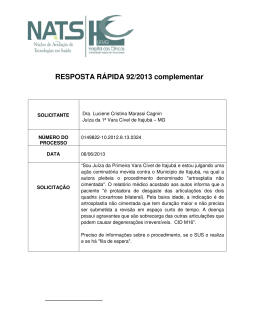
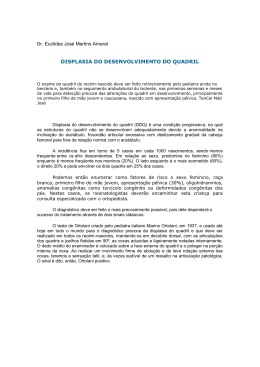
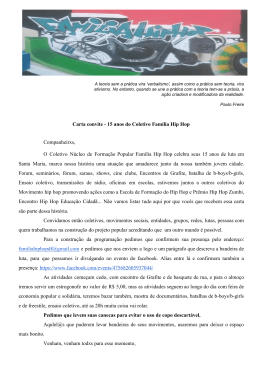
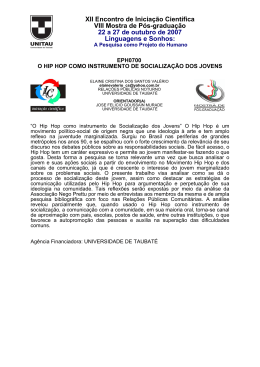
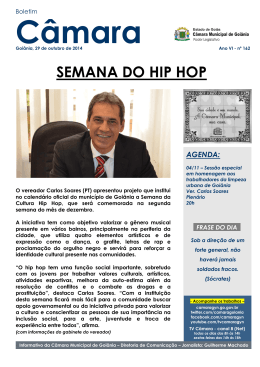
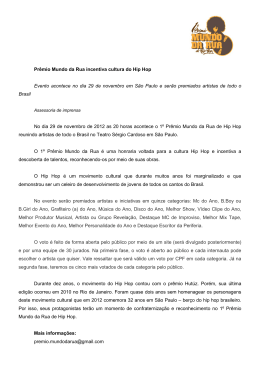
ARTROPLASTIA TOTAL DE QUADRIL MINIMAMENTE INVASIVA ARTIGO ORIGINAL / ORIGINAL ARTICLE Artroplastia total de quadril minimamente invasiva Observação preliminar* Minimally invasive total hip arthroplasty Preliminary observation* LEONARDO CARBONERA BOSCHIN1, MARCO AURÉLIO TELOKEN1, LUÍS ALBERTO RUBIN2, MARLON SCHLEDER CORREA2, PABLO MARIOTTI WERLANG2, CARLOS ROBERTO SCHWARTSMANN3 RESUMO ABSTRACT A artroplastia total de quadril é comumente realizada utilizando abordagem posterior através de uma incisão com 15-25cm de comprimento. A abordagem modificada da via posterior permite que a artroplastia total de quadril seja realizada através de uma incisão com 7-10cm (34 polegadas). A maioria dos pacientes com índice de massa corporal menor do que 30 que não apresentam cirurgias prévias é candidata a essa abordagem. A incisão é centrada no aspecto posterior da grande trocanter e afastadores especialmente desenhados para esse tipo de cirurgia são utilizados. Tanto implantes cimentados como não cimentados foram utilizados. Os pacientes recebem profilaxia farmacológica antitrombolítica e antibiótica e seguem um protocolo de reabilitação pós-operatório básico. Uma revisão dos primeiros 22 casos operados desde abril de 2002 demonstrou que o tempo cirúrgico médio foi de 113 minutos; o tamanho médio da incisão foi de 86mm; o sangramento intra-operatório foi de 388mm e o pós-operatório, de 581mm. O índice de dor pós-operatório foi de 3,14. Não The total hip arthroplasty is commonly performed using a posterior approach with a 15-25 cm incision. A modified posterior approach allows total hip arthroplasty to be performed through a 7-10 cm (3-4 inches) incision. Most patients with body mass index below 30 who have not had previous surgery are candidates for this approach. The incision is centered on the posterior aspect of the greater trochanter, and retractors specially designed for this type of surgery are used. Both cemented and uncemented implants were used. Patients received antithrombotic and antibiotic prophylaxis and followed a basic postoperative rehabilitation protocol. A review of the first 22 cases operated since April 2002 showed that mean surgery time was 113 minutes; the mean incision size was 86 mm; mean perioperative bleeding was 388 mm, and mean postoperative bleeding, 581 mm. The postoperative pain index was 3.14. There were no cases of deep infection, dislocation, or neurovascular lesion, nor failure or early loosening. Key words – Hip; surgery; arthroplasty * Trabalho realizado no Serviço de Ortopedia e Traumatologia da Santa Casa * From the Orthopedics and Traumatology Service of Santa Casa de Porto de Porto Alegre – Rio Grande do Sul (SOT-SCPA-RS). Alegre, Rio Grande do Sul (SOT-SCPA-RS), Brazil. 1. Médico Assistente do Grupo de Quadril da Santa Casa de Porto Alegre (SOT1. Assistant Orthopedic Surgeon, Hip Group of Santa Casa de Porto Alegre SCPA-RS). (SOT-SCPA-RS). 