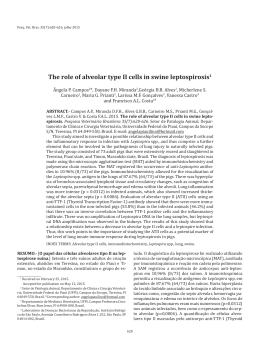
Paraneoplastic neurological syndrome associated with a pulmonary adenocarcinoma: a case report 1 2 1 2 2 3 Chaves M , Abido FC , Verardino GC , Pinheiro C , Lopes-Pontes E , Fainstein L , Carneiro SC 1,4 1. Sector of Dermatology-HUPE/UERJ and Post-Graduation Course, School of Medical Sciences, Universidade do Estado do Rio de Janeiro,Brazil 2. Department of Internal Medicine 9th Infirmary - Santa Casa da Misericórdia do Rio de Janeiro General Hospital 3. Sector of Thoracic Surgery - Bonsucesso General Hospital-Ministry of Health, Brazil 4. Sector of Dermatology-HUCFF/UFRJ and Post-Graduation Course, School of Medicine, Universidade Federal do Rio de Janeiro, Brazil Introduction Case Report Paraneoplastic neurological syndromes (PNS) can be defined as remote effects of cancer that are not caused by the tumor and its metastasis, or by infection, ischemia or metabolic disruptions. PNS are rare, affecting less than 1/10,000 patients with cancer. In most patients, the neurological disorder develops before the cancer becomes clinically. PNS are caused by autoimmune processes triggered by cancer and directed against antigens common to both cancer and the nervous system, designated as onconeural antigens. Due to their high specificity (> 90%), the best way to diagnose a neurological disorder as paraneoplastic is to identify one of the well-characterized anti-onconeural protein antibodies in the patient's serum. In addition, as these antibodies are associated with a restricted range of cancers, they can guide the search for the underlying tumor at a stage when it is frequently not clinically overt. This is a critical point as, to date, the best way to stabilize PNS is to treat the cancer as soon as possible. A 79-year-old male was admitted to this hospital because of a history of dysesthesia involving both legs, which onset was subacute and the clinical course, progressive. The patient described the pain as a uncomfortable sensation of burning induced by tactile stimuli. Approximately 1-year before the admission, the onset of intermitent cough, occasionally productive of whitish mucus, associated with a non-quantified weight-loss was related. After excluding primary neurological diseases, a thoracic CT scan showed a spiciform lung mass, in the left lower lobe (Figure 1). The patient was submitted to a lobectomy and the histopathology of the lung mass revealed an adenocarcinoma (Figure 2). Soon after the neurological symptoms have progressively improved. Most frequently paraneoplastic neurological syndromes and associated antibodies Paraneoplastic neurological syndromes Discussion Although capable of producing diverse clinical presentations, most often the remote effect of cancer takes the form of a predominantly distal, symmetrical sensory neuropathy. All these symptoms may occur months or even years before a malignant tumor is found and the tumor is most often lung cancer. Most or all PNC are immune-mediated and the best way to diagnose them is to identify one of the anti-onconeural antibodies in the patient's serum. Each of this antibodies is associated with a narrow spectrum of clinical syndromes and a restrict subgroup of cancers. ANNA-3 and anti-Hu antibody is related to lung cancer, causing sensory neuropathy as PNS (Tab 1). In most patients, the tumor is found months or even a few years after the development of the neurological disorder. Two treatment approaches have been used: removal of the source of the antigen by treating the tumor or suppression of the immune response. Frequency of Most frequently paraneoplastic origin associated tumors Subacute cerebellar ataxia 50% Ovary, breast SCLC Hodgkin's disease Others Opsomyoclonus 20% Sensory neuronopathy 20% Neuroblastoma Breast, lung SCLC Limbic encephalitis 20% SCLC Testicular SCLC Encephalomyelitis 10% SCLC Others Retinopathy NA Stiff-person syndrome Chronic gastrointestinal pseudoobstruction 20% NA SCLC Melanoma Breast SCLC Most frequently associated paraneoplastic antibodies Yo-Ab (PCA1-Ab) Hu-Ab (ANNA1-Ab) CV2-Ab (CRMP5-Ab) Tr-Ab Ma-Ab (Ta-Ab) Hu-Ab (ANNA1-Ab) Ri-Ab (ANNA2-Ab) Hu-Ab (ANNA1-Ab) CV2-Ab (CRMP5-Ab) Hu-Ab (ANNA1-Ab) CV2-Ab (CRMP5-Ab) Ma2-Ab (Ta-Ab) Amphiphysin-Ab Hu-Ab (ANNA1-Ab) CV2-Ab (CRMP5-Ab) Amphiphysin-Ab Ma2-Ab (Ta-Ab) Recoverin-Ab CV2-Ab (CRMP5-Ab) Rod-bipolar-cell-Ab Amphiphysin-Ab Hu-Ab (ANNA1-Ab) CV2-Ab (CRMP5-Ab) Adapted from Orphanet J Rare Dis 2007;2:22. Figure 1: CT scan showed a spici-form lung mass Figure 2: Lung mass after surgical excision Conclusions Although this patient had not dosed the auto-antibodies described above, his neurological syndrome turned out to be secondary to an pulmonary adenocarcinoma, a description almost identical to literature reports. References 1. Darnell RB, Posner JB. Paraneoplastic syndromes involving the nervous system. N Engl J Med 2003;349:1543-454. 2. Graus F, Delattre JY, Antoine JC, Dalmau J, Giometto B, Grisold W, Honnorat J, Smitt PS, Vedeler Ch, Verschuuren JJ, Vincent A, Voltz R. Recommended diagnostic criteria for paraneoplastic neurological syndromes. J Neurol Neurosurg Psychiatry 2004;75:1135-40. 3. Honnorat J, Antoine JC. Paraneoplastic neurological syndromes. Orphanet Journal of Rare Diseases 2007;2:22. 4. Linke R, Schroeder M, Helmberger T, Voltz R. Antibody-positive paraneoplastic neurologic syndromes: value of CT and PET for tumor diagnosis. Neurology 2004;63:282-6.
Download