Paulo: Roca, 2004. 370p. Arbabi EM, Kelly RJ, Carrim ZI. Chalazion. BMJ. 2010;341:c4044. Gilchrist H, Lee G. Management of chalazia in general practice. Aust Fam Physician. 2009;38(5):311-4. Duarte AF, Moreira E, Nogueira A, Santos P, Azevedo F. Chalazion surgery: advantages of a subconjunctival approach. J Cosmet Laser Ther. 2009;11(3):154-6. Pavan-Langston D. Manual de Oftalmologia – diagnóstico e tratamento. 4 ed. Rio de Janeiro: MEDSI, 2001. 592p. Pereira PR, Odashiro AN, Rodrigues-Reyes AA, Correa ZM, de Souza Filho JP, Burnier MN Jr. Histopathological review of sebaceous carcinoma of the eyelid. J Cutan Pathol. 2005;32(7):496-501. Ozdal PC, Codère F, Callejo S, Caissie AL, Burnier MN. Accuracy of the clinical diagnosis of chalazion. Eye (Lond). 2004;18(2):135-8. Nemet AY, Vinker S, Kaiserman I. Associated morbidity of chalazia. Cornea. 2011;30(12):1376-81. Netto AA, Rolim APQ, Müller, TPS. Prevalência de doenças palpebrais no serviço emergencial de oftalmologia do Hospital Universitário da Universidade Federal de Santa Catarina. Arq Catarin Med. 2006;35(4):64-9. Bagheri A, Hassani HR, Karimian F, Abrishami M, Yazdani S. Effect of chalazion excision on refractive error end corneal topography. Eur J Ophthalmol. 2009;19(4):521-6. Santa Cruz CS, Culotta T, Cohen EJ, Rapuano CJ. Chalazioninduced hyperopia as a cause of decreased vision. Ophthal Surg Lasers. 1997;28(8):683-4. Honda M, Honda K. Spontaneus resolutions of chalazion after 3 to 5 years. Eye Contact Lens. 2010;36(4):230-2. Nemet AY, Vinker S, Kaiserman I. Associated morbidity of blepharitis. Ophthalmology. 2011;118(6):1062-8. CONCLUSION The chalazion occurred in 1.56% of the inhabitants in the area studied, predominantly in women, with a wide range of age of occurrence. There was a significant association with low ametropias, requiring the prescription of optical correction and surgery in a significant number of cases. Rev Bras Oftalmol. 2015; 74 (4): 222-4 Corresponding author: Marjorie Fornazier do Nascimento. Rua Antonio Amando de Barros, 241 - Botucatu (SP) - 18601-260 - Brazil. E-mail: [email protected] ORIGINAL ARTICLE 225 Correlation between the use of the accommodation and symptoms of asthenopia in hyperopic patients Correlação entre o uso da acomodação e sintomas de astenopia em pacientes hipermétropes Juan Carlos Luna da Costa1 , Ian Beltrão de Sá Martins1, Larissa Tavares Albuquerque Nóbrega1, Maria Odília Navarro Medeiros1, Luciana Maria Palitot1, Marília Bezerra Cavalcanti Dias1, Tarcízio José Dias1 ABSTRACT Purpose: The objective of this paper was to compare the symptoms of asthenopia in patients at different levels of hyperopia and corrected for different accommodative efforts. Methods: This study is an experimental design and quantitative approach. Sixty-nine hyperopic patients aged between 15 and 40 were selected. Individuals with a diagnosis of accommodative insufficiency and paralysis, accommodative spasm or any type of ocular deviation were excluded. Subjects were randomly divided into four groups. Each one performed a nearvision task with different corrective lenses, varying the value of the accommodative effort. Results: There is significant reduction in the asthenopia score during the near-vision task when leaving 35% or more of the amplitude of accommodation in reserve. The linear regression showed that the variables total hyperopia (r = 0.109) and the difference between static and dynamic refraction (r = 0.135) did not obtain significant linear relationship to the asthenopia score. Conclusions: There is significant reduction in the asthenopia score when leaving 35% or more of the amplitude of accommodation in reserve. The symptoms of asthenopia are not associated to the severity of the hyperopic refractive error. The search for symptoms before the near vision task, using a questionnaire, related to the symptoms during the accommodative effort task, revealing the importance of searching for complaints about asthenopia during anamnesis, which can help ophthalmologists with prescriptions of glasses for hyperopic patients with asthenopia. Keywords: Accommodation, ocular; Hyperopia; Asthenopia; Refraction, ocular; Eyeglasses RESUMO Objetivos: O presente estudo objetivou avaliar os efeitos do esforço acomodativo e do poder do erro refrativo nos sintomas de astenopia. Métodos: Trata-se de um modelo de estudo experimental e abordagem quantitativa, cuja amostra consistiu de 69 pacientes hipermetropes entre 15 e 40 anos de idade. Foram excluídos os indivíduos com diagnóstico de insuficiência ou paralisia da acomodação, espasmo de acomodação ou qualquer tipo de desvio ocular. Os pacientes foram alocados aleatoriamente em quatro grupos. Cada grupo realizou o trabalho de visão para perto com correções diferentes, variando o valor do esforço acomodativo. Resultado: Houve melhora significativa dos sintomas de astenopia com correções que proporcionaram mais de 35% da amplitude de acomodação em reserva. Não houve relação estatisticamente significativa entre os sintomas e o valor do erro refrativo. Conclusão: Há uma redução significativa dos sintomas quando os pacientes mantêm 35 % ou mais de sua acomodação em reserva. Os sintomas de astenopia não estão associados à gravidade do defeito hipermetrópico. A pesquisa de sintomas antes do teste, através de um questionário, foi o fator que melhor se relacionou com os sintomas durante o teste de visão para perto, revelando a importância da pesquisa das queixas de astenopia durante anamnese na prescrição de lentes para visão de perto. Descritores: Acomodação ocular; Hiperopia; Astenopia; Refração ocular; Óculos 1 Centro Oftálmico Tarcízio Dias, João Pessoa, Paraíba, Brazil. The authors declare no conflicts of interest Received for publication 29/09/2014 - Accepted for publication 08/03/2015 Rev Bras Oftalmol. 2015; 74 (4): 225-30 226 Costa JCL , Martins IBS, Nóbrega LTA, Medeiros MON, Palitot LM, Dias MBC, Dias TJ INTRODUÇÃO H yperopia is the condition of the eye where incoming rays of light reach the retina before they converge into a focused image. Total hyperopia is divided into latent hyperopia and manifest hyperopia. Latent hyperopia is the one which is physiologically supplanted by the tonus of the ciliary muscles. Manifest hyperopia is divided into facultative hyperopia and absolute hyperopia. Facultative hyperopia is the one which can be overcome by the accommodative effort, while this is not possible in the case of the absolute hyperopia(1). For several ophthalmologists, the prescription for the near vision is based on the claim that only half or two-thirds of an individual’s amplitude of accommodation is sustainable for an extended period of time(2). Donders (1972) recommended, for the correction of hyperopia, the value of the manifest hyperopia added to a fourth of the latent hyperopia(3). A rule of thumb which received wide acceptance is that the lens used for near vision should allow that half of the patient’s amplitude of accommodation remain in reserve(4). The younger the patient, the more active is the accommodation; therefore, less correction for the hyperopia is needed. In normal individuals, right after birth the hyperopia is about 2 to 3 diopters. It can increase slightly in the first years of life, but it rapidly and gradually diminishes according to the somatic growth until after the puberty, in which the individuals tend to become emmetropic. After the growth period, refraction tends to remain stationary. In old age, the tendency to hyperopia is greater, due to modifications in the curvature and in the refraction indexes of the crystalline lens layers(1,5). There is also an apparent increase of hyperopia due to progressive insufficiency of accommodation. With the decrease of the ciliary muscle tonus, part of the latent hyperopia also manifests itself and with the reduction of the accommodation capacity, most of the facultative hyperopia becomes absolute. Therefore, in the beginning of life, unless the error is very high, the accommodation capacity is able to correct it entirely, if absolute hyperopia is absent. After the age of 65 virtually all the error becomes absolute(4). The symptoms of eye strain are, in part, due to extreme accommodation and to the extra convergence effort. Asthenopia is the term used to describe the sensation of extreme effort and weakness or eye fatigue derived from the use of vision. It is a common manifestation in many patients with convergence insufficiency, accommodation insufficiency, refractive error and strabismus. Its symptoms are headache, diplopia, difficulty in focusing the image, fatigue, reading problems, blurred vision(6). Accommodative fatigue can be described as the reduction of the performance of the accommodation system due to a prolonged or repetitive accommodative effort(7). In near vision, the temporary insufficiency of the ciliary muscle to maintain contraction can result in visual impairment, on the other hand extreme accommodation or spasm of the ciliary muscle, may cause an artificial condition of myopia(8). Accommodation is a key factor in the correction of hyperopia(5), which motivated us to construct a diagram (diagram J) to correlate the refractive error with the amplitude of accommodation and find the ideal value of the most comfortable reading prescription for the hyperopic patients. In the diagram, the j value can be found relating the values of total hyperopia of the patient to his accommodation and represents the comfortable Rev Bras Oftalmol. 2015; 74 (4): 225-30 refraction for near vision. This way, the diagram can be constructed according to the adequate refraction to hold a determinate fraction of the accommodation in reserve. In other words, the fraction of the accommodation not used by the eyes while fixing in a point in space, avoiding over or undercorrection. The j(50) means the value in the diagram calculated to leave in reserve 50% of the patient’s accommodation. The value of j can be found through the following equation, in which jc is the value of prescription for certain accommodative reserve C; D is the value of the hyperopia in diopters; P is the additional dioptric power for near vision; AA is the amplitude of accommodation in diopters and C is the value of the accommodative reserve in percentage: j(C)= D + P – [AA(100-C).10-2] The deduction of this equation is based on the maintenance of a fraction of the accommodation during near vision effort. Hence, near vision requires the total correction D summed to the value of P (3 diopters in usual conditions), but in these circumstances the prescription of lens would cancel the accommodative effort. The reduction of this value would imply in a progressive increase in the use of accommodation to the maximum of the individual’s accommodation capacity. An evidence of this effort would be the increase of the reduction factor “AA(100-C).10 -2”. Therefore, it was observed that the higher the accommodative reserve C, the lower the accommodative effort, in a way that a correction j(100) would cancel the reduction factor and, consequently, accommodation. This equation explains why individuals with high amplitude of accommodation tend to tolerate higher degrees of hyperopia. For instance, a five-year-old child’s amplitude of accommodation is about 16D. Considering that this child is hyperopic and his/her hyperopia measures two diopters, in order to hold 50% of his/her accommodation in reserve while he/she reads from a distance of 33cm, the ideal prescription would be: j(50) = +2 +3 – [16(100-50).10-2] = -3D. The value of -3D implies that, at this moment, it is not necessary to correct this patient’s near vision, while symptoms are absent. With aging and loss of accommodation, the hyperopic patients tend to present symptoms of asthenopia. Thus, a patient with the same 2 diopters of hyperopia will need +1,5 D correction when his/her amplitude is reduced to 7D (which happens approximately at 30 years of age), to ensure that 50% of his/her accommodation remains in reserve and the patient will be able to read comfortably. Despite the fact that, according to many ophthalmologists, the prescription for near vision is based on the claim that only half or two-thirds of the amplitude of accommodation is sustainable for an extended period of time, a research developed by Wolffsohn et al. showed that adults’ accommodation system is robust and resistant to fatigue during an intensive and prolonged task(2) . Besides, a greater proportion of the amplitude of accommodation can be exercised in a continuous way, in spite of what was suggested previously. Alves suggests the correction of hyperopia for occasional use, for reading or any other activity that requires accommodative effort, in those cases where there is difficulty to relate the symptoms(5). Based on this dissent, one of the objectives of the present article is to compare the symptoms of accommodative effort in patients with correction for j(20), j(35), j(50) e j(60) during a sustained and intensive task for near vision. Correlation between the use of the accommodation and symptoms of asthenopia in hyperopic patients The main objective of this paper was to compare the symptoms of asthenopia in patients at different levels of hyperopia and corrected for different accommodative efforts. The specific objectives were: to compare the relation between the level of asthenopia before and after near vision task; to evaluate the symptoms of accommodative effort in patients with correction for j(20), j(35), j(50) e j(60); to relate the symptoms of asthenopia with the value of refractive error; to construct a diagram to guide the ophthalmologist in prescribing glasses for near vision. METHODS This study is an experimental design and quantitative approach. The sample consists of hyperopic patients treated at Instituto Visão para Todos (IVPT) of Centro Oftálmico Tarcízio Dias, in João Pessoa – State of Paraíba, Brazil, from January, 2013 to April, 2014. Hyperopic patients aged between 15 and 40 were selected. Individuals with a diagnosis of accommodative insufficiency and paralysis, accommodative spasm or any type of ocular deviation were excluded from the study. All the individuals were carefully evaluated with regard to the amplitude of accommodation, refractive error, visual acuity and ocular deviation. The push-up method was adopted in order to obtain the amplitude of accommodation. The method consists of Snellen optotypes for near vision 40 cm distant from the eye with corrected ametropia. In this method the patient is oriented to find the best optotype of the chart that could be clearly seen. Then the chart is placed closer to the patient until a blurred vision of the letters is obtained. This distance is converted into diopters, which corresponds to its amplitude of accommodation(9). Automated refraction without cyclopegia was conducted with the Huvitz MRK-3100 Premium refractor. The total hyperopia was evaluated with the same refractor 40 min after the instillation of Cyclopentolate 1%. Over recent years, several studies comparing the cycloplegic effect of various drugs to the required number of drops have proved that the instillation of a drop of Cyclopentolate 1% is sufficient to obtain adequate cycloplegia(10-13). The individuals were requested to return one week after the refractive evaluation for an accommodative effort task. Before the near-vision task, all the individuals answered the asthenopia symptoms survey (ASS), a questionnaire about symptoms of asthenopia, which was translated to Portuguese. The questionnaire consists of eight questions, which involve symptoms during near-vision task (discomfort, headache, eye pain, blurred vision, double vision, burning sensation, eye strain). Each symptom is graded in five points according to its severity(14). The participants were randomly divided into four groups. Each one performed the near-vision task with different corrections: j(20), j(35), j(50) and j(60). Diagrams that relate the amplitude of accommodation with the total hyperopia were used to find a prescription for each group. The right eye underwent a 20-minute near-vision task, consisting of the use of a computer monitor 33 cm distant from the eye, showing a 2.0 mm wide and 3.0 mm long rectangular white line on a black background. The rectangle was programmed to randomly move, every 4 seconds in the same position of its geometric center, in the following directions: vertical, horizontal, and diagonal. The patients were requested to read the rectangle and inform its direction. This modality was chosen because of the fact that it was ensured that the individuals evaluated kept focusing on their target during most part of the time in order that the blur could be identified as the patient’s difficulty to define the directions. Furthermore, the 227 eye movement effort, which is commonly used in reading, was eliminated in order to evaluate the symptoms related solely to accommodation. By means of monocular testing, we minimized the convergence effort. In order to minimize the dry-eye effect, all the patients received one drop of carmellose sodium 5mg/ml on both eyes before the near-vision task. Astigmatism was completely corrected with cylindrical lens. The average luminance in the monitor position was of 290 Lux, measured with the digital CEL luxmeter, model LD-511. The data was registered on a formulary containing information about the symptoms experienced (headache, blurred vision, double vision, pain, burning sensation, eye strain) and the moment when they occurred. Each of the five symptoms was classified into a scale from 0 to 1, taking into account the time (T) when the symptom appeared. Thus, punctuation 0 means that the symptom did not occur during the 20-minute test; the punctuation tends to the maximum of 1 when the symptom occurs at the very beginning of the test. The resulting asthenopia score was the sum of the punctuation of all the symptoms: Asthenopia Score during the task = Σ (1 – T/20). The IBM SPSS Statistics® software version 18 for Windows was used in the data analysis. ANOVA (analysis of variance), Turkey HSD test and linear regression were used. A significance level of 5% was adopted. The project was approved by the Research Ethics Committee from Paraíba-Brazil (Protocol ID: 652.767).The patients’ identification data were kept confidential during their collection and they were not exposed in the study. Informed consent was obtained. RESULTS Sixty-nine individuals were evaluated (30 male and 39 female). The average age was 26.77, with standard deviation of 6.975. The linear regression showed that the variables age (r = 0.006), total hyperopia (r = 0.109) and the difference between static and dynamic refraction measured by autorefractor (r = 0.135) did not obtain significant linear relationship to the asthenopia score. The factor that contributed the most to the prediction of the symptoms was the Asthenopia Symptoms Survey ASS (r = 0.39), which corresponded to a direct and positive relation (Figure 1). Figure 1: Graph of linar regression that shows the relation between the asthenopia symptoms score during the test (r=0,39) and the Asthenopia Symptoms Survey (ASS). Rev Bras Oftalmol. 2015; 74 (4): 225-30 228 Costa JCL , Martins IBS, Nóbrega LTA, Medeiros MON, Palitot LM, Dias MBC, Dias TJ There was not a linear relationship between the groups and the asthenopia score during the task, but there was a significant decrease in the asthenopia score between the j(20) and j(35) groups, remaining unchanged after the j(35) (Figure 2). Figure 2: Graph the relates the symptoms scores during the nearvision task (mean and confidence interval) the groups tested. Analysis of variance (one-way ANOVA) and Turkey HSD test revealed a statistical difference between level of accommodation and the asthenopia score (F-value = 5.553; p = 0.002). The tests show difference between groups j(20) and j(35) (p=0.03). ANOVA also shows difference between j(20) and j(50) (p=0.033). Groups j(20) and j(60) were statistically different as well (p=0.005). But there was no difference in the following analysis: j(35) versus j(50) (p=0,870), j(35) versus j(60) (p=0.999), j(50) versus j(60) (p=0.931) (Table 1). The j(20) group was paired with the other groups concerning their gender and age, without interference of such factors. Analysis of variance (one-way ANOVA) showed no significant difference between groups concerning the intensity of hyperopia (F-value = 1.445; p = 0.238). Table 1 Relation between the level of accommodation and the variables age, gender and asthenopia score during the nearvision task. One-way ANOVA showed difference between group j(20) and the other groups concerning the asthenopia score (F-value = 5,553; p = 0,002). Group n Age in years (mean ±SD) Gender M F 20% of accommodation in reserve: j(20) 17 27.80 (±6.66) 8 9 1.479 (±0.31) 35% of accommodation in reserve: j(35) 19 30.13 (±5.18) 7 12 0.786 (±0.735) 50% of accommodation in reserve: j(50) 17 24.93 (±7.92) 8 9 0.932 (±0.534) 60% of accommodation in reserve: j(60) 16 24.20 (±6.85) 7 9 0.812 (±0.591) DISCUSSION The value of total hyperopia and the difference between the pre-cycloplegia and the post-cycloplegia refraction measured by the autorefractor were not associated to the symptoms presented during near vision effort. In his book, Duke-Elder states that symptoms do not appear in the proportion of severity of causal defect. The symptoms vary from individual to individual, reaching surprising levels without any apparent cause(1). Among the variables of the study, the one that contributed the most to the linear prediction of the symptoms was the Asthenopia Symptoms Survey (ASS). The pre-test complaint scores had a positive relation with the complaints during the test, regardless of the group tested. Thus, it is possible to conclude that some research on the symptoms of asthenopia during anamnesis is valid in order to help in the refraction and prescription of glasses for near vision. There was no linear relationship between the treatment groups and the asthenopia score during the near vision task. Nevertheless, it could be concluded, from the results, that the prescription of lenses over j (35) considerably reduces the symptoms of asthenopia. Hence, there are no guarantees that the prescription of highly positive lenses, such as the prescription over j(50), will reduce more the patients’ symptoms of asthenopia. We will illustrate the findings of the results into the following example: a 25-year-old individual (amplitude of accommodation Rev Bras Oftalmol. 2015; 74 (4): 225-30 Asthenopia score during the task (mean ±SD) of 8.5 D), with total hyperopia of +3.0 D spherical, has a correction of +0.50 D spherical in diagram J35 (Figure 3); the same individual presents a correction of +1.75 D spherical in diagram J50 for near vision lenses. The results pointed out significant improvement in +0.50 D or over lenses prescription. The prescription of highly positive lenses, namely over +1.75 D, does not ensure improvement in relation to +0.50 D. Therefore, it is possible to infer that, in isolation, the power of accommodation does not explain the symptoms of asthenopia in a linear way. The use of extrinsic muscles was minimized by the test methodology, reducing the biases of the variable in the study. Several studies in the medical literature search for other factors as the causes of eye strain. Studies have shown the effects of psychological and environmental factors, such as stress at work, burnout, luminous intensity, thermal comfort in the ocular complaints at work(15-17). The discovery of this effect may have an ergonomic influence on health, safety and comfort conditions. The complaints during the test could be interpreted as the result of the uninterrupted use of accommodation for 20 min. It is important that longer accommodative effort tests be performed and that new studies aim at evaluating the appearance of symptoms due to prolonged accommodative effort or with pauses for resting. We conclude, therefore, that the accommodative effort, in isolation, does not explain the symptoms presented by patients; however, there is significant reduction in the asthenopia score when leaving 35% or more of the amplitude of accommodation Correlation between the use of the accommodation and symptoms of asthenopia in hyperopic patients in reserve. It was also concluded that the symptoms of asthenopia are not associated to the severity of the hyperopic refractive error. The search for symptoms before the near vision task was the factor that correlated the most with the symptoms during 229 the accommodative effort test, revealing the importance of searching for complaints about asthenopia during anamnesis, which can help ophthalmologists with prescriptions of glasses for hyperopic patients with asthenopia. Figure 3: Diagrams J(20), J(35), J(50) and J(60). Colored cell: diopter is zero or negative, it may not be prescribed for hyperopia. Blank cell: diopter is positive, it may be prescribed for hyperopia. Rev Bras Oftalmol. 