2. Médico Residente do SOT-SCPA-RS. 2. Resident, SOT-SCPA-RS. 3. Chefe do SOT-SCPA-RS. 3. Head of the SOT-SCPA-RS. Endereço para correspondência (Correspondence to): Rua Santo Antônio, 733, apto. 304 – 90220-011 – Porto Alegre, RS, Brasil. Recebido em (Received in) 27/5/03. Aprovado para publicação em (Approved in) 14/10/03. Copyright RBO2003 Rev Bras Ortop _ Vol. 38, Nos 11/12 – Nov/Dez, 2003 645 L.C. BOSCHIN, M.A. TELOKEN, L.A. RUBIN, M.S. CORREA, P.M. WERLANG & C.R. SCHWARTSMANN houve casos de infecção profunda, luxação ou lesão neurovascular, bem como falência ou afrouxamento precoces. Unitermos – Quadril; cirurgia; artroplastia INTRODUÇÃO A técnica cirúrgica para realização da artroplastia total de quadril evoluiu muito com o passar dos anos, desde a sua popularização a partir de Charnley(1). Cirurgias que duravam inicialmente de seis a oito horas atualmente são executadas em uma hora ou menos. A abordagem transtrocantérica foi o procedimento padrão no início da artroplastia total de quadril(2). Embora esse procedimento facilitasse grandemente a abordagem ao quadril, ele aumentava a morbidade, sendo a falta de consolidação do grande trocanter complicação comum. Atualmente, as osteotomias trocantéricas são raramente realizadas. Ântero-lateral(3), lateral(4), póstero-lateral(5) e posterior(6) são abordagens rotineiramente utilizadas na artroplastia de quadril, com incisões que, em média, têm 22cm(7). Cirurgiões tendem a escolher a abordagem com a qual estão mais familiarizados e se sentem mais confortáveis. Muitos cirurgiões preferem a abordagem posterior pela sua relativa facilidade de exposição e simplicidade, com incisões que variam de 15 a 25cm. Nos últimos meses, os autores iniciaram o uso de uma modificação da abordagem posterior, que permite a realização da artroplastia total de quadril por uma incisão muito menor do que a previamente usada. Divulgar o procedimento, na literatura nacional, é o objetivo principal deste artigo. MATERIAL E MÉTODOS Foram analisados os primeiros 21 pacientes (22 cirurgias) submetidos à artroplastia total de quadril com abordagem por via posterior minimamente invasiva, operados consecutivamente a partir de abril de 2002, na Santa de Casa de Porto Alegre (tabela 1). A média de idade dos pacientes era de 65,8 anos; seis pacientes (27,27%) eram do sexo feminino e 16 (72,72%), do masculino. Em seis casos (27,27%) foram utilizadas próteses não-cimentadas e em 16 (72,72%), próteses cimentadas. O quadril direito foi operado em 12 casos (54,54%), e o lado esquerdo em 10 (45,45%). A medida do sangramento intra-operatório foi obtida em estimativa por pesagem de compressas cirúrgicas e avaliação do volume de sangue aspirado do campo operatório. A medida do sangramento pós-operatório foi obtida pela quantificação do volume eliminado através 646 INTRODUCTION Surgical techniques for total hip arthroplasty have advanced a long way over the years since it has become popular after Charnley(1). Procedures that lasted six to eight hours are currently performed in one hour or less. Transtrochanteric approach was the standard procedure in the early days of total hip arthroplasty(2). Although this procedure greatly facilitated hip approach, it increased morbidity, with greater trochanter nonunion showing as a commonly found complication. Nowadays, trochanteric osteotomies are seldom performed. Anterolateral(3), lateral(4), posterolateral(5), and posterior (6) approaches are routinely used for hip arthroplasty, with incisions of averaging 22 cm(7). Surgeons tend to choose the approach with which they are more familiar and feel more comfortable. Many surgeons prefer the posterior approach, for its ease of exposure and simplicity, with incisions ranging from 15 to 25 cm. Over the last months, the authors started using a modified version of the posterior approach, that enables a total hip arthroplasty through a much smaller incision than the previously used approach. The main purpose of this paper is to report this procedure in the national literature. MATERIAL AND METHODS An analysis was carried out of the first consecutively operated 21 patients (22 surgeries) who were submitted to a total hip arthroplasty by minimally invasive posterior approach, since April 2002, at Santa Casa de Porto Alegre (table 1). Patients mean age was 65.8 years; six patients (27.27%) were female and 16 (72.72%) were male. Uncemented prostheses were used in six patients (27,27%) and cemented prostheses in 16 patients (72.72%). The right hip was operated in 12 patients (54.54%), and the left side in 10 (45.45%). The perioperative bleeding measurement was made by estimation, by weighing surgical towels and assessing the volume of blood suctioned from the surgical field. Measuring blood volume aspirated through the suction drain that remained on the patient for 48 hours estimated postoperative bleeding amount. In the analysis of the pain reported by the patient, a subjective scale from zero to 10 was used, with zero being absence of pain and 10 the worst pain reported by him. Therefore, patients were asked to report the pain they felt during the admission period. Hence, a mean pain value was obtained immediately postoperatively. The measurement of incision size was made using a flexible measuring tape with millimetermarks. Rev Bras Ortop _ Vol. 38, Nos 11/12 – Nov/Dez, 2003 ARTROPLASTIA TOTAL DE QUADRIL MINIMAMENTE INVASIVA TABELA 1 / TABLE 1 Dados descritivos Descriptive data Caso Iniciais Sexo Idade/anos SIO* SPO* TC** Dor*** TI**** Case # Initials Gender Age/years SIO* SPO* TC** Pain*** TI**** HA OC RW ILR OP ARR EDC MGF LEW DCD MHRL EDC PPVS EFMC PB EB IBM GP OPB JCS ASR MS F M M F M F M M M M M M M F M M F M F M M M 81 77 55 78 75 69 78 75 72 76 66 79 47 36 71 40 54 78 80 53 59 57 300 500 400 400 250 450 550 450 400 300 400 550 450 400 250 300 350 300 400 450 400 300 800 550 210 470 450 100 685 565 930 850 700 750 610 330 950 760 450 400 470 900 385 470 150 140 135 130 135 130 125 125 110 110 120 125 110 110 115 105 110 120 110 120 80 100 3 3 4 3 2 3 3 2 4 3 2 3 4 3 2 4 3 3 4 3 5 3 110 105 105 90 90 90 70 65 85 85 90 85 90 65 90 95 90 65 95 75 80 75 01 02 03 04 05 06 07 08 09 10 11 12 13 14 15 16 17 18 19 20 21 22 Fonte (Source): SOT-SCPA-RS (SIO: sangramento intra-operatório; SPO: sangramento pós-operatório; TC: tempo de cirurgia; TI: tamanho da incisão). *: Em mililitros; **: Em minutos; ***: Média no período da internação; ****: Em milímetros; F = feminino; M = masculino. (SIO: perioperative bleeding; SPO: postoperative bleeding; TC: surgery time; TI: incision size). *: In milliliters; **: In minutes; ***: Mean index during admission; ****: In milliliters; F = female; M = male. do dreno de aspiração, que permaneceu nos pacientes por 48 horas. Na análise da