2015; 74 (4): 225-30 230 Costa JCL , Martins IBS, Nóbrega LTA, Medeiros MON, Palitot LM, Dias MBC, Dias TJ ACKNOWLEDGEMENTS We are very grateful to translators Rodrigo Araújo e Castro and Raquel Rossini Martins Cardoso. REFERENCES 1. Duke-Elder S. Refração Prática. Rio de Janeiro: Rio Med Livros; 1997. 2. Wolffsohn JS, Sheppard AL, Vakani S. Davies LN. Accommodative amplitude required for sustained near work. Ophthalmic Physiol Opt. 2011;31(5):480-6. 3. Donders FC. On the anomalies of accommodation and refraction of the eye. Boston: Milford House; 1972 4. Yanoff M, Duker JS. Oftalmologia. 3a ed. Rio de Janeiro: Elsevier; 2011. 5. Alves AA. Refração. 5a ed. Rio de Janeiro: Cultura Médica, 2008. 6. Abdi S, Lennerstrand G, Pansell T, Rydberg A. Orthoptic findings and asthenopia in a population of Swedish schoolchildren aged 6 to 16 years. Strabismus. 2008;16(2):47-55. 7. Hasebe S, Graf EW, Schor CM. Fatigue reduces tonic accommodation. Ophthalmic Physiol Opt. 2001;21(2):151-60. 8. Kasthurirangan S, Vilupuru AS, Glasser A. Amplitude dependent accommodative dynamics in humans. Vision Res. 2003;43(27):2945-56. 9. Duane A. Normal values of the accommodation at all ages. JAMA. 1912; 59(2):1010–13. 10. Celebi S, Aykan U. The comparison of cyclopentolate and atropine in patients with refractive accommodative esotropia by means of retinoscopy, autorefractometry and biometric lens thickness. Acta Ophthalmol Scand. 1999;77(4):426-9. Rev Bras Oftalmol. 2015; 74 (4): 225-30 11. Hertwig RV, Netto AL , Souza-Dias CR. Acomodação residual sob o efeito cicloplégico do cloridrato de ciclopentolato a 1%. Arq Bras Oftalmol. 1994;57(6):407-10, 12. Stolovitch C, Loewenstein A, Nemmet P, Lazar M. Atropine cycloplegia: how many instillations does one need? J Pediatr Ophthalmol Strabismus. 1992;29(3):175-6. 13. Pinheiro RK, Netto AL . Estudo comparativo da acomodação residual após instilação de colírios de tropicamida a 1%, ciclopentolato a 1% e associação de tropicamida a 1% + ciclopentolato a 1%. Arq Bras Oftalmol. 2000;63(6): 475-9. 14. Chatterjee D, Kothari M, Mody K. Anomalies of accommodation, fusion and refraction in patients with low asthenopia symptom survey score. AIOC Proceedings; 2010. 15. Ostrovsky A, Ribak J, Pereg A, Gaton D. Effects of job-related stress and burnout on asthenopia among high-tech workers. Ergonomics. 2012;55(8):854-62. 16. Azmoon H, Dehghan H, Akbari J, Souri S. The relationship between thermal comfort and light intensity with sleep quality and eye tiredness in shift work nurses. J Environ Public Health. 2013;2013:639184. 17. Ustinaviciene R, Januskevicius V. Association between occupational asthenopia and psycho-physiological indicators of visual strain in workers using video display terminals. Med Sci Monit, 2006; 12(7): CR296–301. Corresponding author José Faustino Cavalcanti 700, Pedro Gondim, João Pessoa, Paraíba, Brazil. Zip code: 58031180. Phone: +55 83 88082328. E-mail: [email protected]. ORIGINAL ARTICLE 231 Eyelid disorders: frequency of occurrence and profile of carriers in a Brazilian population sample Alterações palpebrais: frequência de ocorrência e perfil dos portadores em amostra populacional brasileira Ana Cláudia Viana Wanzeler1, Marjorie Fornazier do Nascimento1, Roberta Lilian Fernandes Sousa1, Carlos Roberto Padovani2, Silvana Artioli Schellini1 ABSTRACT Purpose: to show the frequency of occurrence of the eyelid disorders in a Brazilian population sample, as well as the characteristics of the carriers. Methods: a transversal study using a random population sample was carried out in the years 2004/2005, involving nine cities of the middle west region of the State of São Paulo - Brazil. We had 7654 participants which were evaluated according to demographic variables and complete ophthalmological examination. The eyelid disorders were detected using a lantern and slit lamp. Data were statistically analyzed. Results: eyelid disorders such as of trichiasis and ectropion were more related to the characteristics men, whites, complaining of reduced near visual acuity and 72.7% of trichiasis underwent surgical treatment, as well as 28.5% of patients with ectropion. Ptosis was related to the females, whites, complaining of reduced near visual acuity and 26.3% required surgery. Entropion was detected only in one case, male, white and a case of epiblepharon was observed in a female, brown. Conclusion: the most frequent palpebral disorder observed in the Brazilian general population is trichiasis, followed by ptosis and ectropion. The authors call attention to the fact that carriers do not have complaints related to the eyelid disorders. Keywords: Eyelid diseases/epidemiology; Population studies; Brazil RESUMO Objetivo: apresentar a frequência de ocorrência das alterações palpebrais em uma amostra populacional brasileira, assim como as características de seus portadores. Métodos: estudo transversal utilizando uma amostra populacional aleatorizada, realizado nos anos de 2004/2005, em nove cidades da região centro-oeste do estado de São Paulo. Foram examinadas 7654 pessoas sendo os participantes avaliados segundo variáveis demográficas e exame oftalmológico completo. As alterações palpebrais foram avaliadas por meio de exame externo usando lanterna e lâmpada de fenda. Os dados obtidos foram analisados estatisticamente. Resultados: as alterações palpebrais como a triquíase e o ectrópio foram mais relacionadas às características homens, brancos, queixa de redução de acuidade visual para perto. Foi realizado tratamento cirúrgico em 72,7% das triquíases detectadas, assim como 28,5% dos ectrópios. Já os casos de ptose palpebral, foram relacionados ao sexo feminino, brancos, com queixa de diminuição da acuidade visual para perto e 26,3% necessitaram de cirurgia. Entrópio foi detectado em um caso, masculino, branco e epibléfaro foi observado em um indivíduo do sexo feminino, parda. Conclusão: a alteração palpebral mais presente na população geral brasileira é a triquíase, seguida da ptose palpebral e do ectrópio. Os autores chamam a atenção para o fato dos portadores não possuírem queixas relacionadas às alterações palpebrais. Descritores: Doenças palpebrais/epidemiologia; Estudos populacionais; Brasil 1 2 Department of Ophthalmology, Medicine College of Botucatu, São Paulo State University “Júlio de Mesquita Filho” Botucatu, SP, Brazil. Department of Biostatistics, Institute of Biosciences of Botucatu, São Paulo State University “Júlio de Mesquita Filho” Botucatu, SP, Brazil. Study conducted at the Medicine College of Botucatu - UNESP The authors declare noconflicts of interest Received for publication 07/10/2014 - Accepted for publication 16/03/2015 Rev Bras Oftalmol. 2015; 74 (4): 231-4 232 Wanzeler ACV, Nascimento MF, Sousa RLF, Padovani CR, Schellini SA INTRODUCTION The eyelids are part of the protective mechanism of the eyes. They are structures composed of very delicate tissues that move constantly, with the possibility of undergoing changes due to external factors or alterations of senility, with the arisal of deformities 1. They have sweat and sebaceous glands in their composition, besides the eyelashes which are differentiated hair follicles that grow with a convexity that takes them away from the eyes, so that the base of the follicle is closer and the end of it more distant to the eye bulb2. Keeping the eyelids opposite to the eye bulb is important for the integrity and distribution of the tear film. When there is eversion, inversion of the eyelid margin, or even loss of convexity of the eyelashes, the eye bulb suffers from failure of the protective mechanism, with the possibility of installation of inflammation and infections of the margin or the ocular surface, which highlights the importance normal positioning of the eyelids3. There is no data on the presence and distribution of the eyelid position changes in the general population. But there is data available on the eyelid changes in convenience samples, as well as in the elderly, which led us to this study developed with the aim of describing the eyelid changes most commomly found in a randomized population sample, as well as the demographic characteristics of the patients. METHODS Analyses were made on the eyelid position changes based on data from a cross-sectional study of a randomized population sample conducted between March 2004 and June 2005 in nine cities of the Midwest region of the state of São Paulo. The research protocol was analised and approved by the Research Ethics Committee of the Medicine College of Botucatu UNESP. Participants were sorted taking into account the place of residence according to the IBGE census tract (Census, 2000). The sample size of 8,010 individuals was stablished, of which 7,654 people were examined. The sample size was based on the total number of inhabitants of the study area and on the prevalence of blindness and low vision in the population studied. The subjects were invited to participate and an appointment was scheduled with the approach of a Mobile Ophthalmic Unit. Participants’ identification data, clinical history, and ocular and systemic background were registered. Then a complete eye examination was performed with the assessment of visual acuity (VA) by means of the Snellen chart for the illiterate, external examination (using hand light), slit lamp examination in (Shin Nippon SL-203, Japan) and refractometry. For the present study a sub-sample of patients with eyelid changes was analyzed. When necessary, the subjects underwent surgical treatment. Trichiasis was defined when there were lashes touching the eye, in that while deployed in the anterior lamella, they were abnormally curved and directed to eye surface4. Ectropion is the eyelid malpositioning characterized by the eversion of the eyelid margin away from the eye bulb. Eyelid entropion means reversing the edge of the eyelid, causing the eyelashes to touch the eyeball1. Ptosis is a condition in which the upper eyelid edge is located below its normal position of 2 mm, covering the superior limbus in the primary position of the eye look3. The data was categorized and transferred to an Excel table, being statistically treated for the frequency analysis of occurrence of the phenomena observed. RESULTS The most significant change observed was the trichiasis, with 22 cases detected, and a frequency of occurrence of 0.29%, 59% being in men, 86.3% in white elderly, 63.6% with complaint of visual acuity reduction to near vision. Surgical treatment was necessary and performed in 72.7% of cases. There were 19 cases of ptosis, with a frequency of occurrence of 0.24%, 63.1% in females, 84.2% in white elderly complaining of visual acuity (VA) reduction to near vision at 52.6%, and 26.3% had surgery. Ectropion was observed in 14 cases, with a frequency of occurrence of 0.18%, 78.5% in males, 100% white elderly with a main complaint of VA reduction to near vision (50%) and ocular hyperemia (42.8%) with the need of surgery in 28.5% of cases. Entropion was detected in one case in a white male, and one case of epiblepharon in a brown female (Table 1). The frequency of occurrence of these two conditions was 0.01%. For all the conditions detected except ptosis the lower eyelid was the most affected. Table 1 Frequency of occurrence of eyelid changes in the Midwest region of the State of São Paulo, Brazil. Change Ectrópio Ptose Triquíase Entrópio Epibléfaro Nº cases 14 19 22 1 1 Sex 78.5% 63.1% 59% 100% 100% Rev Bras Oftalmol. 2015; 74 (4): 231-4 males females males males females Skin color 100% 84,2% 86.3% 100% 100% white white white white brown Complaints BAV PP (50%) /Hyperemia(42.8%) 52.6% BAV PP 63.6% BAV PP 100% whatery eyes BAV PP and Hyperemia Surgical treatment 28.5% 26.3% 72.7% 0% 0% 233 Eyelid disorders: frequency of occurrence and profile of carriers in a Brazilian population sample Figure 1: Frequency of occurrence of eyelid changes in inhabitants of the Midwest region of the State of São Paulo - Brazil DISCUSSION The main value of the present study was that the evaluation was performed in a randomized population sample, which allowed us to know the frequency of occurrence of eyelid position changes in the general population without considering convenience samples. Knowing the frequency of occurrence of eyelid changes is interesting due to characteristics of individuals living in a given area, as it is important to plan the training for residency programs. The most frequent change found in the eyelids was trichiasis, which is an acquired condition usually due to chronic inflammation of the eyelid margin as blepharitis and meibomites, cicatrization conjunctival diseases and cicatrization anomalies of the eyelid margin associated or not to previou surgeries 4. Dermatoses as well as the effect of solar radiation on the delicate skin of the lower eyelid are also important2 with the coincidence of trichiasis being observed primarily in white men who probably worked exposed to the sunlight, as the area under study is primarily agricultural. Another cause of trichiasis and entropion is trachoma, which was very prevalent in the rural area of São Paulo at the beginning of last century, with the characteristic of affecting the upper eyelid where the tarsal plate is wider and being reported that the disease is more frequent in women5,6. Ptosis was observed in 0.24% of the study population, predominantly in females and white people. The prevalence of ptosis in another region was higher than that observed in the present study7, probably due to the presence of older patients in that group of patients or the type of selection that was proposed for the studies. There is no sufficient data available about the frequency of occurrence of ptosis, but it is known that there is equal frequency among different races and between sexes8. The surgery was performed in only 26.3% of patients with ptosis. Surgical treatment is mandatory only in severe ptosis which can lead to serious functional deficit9. Ectropion corresponds to the lower eyelid eversion and may be due to congenital or acquired causes, and the involutional type is the most frequent one10. A study involving only the elderly in São Paulo pointed out the prevalence of ectropion in 2.9% of cases, whereas in the general population we found ectropion in 0.18%. It was found mostly in males and white people, with the consensus that men are more prone to eye disorders, perhaps due to having professions in which they are more exposed to risk factors11. Several patients with ectropion (42.8%) had ocular hyperemia, which can be explained by the concomitance of meibomitis, blepharitis and keratitis with the ectropion position of the eyelid2,12. However, the surgery was performed in only 28.5% of cases, most likely due to the non-adherence to surgical treatment of patients who did not have great complaints. Regarding entropion, the frequency of occurrence was 0.01%, while an entropion of 2.1% have been found when assessing only the elderly. The involutional entropion is the most frequent, and affects only the lower eyelid14. The epiblepharon is clearly influenced by race, being much more frequent in Japanese children, with a prevalence of 4.3%, with no sex preference, with lower eyelids affected and bilateral involvement15. It is rare in our country, being detected in 0.01% of the study participants. By representing a skin fold, most often in the lower eyelid and pushing the eyelashes against the eye bulb2 which can be reduced with the growth of the face in general, surgery is not necessary, as it happened to the subject who was part of this study. It is very important to point out that the vast majority of patients with eyelid position changes complained only about concomitant refractive errors, which values the need for comprehensive eye exams. CONCLUSION The most present eyelid change in the general population of a region of São Paulo, Brazil was trichiasis, followed by ptosis and ectropion. The authors emphasize the fact that patients have no complaints about the changes of the eyelid position. REFERENCES 1. Schellini AS, Zimmermann GPM, Hoyama E, Padovani CR, Padovani CRP. Alterações da margem palpebral associadas ao ectrópio. Arq Bras Oftalmol. 2005; 68(5):619-22. 2. Matayoshi S, Forno EA, Moura EM. Manual de cirurgia plástica ocular. São Paulo: Roca; 2004. 3. Vital Filho J, Cruz AA, Schellini AS, Matayoshi S, Figueiredo AR, Herzog Neto G. Órbita, sistema lacrimal e oculoplástica. 3a ed. Rio de Janeiro: Cultura Médica, Guanabara Koogan; 2013. 4. Hirai FE, Shiguematsu AI, Schellini SA, Padovani CR. Tratamento cirúrgico da triquíase maior. Rev Bras Oftalmol. 1998;57(5):357-61. 5. Muñoz B, Bobo L, Mkocha H, Lynch M, Hsieh YH, West S. Incidence of trichiasis in a cohort of women with and without scarring Int J Epidemiol.1999, 28(6):1167-71. 6. Khandekar R, Mohammed AJ. The prevalence of trachomatous trichiasis in Oman (Oman eye study 2005). Ophthalmic Epidemiol. 2007, 14(5):267-72. 7. Van-Langston D. Manual de oftalmologia: diagnóstico e tratamento. 4a ed. Rio de Janeiro: Ed Medsi; 2001. 8. Finsterer J. Ptosis: causes, presentation, and management. Aesthet Plast Surg. 2003;27(3):193-204. 9. Soares EJ, Figueiredo AR, Souza GL, Almeida HC, Oliveira LR, Magalhães MM, Portellinha WM. Blefaroptose. In: Soares EJ, Moura EM, Gonçalves JOR, ed. Cirurgia plástica ocular. São Paulo: Rocca; 1997. p.77-152. 10. Cruz AA, Chahud F, Guimarães FC. Patologias dos anexos oculares. Medicina(Ribeirão Preto). 1997;30(1):36-51. Rev Bras Oftalmol. 2015; 74 (4): 231-4 234 Wanzeler ACV, Nascimento MF, Sousa RLF, Padovani CR, Schellini SA 11. Romani FA. Prevalência de transtornos oculares na população de idosos residentes na cidade de Veranópolis - RS, Brasil. Arq Bras Oftalmol. 2005;68(5):649-55. 12. Veloso CE, Schellini SA, Padovani CR, Padovani CR. Ectrópio palpebral: características e relação com alterações óculopalpebrais. Rev Bras Oftalmol. 2006;65(3):147-51. 13. Damasceno RW, Osaki MH, Dantas PE, Belfort Jr R. Involutional entropion and ectropion of the lower eyelid: prevalence and associated risk factors in the elderly population. Ophthal Plast Resconstr Surg. 2011;27 (5): 317-20. 14. Kersten RC, Hammer BJ, Kulwin DR. The role of enophthalmos in involutional entropion. Ophthal Plast Reconstr Surg. 1997;13(3):195-8. Rev Bras Oftalmol. 2015; 74 (4): 231-4 15. Hayasaka Y, Hayasaka S. Epiblepharon with inverted eyelashes and high body mass index in Japanese children. J Pediatr Ophthalmol Strab. 2005;42 (5):300-3. Corresponding author: Ana Cláudia Viana Wanzeler Rua Antônio Amando de Barros, 241 – Botucatu (SP) ZIP Code: 18601-260 Email: [email protected] ORIGINAL ARTICLE235 Patient’s perception on glaucoma and different types of treatment (medical versus surgical treatment) Percepção dos pacientes portadores de glaucoma sobre sua doença e os diferentes tipos de tratamento (clínico versus cirúrgico) Augusto Alves Pinho Vieira1, Ricardo Augusto Paletta Guedes2, Rita de Cássia Padula Alves Vieira3, Vanessa Maria Paletta Guedes4 ABSTRACT Objective: To identify the meaning and impact on their quality of life of having glaucoma and to understand the patients’ perception on the different types of treatment (medical or surgical). Methods: Through a qualitative research, focus groups were conducted with patients in clinical treatment (group 1) and patients who underwent glaucoma surgery in both eyes and were without medication (group 2). The responses were analyzed using the technique of content analysis. Results: Fear of blindness and lack of information about the disease were the most cited issues in relation to how it is like to having glaucoma. Medication costs, impact of drops on patients’ daily lives and the side effects were the main points discussed in relation to medical treatment. All patients in the surgical group preferred the current situation (without medication) when compared to the need for chronic use of medication. In the two groups, both glaucoma and its treatment had a profound impact on people, not only from a psychological standpoint, but also affecting their daily lives. Patients operated on for glaucoma appear to have less impact on their daily lives, but the concern about the disease persists. Conclusion: We identified the most significant negative aspects of glaucoma and its treatment from patients’ perspectives. Confidence in the correct indication of the type of treatment, clinical or surgical, and a solid relationship between the patient the doctor are determining factors for extra peace of mind of patients being treated for glaucoma. Keywords: Glaucoma, open-angle/psychology; Glaucoma, open-angle/therapy; Glaucoma, open-angle/surgery; Quality of life RESUMO Objetivo: Identificar a percepção dos pacientes sobre o significado de ser portador de glaucoma e a percepção que tem sobre o tratamento clínico ou cirúrgico. Métodos: Para a coleta dos dados utilizou-se a pesquisa qualitativa através da estratégia de grupos focais realizados com pacientes em tratamento clínico (grupo 1) e pacientes submetidos à cirurgia antiglaucomatosa (grupo 2). A análise e a interpretação dos resultados foram feitas pela técnica da análise de conteúdo. Resultados: O medo da cegueira e a desinformação sobre a doença foram os aspectos negativos mais encontrados com relação a ser portador de glaucoma. O grupo cirúrgico preferiu a situação atual quando comparada à necessidade do uso de medicação. Verificou-se que tanto o glaucoma quanto o seu tratamento impactaram profundamente esses pacientes e que, embora a preocupação com a doença ainda persista, os pacientes operados demonstraram apresentar menos impacto no seu cotidiano. Foram determinantes para a aceitação da indicação da cirurgia a falta de controle da doença e a confiança no médico, sendo esta última considerada um fator primordial nos dois grupos pesquisados, o que aponta para sua importância, independente da decisão tomada pelo paciente na convivência com sua doença. Conclusão: Identificaram-se os aspectos negativos mais relevantes com relação ao glaucoma e ao seu tratamento. A confiança na correta indicação do tipo de tratamento, clínico ou cirúrgico, e uma relação sólida entre o paciente o médico são os fatores determinantes para uma maior tranquilidade dos pacientes em tratamento de glaucoma (clínico ou cirúrgico). Descritores: Glaucoma de ângulo aberto/psicologia; Glaucoma de ângulo aberto/terapia; Glaucoma de ângulo aberto/cirurgia; Qualidade de vida Hilton Rocha Foundation, Belo Horizonte, MG, Brazil. Federal University of Juiz de Fora, Juiz de Fora, MG, Brazil. 3 College of Health and Medical Sciences of Juiz de Fora, Juiz de Fora, MG, Brazil. 4 Ophthalmology Service of the Charity Hospital of Juiz de Fora, Juiz de Fora, MG, Brazil. The authors declare no conflicts of interest Received for publication 04/03/2015 - Accepted for publication 29/03/2015 1 2 Rev Bras Oftalmol. 2015; 74 (4): 235-40 236 Vieira AAP, Guedes RAP, Vieira RCPA, Guedes VMP INTRODUCTION T he maintenance and/or improvement of the quality of life at a reasonable cost should be seen as the highest goal of the glaucoma treatment.1,2 The quality of life is closely related to: the stage of visual function damage of the patient; the psychological impact of the disease and its treatment; the doctor-patient relationship; the cost and side effects of the treatment; the independence to perform household and work tasks, such as driving and reading; the inconvenience of instilling eyedrops; and disbelief in its true usefulness and efficiency due to missinformation. 3-11 To achieve properly and efficiently the goal of the glaucoma treatment, patient education and counselling by the doctor are very important in the pursuit of establishing a therapeutic regimen capable of overcoming the following barriers: age, ethnicity, sex and social class.2,4 There are also other more subjective factors that may serve as barriers to the treatment proposed, such as: values, beliefs and culture of the patients.11,12 Basically the glaucoma treatment is accomplished through the proper control of intraocular pressure, which may be done with medication (eyedrops), laser or surgery.13The guidelines for glaucoma treatment advise to always start the treatment with eyedrops, and classically surgery is left for cases where medical treatment is not well indicated (intolerance, cost, low adherence and persistence) or is not enough.14,15 There is no evidence in the literature of what kind of glaucoma treatment is preferred by the patients. What is the impact of having glaucoma for the patient? What do they think about the treatment? How is the possible need for surgery understood and how it influences the treatment? These are some examples of questions that would be very difficult to be answered with a quantitative methodology. In the medical literature qualitative studies that attempt to clarify the beliefs and values assigned by glaucoma patients themselves to the type of treatment (medical or surgical) proposed by the doctor are virtually absent. This study aimed to identify, from the perspective of patients, the meaning of being a glaucoma carrier, emphasizing the impact of this disease on their quality of life and in the perception (values, beliefs, fears) that had about the type of treatment (clinical versus surgical). METHODS The clinical data of the patients was obtained through the analysis of their medical records, and were used to characterize the research participants. The study groups were formed of patients in clinical treatment (group 1) and patients who had undergone the glaucoma surgery (group 2), and the criteria for inclusion in the study were: patients over 21 years old with controled and in advanced stage primary open-angle glaucoma (index Mean Deviation of computerized campimetry < -12.00 dB) in at least 1 eye. In group 1 patients were in continuous use of antiglaucoma eyedrops in both eyes, and in group 2 they underwent surgery in both eyes at least one year before. We excluded those patients who had been operated and that had returned to the chronic use of antiglaucoma eyedrops, as well as patients whose desease were not considered controlled by the attending physician (Table 1). The selection of patients who meet the inclusion criteria was made through invitation to them when they went to their appointment consecutively until completing the number of 10 patients per group. All the patients read, agreed and signed the Informed Consent Term approved by the Research Ethics Committee of the SCMJF. For the focal group, we used a script of questions previously elaborated based on guiding questions (Example: How do you deal with the fact of having glaucoma? What do you think about the treatment? How do you understand the need for surgery and how it influences the treatment?). The questions were pre-tested with patients with the same characteristics of the future survey subjects. The meetings with the groups were in different days, and data collection was interrupted when the “saturation point” was reached, i.e., when information obtained during the group dynamics and the interviews became recurrent. The discussions and interviews were recorded on electronic media, and later literally transcribed. The content obtained was organized and categorized along with the document research based on the operation summarized in Minayo16, which consists of three steps: pre-analysis; study of the material; and treatment of the results obtained and interpretation. The procedures for the data analysis were based on the content analysis technique. Finally, the data obtained was related to the theoretical framework adopted, in order to apprehend the subjects’ perception on the core question of this study, i.e., the perception of subjects surveyed about glaucoma and its treatment. RESULTS The method proposed for this study is based on the assumptions of qualitative research, where we work with the notions of meaning, beliefs, aspirations, reasons, values and attitudes, seeking an approch with the object of study, as proposed by Minayo.16 The field of study chosen was a private clinic specialized in glaucoma, and the research project was approved by the Research Ethics Committee of the Charity Hospital of Juiz de Fora (SCMJF) by Opinion No. 040/2011. As methodological strategy for collecting data, this study used focus groups (discussions and presentation of ideas in group) and individual semi-structured interviews, when necessary, used to complement the data obtained during the group discussion. Rev Bras Oftalmol. 2015; 74 (4): 235-40 From the 10 patients selected to bex each sample group, only 9 attended the meeting. The characteristics of each one of the participants are described in Table1, and the subjects in group 1 are coded by numbers (1 to 9) and in group 2 by letters (‘A’ through ‘I’). The medical discourse and common sense contribute at the same time to the meaning of the “having glaucoma”, unanimously translated by fear of blindness, mentioned several times by the subjects interviewed (Table 2). Some patients have reported lack of knowledge about glaucoma before being diagnosed with the disease. Speeches like “I got gcared for not Patient’s perception on glaucoma and different types of treatment (medical versus surgical treatment) 237 Table 1 Características dos participantes da pesquisa: Group 1: Clinical treatment Patient Patient Patient Patient Patient Patient Patient Patient Patient 1 2 3 4 5 6 7 8 9 Group 2: Clinical treatment Patient Patient Patient Patient Patient Patient Patient Patient Patient A B C D E F G H I Age (years) 75 63 69 65 93 72 63 72 83 Age (years) 78 59 80 55 81 47 70 68 58 Ethnicity Sex Education white black black black white white white white white M F F F F M F M M High school Elementary Graduated Elementary Elementary Graduated Elementary Elementary Graduated Ethnicity Sex Education black black white white white white white white white M F F M F M F F F Elementary Elementary High school Graduated High school Elementary Graduated High school Elementary knowing it” (Patient 1) and “I had never heard about this particular desease” (Patient 1) are examples of how lack of knowlege can generate an even greater negative impact in the diagnosis of glaucoma. Patients mentioned that giving up activities that gave them pleasure or that were part of their routine was a difficult change to accept. Some examples are as follows: “I stopped working earlier than I wanted to. For example, driving. I’ve always wanted to get my license, but I never could (Patient 6); “When I knew I Table 2 Examples of speeches about the subjet “having glaucoma”. Patient 4 “At first, I was very worried about blindness. I couldn’t read.” Patient 5 “Really worried about being blind. I was afraid of falling; I was really concerned.” Patient 8 “I heard glaucoma was blindness for sure. But the doctor said it wasn’t true at all.” Patient 9 “I got, like, really worried. My mother was blind before dying.” had glaucoma, I had to stop working, and now I don’t work anymore, you know…” (Patient 7). During the meetings of the focus groups, the speeches about the use of eyedrops were recurrent, even in patients who had Time since the discovery of the disease (anos) 7 3 10 11 2 4 15 1 20 Time since the discovery of the disease (anos) 12 25 16 13 6 34 26 30 10 Number of droplet per day per eye 5 3 1 5 6 3 6 3 3 Number of droplet per day per eye 2 5 3 3 2 5 5 4 3 undergone surgery and were no longer using them. The need for chronic use of eyedrops generated discussions related to the concern of relying on an expensive drug, as well as the discomfort represented by the change of routine due to the care involved in the correct use of eyedrops. Patients in the clinical group were the ones who talked the most about the cost of the drug treatment. All patients in this group were unanimous when reporting the problems related to the chronic use of medication. Table 3 gives some examples of speeches about the patients’ perception on the routine of the chronic treatment with eyedrops. The pharmacological treatment then becomes a necessary discomfort, according to the speeches of all patients interviewed. In the clinical group, living with the eyedrops is considered a dependence of which they complain, claiming concern for forgetting or having difficulties in the transportation because of the need to keep some medicines under refrigeration. The concern with time was dominant, and some even affirmed they make use of the most diverse and creative resources, such as the use of warnings or “timers”. In the surgical group we noted a kind of freedom in relation to such routine. This group showed satisfaction with the freedom that surgery provided; however, they were still concerned about the disease and the possible need to use the medication again. Table 4 shows examples of speeches about the patients’ perception regarding the surgical treatment of glaucoma. Side effects were remembered by patients in the surgical group, such as: bitter taste, blurred vision after instillation, dry eye and allergy, confirmed by the patients in the clinical group, which still make chronic use of same. Rev Bras Oftalmol. 2015; 74 (4): 235-40 238 Vieira AAP, Guedes RAP, Vieira RCPA, Guedes VMP Table 3 Table 4 Examples of speeches about the difficulties and concerns an the clinical treatment of glaucoma Examples of speeches about the patients’ perception regarding the surgical treatment: Patient A “...anyway I would choose surgery... eyedrops are expensive and you’ll be using and not solving the problem of pressure.””…but the doctor seems confident.” Patient B “…I really prefer the surgery. And trust in God first and then the doctor.” Patient D “...surgery is the last stage.””So I think there are many risks in it (Authors’ note: regarding the indication of treatment), especially the trust relation between the patient and the doctor. Many times the doctor is more important than the medical or surgical treatment.” Patient E “...I feel better after the surgery because I think I’m free from the evil....””And when we find a doctor who gives us attention, who speaks clearly, objectively, we trust them and go on.” Patient F “…I trust better the surgery. Surgery nipped the evil in the bud.” Patient G “…my eye got very red when I instilled eyedrops. I prefer surgery.”””..in my case eyedrops were not working, so I had to go on surgery. But always trusting, because I knew God and the doctor were there for me.” DISCUSSION Patient H “The eyedrops were not working for me… I was afraid of being blind.””We must trust the doctor.” When trying to understand the meaning of “having glaucoma”, other aspects should be considered besides the biological and physiological ones, and the treatment of the sick body. The glaucoma patient assimilates what society offers in terms of values, information, ideas, and theories, building from that their own history, becoming a socio-historical-cultural being. 17,18 The visual assessment itself is often more valued (clinical data of ophthalmological examination) than the impact of vision loss, or even the threat that this loss may represent on these people lives, because “having glaucoma” is the same as no longer being productive, no longer being independent, is facing the unknown, a situation the patient fears. The lack of information about the disease and the fear of blindness were themes really mentioned by the patients in this study. “Having glaucoma” for some patients means certain blindness, and the lack if information generated anxiety and fear about the disease. Education about the disease becomes important not only to the patient already diagnosed with the disease, but also to the general population. A more conscious society on glaucoma would help reduce the psychological impact of “having glaucoma”. The clinical treatment of glaucoma can paradoxically compromise the quality of life of the patient. Need for chronic use of medication, possible side effects, concerns and anxieties Patient I “...I am allergic to drops. I can not use any eyedrops! So I had to go on surgery, you know...””...I also prefer the surgery because I really trust the doctor. First God, then her.” Patient 2 “Besides price, what I think is absurd is the amount. The amount is minimal! If we miss one drop, it is worth gold!” Patient 3 “In one month the situation got worse: three people using eyedrops” (in the family). Patient 4 “But it’s so expensive, so expensive that I came came up with the decision of asking the doctor if I could change the medicine” Patient 2 “I put my eyedrops in two shelves, in the bathrooms... with a warning!” Patient 6 “To me, it’s so bad to use eyedrops every ten minutes. I need a timer… to track time.” Patient 8 “In this sense, this thing of instilling eyedrops at a certain time bothers me and makes me very uncomfortable.” For patients in surgical treatment group, the main motivation for undergoing surgery was the medical indication, given the inability to control glaucoma only with topical medication. The fear of being blind, even though in treatment with eyedrops, made patients accept the surgical indication as a valid option. Rev Bras Oftalmol. 2015; 74 (4): 235-40 about the daily routine of treatment are some examples mentioned by patients in the presnet study about the negative impact on the quality of life of the patients chronicaly using eyedrops. Another important factor is the cost of the treatment. Speeches like type “each droplet is worth gold” were reccurent during the interviews. The need to sacrifice part of the family budget also has a big impact, since the patient gives up “extra” activities. Such activities which rely on part of their salary now spent on medication could represent an improvement of the same quality of life. In this context are includes trips, special meals, leisure, among others. Glaucoma and its chronic course requires prolonged treatment and follow-up, and a high cost that can compromise 25% or more of the patient’s family income. A Brazilian study found out that the lack of financial resources was reported by 47.6% of respondents as the main cause of treatment discontinuation, making the adhesion difficult and being responsible for the loss of visual field.8 The difficulties in using Patient’s perception on glaucoma and different types of treatment (medical versus surgical treatment) eyedrops are added to the cost itself, since each lost droplet has to be administered again. Studies comparing the different kinds of glaucoma treatment using the quality of life as an outcome are rare. Encouraged by the clinical impression that the glaucoma-operated undergoing have a better quality of life than those in chronic use of eyedrops, researchers in the United States (Collaborative Initial Glaucoma Treatment Study - CIGTS), randomized newly diagnosed glaucoma patients for clinical or surgical treatment (Trabeculectomy). Both groups had worse quality of life indexes soon after the diagnosis. The indexes were improving during the follow-up (9 years), demonstrating that patients tend to get used to the disease and its treatment. Patients in the surgical group had a slight worsening of quality of life in the early postoperative stage, directly linked to the local effects of the surgery. In the long term, the quality of life indexes did not differ. 19 In Brazil, Paletta Guedes et al. identified, also by means of a questionnaire, that patients with early-stage of glaucoma showed an association between surgical treatment and lower indexes of quality of life, which did not happen to more advanced stages of the disease. The most affected dimension in these cases was the psychological one, leading to the belief that a surgery for early glaucoma patients can give a great psychological impact.20 The question of patient preference on the type of treatment (medical or surgical) is difficult to be elucidated with quantitative research, as mentioned above. The CIGTS could not answer this question, and it can be seen in the research of Paletta Guedes et. al. 20 that choosing the type of treatment may have a nonnegligible psychological impact for some patients. Before surgery, the patients in this study who had undergone surgical treatment were chronic users of eyedrops for a long time, and now were free of this commitment. So they had a unique condition of having lived the problem both from a clinical treatment point of view and from the point of view of the surgical treatment. When asked about their preference between the two conditions (clinical treatment versus surgical treatment), they were unanimous in reporting that they preferred surgery, and despite the discomfort of using eyedrops, confidence in the medical indication and a good control of the disease were the most important factors for this treatment option. Confidence in the indication of the type of treatment, clinical or surgical, and a solid relationship between doctor and patient are the most important findings of the present study. A similar result was found by Lemaitre et al.21 In a study carried out with glaucoma patients who required a filtering surgery, these authors found that both the disease and the surgical procedure are sources of anxiety. The relationship between doctor and patient and the confidence in the indication of the treatment appeared as key to decreasing the preoperative anxiety reported by the patients.21 A limitation of the present study is that the sample may not be representative of the entire population of primary openangle glaucoma patients. This fact is inherent in any survey conducted by the qualitative method because it is intended to deepen the most the question to be answered, and not generalize it. The saturation point for the qualitative methodology is an indication that a larger sample would be unnecessary to achieve the goal proposed in this research. A deep understanding of values, beliefs, concerns, anxieties and fears is only possible by means of a qualitative research. Another limitation is that patients in the surgical group may have been influenced by the conduct of the attending 239 physician (type of surgical technique). Also as a limitation we can mention the fact that the research was conducted in a private practice environment, which may influence the perception of the patients. We believe that values, beliefs and culture base are different between patients attending a private clinic and those who are seen at the Single Health System (SUS). Another similar study with patients enrolled in the Single Health System (SUS) could clarify this point. However, these limitations do not invalidate our results. In conclusion, glaucoma gives patients a deep sense of fear and concern not about the loss of vision, but also about the impact of the disease and its treatment on their daily lives. The cost and side effects of the clinical treatment were the main negative factors raised by the patients. The patients in the surgical group were unanimous in preferring surgery in relation to the chronic use of eyedrops. Glaucoma-operated patients seem to have less negative impact on their daily lives, but the concern about the disease persists. The confidence in the doctor and the correct indication of proper treatment, be it clinical or surgical, is a major factor for extra peace of mind of the patient. The ophthalmologist is privileged with regard to the possibility of contributing to the reduction of the patient’s anxiety about the procedures necessary to a better quality of life. REFERENCES 1. Dietlein TS, Hermann MM, Jordan JF. The medical and surgical treatment of glaucoma. Dtsch Arztebl Int. 2009; 106(37):597-606. 2. Silva LR, Paula JS, Rocha EM, Rodrigues ML. Fatores relacionados à fidelidade ao tratamento do glaucoma: opiniões de pacientes de um hospital universitário Arq Bras Oftalmol. 2010; 73(2):116-9. 3. Hong S, Kang SY, Yoon JU, Kang U, Seong GJ, Kim CY. Drug attitude and adherence to anti-glaucoma medication. Yonsei Med J. 2010; 51(2):261-9. 4. Kulkarni SV, Damji KF, Buys YM. Medical management of primary open-angle glaucoma: best practices associated with enhanced patient compliance and persistency. Patient Prefer Adherence. 2008; 2:313-4. 5. World Health Organization (WHO)/ International Agency for the Prevention of Blindness. Data Vision 2020: the right to sight. Global initiative for the elimination of avoidable blindness: action plan 2006-2011. Geneva: WHO International Agency for the Prevention of Blindness; 2007. 6. Mello PA, Melo Júnior LA. Glaucoma dos nossos dias: revendo conceitos e custos. Rev Bras Oftalmol. 2003; 62(9):669-77. 7. Ramulu P. Glaucoma and disability: which tasks are affected, and at what stage of disease? Curr Opin Ophthalmol. 2009; 20(2):92-8. 8. Silva LM, Vasconcellos JP, Temporini ER, Costa VP, NewtonCara J. Tratamento clínico do glaucoma em um hospital universitário: custo mensal e impacto na renda familiar. Arq Bras Oftalmol. 2002;65(2):299-303. 9. European Glaucoma Society (EGS). Terminology and guidelines for glaucoma. 3a ed. Savona: Dogma; 2008. 10. Severn P, Fraser S, Finch T, May C. Which quality of life score is best for glaucoma patients and why? BMC Ophthalmol. 2008;8:2. 11. Lacey J, Cate H, Brodway DC. Barriers to adherence with glaucoma medications: a qualitative research study. Eye (Lond). 2009; 23(4):924-32. 12. Almeida LD, Machado MC. Atitude médica e autonomia do doente vulnerável. Rev Bioética. 2010;18(1):165-83. Rev Bras Oftalmol. 2015; 74 (4): 235-40 240 Vieira AAP, Guedes RAP, Vieira RCPA, Guedes VMP 13. Leske MC, Heijl A, Hyman L, Bengtsson B, Komaroff E. Factors for progression and glaucoma treatment: the early manifest glaucoma trial. Curr Opin Ophthalmol. 2004;15(2):102-6. 14. Nayak B, Gupta S, Kumar G, Dada T, Gupta V, Sihota R. Socioeconomics of long-term glaucoma therapy in India. Indian J Ophthalmol. 2015;63(1):20-4. 15. Heijl A, Leske MC, Bengtsson B, Hyman L, Bengtsson B, Hussein M; Early Manifest Glaucoma Trial Group. Reduction of intraocular pressure and glaucoma progression: results from the early manifest glaucoma trial. Arch Ophthalmol. 2002;120(10):1268-79. 16. Minayo MCS. O desafio do conhecimento: pesquisa qualitativa em saúde. 9a ed. São Paulo: Hucitec; 2006. 17. Cintra FA, Sawaia BB. A significação do glaucoma e a mediacão dos significados de velhice na perspectiva Vygotskiana: subsídios para a educação à saúde. Rev Esc Enferm USP. 2000; 34(4): 339-46. 18. Vigotsky LS. A formação social da mente. São Paulo: Martins Fontes; 1994. Rev Bras Oftalmol. 2015; 74 (4): 235-40 19. Burr J, Azuara-Blanco A, Avenell A. Medical versus surgical interventions for open-angle glaucoma. Cochrane Database Syst Rev. 2007; (4):CD004399. 20. Paletta Guedes RA, Paletta Guedes VM, Freitas SM, Chaoubah A. Quality of life of medically versus surgically treated glaucoma patients. J Glaucoma. 2012; 22(5):369-73. 21. Lemaitre S, Blumen-Ohana E, Akesbi J, Lapalce O, Nordmann JP. Evaluation of preoperative anxiety in patients requiring glaucoma filtration surgery. J Fr Ophtalmol. 2014; (1):47-53. Corresponding author: Augusto Alves Pinho Vieira. Rua Dr. Asclepíades da Paixão Lucas 147, Portal da Torre. 36037-462 Juiz de Fora MG. Phone:(32) 3231 2111; (31) 8811 3691 E-mail: [email protected] CASE REPORT 241 X-linked juvenile retinoschisis Retinosquise juvenil ligada ao X Cesar Gomes da Silveira1, Gabriela Hertz Soares2, Jacqueline Provenzano3 ABSTRACT Report the case of a male 28 years-old patient, who was referred to Centro de Estudos e Pesquisas Oculistas Associados – RJ, to retina assessment and presented the tipical findings of the X-Linked Juvenile Retinoschisis: A cystoid maculopathy with formation of foveal cysts and schisis of the peripheral retina. It was carried out the conservative management, with attention to the complications. Keywords: Retinoschisis/diagnosis; Genetic diseases, X-linked/diagnosis; Case reports RESUMO Relatar o caso de um paciente masculino de 28 anos, que foi encaminhado ao Centro de Estudos e Pesquisas Oculistas Associados – RJ, para avaliação de retina e apresentou os achados típicos de Retinosquise Juvenil Ligada ao Cromossomo X: maculopatia cistóide com formação de cistos na fóvea e retinosquise periférica. Foi realizado o manejo conservador, com atenção para as complicações. Descritores: Retinosquise/diagnóstico; Doenças genéticas ligadas ao cromossomo X/diagnóstico; Relatos de casos 1 3 Third-year resident physician of the Study and Research Center Opticians Associates - Rio de Janeiro, RJ, Brazil. PhD at. Head of the Study and Research Center Opticians Associates - Rio de Janeiro, RJ, Brazil. The authors declare no conflicts of interest Received for publication 18/11/2011 - Accepted for publication 20/01/2013 Rev Bras Oftalmol. 2015; 74 (4): 241-3 242 Silveira CG, Soares GH, Provenzano J INTRODUCTION X -linked juvenile retinoschisis (XJR) is a inherited recessive vitreoretinal degeneration more common in young men characterized by bilateral maculopathy with associated peripheral retinoschisis in 50% of patients. (1-6) A prevalence of 1:5000 to 1:28000 is estimated.(1,3) There are descriptions of mutations in the XLRS1 gene(13,7) , responsible for coding of retinoschisis - a protein that provides adhesion and interaction among cells and among the retinal layers. Defects or absence of its secretion may reduce the adherence between the layer of nervous fibers and the remainder of the sensory retina, forming cystic cavities.(1,6) XJR manifests with reduced visual acuity (VA) between the ages of five and ten years of age, and evolves with progressive visual loss during the first two decades of life. There is the possibility of stabilization of the VA until the fifth or sixth decade, when it can worsen due to macular atrophy, no longer showing the cystic aspect.(5) The visual acuity may be less than 20/200, keeping an average of 20/70 in young adults. Abnormalities in the angle of the anterior chamber such as occlusion angle, strabismus and nystagmus are described as other findings. Vitreous hemorrhage and retinal detachment are the main complications.(1,3,5) The foveal retinoschisis is characterized by the “wagon wheel” standard of radial streaking due to changes in the layer of nerve fibers related to a defect of the Müller cells.(8) Despite the cystic appearance, the exam of fluorescein angiography does not evidence the progressive extravasation characteristic of cystoid macular edema and contributes to the differential diagnosis between pathologies. (8) Peripheral retinoschisis predominantly involves the inferior temporal quadrant, often with large detachments of the inner retinal layers. These changes of the inner layers of the retina predispose vitreous hemorrhage and retinal detachment.(8) of macular and peripheral retinal images. These findings corroborate the diagnosis of X-linked juvenile retinoschisis. A new fluorescein angiography (Figure 3) was made in 2011 showing similar appearance to that found in the previous exam. The exam of optical coherence tomography (OCT) (Figure 4) also held in 2011 showed an image of subfoveolar cystic confluence, further changing the fovea architecture and justifying the visual impairment. Figure 1: Simple retinography (on the left): macular changes in retinoschisis or “wagon wheel”. Fluorescein angiography (on the right): absence of contrast extravasation. 2008. CASE REPORT MJS, male, 28, white, single, born and raised in Rio de Janeiro - RJ was referred to the Study and Research Center Opticians Associates - RJ (CEPOA) in February 2011, for retinal evaluation with the diagnosis of XJR. When asked about his family history, he mentioned a brother with whom he is no longer in contact, but who suffers from the same pathology diagnosed. He brought additional exams from 2008, in which the redfree photography showed the standard of foveolar retinoschisis that extends circumferentially to the parafovelar area. Fluorescein angiography demonstrates cystic changes in the macula without fluid leakage through the subcystoid space (Figure 1). Optical coherence tomography (OCT) (Figure 2) shows foveal cysts with retinal cleavage between the outer and inner plexiform layers in both eyes (BE). In the eye exam held on 02/01/2011 the visual acuity was 20/ 60 in BE, with the best correction. The biomicroscopy of the anterior segment shows no changes. The intraocular pressure was 17 mmHg at 04pm in BE. The retinal mapping performed showed a macular image in foveolar retinoschisis and inferior temporal retinoschisis in the right eye. The left eye showed the same pattern Rev Bras Oftalmol. 2015; 74 (4): 241-3 Figure 2: OCT images from 2008. Presence of foveal cysts in both eyes. DISCUSSION X-linked juvenile retinoschisis is a relatively rare disorder which determines low visual acuity, mainly by foveolar retinoschisis.(1-6) The inferior temporal bilateral presentation is considered the classic pattern of disease, and the most frequent complications and of worst prognosis are vitreous hemorrhage and retinal detachment.(5) 243 X-linked juvenile retinoschisis The treatment aims to prevent complications that increase visual loss, since nothing has been proven effective in preventing the development of the disease.(2) The possibility of treatment with topical dorzolamide is being studied, but still remains unproven. (6,9,10) In cases of vitreous hemorrhage, some authors suggest the use of photocoagulation of the vessels responsible for the bleeding.(11,12) But in cases of retinal detachment, a tamponade on the rupture and vitrectomy via pars plana are indicated.(2,11) Children who have concomitant strabismus deserve attention, and factors that can induce amblyopia should be minimized. Aid for low vision, and adaptive skills training can help individuals who develop visual loss. Genetic counseling can help identify family members who are carriers of the gene XLRS1, in order to avoid further damage.(2) REFERENCES Figure 3: Simple retinography (on the left): macular changes in retinoschisis or “wagon wheel”. Fluorescein angiography (on the right): absence of contrast extravasation. 2008. Figure 4: OCT images from 2011. Presence of foveal cysts in both eyes The fluorescein angiography reaffirms the diagnosis, ruling out the possibility of cystoid macular edema, since there is no extravasation of dye through the macula.(4,5) The optical coherence tomography (Figures 2 and 4) show changes in the evolving foveolar architecture (foveal thickness changes in BE), resulting from cysts on the layer of nerve fibers. These cystic formations are also found in the retinal periphery, where they may break to the vitreous and the retina, causing retinal ruptures and hemorrhages.(1,5) The electroretinogram is important in the diagnosis of this disease. The wave amplitude A is normal or close to normal, but wave B has a very reduced amplitude. This reduction in the wave of the B is justified by the change in the initiation of the electrical impulse in the Müller cells.(5) Literature considers the possibility of stabilization of VA around 20/70 during the second decade of life, with possible progression to atrophic maculopathy around 60 years old.(5,9) 1. Song MK, Small KW, Jayne RP, Law SK, Charles S, Brown LL, et al. Retinoschisis, juvenile [Internet]. [cited 2013 Jan 12]. Available from: http://emedicine.medscape.com/article/1225857-overview. 2. Kugler M. Juvenile retinoschisis: causes progressive loss of vision [Internet]. [cited 2013 Jan 13]. Available from: http:// rarediseases.about.com/od/rarediseasesr/a/retinoschisis05.htm 3. Puech B. X-linked juvenile retinoschisis. Orphanet Encyclopedia. May 2004. Disponível em: http://www.orpha.net/data/patho/GB/ uk-XLRS.pdf 4. Edwards AO, Robertson JE. X-linked juvenile retinoschisis. In: Ryan SJ, editor. Retina. 3rd ed. St. Louis: Mosby; 2001. p. 487-90. 5. Cunha AA, Picanço BC, Almeida GA, Rodrigues NH, Rocha GM. Retinosquise juvenil: relato de caso. Arq Bras Oftalmol. 2008;71(6):878-80. 6. Caye LM, Barbosa PH, Scheid KL, Cardoso IH, Fortes Filho JB. Uso da dorzolamida tópica em paciente portador de retinosquise juvenil ligada ao X. Rev Bras Oftalmol. 2010;69(2):129-31. 7. Sauer CG, Gehrig A, Warneke-Wittstock R, Marquardt A, Ewing CC, Gibson A, et al. Positional cloning of the gene associated with X-linked juvenile retinoschisis. Nat Genet. 1997;17(2):164-70. 8. Shukla D, Rajendran A, Gibbs D, Suganthalakshmi B, Zhang K, Sundaresan P. Unusual manifestations of x-linked retinoschisis: clinical profile and diagnostic evaluation. Am J Ophthalmol. 2007;144(3):419-23. 9. Bastos AL, Freitas BP, Villas Boas O, Ramiro AC. Use of topical dorzolamide for patients with X-linked juvenile retinoschisis: case report. Arq Bras Oftalmol. 2008;71(2):286-90. 10. Apushikin MA, Fishman GA. Use of dorzolamide for patients with X-linked retinoschisis. Retina. 2006;26(7):741-5. Erratum in: Retina. 2007;27(1):128. 11. George ND, Yates JR, Moore AT. X linked retinoschisis. Br J Ophthalmol. 1995;79(7):697-702. Review. 12. Gopal L, Shanmugam MP, Battu RR, Shetty NS. Congenital retinoschisis: successful collapse with photocoagulation. Indian J Ophthalmol. 2001;49(4):265-6. Rev Bras Oftalmol. 2015; 74 (4): 241-3 244 CASE REPORT Atypical presentation of Graves’ ophthalmopathy Apresentação atípica da oftalmopatia de Graves Flávia Marques Rodrigues1, Nilson Lopes da Fonseca Junior 2, José Ricardo Carvalho Lima Rehder3 , Celso Lopez Fernandez 4, Debora Mayumi Sugano 5 ABSTRACT Graves ‘ophthalmopathyis themost commonorbital diseaseand affects25-50% of the patients withGraves’ disease. It`s morecommon in females, between the second andfifth life`s decade. The disease hasanacute andachronic stage, slowly progressing until it stabilizes, with rarecasesof spontaneous resolution.The treatment depends on thestage andthe disease ismainly treated withoralor intravenous corticosteroids with or without radiotherapy;colchicine is usedin individual cases. In the followingcase report, we discuss an atypicalmanifestation ofGraves’ ophthalmopathyin an euthyroid patientwith negative antibodiesin the inicial presentation. Keywords: Graves’ ophthalmopathy;Euthyroid;Atypical manifestation; Negative antibodies; Colchicine; Case reports RESUMO A oftalmopatia de Graves é a doença orbitária mais comum e acomete 25 a 50 % dos pacientes portadores da Doença de Graves sendo mais frequente no sexo feminino, entre a segunda e quinta décadas de vida. A doença apresenta uma fase aguda e uma crônica, evoluindo lenta e progressivamente até estabilizar, sendo raros os casos de resolução espontânea. O tratamento dependerá da fase em que a doença se encontra sendo baseado principalmente na corticoterapia via oral e endovenosa e/ou radioterapia, sendo a colchicina empregada em casos isolados. No seguinte relato de caso, abordaremos uma forma atípica de manifestação clínica da Oftalmopatia de Graves em paciente eutireoidéia com anticorpos negativos na sua apresentação inicial. Descritores: Oftalmopatia de Graves; Eutireoidea; Manifestação atípica; Anticorpos negativos; Colchicina; Relatos de casos 1 2 3 4 5 Sector at the Medicine College of ABC – FMABC - Santo André (SP) - Brazil Medicine College of ABC - FMABC - Santo André (SP) - Brazil. FMABC - Santo André (SP) - Brazil. Medicine College of ABC Medicine College of ABC Study conducted in the Discipline of Ophthalmology at the Medicine College of ABC - FMABC - Santo André (SP) - Brazil. The authors declare no conflicts of interest Received for publication 11/06/2012 - Accepted for publication 03/09/2012 Rev Bras Oftalmol. 2015; 74 (4): 244-7 245 Atypical presentation of Graves’ ophthalmopathy INTRODUCTION T he Graves ophthalmopathy is the most common orbital disease, and it affects 25-50% of patients with Graves’ disease(1). It is an autoimmune disease characterized by the deposition of immune complexes antithyroglobulin in the extraocular muscles. In the early stages of the disease, there is an infiltration of adipose, muscle, and connective tissues in the orbit by T lymphocytes, mast cells, macrophages and plasma cells(2-4). It is believed that activated T lymphocytes directed against the thyroid follicular cells recognize and bind to similar antigens present in the orbital tissues. Macrophages and dendritic cells initiate the immune response, which is propagated by the recruitment of sensitized T cells(2-4). Then various inflammatory mediators are released (IFN gamma, TNF, IL-1), which stimulate fibroblasts to produce glycosaminoglycans, which have a hydrophilic characteristic that draws water into the fat, muscle and connective tissues, causing edema and consequently fibrosis of all the periorbit, with hypertrophy of the extraocular muscles, particularly the medial and lower rectus and orbital fat, resulting in increased orbital volume, causing mainly proptosis(2-4). Although the Graves ophthalmopathy is more common between the second and fifth decades of life, it can occur in any age group. It is eight times more frequent in women, but in men the involvement is more serious. It usually occurs when there is thyroid dysfunction, but the ocular or orbital changes may precede or follow the thyroid dysfunction in up to 18 months(2). Currently there are important systems to rate the severity and activity of the disease. In this context we may mention the NOSPECS which includes the following criteria: class 0 for patients who have no signs or symptoms, class 1 for presenting only signs (retraction of upper eyelid, stare, retraction of the upper eyelid to look down and proptosis above 22mm) and without symptoms, class 2 in those with soft tissue involvement (symptoms and signs), class 3 in patients with proptosis, class 4 when there is involvement of the extraocular muscles, class 5 when there is corneal involvement and class 6 in those with a loss of visual acuity (involvement of the optic nerve) and CAS (clinical activity score), including signs of acute inflammation such as hyperemia, pain, edema, and secondary functional impairment to the presence of inflammation(1-3). The disease develops slowly and progressively until stabilization, with rare cases of spontaneous resolution being reported. It usually manifests clinically in the acute phase with ocular hyperemia, chemosis, eyelid edema, proptosis of varying degrees, diplopia, impairment of ocular extrinsic muscles, with the most affected muscles being the lower, the medial, the upper and finally the side rectus, respectively. The most frequent signs are: retraction of the upper eyelid when looking down (lidlag), retraction of the lower eyelid (which worsens in the attempt to look up), reduced frequency of blinking, decreased convergence, inability to keep fixation on the side look and look scared in the attempt to fixate (Kocher’s sign). In the chronic phase of the inflammatory process, some patients develop restricted, fibrotic muscles which can increase the deviation observed in the acute phase(2,3). The treatment is based on the phase in which the disease is (acute or chronic). In the acute phase, the anti-inflammatory treatment of choice is the corticosteroid therapy orally or intravenously. Corticosteroid therapy is associated with the use of radiation, using the linear accelerator in ten continuous sessions in the most severe cases or ten weekly sessions with total doses of 2000cGy. Another drug treatment option is the use of colchicine, with a dosage of 0.5 to 1.5 mg/day, alone or combined with radiotherapy and/or corticosteroids, with good therapeutic response. Except for the emergency cases in which there is the risk of vision loss by exposure of the cornea or compressive optic neuropathy, surgical treatment should be indicated in the inactive phase of Graves’ orbitopathy. This treatment consists of orbital decompression, treatment of strabismus, and correction of eyelid retraction and aesthetic blepharoplasty, in that order(2,3). The following case report will discuss an atypical form of clinical manifestation of Graves’ ophthalmopathy. CASE REPORT EMS, 49, female, brown, single, general services assistant, from São Bernardo do Campo – SP, referred to the Orbit Sector in the Discipline of Ophthalmology at the Medicine College of ABC complaining of pain in the left eye for 5 months associated to red eye, double vision, blurred vision, eyelid swelling and intense pain on eye movement. She denied personal and family history of eye disease. As systemic personal history she had a history of cervical cancer treated 8 years ago. The visual acuity with the best correction was 20/25 RE and 20/40 LE. Upon inspection changes were found only in the left eye: bipalpebral edema 2+/4+, exotropia and conjunctival hyperemia 2+/4+. The ocular extrinsic motility presented limitation to lateroversions, being mild to adduction and severe to abduction. Direct and consensual pupillary light reflexes were preserved. The intraocular pressure was measured with the flattening technique and presented 12 mmHg in the RE and 36 mmHg in the LE (01pm). There were no changes in the anterior segment or in fundoscopy. Initially the following serum dosages were asked: TSH, free T4, anti-thyroglobulin antibody (anti-TG Ab), anti-thyroid peroxidase antibody (Anti-TPO Ab) and TRAb, Antinuclear (ANA) Ab, Anti-native DNA Ab, Anti-Sm Ab, Antihistone Ab, VDRL, CH50, ACE, Lysozyme, Calcium, RF, ANA, HSS, c-ANCA and p-ANCA. In addition to said dosages, the following tests were requested: PPD, chest X-ray, abdominal ultrasonography, orbit CT, urinary calcium dosage and complete gynecological examination. Colchicine was introduced orally (0.5 mg every 12 hours), timolol maleate and brimonidine tartrate both 1 droplet every 12 hours in the left eye. After 4 weeks, the patient returned with partial reduction of pain, eyelid edema and conjunctival hyperemia, but still complaint of diplopia. The IOP measured was: RE - 13 mmHg, and LE - 16 mm Hg (01pm). The extrinsic motility showed limitations to lateroversions and supraversion of the LE. Among the exams requested, only the following were outside the normal range: 1) The orbit CT (Figure 1) showed a thickening of the medial rectus muscle of the left eye, 2) PPD (19mm = strong reactor), 3) HSS of the first hour (40mm) and 4) the chest X-ray revealed the presence of multiple diffuse consolidations in the pulmonary parenchyma in the hilar region, suggestive of pulmonary cicatrization change (Figure 2). Thus, a biopsy of the medial rectus muscle of the LE under general anesthesia was suggested, and the patient was referred for assessment of the Pulmonologist who requested: 1) computed tomography of the chest showing multiple hyperattenuating lesions in the lung parenchyma suggestive of calcification and ancient cicatrization process (Figure 1), direct BK search with negative result. Rev Bras Oftalmol. 2015; 74 (4): 244-7 246 Rodrigues FM, Fonseca Junior NL, Rehder JRCL , Fernandez CL, Sugano DM The results of all the exams described above and the clinical approval for the surgical procedure proposed were obtained after 7 weeks. On hospitalization the patient had were significantly better in signs and symptoms of the LE and acute impairment of the RE. At extrinsic motility, there were moderate limitations to lateroversions and supraversions of the RE (Figure 3). So the choice was a new imaging study (orbit CT), and after the analysis of the images (Figure 1) the biopsy of medial and lower rectus of the RE was indicated under general anesthesia, and also a new serum dosage of TSH, free T4 , Anti-TG Ab, Anti-TPO Ab and TRAb. The anatomic and pathological study revealed the presence of striated skeletal muscle tissue with intense lymphoplasmocytic inflammatory infiltrate with a predominance of T lymphocytes and the presence of macrophages found consistent with the inflammatory phase of Graves’ ophthalmopathy. The serum dosage of TRAb was 35U/L, interpreted as a positive result. The other results are within the normal limits. Figure 3: Clinical picture. Clinical presentation in the immediate preoperative period. Presence of conjunctival hyperemia, bipalpebral edema and limitation of ocular extrinsic movement in the right eye, and significant reduction of signs and symptoms in the left eye. DISCUSSION Figure 1: Computed tomography of orbit - A) Coronal section (soft tissue window). B) Axial section (soft tissue window). Thickening of the medial rectus muscle of the left eye with tendon involvement at the time of initial care of patient. C) Coronal section (soft tissue window). D) Axial section (soft tissue window). Diffuse thickening of the extraocular muscles of the right eye before surgery immediately before the biopsy. Figure 2: Image Exam. A) Chest X-ray - presence of multiple diffuse consolidations in the pulmonary parenchyma in the hilar region suggestive of pulmonary cicatrization change. B) Computed tomography of the chest - presence of multiple hyperattenuating lesions in the lung parenchyma suggestive of calcifications and ancient cicatrization process. Rev Bras Oftalmol. 2015; 74 (4): 244-7 Thyroid ophthalmopathy is classified into acute or inflammatory disease, progressive and histologically associated to lymphocytic infiltration and edematous changes, and in chronic or inactive disease associated with fibrotic changes and fat infiltration in the retro-orbital tissues, especially the extraocular muscles(5,6). The acute phase of the disease presents as main symptoms: pain, conjunctival hyperemia, edema and eyelid hyperemia, proptosis, caruncle edema, chemosis, diplopia and blurred vision(3). The involvement is bilateral in 80% of cases; and usually manifests in patients with hyperthyroidism, involving two or more extraocular muscles without tendon involvement(7). In this case, the initial manifestation was unilateral, involving only one extraocular muscle (MRI LE) and its respective tendon in a patient in clinical and laboratory euthyroid state. The literature reveals that only 10% of patients with thyroid ophthalmopathy do not develop hyperthyroidism as the initial manifestation of the disease (7). From these, 3% presented hypothyroidism, and 7% euthyroid(7). Among the euthyroid patients (7%), only 2.5% did not have positive results for AntiTG Ab, Ant-TPO Ab and/or TRAb, revealing the atypical form of the initial clinical presentation of the disease in this case. The biopsy should be indicated in cases where the diagnosis is doubtful based only on the clinical profile and additional exams or when there is recurrence or resistance to the treatment being very important to rule out differential diagnoses. Colchicine, a drug used to treat the patient in question, inhibits mobility, chemotaxis, adhesion and phagocytosis of granulocytes; reduces the levels of adhesion molecules; inhibits the action and proliferation of fibroblasts and lymphocytes, and inhibits the synthesis of collagen. This drug was indicated due to the patient being strong reactive to PPD, in this case being contraindicated the use of systemic corticosteroids. One study compared the use of colchicine to prednisone in the treatment of 22 patients during the inflammatory phase of Graves’ ophthalmopathy. All the patients were similar regarding age, sex and smoking habits, and suffered euthyroidism for at least 3 months. They were randomized into 2 groups. Group 1 247 Atypical presentation of Graves’ ophthalmopathy (G1) received colchicine (1.5 mg/day), and group 2 (G2) was treated with prednisone (0.75 mg/kg/day). Although it was verified a reduction in the clinical activity of the disease in the 2 groups, the patients treated with colchicine did not suffer the side effects of prednisone such as weight gain, stomach problems, weakness, depression and changes in blood pressure, as observed in the present case(8). The orbital radiotherapy is an important adjuvant treatment of severe Graves’ orbitopathy in activity due to its anti-inflammatory effects and local immunosuppressants. About 60% of patients treated showed a favorable response(9). The successful approach will depend on the correct selection of patients, showing better results the earlier it is established. REFERENCES 1. 2. 3. 4. Kuriyan AE, Phipps RP, Feldon SE.The eye and thyroid disease. Curr Opin Ophthalmol.2008;19(6):499-506. Höfling Lima AL, Morales PH, Manso PG, Farah ME. Alterações oculares de doenças sistêmicas: retinopatia diabética e oftalmopatia de Graves. RBM Rev Bras Med.2006;63(5). Saraci G, Treta A.Ocular changes and approaches of ophthalmopathy in basedow - graves- parry- flajani disease. Maedica (Buchar). 2011;6(2):146-52. Weetman AP. Thyroid-associated eye disease: Pathophysiology. Lancet. 1991;338(8758):25-8. Review. 5. 6. 7. 8. 9. Fung S, Malhotra R, Selva D. Thyroid orbitopathy. Aust Fam Physician. 2003;32(8):615-20. Review. Yokoyama N, Nagataki S, Uetani M, Ashizawa K, Eguchi K. Role of magnetic resonance imaging in the assessment of disease activity in thyroid-associated ophthalmopathy.Thyroid. 2002;12(3):223-7. Stamato FJ, Manso PG, Maciel JR, Wolosker AM, Maciel RM, Furlanetto RP. Colchicine as a new option for the clinical treatment of Graves’ ophthalmopathy. Proceedings of the VIth International Symposium on Graves’ Ophthalmopathy, Amsterdam, November 27 to 28, 1998, p. 22. Stamato FJ, Maciel RM,Manso PG, Wolosker AM, Paiva ER, Lopes AC,et al. Colchicina no tratamento da fase inflamatória da oftalmopatia de Graves: um estudo prospectivo e randomizado com prednisona. Arq Bras Oftalmol.2006;69(6):811-6. Pitz S, Kahaly G, Rösler HP, Krummenauer F, Wagner B, Stübler M, et al. [Retrobulbar irradiation for Graves’ ophthalmopathy — long-term results]. Klin Monbl Augenheilkd. 2002;219(12):87682.German. Corresponding author: Flavia Marques Rodrigues Rua de Ceuta 222 Jardim Lusitânia São Paulo (SP) ZIP Code 04031-01 Email: [email protected] Rev Bras Oftalmol. 2015; 74 (4): 244-7 248 CASE REPORT Retro-orbital tumor suggestive of optic nerve sheath meningocele Tumoração retroorbitária sugestiva de meningocele da bainha do nervo óptico Michelle Rodrigues Gonçalve Dias Chavess 1, Isabella Bezerra Wanderley de Queiroga 2, Mario Augusto Pereira Dias Chaves 1,3,4, Fernando Melo Gadelha 1,2 , Debora Apolônio Vieira 2 ABSTRACT Meningocele of the optic nerve sheath is an extremely rare condition with a few cases reported in literature. Image studies reveal tubularcystic enlargement of the optic nerve although with the same thickness. Symptoms are often related to the involvement of the optic nerve, leading from slow to accelerated decreasing of the visual acuity. The early surgical treatment is the decompression of the optic nerve sheath, which it could provide improvement of visual function. We are presenting a case report of a patient who showed clinical and radiological signs of this rare pathological condition. Male patient attended at service complaining of proptosis of right eye (OD) since birth, in progress during the last months associated to stabbing pain. Best corrected visual acuity (BCVA) of OD was movements at 50 cm far; OS showed no abnormalities. Nuclear Magnetic Resonance of the OD showed expansive formation with cystic aspect, defined boundaries, located in an intraconal situation on the right orbit cavity and in a closing anatomical relationship to the optic nerve, inducing compression, deformity and anterior displacement of this eye besides presenting signal similar to spine liquor in all sequences obtained. The first hypothesis was meningocele of right optic nerve sheath. Then, patient was referred for surgical decompression. Keywords: Meningocele/diagnosis; Exophthalmia; Optic nerve/pathology; Neoplasms; Case reports RESUMO Meningocele da bainha do nervo óptico é uma condição extremamente rara, com poucos casos relatados na literatura. Exames de imagem revelam alargamento tubular-cístico do nervo óptico, com espessamento do mesmo. Os sintomas são muitas vezes relacionados com o comprometimento do nervo, ocasionando diminuição de lenta a acelerada da acuidade visual. O tratamento cirúrgico precoce por meio da descompressão da bainha do nervo óptico pode proporcionar melhora da função visual. Apresenta-se um caso de paciente com as características clínicas e radiológicas desta condição patológica rara. Paciente masculino, atendido no serviço com queixa de proptose do olho direito (OD) desde nascimento, com progressão nos últimos meses associada à dor. Melhor acuidade visual corrigida de conta dedos a 50 cm do OD. Olho esquerdo sem anormalidades. Ressonância Magnética de OD demonstrou formação expansiva cística de limites definidos em situação intraconal em órbita direita, em íntima relação com nervo óptico, determinando compressão, deformidade e deslocamento anterior do bulbo ocular, além de apresentar sinal semelhante ao líquor em todas as sequências obtidas. Suscitou-se hipótese diagnóstica de meningocele da bainha do nervo óptico direito e o paciente foi encaminhado para cirurgia descompressiva. Descritores: Meningocele/diagnóstico; Nervo óptico/patologia; Neoplasias; Exoftalmia; Relatos de casos 1. Hospital Visão, João Pessoa (PB), Brasil. 2. Centro de Referência Oftalmológica do Hospital Universitário Lauro Wanderley, Universidade Federal da Paraíba, João Pessoa (PB), Brasil. 3. Centro de Estudos Oftalmológicos Renato Ambrósio (CEORA) do Hospital Oftalmológico de Brasília (HOB), Brasília (DF), Brasil. 4. Fundação Altino Ventura (FAV), Recife (PE), Brasil The authors declare no conflicts of interest Received for publication 09/07/2012 - Accepted for publication 31/03/2013 Rev Bras Oftalmol. 2015; 74 (4): 248-50 249 Retro-orbital tumor suggestive of optic nerve sheath meningocele INTRODUCTION ptic nerve sheath meningocele (ONAM) is an extremely rare condition, with few cases reported in the literature, being it defined as a sheath swelling of the optic nerve by spinal fluid. There is an expansion of the cerebrospinal fluid space around the optic nerve without associated inflammation, cerebral or orbital neoplasia. Imaging exams show a tubularcystic enlargement of the optic nerve / sheath-optical complex with thickening of the optic nerve. The differential diagnosis includes tumors of the optic nerve as meningioma, vascular hamartoma, glioma, neurofibromatosis, Von Hippel-Lindau desease, hemangioendothelioma, or skull-orbital fracture(1). The symptoms are often related to nerve impairment, classically causing headaches or progressive, slow or fast visual decline(2). This paper aims at reporting the case of a patient whose clinical data and imaging exams are highly suggestive of optic nerve sheath meningocele, and stressing the main features of this rare disease. O in the RE. The physical examination of the RE showed significant improvement in ocular proptosis, but with persistence of corrected visual acuity of hand movements, esotrope, direct photomotor reflex and consensual absent; onset of conjunctival and corneal lesion, superior temporal quadrant of the cornea, extending until close to the visual axis (Figure 5). The pathology report showed that the withdrawal piece was a “typical fibroadipous hyaline tissue without epithelial lining, compatible with benign cystic lesion wall.” Figure 1: Patient in initial eye exam during inspection, demonstrating important ocular proptosis in the RE CASE REPORT Male patient, 28, attended at the Lauro Wanderley University Hospital complaining of congenital exophthalmos in the right eye (RE) in progress during the last months associated with pain in sporadic twinge. Background: 28 weeks of pre-term, delayed neuro-psycho-motor development. Inspection: Proptosis of the RE (Figure 1). Visual acuity (VA): RE: Counting fingers at 50 cm and 20/20 (1.0) LE (-4.50 D -1.00D 170o). Bio: RE: Cortical cataract 2+/4; LE with no abnormalities. Fundoscopy: RE: Posterior pole choroidal with significant optic atrophy and wide area of atrophy of the Retinal Pigment Epithelium associated to the hyperpigmentation area adjacent to the optical disc. LE: Excavation/cup relationship increased, characteristic macular color, vascular arcades of usual conformity and applied retina. IOP: RE: impracticable, LE: 12mmHg. RE ultrasound showed cystic, retro orbital lesion in the optic nerve topography, with other exams being asked. Computed tomography (CT) showed the ventricular system with normal dimensions, morphology and topography, basal cisterns of normal aspect, brain structures with normal radiographic density, observing fusiform thickening of the right optic nerve associated to ipsilateral exophthalmos, with no changes in the optical channel or the intracranial route of the optic nerve. Nuclear magnetic resonance (NMR) in the RE showed expansive formation of cystic aspect with defined limits and thin walls located in intrachoanal situation in the right orbit, with close anatomical relation with the topography of the optic nerve, determining anterior compression, deformity and displacement of the ipsilateral eye bulb, besides showing a signal similar to CSF in all sequences obtained, with size of 3.4 x 3.2 x 3.1 cm (Figures 2, 3 and 4). There was no significant anomalous impregnation of the paramagnetic contrast (GADOLINIUM) in the walls or within the lesion. The extraocular muscles were displaced by said formation, determining compression, deformity and proptosis of the RE eye bulb. Being it very characteristic, the first diagnostic hypothesis raised was rioght optic nerve sheath meningocele. The patient was then referred to decompression surgery, returning eight months after surgery with no complaints of pain or headache, however reporting persistence of low visual acuity abducens nerve aortic siphon Figure 2: Pre-contrast axial section weighted in T1 showing isosignal of mass lesion, leading to proptosis of the RE Figure 3: . Axial MRI, heavy sequence in T1 with fat saturation. Lesion with low signal after the use of paramagnetic contrast, highlighting significant dilation of the optic nerve sheath, with consequent proptosis of the RE. DISCUSSION According to Garrity et al. (2) the pathology in question arises from the perineural subarachnoid space of the optic nerve, and should be differentiated from congenital cerebrospinal fluid accumulation (CSF) in the perioptic subarachnoid space. In such case, the lesion arises from an abnormal CSF flow through a diverticulum in the arachnoid membrane. They also report the cases of 13 patients with MBNO, with blurred vision and headache being the main symptoms. Rev Bras Oftalmol. 2015; 74 (4): 248-50 250 Chaves MRGD, Queiroga IBW, Chaves MAPD, Gadelha FM, Vieira DA Figure 4: Axial section, heavy sequence in T2 with fat saturation. Lesion with high signal, highlighting significant dilation of the optic nerve sheath. Mesa-Gutiérrez et al. reported the case of a patient, 53, with MBNO associated to intracranial hypertension, but with visual acuity corrected to 20/20 (1.0), with +2.00D in the initial exam. The diagnosis was confirmed only with imaging studies. The MRI identified a dilation of the optic nerve sheath caused by a fluid with characteristics consistent with cerebrospinal fluid. There were no changes in the optic nerves, as well as there was also no evidence of brain or orbit tumors. The lumbar puncture was performed with opening pressure of 22 mmHg, and the chemical analysis of cerebrospinal fluid was normal. After neurosurgical evaluation, the patient was only clinically treated with acetazolamide for three months, remaining stable over the 24 months of follow-up. In all follow-up examinations, the nerve function was normal, with a visual acuity of 20/20 without optical correction after treatment. The authors conclude that surgery should be reserved to severe cases with pain, considerable proptosis, or rapid and progressive decrease in visual acuity. Spooler et al. (5) describe a case of a child with multiple congenital anomalies, including unilateral MBNO with rapid expansion and displacement of the lateral orbit, resulting in severe cosmetic deformity and complete blindness in his left eye, which was treated with surgical decompression. The authors also rectify that surgical decompression is the standard treatment, with improvement or progression interruption in most cases. CONCLUSION Figure 5: Patient in physical exam after surgery, in inspection to a greater lower increase, showing significant reduction in the proptosis of the RE Lunardi et al. (1) reviewed the existing literature, finding only about 31 cases of MBNO throughout literature, and they describe the disease as primary cysts of the optic nerve sheath without apical mass or malformation of the skull-orbital junction. The symptoms are often related to the involvement of the optic nerve, with a slow or rapid decrease in visual acuity. Additional tests such as CT and MRI revealed a tubular-cystic enlargement of the optic nerve sheath, with thickening of the same. The authors suggest that early surgical intervention by means of the optic nerve sheath decompression enables an improvement of visual function with minimal morbidity in patients with a rapid decrease of visual acuity within 3-6 months. Shanmuganathan et al. reported the case of an adult, 59, with symmetrical bilateral proptosis and complaint of progressive loss of visual acuity associated to retro-orbital pain and subsequently to cystoid macular edema (CME) in the RE. MRI showed bilateral optic nerve sheath dilation and enlargement, but with normal-sized optic nerve. They describe that EMC can be caused by a tractional meningocele force on the eyeball, and that the role of increased intracranial pressure (ICP) is not clear yet in the etiology of the disease, as only some of the reported cases had increased ICP, measured by lumbar puncture. They also concluded that early surgical decompression of the optic nerve sheath should always be considered in cases of progressive visual loss. Rev Bras Oftalmol. 2015; 74 (4): 248-50 The present case reports the presence of a retro-orbital lesion in intrachoanal situation and intimately anatomically related to the nerve, strongly suggestive of optic nerve sheath meningocele. The diagnosis can be given by the NMR, and even if pending histological examination, the investigative conduct is consistent, besides the indication of decompressive surgery in selected cases, exceptionally with rapid development and imminent functional and anatomical impairment of the surrounding structures (4). In conclusion, the importance of remembering that entity is demonstrated by this case report, despite the rarity of the disease. REFERENCES 1. 2. 3. 4. 5. Lunardi P, Farah JO, Ruggeri A, Nardacci B, Ferrante L, Puzzilli F. Surgically verified case of optic sheath nerve meningocele: case report with review of the literature. Neurosurg Rev. 1997;20(3):201-5. Garrity JA, Trautman JC, Bartley GB, Forbes G, Bullock JD, Jones TW Jr, et al. Optic nerve sheath meningoceles. Clinical and radiographic features in 13 cases with a review of the literature. Ophthalmology. 1990;97(11):1519-31. Comment in Ophthalmology. 1991;98(5):562. Shanmuganathan V, Leatherbarrow B, Ansons A, Laitt R. Bilateral idopathic optic nerve sheath meningocele associated with unilateral transient cystoid macular oedema. Eye (Lond). 2002;16(6):800-2. Mesa-Gutiérrez JC, Quiñones SM, Ginebreda JA. Optic nerve sheath meningocele. Clin Ophthalmol. 2008;2(3):661-8. Spooler JC, Cho D, Ray A, Zouros A. Patient with congenital optic nerve meningocele presenting with left orbital cyst. Childs Nerv Syst. 2009;25(2):267-9. CASE REPORT 251 Macular granuloma due to tuberculosis without pulmonary symptoms Granuloma macular por tuberculose sem manifestação pulmonar Albert Costa Rebello1, João Helio Leonardo de Sousa2, José Gilberto de Sá3, Karime Kalif de Sousa Rebello4 ABSTRACT Tuberculosis is an infectious disease caused by Mycobacterium tuberculosis. The main site of involvement is the lung, but the bacillus may spread by hematogenous/lymph systems to other organs, including the eye. The incidence of ocular TB is 1-2% of extra-pulmonary cases. The authors present a case of a 28 years old female patient seeking medical care due to reduction of visual acuity in the left eye for 8 days. She had the best corrected visual acuity in the affected eye of 20/200, and the opposite eye was 20/20. At fundoscopy was shown a granuloma in the macular area of the left eye, with retinal edema and hemorrhage. After diagnostic investigation the patient was treated with antibiotic therapy for tuberculosis during 6 months, obtaining lesion regression and visual acuity improvement to 20/50. Keywords: Tuberculosis, ocular/diagnosis; Tuberculosis, ocular/drug therapy; Macula lútea; Uveitis/diagnosis; Uveitis/therapy; Case reports RESUMO Tuberculose é uma doença infecciosa causada pelo Mycobacterium tuberculosis, também conhecido como bacilo de Koch. O principal sítio de acometimento é o pulmonar, porém o bacilo pode disseminar-se por via linfo-hematogênica para outros órgãos, dentre eles: o olho. A incidência de tuberculose ocular é de 1 a 2% dos casos extra pulmonares. Os autores apresentam um caso clínico de um paciente do sexo feminino de 28 anos que procura atendimento médico devido a redução da acuidade visual em olho esquerdo há 7 dias. Apresentava a melhor acuidade visual corrigida no olho acometido de 20/200, e no olho contralateral de 20/20. Na fundoscopia era evidenciado um granuloma em área macular do olho esquerdo, com edema e hemorragia intrarretiniana adjacente. Após investigação diagnóstica, a paciente foi tratada com esquema antibiótico para tuberculose durante 6 meses, obtendo regressão do granuloma e melhora da acuidade visual deste olho para 20/50. Descritores: Tuberculose ocular/diagnóstico; Tuberculose ocular/tratamento; Macula lutea; Uveíte/diagnóstico; Uveíte/tratamento; Relatos de casos Ophthalmology Center Rio – Rio de Janeiro, RJ, Brazil. Municipal Hospital Jesus – Rio de Janeiro, RJ, Brazil. 3 Municipal Hospital Jesus – Rio de Janeiro, RJ, Brazil. 4 Ophthalmology Center Rio – Rio de Janeiro, RJ, Brazil. Study conducted at the Municipal Hospital Jesus and the Ophthalmology Center Rio – Rio de Janeiro (RJ), Brazil. 11 2 The authors declare no conflicts of interest Received for publication 10/07/2012 - Accepted for publication 26/03/2013 Rev Bras Oftalmol. 2015; 74 (4): 251-3 252 Rebello AC, Sousa JHL, Sá JG, Rebello KKS INTRODUCTION B razil is one of 22 countries prioritized by the World Health Organization (WHO) covering 80% of the global cases of tuberculosis(1). Currently the country is in the 19th place, and was formerly the 14th in 2004. In 2009, there were 71,700 new cases of the disease, with an incidence rate of 37 per each group of 100 thousand inhabitants. In Rio de Janeiro the incidence rate is 73.99 per 100,000 inhabitants, giving the state a sad first place when compared to other States(2). According to data collected by the Ministry of Health and the Department of Health Surveillance, in the case of extra pulmonary tuberculosis the incidence rate drops to 10.06 per 100,000 inhabitants in Rio de Janeiro. This number includes the cases of pleural, lymph node, osteoarticular, genitourinary, intestinal, peritoneal, pericardial, central nervous system, eye and skin tuberculosis(3,4). The authors present a case of ocular manifestation of tuberculosis that was satisfactorily responsive to the treatment against tuberculosis for 6 months. CASE REPORT Female patient, 28, white, sought medical care due to decreased visual acuity in the left eye for 7 days, with sudden and spontaneous onset. Past medical history without relevant data, but reporting contact with a tuberculosis patient two years ago in her own home. The eye exam showed better corrected visual acuity for farsight on the right eye: 20/20, and on the left eye: 20/200; Ocular motility without change; Normal biomicroscopy; Tonometry RE: 12 mmHg and LE: 13 mmHg; Fundoscopy: stained buds, physiological excavations, preserved arteriovenous ratio, presence of a yellowish granulomatous lesion with adjacent retinal edema and hemorrhage in the macula of the left eye (Figure 1). Figure 1: Granulomatous lesion with hemorrhage and retinal edema. Initial diagnostic research showed no changes in blood count, microbiology, biochemistry and immunochemistry. It is important to emphasize the negative serology for toxoplasmosis, both IgM as IgG. Normal chest radiograph. Tuberculin skin test equal to 20mm. Antituberculosis oral therapy was initiated with follow-up in specialized unit of the public health service. To improve the retinal edema, she received topical treatment with dexamethasone eyedrops for 30 days, with gradual dose reduction and monitoring of the intraocular pressure. Rev Bras Oftalmol. 2015; 74 (4): 251-3 After follow-up for 6 months, with the respective end of the oral treatment, the patient improved the visual acuity of the left eye to 20/50. In the fundoscopy, the lesion improved and the retinal edema disappeared, the hemorrhage was absorbed and the retinal pigment epithelium in the macular area was atrophied (Figure 2). Figure 2: Regression of the lesion after antituberculous therapy for 6 months . DISCUSSION Given the high prevalence of the disease in our country, it is always advisable to investigate tuberculosis in cases of chorioretinitis. It is a especially important fact, considering that some treatments directed to other etiologies may worsen the tuberculosis condition (as an example we can mention the use of systemic corticosteroids, used in some cases of toxoplasmosis chorioretinitis). The standard test for the diagnosis finding Mycobacterium tuberculosis in ocular specimens, but due to the paucibacillary lesions and the noble condition of the visual apparatus significantly limit the histological study, the diagnosis of ocular tuberculosis is supported by epidemiological data, clinical examination, positive tuberculin skin test and laboratory exclusion of other conditions(5), among them toxoplasmosis. The tuberculin skin test is still the exam which guides us about possible infections with Mycobacterium tuberculosis, although a positive result does not mean active disease. Therefore, other criteria are needed to confirm the diagnosis of ocular tuberculosis. Among them are: observing if there is improvement with the basic scheme in the first two months, if there is no recurrence of the disease during treatment, or if there is no recurrence in the first two years after interrupting the medication. Otherwise, probably the etiology of tuberculosis is not considered, forcing the search for other causes(6). We must also take into account the differential diagnosis with syphilis, sarcoidosis, brucellosis, histoplasmosis and toxocariasis. Any tissue in the eye may be affected, though the most common site is the uvea. As illustrated in the present case, the disease may be present even without systemic disease. The changes can be caused by bacterial invasion or be immunological, by hypersensitivity reaction type IV. Some of the possible ocular manifestations are anterior, posterior, intermediate uveitis, panuveitis, serpiginous-like choroiditis, subretinal abscesses, 253 Macular granuloma due to tuberculosis without pulmonary symptoms serous retinal detachment, retinitis, choroiditis, retinochoroiditis, retinal vasculitis and endophthalmitis(6). In this case, the improved healing of the macular injury after the use of anti tuberculous medication is an important evidence to establish the diagnosis, along with the positive history of contact. But also, there was healing and regression of the lesion after the beggining of the treatment without reincidence, and apparently it continues healed even after the end of 6-month therapy. As the prognosis is influenced by the location of the lesion and the adherence to treatment, in this case the significant improvement in vision draws attention, despite the proximity between the granuloma and the macula. 3. 4. 5. 6. Brasil. Ministério da Saúde. Secretaria de Políticas de Saúde. Departamento de Atenção Básica. Manual técnico para controle da tuberculose. (Cadernos de Atenção Básica, 6). Brasília: Ministério da Saúde; 2002. Brasil. Ministério da Saúde. Secretaria de Vigilância em Saúde. Departamento de Vigilância Epidemiológica. Doenças infecciosas e parasitárias: guia de bolso. 8a ed. rev. Brasília: Ministério da Saúde; 2010. Lopes AJ, Capone D, Mogami R, Tessarollo B, Cunha DL, Capone RB, et al. Tuberculose extrapulmonar: aspectos clínicos e de imagem. Pulmão RJ. 2006;15(4):253-61. Campos WR, Campos GS, Miranda SS. Tuberculose intraocular. Rev Bras Oftalmol. 2011;70(6):437-51. REFERENCES 1. 2. Arakaki D, Oliveira G, Barreira D, Moherdaui F, Codenotti S, Bartholomay P. Novo sistema de tratamento da tuberculose para adultos e adolescentes no Brasil. Informe Técnico de Tuberculose. Edição nº 5, julho de 2010. Disponível em: http://portal.saude.gov.br/ portal/arquivos/pdf/informe_tb_julho10_certo_22_07_2010.pdf Brasil. Ministério da Saúde. Departamento de Informatica do SUS. DATASUS. Disponível em http://tabnet.datasus.gov.br/cgi/ e http://www2.datasus.gov.br/DATASUS Corresponding author: Albert Costa Rebello Av. Passos, 101 / 1609 - Centro ZIP Code: 20051-040 - Rio de Janeiro (RJ), Brazil Fax No.: (21) 2263-4838 E-mail: [email protected] Rev Bras Oftalmol. 2015; 74 (4): 251-3 254 CASE REPORT Irreversible visual loss after use of Paclitaxel Perda visual irreversível após uso de Paclitaxel Maria Helena Lopes Amigo1, Paulo Falabella2, Ângela Bettarello2, Wagner Ghirelli2 ABSTRACT We describe a case of bilateral irreversible visual loss of a 64 year-old patient after prolonged use of paclitaxel. Patient presented best corrected visual acuity of 20/400 in both eyes at first visit and optical coherence tomography showed increased macular in both eyes. After six months of the interruption of suspension paclitaxel therapy, the patient showed slight improvement of visual acuity reaching 20/200 in both eyes, while OCT demonstrated resolution of macular edema. Keywords: Chemotherapy/adverse effects; Paclitaxel/toxicity; Macular edema/chemically induced; Visual acuity/drug effects; Ovarian neoplasms/drug therapy; Case reports RESUMO Descrevemos um caso de perda visual irreversível bilateral em uma paciente de 64 anos após uso prolongado de paclitaxel. Ao exame oftalmológico apresentou acuidade visual (AV) de 20/400 em ambos os olhos (AO) na primeira consulta e tomografia de coerência óptica (TCO) evidenciando espessamento macular AO. Após seis meses da suspensão do paclitaxel, a paciente apresentava melhora discreta da AV atingindo 20/200 com correção em AO, além de TCO demostrando resolução do espessamento retiniano. Descritores: Quimioterapia/efeitos adversos; Paclitaxel/toxicidade; Edema macular/induzido quimicamente; Acuidade visual/ efeitos de drogas; Neoplasias ovarianas/quimioterapia; Relatos de casos 1 2 Ophthalmology Center Tadeu Cvintal – São Paulo (SP), Brazil. Retina and Vitreous Department of the Ophthalmology Center Tadeu Cvintal – São Paulo (SP), Brazil The authors declare no conflicts of interest Received for publication 27/07/2012 - Accepted for publication 05/12/2012 Rev Bras Oftalmol. 2015; 74 (4): 254-6 Irreversible visual loss after use of Paclitaxel 255 INTRODUCTION P aclitaxel is a chemotherapeutic of the taxane family primarily used in the treatment of breast and ovarian cancer and in a variety of other solid tumors. Among the toxic effects are myelosuppression and peripheral neuropathy (1) . There are rare cases of retinal toxicity reported in the literature, especially those culminating in visual loss due to maculopathy(2,3). We describe below a report of irreversible low visual acuity associated to the use of paclitaxel. Figure 1: Retinography of both eyes (BE) showing the normal aspects of retinal macula and periphery. CASE REPORT Female patient, white, 64, came to her first appointment in February 2007 complaining of progressive low visual acuity (VA) during the last year in both eyes (BE), and was initially referred with a suspicion of cataract. She brought with her the result of an electroretinography with no changes carried out one month before the appointment, and result of nuclear magnetic resonance imaging showed ethmoid sinusitis. She had a history of surgery for excision of ovarian cancer and chemotherapy with paclitaxel due to intestinal metastasis eighteen years ago (not knowing the dose and the medication use interval). She also reported history of facial paralysis eight months ago and left lower limb thrombosis 7 months ago. The eye exam showed normal external eye exam and best corrected visual acuity of 20/400 (+0.50 spherical dioptres in BE). Biomicroscopy: transparent cornea, deep anterior chamber and without inflammatory cells, iris unchanged and crystalline with mild nuclear opacity. Applanation tonometry of 20 mmHg in BE. Fundoscopy showed signs of mild bilateral arteriosclerosis. Macula and medium periphery with physiological aspect. (Figure 1) Fluorescein angiography exam revealed the presence of hyperfluorescence of the optic nerve and macula without extravasation signs in BE (Figure 2). Optical coherence tomography (OCT) showed an increase in the retinal thickness with cystic spaces and aspect of sectoral retinoschisis. The right eye (RE) showed: total macular volume of 9785 mm3, and foveal thicknesses of 243 (+/-91) microns; in the left eye: total macular volume of 9415 mm3, and foveal thicknesses of 212 (+/-41) microns. (Figure 3) In April 2007 we chose to use acetazolamide oral and triamcinolone acetate 4 mg intravitreal in the RE seeking anatomical and functional improvement, but there were no satisfactory results both in the visual acuity and retinal edema. A literature review resulted in the location of a case report which described a bilateral cystoid macular edema secondary to the use of paclitaxel. In this case, suspending the medication led to total remission of the edema and improvement of the visual acuity after 6 weeks(3). Therefore, we decided to interrupt chemotherapy and, after six months, the patient showed a mild improvement of the VA and reached 20/200 with correction in BE, whereas the OCT showed complete resolution of the cystoid macular edema in BE. (Figure 4) Figure 2: Retinal fluorescein angiography: hyperfluorescence in the optic nerve, and macula with no signs of extravasation in BE. Figure3: Optical coherence tomography: Increase in the retinal thickness with cystic spaces and aspect of retinosquise in some places. Presented respectively: Total macular volume in the RE of 9785 mm3, foveal thicknesses of 243 (+/-91) microns in the RE (A), and in the LE 9415mm3 and 212 (+/-41) microns in the LE (B).. Figure 4: OCT six months after suspending the use of paclitaxel, showing retinal thickening improvement in the RE A) and LE B). Rev Bras Oftalmol. 2015; 74 (4): 254-6 256 Amigo MHL, Falabella P, Bettarello Â, Ghirelli W DISCUSSION Ocular toxicity by paclitaxel is little known by both ophthalmologists and oncologists. It is a chemotherapeutic agent that inhibits the formation of intracellular microtubules, and whose ophthalmological side effects often include low visual acuity, scintillating scotomas and changes in evoked visual potential. Some articles have suggested the association of the drug to the onset of cystoid macular edema, but we understand this is the first one in which there was severe and irreversible loss of visual acuity, even after discontinuation of medication(2,3). We envisaged the differential diagnosis of cancer associated retinopathy (CAR) because of low visual acuity, which is why the electroretinography was held and the result showed no changes. Electrophysiological assessment of vision in patients treated with paclitaxel showed little correlation with visual symptoms(4) as in this case, being therefore further data to the diagnosis. We highlight the important clinical characteristic related to paclitaxel toxicity and the presence of cystoid macular edema observed in the TCO associated to the absence of contrast extravasation on fluorescein angiography. This fact has been previously described for both paclitaxel and other chemotherapeutic of the taxane family, docetaxel. Toxicity to Müller cells is the theory for the pathophysiological mechanism, with subsequent accumulation of intracellular fluid and subclinical extracellular extravasation(3,5,6). The irreversibility of low visual acuity even after discontinuation of medication and subsequent settlement of the cystoid macular edema suggests a distinct toxicity mechanism of paclitaxel associated to permanent cell damage. Rev Bras Oftalmol. 2015; 74 (4): 254-6 In this case report there was the relation to the use of medication, not only with the onset of macular edema, but also with the patient’s irreversible visual loss, emphasizing therefore the maculotoxicity potential of paclitaxel. REFERENCES 1. 2. 3. 4. 5. 6. Marupudi NI, Han JE, Li KW, Renard VM, Tyler BM, BremH. Paclitaxel: a review of adverse toxicities and novel delivery strategies. Expert Opin Drug Saf. 2007; 6 (5): 609-21. Hofstra LS, de Vries EG, Willemse PH. Ophthalmic toxicity following paclitaxel infusion. Ann Oncol. 1997; 8 (10): 1053. Joshi MM, Garretson BR. Paclitaxel maculopathy. Arch Ophthalmol. 2007; 125 (5): 709-10. Scaioli V, Caraceni A, Martini C, Curzi G, Luca G. Electrophysilogical evaluation of visual pathways in plactaxeltreated patients. J Neurooncol. 2006; 77 (1):79-87. Teitelbaum BA, Tresley DJ. Cystic maculopathy with normal capillary permeability secundary to docetaxel. Optom Vis Sci. 2003; 80 (4):277-9. Telander DG, Sarraf D. Cystoid macular edema with docetaxel chemotherapy and the fluid retention syndrome. Semin Ophthalmol. 2007; 22 (3): 151-3. Corresponding author: Wagner Ghirelli Rua Maria Figueiredo 283 Phone No.: 11 33713324 Email: [email protected] REVIEW ARTICLE 257 Biomarkers and surrogate endpoints in the glaucomatous optic neuropathy: new developments and a review Biomarcadores e desfechos substitutos na neuropatia óptica glaucomatosa: novos desenvolvimentos e uma revisão Niro Kasahara1 ABSTRACT Glaucoma is a group of progressive optic neuropathies that have in common a slow progressive degeneration of retinal ganglion cells and their axons, resulting in a distinct appearance of the optic disc and a concomitant pattern of visual loss. Biomarkers are characteristics objectively measured and evaluated as indication of normal biologic processes, pathogenic processes, or pharmacologic responses to a therapeutic intervention. Several biological markers have been implicated with glaucoma, especially genetics, proteomics, autoimmune and other molecular biomarkers, although, most awaits clinical validation. There are clear potential benefits in using biomarkers. Information can be obtained earlier, faster, and less costly. This review summarizes the latest developments and approaches in glaucoma biomarkers and its possible uses in the diagnosis, staging, and as predictors of response to treatment. Keywwords: Glaucoma; Optic nerve diseases; Biological makers RESUMO O glaucoma compreende um grupo de neuropatias ópticas progressivas que tem em comum a degeneração lenta e progressiva das células ganglionares e seus axônios, resultando em aparência única do disco óptico e, simultaneamente, um padrão correspondente de perda visual. Biomarcadores são características medidas objetivamente e avaliadas como indicadores de processo biológico normal, processos patológicos ou respostas farmacológicas à uma intervenção terapêutica. Vários marcadores biológicos foram associados com glaucoma, especialmente os genéticos, proteômicos, autoimunes e outros biomarcadores moleculares, embora a maioria ainda necessite de validação clínica. Existem potenciais benefícios em usar biomarcadores. Informações podem ser obtidas mais precocemente, de forma mais rápida e menos onerosa. Esta revisão resume os últimos avanços e métodos em biomarcadores de glaucoma e seu possível uso no diagnóstico, estadiamento e como preditores da resposta ao tratamento. Descritores: Glaucoma; Doenças do nervo óptico; Marcadores biológicos 1 Departamento de Oftalmologia, Irmandade da Santa Casa de Misericórdia de São Paulo; Faculdade de Ciências Médicas da Santa Casa de São Paulo, São Paulo, SP, Brazil. The authoes declare no conflicts of interest Received for publication 21/08/2014 - Accepted for publication 17/12/2014 Rev Bras Oftalmol. 2015; 74 (4): 257-65 258 Kasahara N B iomarkers are characteristics objectively measured and evaluated as indication of normal biologic processes, pathogenic processes, or pharmacologic responses to a therapeutic intervention.(1) Although what the marker marks is clearly defined as being intrinsic, the marker itself can be either intrinsic or extrinsic. Intrinsic markers can be physical (clinical or radiographic) or laboratorial (physiological, pharmacological, genetic, biochemical, etc.). An example of an extrinsic marker is cigarette consumption in lung cancer.(2) A surrogate marker or surrogate endpoint has been defined as a biomarker intended to substitute for a clinical endpoint, the latter being a characteristic or variable that reflects how a patient feels, functions, or survives.(1) Both biomarkers and surrogate endpoints can be used in diagnosing, staging, and monitoring disease, and in determining its response to therapy. The difference between a biomarker and surrogate endpoint is that a biomarker is a “candidate” surrogate marker, whereas a surrogate marker is a test used, and taken, as a measure of the effects of a specific treatment.(3) Biomarkers are often cheaper and easier to measure than true endpoints and can be measured more quickly and earlier. There may also be ethical issues associated with measuring true endpoints. For example, in paracetamol overdose it is unethical to wait for evidence of liver damage before deciding whether or not to treat a patient; instead, a pharmacological biomarker, the plasma paracetamol concentration, is used to predict whether treatment is required.(2) Biomarkers can be used at any point in the chain of events that leads from the pathogenesis of a disease to its clinical manifestations, whether at the molecular, cellular, or organ levels. Likewise, a therapy might be developed to tackle any one of these links, in order to try to treat the disease. Any measurement short of the actual outcome could be regarded as a surrogate endpoint biomarker. However, although all surrogate endpoints are biomarkers, not all biomarkers are useful surrogate endpoints.(2) Surrogate endpoints are used in clinical trials and, as such, it is defined as a response variable for which a test of the null hypothesis of no relationship to the treatment groups under comparison is also a valid test of the corresponding null hypothesis based on the true endpoint.(4) It’s use, however, introduces heterogeneous variance and the problem of regression to the mean. In clinical practice, biomarkers are used frequently and without notice. In a patient with cancer, a clinician measures the time to relapse as a surrogate endpoint for survival time. Ophthalmologists measure intraocular pressure (IOP) instead of loss of vision in patients with glaucoma. Physicians use biomarkers to stage disease (e.g., the number of lymph nodes affected by cancer), in diagnosis (e.g., magnetic resonance imaging, electrocardiography, and autoimmune antibodies), and to monitor the progress of a disease or its treatment (e.g., serum glucose concentration and blood pressure).(2) The increased sensitivity and the developments of genomic, proteomic, and metabolomic research techniques have caused the potential to identify molecules that may serve as potentially useful markers, including (1) markers for early detection of a disease, (2) markers to predict disease severity, (3) markers to predict the rate of disease progression, and (4) markers to serve as predictors of response to treatment.(5) Rev Bras Oftalmol. 2015; 74 (4): 257-65 Glaucoma is a group of progressive optic neuropathies that have in common a slow progressive degeneration of retinal ganglion cells and their axons, resulting in a distinct appearance of the optic disc and a concomitant pattern of visual loss.(6) It is estimated that glaucoma affects more than 66 million individuals worldwide with at least 6.8 million bilaterally blind.(7) Although not completely understood, it is a multifactorial complex neurodegenerative disease triggered by different factors including mechanical stress due to intraocular pressure, decreased blood flow to retina, reperfusion injury, oxidative stress, glutamate excitotoxicity, and aberrant immune response. The discovery of clinically useful biomarkers in glaucoma is constantly expanding and includes from genes to proteomic markers, and analyses of serum antibodies to retina and optic nerve proteins. We summarize herein the current knowledge regarding the factors related to the diagnosis, progression, and response to treatment of glaucoma, which have not been definitely established but represent biomarker candidates to be validated. These markers include clinical, genetic, proteomic, autoimmune, and neurodegenerative candidates yet to be corroborated. Clinical biomarkers Automated perimetry, IOP, optic disk, and retinal nerve fiber layer are surrogate markers for glaucomatous optic neuropathy used in clinical practice and as outcome measures in research. From another standpoint, biomarkers are biological quantitative measurements that may differentiate suspected disease from healthy individuals, and predict the course of disease, or treatment response. So far, we recognize some of the risk factors for glaucoma, such as elevated IOP, although it is not always present in every patient. A combination of two or more biomarkers such as optic nerve structure, visual function and IOP, is a “biosignature” of glaucoma disease, just as measurements of high density lipoprotein (HDL), low density protein (LDL), and cholesterol have become biosignatures of cardiovascular disease.(8) Intraocular pressure A number of randomized clinical trials have convincingly shown that elevated IOP is the leading risk factor for glaucoma development and that IOP reduction can significantly reduce the incidence and progression of the disease. However, IOP can be deceiving in that it is not a defining criterion for primary open-angle glaucoma (POAG). Population surveys show that up to 50% of open-angle glaucoma patients have an IOP of 21 mm Hg or lower.(9,10) Besides, the effect of IOP fluctuation, either diurnal or long-term visit to visit, on the risk of developing POAG is still controversial.(11) Some investigators propose a joint analysis approach to assess whether variability of IOP as a biomarker is independently predictive of clinical outcomes. Using data from two long-term clinical trials of the efficacy of IOP lowering medication in the prevention of glaucoma (the Ocular Hypertension Treatment Study - OHTS and the European Glaucoma Prevention Study - EGPS), they determined if longterm IOP fluctuation is independently predictive of POAG. A linear mixed model incorporating patient-specific variance describes the trajectory of IOP, and its association with the time to POAG is assessed using both semi-parametric and full parametric survival models. Substantively, the authors results show that IOP variability is independently predictive of POAG Biomarkers and surrogate endpoints in the glaucomatous optic neuropathy: new developments and a review in the OHTS, and the subjects with high IOP fluctuation have an increased risk of developing POAG.(12) Visual function: automated perimetry The loss of retinal ganglion cells in glaucoma leads to characteristic visual field defects as evaluated by automated perimetry, although a great amount of axons has to be lost before initial visual field defects can be detected. To patients, visual function may be the clearest marker of glaucoma. There seems to be a clear relationship between visual function and quality of life.(13) Automated perimetry is a particularly useful clinical biomarker to predict disease severity, since the visual fields of apatient immediately give an appraisal about the amount of damage, and also the amount of residual vision that is available before the patient will suffer definite and clear loss of quality of life. Nevertheless, automated perimetry do have some limitations as a biomarker. Visual field defects are not disease specific. Although visual field defects in glaucoma follows typically a ganglion cell loss pattern, other optic neuropathies do cause ganglion cell loss and visual field defects similar to glaucoma.(14) The visual field index (VFI) has been developed to evaluate progression of glaucoma in time.(15) As a marker to predict the rate of disease progression, automated perimetry is not ideal, since it is usually necessary to perform a number of tests to assess progression. Besides, as a psychophysical test it is dependent on patient response and can be very variable from one exam from another. Automated perimetry is not a useful marker for early detection of a disease since a large amount of ganglion cells must be lost before initial visual field defects can be detected. Structural measures: optic nerve and retinal nerve fiber layer Direct assessment of the optic nerve and the retinal nerve fiber layer is of paramount importance in glaucoma diagnosis and progression. Progressive optic disc damage is highly predictive for the development of functional loss in glaucoma. Some changes in the optic disk are typical of the glaucomatous optic neuropathy, however, there is a number of patients with suspicious looking disks in which the structural evaluation per se is not enough for diagnosis. Although ephemeral and not very frequent, disk hemorrhage is a very typical feature in glaucoma patients and almost pathognomonic of glaucoma. It may be a marker of rapid glaucoma progression, in that localized subclinical structural change predisposes to disk hemorrhage, after which subsequent disease progression is accelerated, and recurrent optic disk hemorrhages are related to rapid structural progression of glaucomatous damage.(16) The development of new imaging devices provides better access to view the optic disk and the nerve fiber layer as potential biomarkers. Optic coherence tomography is a useful device to assess the optic nerve, and careful monitoring of the optic disc appearance is important to evaluate glaucoma progression. However, whether changes detected by imaging instruments are associated with future progression remains a key question and the ability to longitudinally evaluate imaging instruments is difficult as the technology is always evolving. Genetic biomarkers Family history is a risk factor of glaucoma. In fact, about 20% of glaucoma patients have family history of the disease and the prevalence of open-angle glaucoma increases up to 13.5% 259 among relatives of glaucoma patients indicating an important genetic component.(17,18) Genetic biomarkers might be invaluable tools to identify individuals at risk for disease as well as serving to measure the outcomes of therapies. One drawback is that no all genes can function as biomarkers. In order to have a large effect size the allele frequency has to be low; conversely, a high allele frequency has low effect size. Besides, most gene mutations and polymorphism are population specific; so one particular gene mutation in Europeans descendents may not be implicated in an African population. Model-dependent linkage analyses using multiplex POAG pedigrees have generated a number of potential loci (GLC1A– GLC1H and GLC1L) however, only three genes have been recognized. MYOC (myocilin) was the first gene identified from the GLC1A locus. (19,20) Myocilin is an extracellular protein of unknown ocular function. Missense mutations account for 3% to 5% of POAG cases.(21,22) The underlying genetic mechanism is possibly gain-of function or dominant-negative effect, since the loss of protein function does not result in glaucoma.(23-25) The disease-associated missense changes reduce the solubility of the protein, causing it to aggregate in the endoplasmic reticulum and preventing its secretion to the extracellular matrix.(26) The absence of protein does not cause disease, however, intracellular accumulation of myocilin aggregates may sensitize trabecular meshwork cells to apoptosis.(27) The second gene optineurin (OPTN) was identified at GLC1E (10p15-p14) and is primarily responsible for rare cases of familial normal tension glaucoma. (28-30) Optineurin may possibly influence ganglion cell apoptosis directly through rab8 signaling.(31,32) WD repeat domain 36 (WDR36) at GLC1G (5q21.3-q22.1) seems to be related to POAG severity in some cases, although it is neither necessary nor sufficient for disease development.(33,34) A zebrafish homolog of WDR36 stimulates apoptosis mediated by p53, implying a possible role for the gene in retinal ganglion cell susceptibility to apoptotic cell death.(35) Genome-wide scans using nonparametric linkage methods in different populations of POAG pedigrees identified 10 genomic regions that may harbor POAG susceptibility genes (2p14, 2q3334, 10-12-p13, 14q11-q22, 17p13, 17q25, 19q12-q14).(36-38) Using ordered subset analysis with the mean family age of onset as a covariate, a follow-up study of the scan performed on European descent pedigrees, distinguished some families with significant linkage to 15q11- q13, designated GLC1I.(39) TANK-binding kinase 1 is an enzyme encoded by TBK1 that can mediate NFKB activation in response to certain growth factors. The gene is specifically expressed in retinal ganglion cells affected by glaucoma. Located in chromosome 12q14, duplications of the gene were discovered in normal tension glaucoma patients. This duplication leads to increased transcription of TBK1.(40,41) Besides, TBK1 associates with the product of OPTN. (42) Nevertheless, this is a rare observation, given that, only 1% of patients displayed duplication of the TBK1 gene in a multicenter case-control study.(43) Useful genetic screening tests for POAG are not available.(44) Currently only 30% of individuals at risk for earlyonset forms of glaucoma cases can be identified.(45) Continuing research using genome-wide association in large population may reveal new genetic biomarkers and useful screening tests.(46) Rev Bras Oftalmol. 2015; 74 (4): 257-65 260 Kasahara N In order to use genes as biomarkers, one needs to have causative genes or to have genes that are associated with disease. At present, gene-based risk prediction and prognosis at early stages of the disease are possible; however, studies that isolate genes associated with late onset forms of glaucoma are still underway. Most of the genes associated with glaucoma are causative, so that, a molecular diagnosis and genetic counseling with families who carry disease are possible. Future research will aim to target newly identified genes with clinical phenotypes and outcomes, to identify genes associated with POAG, and to correlate genetic variation with disease, clinical outcome, and treatment response. Proteomic biomarkers The term proteomics was first introduced in 1994 for the aim of global characterization of a proteome (referring the proteins expressed by the genome), including protein expression, structure, modifications, functions, and interactions.(47) The proteome is the entire set of proteins, produced or modified by an organism or system.(48) Proteomics is one of the most important post-genomic approaches to improve the understanding of gene function. Nevertheless, when compared to genome, proteome is a much more complex and dynamic system. Although proteins provide the most important clues to disease mechanisms, their analysis is difficult due to large diversity in properties, such as molecular size, dynamic range in quantity, and their hydrophilicity or hydrophobicity.(49) Conversely, since blood samples can be easily collected, the proteins detectable in serum or plasma have formed the basis of commonly used tests to screen and monitor disease biomarkers in various fields. Proteomics is highly useful in the identification of candidate biomarkers (proteins in body fluids that are of value for diagnosis), identification of the bacterial antigens that are targeted by the immune response, and identification of possible immunohistochemistry markers of infectious or neoplastic diseases.(50) Recent studies of glaucoma using proteomics analysis techniques have resulted in a lists of differentially expressed proteins in human glaucoma and animal models. The global analysis of protein expression in glaucoma has been followed by cell-specific proteome analysis of both retinal ganglion cells and astrocytes. The proteomics data have also guided targeted studies to identify post-translational modifications and protein-protein interactions during glaucomatous neurodegeneration. In addition, recent applications of proteomics have provided a number of potential biomarker candidates.(49) To date, most of the studies in glaucoma molecular biomarkers comprise the studies of autoantibodies and their target antigens. A panel of antigenic proteins that elicit serum immunoreactivity at a high frequency among glaucoma patients can provide an effective tool for biomarker screening. (49) However, a much lower abundance of most protein biomarkers than some disease-irrelevant serum proteins poses a challenge of serum biomarker detection. Currently, 22 proteins were detected in glaucoma patients and included immune mediators and components of cell death signaling which may serve as biomarker candidates (Table 1).(49) Nevertheless, the clinical validation of candidate molecules still poses a major challenge. Large studies of heterogeneous cohorts for appropriate statistical power and blinding are deemed necessary to eliminate false positives and to calculate the Rev Bras Oftalmol. 2015; 74 (4): 257-65 sensitivity and specificity of candidate molecules for clinical prediction.(51,52) Besides, given the highly complex pathogenesis and the characteristic inter-patient heterogeneity of glaucoma, a panel of biomarkers, rather than a single biomarker, is needed to provide appropriate sensitivity and specificity needed.(49) Table 1. Potencial glaucoma protein biomarkers candidates (adapted from Tezel49). Protein name Accession number* A-kinase anchor protein 10, mitochondrial precursor gi|21493033 Actin, cytoplasmic gi|45011885 Heterogenius nuclear ribonucleoprotein C-like gi|282396082 Insulin-like growth factor 2 mRNA-binding protein 2 isoform b gi|56118219 Rho guanine nucleotide exchange factor 40 gi|50843837 Toll-like receptor 8 precursor gi|20302168 Tripartite motif-containing protein 5 isoform delta gi|203046698 RNA polymerase I-specific transcription initiation factor RRN3 gi|93102377 Minichromosome maintenance complex component-like isoform a gi|209954821 Hypothetical protein LOC100510472 gi|310133112 GRIP and coiled-coil domain-containing protein 2 gi|31563507 DNAJ homolog subfamily C member 7 isoform 2 gi|221219056 Zinc finger protein 804B gi|31791053 1-phosphatidylinositol-4,5-biphsophate phosphodiesterase gamma-1 isoform b gi|33598946 C-Jun-amino-terminal kinase-interacting protein 1 gi|4885433 Kinesin-like protein KIF17 isoform a gi|170784807 NACTH, LRR and PYD domains-containing protein 6 gi|21264320 Sialic acid-binding Ig-like lectin 5 precursor gi|4502659 Testis-specific serine/ threonine-protein kinase 2 gi|194294513 Poly [ADP-ribose] polymerase 1 gi|156523968 NACTH, LRR and PYD domains-containing protein 8 gi|33667040 Protocadherin gamma-A11 isoform 1 precursor gi|11128039 * GenInfo Identifier (gi) was an early system used in bioinformatics to access GenBank and related databases. A gi number was assigned to each nucleotide and protein sequence accessible through the NCBI search systems, and was a means of tracking changes to the sequence. It is an unique identifier given to a DNA or protein sequence record to allow for tracking of different versions of that sequence record and the associated sequence over time in a single data repository. Biomarkers and surrogate endpoints in the glaucomatous optic neuropathy: new developments and a review Autoimmune biomarkers There is growing evidence implying an autoimmune involvement in the pathogenesis of glaucoma. A number of studies provide fundamental insights into neurodegenerative properties of autoreactive IgG antibodies, which impair retinal ganglion cells (RGC) survival by specific binding, and assume direct and indirect triggered pathways for cell death in vivo.(53) Additional evidence of the role of autoimmunity in glaucoma is provided by the finding of elevated levels of antibodies against small heat shock proteins (a-A-crystalline, aBcrystalline, and HSP27) in normal tension glaucoma patients.(54,55) Disease-specific changes in complex profiles of naturally occurring IgG autoantibodies were detected in the sera of glaucoma patients.(56-58) Increased antibody levels (e.g. HSP70, anti-phosphatidylserine, g-enolase, glycosaminoglycans, neuron specific enolase, glutathione-S-transferase, a-fodrin, vimentin, MBP, glial fibrillary acidic protein, and retinal S-antigen) were identified and implicated as player for autoimmunity in glaucoma and also significant and selective downregulations (e.g. anti-GFAP, anti-14-3-3) could be detected in glaucoma patients.(59-68) However, whether the autoantibodies have a causative effect or appear as an epiphenomenon of the disease is yet to be unraveled. The downregulations are possibly related to a loss of natural protective autoimmunity and a disbalance of naturally occurring autoantibodies promoting neurodegenerative processes. (69,70) This unsteadiness may shift the physiological balance of protective immunity into a neuroinflammatory degenerative process leading to a predisposition for glaucoma which raises the question whether elicited autoimmunity can cause RGC loss.(53) There is a controversial debate whether autoantibodies are aberrant and contribute to disease pathogenesis or are beneficial, being part of a protective mechanism. Contradicting the principle that autoantibodies are always associated with pathological conditions, cumulative evidence demonstrate that natural autoantibodies entail protective characteristics and that autoimmunity can be protective in some situations. (71,72) Accordingly, the downregulation of some autoantibodies in glaucoma patients could lead to a loss of protective autoimmunity.(53) As a parameter associated with the presence and severity of specific disease states, autoantibody patterns are useful biomarkers for glaucoma diagnosis before its clinical manifestations. Using mass spectrometry-based proteomics to compare the autoantibody profiles in body fluids (serum, aqueous humor or tears) from patients with glaucoma with those obtained from healthy individuals, autoantibody patterns that are the most discriminating can be classified.(53) Autoantibody profiles are useful laboratory markers for the diagnosis of diseases such as cancer, rheumatoid arthritis and Alzheimer’s disease.( 73-75) In glaucoma, the complex antibody profiles are stable and consistently exist among different study populations.(65) As described previously, many autoantibody reactivities are significantly increased or decreased in glaucoma patients as compared to non-glaucoma control group. Using a pattern recognition algorithm such as artificial neural networks for unique serum autoantibody patterns, it is possible to differentiate between sera of POAG patients and healthy subjects with a sensitivity and specificity of approximately 93%.(53) Hence, autoantibodies can be highly-specific and accurate useful biomarkers for glaucoma diagnosis by simple blood testing. 261 Miscellaneous Some non-genetic molecular candidate biomarkers includes hormones such as erythropoietin, which exert its neuroprotective effect by reducing the nitric oxide-mediated formation of free radicals or antagonizing their toxicity, and hepcidin that regulates of iron efflux from numerous cell types and is expressed in the Müller cells, photoreceptors, and retinal pigmented epithelium. Table 2 depicts a list of potential nongenetic glaucoma biomarkers.(76) New proteins detected in the aqueous humor of glaucoma patients are involved in molecular events that resemble those that occur during atherosclerosis, such as, endothelial dysfunction, lipoprotein alteration, modification of smooth muscle cell functions, oxidative damage, inflammation, loss of intercellular adhesion, mitochondrial failure, and apoptosis.(77) As a whole, these observations indicate that a remarkable endothelial damage affects the anterior chamber in glaucoma, especially in the trabecular meshwork. From a biological point of view, the anterior chamber is a space that is surrounded by an endothelium and a path by which a liquid travels, so it can be considered as being similar to a vessel. (78) Hence, these new proteins are referred as vascular biomarkers ( Table 2). Neurodegenerative markers Neurodegenerative diseases are slowly progressive and irreversible disorders of the nervous system. Early detection of disease is possible by means of neurochemical measurements and neuroimaging biomarkers specifically related to the pathogenic events.(79,80) Parkinson’s and Alzheimer’s disease are typical neurodegenerative diseases and although its primary causes are different from the glaucomatous optic neuropathy, they share close similarities in several pathological findings.(81) Retinal ganglion cell bodies are located within the eyeball and its axons emerge the eye forming the optic nerve, chiasm and optic tract. As retinal ganglion cell axons project to the central nervous system, their number within the retrobulbar optic nerve may be a suitable surrogate marker for optic atrophy.(82) Thinning of the retrobulbar optic nerve has been reported both in histological and diagnostic imaging studies suggesting that the diameter of the nerve may correlate with the extent of the optic atrophy. (83-87) High-resolution magnetic resonance imaging (MRI) using an ultra fast HASTE-sequence at 3 T sequences of the optic nerve can portray axonal loss in the optic nerve comparing closely with the retinal nerve fiber layer-related parameters and could be used as a biomarker for axonal loss in glaucoma.(82) 3-T diffusion tensor imaging of the optic nerve in patients with glaucoma displays good correlation with the retinal nerve fiber layer thickness measured by OCT and may serve as a biomarker of disease severity.(88) The majority of the ganglion cells axons terminate in the lateral geniculate nucleus (LGN), the major relay station between the retina and the visual cortex.(89) In an experimental glaucoma model on monkeys, the loss of optic nerve fibers leads to degenerative changes in the LGN, with decrease in number and size of neurons and overall nucleus shrinkage.(90,91) These findings provide evidence of trans-synaptic degeneration in glaucoma, and may be relevant to understanding disease spread in select patients.(81) In vivo MRI evidence of LGN degeneration in human glaucoma is consistent with ex vivo primate and human neuropathological studies. LGN atrophy may be a relevant biomarker of visual system injury and/or progression in some cases of moderate to severe glaucoma patients.(92) Rev Bras Oftalmol. 2015; 74 (4): 257-65 262 Kasahara N Table 2. Non genetic candidate biomarkers in glaucoma (adapted from Kokotas et al76). Candidate biomarker Type Source 3 α -HSD enzyme blood Ankyrin-2* protein AH ANGPTL7 protein TM and AH Antibody for glycosaminoglycans antibody serum Antibody for GST antibody serum Antibody for NSE antibody serum Antibody for heat shock proteins antibody serum Antibody for anti-Helicobacter pylori antibody AH and serum Antibody for Chlamydia pneumoniae antibody serum nucleotide AH AP4A compound Apoliprotein B and D* proteins AH BDNF protein serum Caspase-14 enzyme AH CD44H protein TM and AH Cellular senescence antagonistic pleiotropic response AH Citrate multifunctional acid Plasma Cystatin C protein AH Cytokines proteins TM, AH, and serum ELAM1* protein AH Erythropoietin hormone AH GRP78 protein TM Heat shock 60 and 90 proteins AH kDa* Hepcidin hormone AH Homocysteine amino acid AH, plasma, and tear fluid Hydroxyproline imino acid AH and plasma Malondialdehyde aldehyde AH and plasma Myoblast determination protein 1* protein AH Myocilin protein AH and TM Myogenin* protein AH Myotrophin* protein AH Nitric oxide synthase enzyme TM, Schlemm’s canal, and collecting channels PGDS enzyme AH, TM, and serum enzyme TM Phospholipase A2 Phospholipase C β and γ* enzyme AH Transferrin protein AH Transthyretin protein AH Tumor necrosis factor α protein AH Ubiquitin fusion degradation 1-like* protein AH Vasodilator stimulated phosphoprotein* protein AH and TM AH: aqueous humor; TM: trabecular meshwork; * vascular biomarkers77 Rev Bras Oftalmol. 2015; 74 (4): 257-65 Future developments and conclusion In summary, a biomarker is an anatomic, physiologic, biochemical, or molecular parameter associated with the presence and severity of specific disease states. A biomarker may be detectable and measurable by a variety of methods, including physical examination, laboratory assays, and medical imaging. As a laboratory measurement or physical sign used in therapeutic trials as a substitute for a clinically meaningful endpoint, surrogate endpoints are used as direct measures of how a patient feels, functions, or survives and are expected to predict the effects of the therapy. For validation, a biomarker has to exhibit the capability to capture the net effects of treatment on clinical outcome, using an established scientific framework or body of evidence that elucidates the physiologic, toxicologic, pharmacologic, or clinical significance of the test results.(5) The glaucomatous optic neuropathy encompasses a number of different forms of disease, from childhood, early onset juvenile glaucoma to secondary and adult glaucoma. The discovery of specific biomarkers for each particular glaucoma is deemed necessary and poses a challenge to researchers. Hence, there is probably no single ‘ideal’ glaucoma biomarker that is going to cover all aspects of clinical disease including early detection, severity prediction, progression, and response to treatment.(5) Despite the plethora of candidates biomarkers discusses in this review, there are still unmet needs for glaucoma. What are the candidate genes that affect connective tissue biomechanics and how would that relate to glaucoma susceptibility? Is there any biomarker that indicates the speed of disease progression? Future research should focus on these issues. In the near future, as physicians, we expect to be able to establish a patient’s risk for POAG using a combination of genetic, clinical and biochemical markers, to assess the ganglion cell disease by novel imaging techniques, and initiate appropriate therapy to restore ganglion cell health.(76) REFERENCES 1. NIH Definitions Working Group. Biomarkers and surrogate endpoints in clinical research: definitions and conceptual model. In: Downing GJ, editors. Biomarkers and Surrogate Endpoints. Amsterdam: Elsevier; 2000. p.1-9. 2. Aronson JK. Biomarkers and surrogate endpoints. Br J Clin Pharmacol. 2005; 59(5):491-4. 3. Katz R. Biomarkers and Surrogate Markers: An FDA perspective. NeuroRx. 2004; 1(2):189-95. 4. Prentice RL. Surrogate endpoints in clinical trials: definition and operational criteria. Stat Med. 1989; 8(4):431-40. 5. Bhattacharya SK, Lee RK, Grus FH. Molecular biomarkers in glaucoma. Invest Ophthalmol Vis Sci. 2013; 54(1):121-31. 6. Weinreb RN, Khaw PT. Primary open-angle glaucoma. Lancet. 2004; 363(9422):1711-20. 7. Quigley HA. Number of people with glaucoma worldwide. Br J Ophthalmol. 1996; 80(5):389-93. 8. Gupta N. Playing tag with biomarkers of glaucoma. Open Ophthalmol J. 2009; 3: 29. 9. Tielsch JM, Sommer A, Katz J, Royall RM, Quigley HA, Javitt J. Racial Variations in the Prevalence of Primary Open-angle Glaucoma. The Baltimore Eye Survey. JAMA. 1991; 266(3):369-74. 10. Leske MC, Connell AM, Schachat AP, Hyman L. The Barbados Eye Study. Prevalence of open angle glaucoma. Arch Ophthalmol. 1994; 112(6):821-9. Biomarkers and surrogate endpoints in the glaucomatous optic neuropathy: new developments and a review 11. Singh K, Shrivastava A. Intraocular pressure fluctuations: how much do they matter? Curr Opin Ophthalmol. 2009; 20(1):84-7. 12. Gao F, Miller JP, Miglior S, Beiser JA, Torri V, Kass MA, Gordon MO. A joint model for prognostic effect of biomarker variability on outcomes: long-term intraocular pressure (IOP) fluctuation on the risk of developing primary open-angle glaucoma (POAG). JP J Biostat. 2011; 5(1):73-96. 13. Gutierrez P, Wilson MR, Johnson C, Gordon M, Cioffi GA, Ritch R, et al. Influence of glaucomatous visual field loss on healthrelated quality of life. Arch Ophthalmol. 1997; 115(6):777-84. 14. Hayreh SS, Zimmerman B. Visual field abnormalities in nonarteritic anterior ischemic optic neuropathy: their pattern and prevalence at initial examination. Arch Ophthalmol. 2005; 123(11):1554-62. 15. Bengtsson B, Heijl A. A visual field index for calculation of glaucoma rate of progression. Am J Ophthalmol. 2008; 145(2):343-53. 16. Suh MH, Park KH. Pathogenesis and clinical implications of optic disk hemorrhage in glaucoma. Surv Ophthalmol. 2014; 59(1):19-29. 17. Ray K, Mukhopadhyay A, Acharya M. Recent advances in molecular genetics of glaucoma. Mol Cell Biochem. 2003; 253(1-2): 223-31. 18. van Koolwijk LM, Despriet DD, van Duijn CM, Pardo Cortes LM, Vingerling JR, Aulchenko YS, et al. Genetic contributions to glaucoma: heritability of intraocular pressure, retinal nerve fiber layer thickness, and optic disc morphology. Invest Ophthalmol Vis Sci. 2007; 48(8):3669-76. 19. Stone EM, Fingert JH, Alward WLM. Identification of a gene that causes primary open angle glaucoma. Science. 1997; 275(5300):668-70. 20. Kubota R, Noda S, Wang Y, Minoshima S, Asakawa S, Kudoh J, et al. A novel myosin-like protein (myocilin) expressed in the connecting cilium of the photoreceptor: molecular cloning, tissue expression, and chromosomal mapping. Genomics. 1997; 41(3):360-9. 21. Wiggs JL, Allingham RR, Vollrath D, Jones KH, De La Paz M, Kern J, et al. Prevalence of mutations in TIGR/Myocilin in patients with adult and juvenile primary open-angle glaucoma. Am J Hum Genet. 1998; 63(5):1549-52. 22. Fingert JH, Ho E, Liebmann JM, Yamamoto T, Craig JE, Rait J, et al. Analysis of myocilin mutations in 1703 glaucoma patients from five different populations. Hum Mol Genet. 1999; 8(5):899905. 23. Wiggs JL, Vollrath D. Molecular and clinical evaluation of a patient hemizygous for TIGR/MYOC. Arch Ophthalmol. 2001; 119(11):1674-8. 24. Kim BS, Savinova OV, Reedy MV, Martin J, Lun Y, Gan L, et al. Targeted disruption of the myocilin gene (Myoc) suggests that human glaucoma-causing mutations are gain of function. Mol Cell Biol. 2001; 21(22):7707-13. 25. Resch ZT, Fautsch MP. Glaucoma-associated myocilin: a better understanding but much more to learn. Exp Eye Res. 2009; 88(4):704-12. 26. Aroca-Aguilar JD, Martínez-Redondo F, Sánchez-Sánchez F, Coca-Prados M, Escribano J. Functional role of proteolytic processing of recombinant myocilin in self-aggregation. Invest Ophthalmol Vis Sci. 2010; 51(1):72-8. 27. Joe MK, Tomarev SI. Expression of myocilin mutants sensitizes cells to oxidative stress-induced apoptosis. Implication for glaucoma pathogenesis. Am J Pathol. 2010; 176(6):2880-90. 28. Rezaie T, Child A, Hitchings R, Brice G, Miller L, Coca-Prados M, et al. Adult-onset primary open-angle glaucoma caused by mutations in optineurin. Science. 2002; 295(5557):1077-79. 29. Hauser MA, Sena DF, Flor J, Walter J, Auguste J, LarocqueAbramson K, et al. Distribution of optineurin sequence variations in an ethnically diverse population of low-tension glaucoma patients from the United States. J Glaucoma. 2006; 15(5):358-63. 263 30. Aung T, Rezaie T, Okada K, Viswanathan AC, Child AH, Brice G, et al. Clinical features and course of patients with glaucoma with the E50K mutation in the optineurin gene. Invest Ophthalmol Vis Sci. 2005; 46(8):2816-22. 31. Chalasani ML, Radha V, Gupta V, Agarwal N, Balasubramanian D, Swarup G. A glaucoma-associated mutant of optineurin selectively induces death of retinal ganglion cells which is inhibited by antioxidants. Invest Ophthalmol Vis Sci. 2007; 48(4):1607-14. 32. Chibalina MV, Roberts RC, Arden SD, Kendrick-Jones J, Buss F. Rab8-optineurin-myosin VI: analysis of interactions and functions in the secretory pathway. Methods Enzymol. 2008; 438(1):11-24. 33. Monemi S, Spaeth G, DaSilva A, Popinchalk S, Ilitchev E, Liebmann J, et al. Identification of a novel adult onset primary open-angle glaucoma (POAG) gene on 5q22.1. Hum Mol Genet. 2005; 14(6):725-33. 34. Hauser MA, Allingham RR, Linkroum K, Wang J, LaRocqueAbramson K, Figueiredo D, et al. Distribution of WDR36 DNA sequence variants in patients with primary open-angle glaucoma. Invest Ophthalmol Vis Sci. 2006; 47(6):2542-46. 35. Skarie JM, Link BA. The primary open-angle glaucoma gene WDR36 functions in ribosomal RNA processing and interacts with the p53 stress-response pathway. Hum Mol Genet. 2008; 17(6):2474-85. 36. Wiggs JL, Allingham RR, Hossain A, Kern J, Auguste J, DelBono EA, et al. Genome-wide scan for adult onset primary open angle glaucoma. Hum Mol Genet. 2000; 9(7):1109-17. 37. Nemesure B, Jiao X, He Q, Leske MC, Wu SY, Hennis A, et al. A genome-wide scan for primary open-angle glaucoma (POAG): the Barbados Family Study of Open-Angle Glaucoma. Hum Genet. 2003; 112(5-6):600-9. 38. Rotimi CN, Chen G, Adeyemo AA, Jones LS, Agyenim-Boateng K, Eghan BA Jr, et al. Genomewide scan and fine mapping of quantitative trait loci for intraocular pressure on 5q and 14q in West Africans. Invest Ophthalmol Vis Sci. 2006; 47(8):3262-67. 39. Allingham RR, Wiggs JL, Hauser ER, Larocque-Abramson KR, Santiago-Turla C, Broomer B, et al. Early adult-onset POAG linked to 15q11-13 using ordered subset analysis. Invest Ophthalmol Vis Sci. 2005; 46(6):2002-5. 40. Fingert JH, Robin AL, Stone JL, Roos BR, Davis LK, Scheetz TE, et al. Copy number variations on chromosome 12q14 in patients with normal tension glaucoma. Hum Mol Genet. 2011; 20(12):2482-94. 41. Kawase K, Allingham RR, Meguro A, Mizuki N, Roos B, SolivanTimpe FM, et al. Confirmation of TBK1 duplication in normal tension glaucoma. Exp Eye Res. 2012; 96(1):178-80. 42. Morton S, Hesson L, Peggie M, Cohen P. Enhanced binding of TBK1 by an optineurin mutant that causes a familial form of primary open angle glaucoma. FEBS Lett. 2008; 582(6):997-1002. 43. Ritch R, Darbro B, Menon G, Khanna CL, Solivan-Timpe F, Roos BR, et al. TBK1 gene duplication and normal-tension glaucoma. JAMA Ophthalmol. 2014; 132(5):544-8. 44. Fan BJ, Tam PO, Choy KW, Wang DY, Lam DS, Pang CP. Molecular diagnostics of genetic eye diseases. Clin Biochem. 2006; 39(3):231-9. 45. Mackey DA, Craig JE. Predictive DNA testing for glaucoma: reality in 2003. Ophthalmol Clin North Am. 2003; 16(4):639-45. 46. Fan BJ, Wiggs JL. Glaucoma: genes, phenotypes, and new directions for therapy. J Clin Invest. 2010; 120(9):3064-72. 47. Domon B, Aebersold R. Mass spectrometry and protein analysis. Science. 2006; 312(5771):212-7. 48. Wilkins MR, Pasquali C, Appel RD, Ou K, Golaz O, Sanchez JC, et al. From proteins to proteomes: large scale protein identification by two-dimensional electrophoresis and amino acid analysis. Biotechnology (NY). 1996; 14(1):61-5. Rev Bras Oftalmol. 2015; 74 (4): 257-65 264 Kasahara N 49. Tezel G. A proteomics view of the molecular mechanisms and biomarkers of glaucomatous neurodegeneration. Prog Retin Eye Res. 2013; 35(1):18-43. 50. Ceciliani F, Eckersall D, Burchmore R, Lecchi C. Proteomics in veterinary medicine: applications and trends in disease pathogenesis and diagnostics. Vet Pathol. 2014; 51(2):351-62. 51. Filiou MD, Martins-de-Souza D, Guest PC, Bahn S, Turck CW. To label or not to label: applications of quantitative proteomics in neuroscience research. Proteomics. 2012; 12(4-5):736-47. 52. Matt P, Fu Z, Fu Q, Van Eyk JE. Biomarker discovery: proteome fractionation and separation in biological samples. Physiol Genomics. 2008; 33(1):12-7. 53. Gramlich OW, Bell K, Hohenstein-Blaul NT, Wilding C, Beck S, Pfeiffer N, Grus J. Autoimmune biomarkers in glaucoma patients. Curr Op Pharmacol. 2013; 13(1):90-7. 54. Wax MB, Barrett DA, Pestronk A. Increased incidence of paraproteinemia and autoantibodies in patients with normal pressure glaucoma. Am J Ophthalmol. 1994; 117(5):561-8. 55. Tezel G, Seigel GM, Wax MB. Autoantibodies to small heat shock proteins in glaucoma. Invest Ophthalmol Vis Sci. 1998; 39(12):2277-87. 56. Grus FH, Joachim SC, Hoffmann EM, Pfeiffer N. Complex autoantibody repertoires in patients with glaucoma. Mol Vis. 2004; 10:132-7. 57. Joachim SC, Grus FH, Pfeiffer N. Analysis of autoantibody repertoires in sera of patients with glaucoma. Eur J Ophthalmol. 2003; 13(9-10):752-8. 58. Joachim SC, Pfeiffer N, Grus FH. Autoantibodies in patients with glaucoma: a comparison of IgG serum antibodies against retinal, optic nerve, and optic nerve head antigens. Graefes Arch Clin Exp Ophthalmol. 2005; 243(8):817-23. 59. Joachim SC, Bruns K, Lackner KJ, Pfeiffer N, Grus FH: Antibodies to alpha B-crystallin, vimentin, and heat shock protein 70 in aqueous humor of patients with normal tension glaucoma and IgG antibody patterns against retinal antigen in aqueous humor. Curr Eye Res. 2007; 32(6):501-9. 60. Kremmer S, Kreuzfelder E, Klein R, Bontke N, HennebergQuester KB, Steuhl KP, Grosse-Wilde H. Antiphosphatidylserine antibodies are elevated in normal tension glaucoma. Clin Exp Immunol. 2001; 125(2):211-5. 61. Maruyama I, Ohguro H, Ikeda Y: Retinal ganglion cells recognized by serum autoantibody against gamma-enolase found in glaucoma patients. Invest Ophthalmol Vis Sci. 2000, 41(7):1657-65. 62. Tezel G, Edward DP, Wax MB: Serum autoantibodies to optic nerve head glycosaminoglycans in patients with glaucoma. Arch Ophthalmol. 1999; 117(7):917-24. 63. Ikeda Y, Maruyama I, Nakazawa M, Ohguro H. Clinical significance of serum antibody against neuron-specific enolase in glaucoma patients. Jpn J Ophthalmol. 2002; 46(1):13-17. 64. Yang J, Tezel G, Patil RV, Romano C, Wax MB. Serum autoantibody against glutathione S-transferase in patients with glaucoma. Invest Ophthalmol Vis Sci. 2001; 42(6):1273-76. 65. Grus FH, Joachim SC, Bruns K, Lackner KJ, Pfeiffer N, Wax MB. Serum autoantibodies to alpha-fodrin are present in glaucoma patients from Germany and the United States. Invest Ophthalmol Vis Sci. 2006; 47(3):968-76. 66. Joachim SC, Reichelt J, Berneiser S, Pfeiffer N, Grus FH. Sera of glaucoma patients show autoantibodies against myelin basic protein and complex autoantibody profiles against human optic nerve antigens. Graefes Arch Clin Exp Ophthalmol 2008; 246(4):573-80. 67. Reichelt J, Joachim SC, Pfeiffer N, Grus FH. Analysis of autoantibodies against human retinal antigens in sera of patients with glaucoma and ocular hypertension. Curr Eye Res. 2008; 33(3):253-61. Rev Bras Oftalmol. 2015; 74 (4): 257-65 68. Boehm N, Wolters D, Thiel U, Lossbrand U, Wiegel N, Pfeiffer N, Grus FH. New insights into autoantibody profiles from immune privileged sites in the eye: a glaucoma study. Brain Behav Immun. 2012; 26(1):96-102. 69. Schwartz-Albiez R, Monteiro RC, Rodriguez M, Binder CJ, Shoenfeld Y. Natural antibodies, intravenous immunoglobulin and their role in autoimmunity, cancer and inflammation. Clin Exp Immunol. 2009; 158(Suppl 1):43-50. 70. Shoenfeld Y, Toubi E: Protective autoantibodies: role in homeostasis, clinical importance, and therapeutic potential. Arthritis Rheum. 2005; 52(9):2599-606. 71. Schwartz M. Physiological approaches to neuroprotection: boosting of protective autoimmunity. Surv Ophthalmol. 2001; 45(Suppl 3): S256-S260. 72. Schwartz M. Protective autoimmunity as a T-cell response to central nervous system trauma: prospects for therapeutic vaccines. Prog Neurobiol. 2001; 65(5):489-96. 73. Huijbers A, Velstra B, Dekker TJ, Mesker WE, van der Burgt YE, Mertens BJ, et al. Proteomic serum biomarkers and their potential application in cancer screening programs. Int J Mol Sci. 2010; 11(11):4175-93. 74. Nagele E, Han M, Demarshall C, Belinka B, Nagele R. Diagnosis of Alzheimer’s disease based on disease-specific autoantibody profiles in human sera. PLoS ONE. 2011; 6:e23112. 75. Hueber W, Kidd BA, Tomooka BH, Lee BJ, Bruce B, Fries JF, et al. Antigen microarray profiling of autoantibodies in rheumatoid arthritis. Arthritis Rheum. 2005; 52(9):2645-55. 76. Kokotas H, Kroupis C, Chiras D, Grigoriadou M, Lamnissou K, Petersen MB, Kitsos G. Biomarkers in primary open angle glaucoma. Clin Chem Lab Med. 2012; 50(12):2107-19. 77. Saccà SC, Centofanti M, Izzotti A. New proteins as vascular biomarkers in primary open angle glaucomatous aqueous humor. Invest Ophthalmol Vis Sci. 2012; 53(7):4242-53. 78. Izzotti A, Saccà SC, Di Marco B, Penco S, Bassi AM. Antioxidant activity of timolol on endothelial cells and its relevance for glaucoma course. Eye (Lond). 2008; 22(3):445-53. 79. Fjell AM, Walhovd KB, Fennema-Notestine C, McEvoy LK, Hagler DJ, HollandD, et al. CSF biomarkers in prediction of cerebral and clinical change in mild cognitive impairment and Alzheimer’s disease. J Neurosci. 2010; 30(6):2088-101. 80. Dickerson BC, Wolk DA. MRI cortical thickness biomarker predicts AD-like CSF and cognitive decline in normal adults. Neurology. 2012; 78(1):84-90. 81. Gupta N, Yucel YH: Glaucoma as a neurodegenerative disease. Curr Opin Ophthalmol. 2007; 18(2):110-4. 82. Lagreze WA, Gaggl M, Weigel M, Schulte-Monting J, Bubler A, Bach M, et al. Retrobulbar optic nerve diameter measured by high-speed magnetic resonance imaging as a biomarker for axonal loss in glaucomatous optic atrophy. Invest Ophthalmol Vis Sci. 2009; 50(9):4223-8. 83. Jonas JB, Schmidt AM, Muller-Bergh JA, Naumann GO. Optic nerve fiber count and diameter of the retrobulbar optic nerve in normal and glaucomatous eyes. Graefes Arch Clin Exp Ophthalmol.1995; 233(7):421-4. 84. Beatty S, Good PA, McLaughlin J, O’Neill EC. Echographic measurements of the retrobulbar optic nerve in normal and glaucomatous eyes. Br J Ophthalmol. 1998; 82(1):43-7. 85. Boles Carenini B, Tettoni E, Brogliatti B. CT and a echography of optic nerve in glaucoma. Acta Ophthalmol Scand Suppl. 2002; 236:40-1. 86. Dichtl A, Jonas JB. Echographic measurement of optic nerve thickness correlated with neuroretinal rim area and visual field defect in glaucoma. Am J Ophthalmol. 1996; 122(4):514-9. Biomarkers and surrogate endpoints in the glaucomatous optic neuropathy: new developments and a review 87. Kashiwagi K, Okubo T, Tsukahara S. Association of magnetic resonance imaging of anterior optic pathway with glaucomatous visual field damage and optic disc cupping. J Glaucoma. 2004; 13(3):189-95. 88. Wang MY, Wu K, Xu JM, Dai J, Qin W, Liu J, et al. Quantitative 3-T diffusion tensor imaging in detecting optic nerve degeneration in patients with glaucoma: association with retinal nerve fiber layer thickness and clinical severity. Neuroradiology. 2013; 55(4):493-8. 89. Perry VH, Oehler R, Cowey A. Retinal ganglion cells that project to the dorsal lateral geniculate nucleus in the macaque monkey. Neuroscience. 1984; 12(4):1101-23. 90. Weber AJ, Chen H, Hubbard WC, Kaufman PL. Experimental glaucoma and cell size, density, and number in the primate lateral geniculate nucleus. Invest Ophthalmol Vis Sci. 2000;41(6):1370-9. 265 91. Yücel YH, Zhang Q, Weinreb RN, Kaufman PL, Gupta N. Atrophy of relay neurons in magno- and parvocellular layers in the lateral geniculate nucleus in experimental glaucoma. Invest Ophthalmol Vis Sci. 2001;42(13):3216-22. 92. Gupta N, Greenberg G, Noel-de-Tilly L, Gray B, Polemidiotis M, Yucel YH. Atrophy of the lateral geniculate nucleus in human glaucoma detected by magnetic resonance imaging. Br J Ophthalmol. 2009; 93(1):56-60. Corresponding author: Alameda Madeira, 258 – sala 1206 -Alphaville – Barueri - SP CEP: 06454-010 Email: [email protected] Rev Bras Oftalmol. 2015; 74 (4): 257-65 266 Instruções aos autores A Revista Brasileira de Oftalmologia (Rev Bras Oftalmol.) - ISSN 0034-7280, publicação científica da Sociedade Brasileira de Oftalmologia, se propõe a divulgar artigos que contribuam para o aperfeiçoamento e o desenvolvimento da prática, da pesquisa e do ensino da Oftalmologia e de especialidades afins. Todos os manuscritos, após aprovação pelos Editores, serão avaliados por dois ou três revisores qualificados (peer review), sendo o anonimato garantido em todo o processo de julgamento. Os comentários dos revisores serão devolvidos aos autores para modificações no texto ou justificativa de sua conservação. Somente após aprovações finais dos revisores e editores, os manuscritos serão encaminhados para publicação. O manuscrito aceito para publicação passará a ser propriedade da Revista e não poderá ser editado, total ou parcialmente, por qualquer outro meio de divulgação, sem a prévia autorização por escrito emitida pelo Editor Chefe. Os artigos que não apresentarem mérito, que contenham erros significativos de metodologia, ou não se enquadrem na política editorial da revista, serão rejeitados não cabendo recurso. Os artigos publicados na Revista Brasileira de Oftalmologia seguem os requisitos uniformes proposto pelo Comitê Internacional de Editores de Revistas Médicas, atualizado em fevereiro de 2006 e disponível no endereço eletrônico http://www.icmje.org Artigo de Revisão: Tem como finalidade examinar a bibliografia publicada sobre um determinado assunto, fazendo uma avaliação crítica e sistematizada da literatura sobre um determinado tema e apresentar as conclusões importantes, baseadas nessa literatura. Somente serão aceitos para publicação quando solicitado pelos Editores. Deve ter: Texto, Resumo, Descritores, Título em Inglês, Abstract, Keywords e Referências. Artigo de Atualização: Revisões do estado-da-arte sobre determinado tema, escrito por especialista a convite dos Editores. Deve ter: Texto, Resumo, Descritores, Título em Inglês, Abstract, Keywords e Referências. Relato de Caso: Deve ser informativo e não deve conter detalhes irrelevantes. Só serão aceitos os relatos de casos clínicos de relevada importância, quer pela raridade como entidade nosológica, quer pela não usual forma de apresentação. Deve ter: Introdução, Descrição objetiva do caso, Discussão, Resumo, Descritores, Título em Inglês, Abstract e Keywords e Referências. Cartas ao Editor: Têm por objetivo comentar ou discutir trabalhos publicados na revista ou relatar pesquisas originais em andamento. Serão publicadas a critério dos Editores, com a respectiva réplica quando pertinente. APRESENTAÇÃO E SUBMISSÃO DOS MANUSCRITOS Preparo do Manuscrito: A) Folha de Rosto deverá conter: • Título do artigo, em português e inglês, contendo entre dez e doze palavras, sem considerar artigos e preposições. O Título deve ser motivador e deve dar idéia dos objetivos e do conteúdo do trabalho; • Nome completo de cada autor, sem abreviaturas, porém se o autor já possui um formato utilizado em suas publicações, deve informar à secretaria da revista; • Indicação do grau acadêmico e/ou função acadêmica e a afiliação institucional de cada autor, separadamente. Se houver mais de uma afiliação institucional, indicar apenas a mais relevante. Cargos e/ou funções administrativas não devem ser indicadas. • Indicação da Instituição onde o trabalho foi realizado; • Nome, endereço, fax e e-mail do autor correspondente; • Fontes de auxílio à pesquisa, se houver; • Declaração de inexistência de conflitos de interesse. O artigo enviado deverá ser acompanhado de carta assinada por todos os autores, autorizando sua publicação, declarando que o mesmo é inédito e que não foi, ou está sendo submetido à publicação em outro periódico e foi aprovado pela Comissão de Ética em Pesquisa da Instituição em que o mesmo foi realizado. A esta carta devem ser anexados: • Declaração de Conflitos de Interesse, quando pertinente. A Declaração de Conflitos de Interesses, segundo Resolução do Conselho Federal de Medicina nº 1595/2000, veda que em artigo científico seja feita promoção ou propaganda de quaisquer produtos ou equipamentos comerciais; • Informações sobre eventuais fontes de financiamento da pesquisa; • Artigo que trata de pesquisa clínica com seres humanos deve incluir a declaração de que os participantes assinaram Termo de Consentimento Livre Informado. Todas as pesquisas, tanto as clínicas como as experimentais, devem ter sido executadas de acordo com a Declaração de Helsinki. A Revista Brasileira de Oftalmologia não endossa a opinião dos autores, eximindo-se de qualquer responsabilidade em relação a matérias assinadas. Os artigos podem ser escritos em português, espanhol, inglês ou francês. A versão “on-line” da revista poderá ter artigos apenas em inglês. A Revista Brasileira de Oftalmologia recebe para publicação: Artigos Originais de pesquisa básica, experimentação clínica ou cirúrgica; Divulgação e condutas em casos clínicos de relevante importância; Revisões de temas específicos, Atualizações; Cartas ao editor. Os Editoriais serão escritos a convite, apresentando comentários de trabalhos relevantes da própria revista, pesquisas importantes publicadas ou comunicações dos editores de interesse para a especialidade. Artigos com objetivos comerciais ou propagandísticos serão recusados. Os manuscritos deverão obedecer as seguintes estruturas: Artigo Original: Descreve pesquisa experimental ou investigação clínica - prospectiva ou retrospectiva, randomizada ou duplo cego. Deve ter: Título em português e inglês, Resumo estruturado, Descritores; Abstract, Keywords, Introdução, Métodos, Resultados, Discussão, Conclusão e Referências. Rev Bras Oftalmol. 2015; 74 (4): 266-8 B) Segunda folha Resumo e Descritores: Resumo, em português e inglês, com no máximo 250 palavras. Para os artigos originais, deverá ser estruturado (Objetivo, Métodos, Resultados, Conclusão), ressaltando os dados mais significativos do trabalho. Para Relatos de Caso, Revisões ou Atualizações, o resumo não deverá ser estruturado. Abaixo do resumo, especificar no mínimo cinco e no máximo dez descritores (Keywords) que definam o assunto do trabalho. Os descritores deverão ser baseados no DeCS Descritores em Ciências da Saúde - disponível no endereço eletrônico http://decs.bvs.br/ Abaixo do Resumo, indicar, para os Ensaios Clínicos, o número de registro na base de Ensaios Clínicos (http://clinicaltrials.gov)* C) Texto Deverá obedecer rigorosamente a estrutura para cada categoria de manuscrito. Em todas as categorias de manuscrito, a citação dos autores no texto deverá ser numérica e sequencial, utilizando algarismos arábicos entre parênteses e sobrescritos. As citações no texto deverão ser numeradas sequencialmente em números arábicos sobrepostos, devendo evitar a citação nominal dos autores. Introdução: Deve ser breve, conter e explicar os objetivos e o motivo do trabalho. 267 Métodos: Deve conter informação suficiente para saber-se o que foi feito e como foi feito. A descrição deve ser clara e suficiente para que outro pesquisador possa reproduzir ou dar continuidade ao estudo. Descrever a metodologia estatística empregada com detalhes suficientes para permitir que qualquer leitor com razoável conhecimento sobre o tema e o acesso aos dados originais possa verificar os resultados apresentados. Evitar o uso de termos imprecisos tais como: aleatório, normal, significativo, importante, aceitável, sem defini-los. Os resultados da pesquisa devem ser relatados neste capítulo em seqüência lógica e de maneira concisa. Informação sobre o manejo da dor pós-operatório, tanto em humanos como em animais, deve ser relatada no texto (Resolução nº 196/96, do Ministério da Saúde e Normas Internacionais de Proteção aos Animais). Resultados: Sempre que possível devem ser apresentados em Tabelas, Gráficos ou Figuras. Discussão: Todos os resultados do trabalho devem ser discutidos e comparados com a literatura pertinente. Conclusão: Devem ser baseadas nos resultados obtidos. Agradecimentos: Devem ser incluídos colaborações de pessoas, instituições ou agradecimento por apoio financeiro, auxílios técnicos, que mereçam reconhecimento, mas não justificam a inclusão como autor. Referências: Devem ser atualizadas contendo, preferencialmente, os trabalhos mais relevantes publicados, nos últimos cinco anos, sobre o tema. Não deve conter trabalhos não referidos no texto. Quando pertinente, é recomendável incluir trabalhos publicados na RBO. As referências deverão ser numeradas consecutivamente, na ordem em que são mencionadas no texto e identificadas com algarismos arábicos. A apresentação deverá seguir o formato denominado “Vancouver Style”, conforme modelos abaixo. Os títulos dos periódicos deverão ser abreviados de acordo com o estilo apresentado pela National Library of Medicine, disponível, na “List of Journal Indexed in Index medicus” no endereço eletrônico: http://www.ncbi.nlm.nih.gov/ entrez/query.fcgi?db=journals. Para todas as referências, citar todos os autores até seis. Quando em número maior, citar os seis primeiros autores seguidos da expressão et al. Artigos de Periódicos: Dahle N, Werner L, Fry L, Mamalis N. Localized, central optic snowflake degeneration of a polymethyl methacrylate intraocular lens: clinical report with pathological correlation. Arch Ophthalmol. 2006;124(9):1350-3. Arnarsson A, Sverrisson T, Stefansson E, Sigurdsson H, Sasaki H, Sasaki K, et al. Risk factors for five-year incident age-related macular degeneration: the Reykjavik Eye Study. Am J Ophthalmol. 2006;142(3):419-28. Livros: Yamane R. Semiologia ocular. 2a ed. Rio de Janeiro: Cultura Médica; 2003. Capítulos de Livro: Oréfice F, Boratto LM. Biomicroscopia. In: Yamane R. Semiologia ocular. 2ª ed. Rio de Janeiro: Cultura Médica; 2003. Dissertações e Teses: Cronemberger S. Contribuição para o estudo de alguns aspectos da aniridia [tese]. São Paulo: Universidade Federal de São Paulo; 1990. Publicações eletrônicas: Herzog Neto G, Curi RLN. Características anatômicas das vias lacrimais excretoras nos bloqueios funcionais ou síndrome de Milder. Rev Bras Oftalmol [periódico na Internet]. 2003 [citado 2006 jul 22];62(1):[cerca de 5p.]. Disponível em: www.sboportal.org.br Tabelas e Figuras: A apresentação desse material deve ser em preto e branco, em folhas separadas, com legendas e respectivas numerações impressas ao pé de cada ilustração. No verso de cada figura e tabela deve estar anotado o nome do manuscrito e dos autores. Todas as tabelas e figuras também devem ser enviadas em arquivo digital, as primeiras preferencialmente em arquivos Microsoft Word (r) e as demais em arquivos Microsoft Excel (r), Tiff ou JPG. As grandezas, unidades e símbolos utilizados nas tabelas devem obedecer a nomenclatura nacional. Fotografias de cirurgia e de biópsias onde foram utilizadas colorações e técnicas especiais serão consideradas para impressão colorida, sendo o custo adicional de responsabilidade dos autores. Legendas: Imprimir as legendas usando espaço duplo, acompanhando as respectivas figuras (gráficos, fotografias e ilustrações) e tabelas. Cada legenda deve ser numerada em algarismos arábicos, correspondendo as suas citações no texto. Abreviaturas e Siglas: Devem ser precedidas do nome completo quando citadas pela primeira vez no texto ou nas legendas das tabelas e figuras. Se as ilustrações já tiverem sido publicadas, deverão vir acompanhadas de autorização por escrito do autor ou editor, constando a fonte de referência onde foi publicada. O texto deve ser impresso em computador, em espaço duplo, papel branco, no formato 210mm x 297mm ou A4, em páginas separadas e numeradas, com margens de 3cm e com letras de tamanho que facilite a leitura (recomendamos as de nº 14). O original deve ser encaminhado em uma via, acompanhado de CD, com versão do manuscrito, com respectivas ilustrações, digitado no programa “Word for Windows 6.0. A Revista Brasileira de Oftalmologia reserva o direito de não aceitar para avaliação os artigos que não preencham os critérios acima formulados. Versão português-inglês: Seguindo os padrões dos principais periódicos mundiais, a Revista Brasileira de Oftalmologia contará com uma versão eletrônica em inglês de todas as edições. Desta forma a revista impressa continuará a ser em português e a versão eletrônica será em inglês. A Sociedade Brasileira de Oftalmologia, Sociedade Brasileira de Catarata e Implantes Intraoculares e Sociedade Brasileira de Cirurgia Refrativa, se comprometem a custear a tradução dos artigos para língua inglesa, porém seus autores uma vez que tenham aprovado seus artigos se disponham a traduzir a versão final para o inglês, está será publicada na versão eletrônica antecipadamente a publicação impressa (ahead of print). * Nota importante: A “Revista Brasileira de Oftalmologia” em apoio às políticas para registro de ensaios clínicos da Organização Mundial de Saúde (OMS) e do Intemational Committee of Medical Joumal Editors (ICMJE), reconhecendo a importância dessas iniciativas para o registro e divulgação internacional de informação sobre estudos clínicos, em acesso somente aceitará para publicação, a partir de 2008, os artigos de pesquisas clínicas que tenham recebido um número de identificação em um dos Registros de Ensaios Clínicos validados pelos critérios estabelecidos pela OMS e ICMJE, disponível no endereço: http:/ /clinicaltrials.gov ou no site do Pubmed, no item <ClinicalTrials.gov>. O número de identificação deverá ser registrado abaixo do resumo. Os trabalhos poderão ser submetidos pela Internet, pelo site rbo.emnuvens.com.br Rev Bras Oftalmol. 2015; 74 (4): 266-8 268 Revista Brasileira de Oftalmologia Declaração dos Autores (é necessária a assinatura de todos os autores) Em consideração ao fato de que a Sociedade Brasileira de Oftalmologia está interessada em editar o manuscrito a ela encaminhado pelo(s) o(s) autor(es) abaixo subscrito(s), transfere(m) a partir da presente data todos os direitos autorais para a Sociedade Brasileira de Oftalmologia em caso de publicação pela Revista Brasileira de Oftalmologia do manuscrito............................................................. . Os direitos autorais compreendem qualquer e todas as formas de publicação, tais como na mídia eletrônica, por exemplo. O(s) autor (es) declara (m) que o manuscrito não contém, até onde é de conhecimento do(s) mesmo(s), nenhum material difamatório ou ilegal, que infrinja a legislação brasileira de direitos autorais. Certificam que, dentro da área de especialidade, participaram cientemente deste estudo para assumir a responsabilidade por ele e aceitar suas conclusões. Certificam que, com a presente carta, descartam qualquer possível conflito financeiro ou de interesse que possa ter com o assunto tratado nesse manuscrito. Título do Manuscrito___________________________________________________________________________ Nome dos Autores_______________________________________________________________________________ _____________________________________________________________________________________________ Minha assinatura abaixo indica minha total concordância com as três declarações acima. Data____________Assinatura do Autor____________________________________________________________ Data____________Assinatura do Autor____________________________________________________________ Data____________Assinatura do Autor_____________________________________________________________ Data____________Assinatura do Autor_____________________________________________________________ Data____________Assinatura do Autor____________________________________________________________ Data____________Assinatura do Autor_____________________________________________________________ Rev Bras Oftalmol. 2015; 74 (4): 266-8
Baixar