dor referida pelos pacientes, utilizou-se uma escala subjetiva de dor, marcada com escala de 0 a 10, sendo 0 a ausência de dor e 10 a pior dor referida pelo paciente. Assim, foi solicitado ao paciente que relatasse a dor sentida durante o período de internação. Foi obtido, então, um valor médio da dor no pós-operatório imediato. A medida do tamanho da incisão foi realizada utilizando-se fita métrica flexível milimetrada. Seleção do paciente O índice de massa corporal (IMC) ou índice de Quetelet(8) é o método mais útil e prático de medir o tamanho do paciente. O peso em quilogramas é dividido pela altura em metros elevada ao quadrado. Embora esse método não leve em conta a localização da gordura corporal, esta é uma simples ferramenta Rev Bras Ortop _ Vol. 38, Nos 11/12 – Nov/Dez, 2003 Patient selection The body mass index (BMI) or Quetelet’s index (8) is the most widely employed and practical method to measure the size of the patient. The weight in kilograms is divided by the squared height in meters. Although this method does not consider body fat location, it is a simple tool for patient selection. A patient with BMI above 25 is considered overweight, and above 30 is obese. The total hip arthroplasty through a small incision was originally developed as an answer to patients’ concerns with esthetic issues. Minimally invasive techniques have been developed in all areas of medicine, such as general surgery, urology, gynecology, etc., leading to a faster recovery, better cosmetic results and less morbidity. As a rule, patients who have such kind of surgery present a body mass index below 30 and have not had previous procedures onto the affected hip. The loca647 L.C. BOSCHIN, M.A. TELOKEN, L.A. RUBIN, M.S. CORREA, P.M. WERLANG & C.R. SCHWARTSMANN para seleção dos pacientes. IMC maior do que 25 é considerado de sobrepeso e acima de 30, obesidade. Realizar a artroplastia total de quadril através de uma incisão pequena foi originalmente desenvolvida como resposta às preocupações do paciente em relação à estética. Técnicas minimamente invasivas têm sido desenvolvidas em todas as áreas da medicina, tais como cirurgia geral, urologia, ginecologia, entre outras, trazendo os benefícios de recuperação mais rápida, mais cosmética e com menor morbidade. Como regra, os pacientes submetidos a esse tipo de cirurgia têm índice de massa corporal menor do que 30 e não apresentam cirurgias prévias no quadril envolvido. A localização da gordura corporal também deve ser considerada. Pacientes que apresentam grande quantidade de gordura corporal, a despeito de seu IMC, mas que têm pequena quantidade de gordura na região dos quadris, também são candidatos à pequena incisão. Entretanto, a experiência também demonstrou que coxas extremamente musculosas dificultam a exposição e, nestes casos, uma abordagem maior pode ser necessária. Técnica cirúrgica Anestesia epidural hipotensiva é recomendada para a realização do procedimento, uma vez que um campo cirúrgico com pouca presença de sangue facilita bastante a visualização. Profilaxia antibiótica, com 2g de cefalotina para pacientes com mais de 60kg, é realizada rotineiramente. O paciente é posicionado em decúbito lateral, devendo o cirurgião certificar-se de que a pelve do paciente está segura e perpendicularmente fixada em relação à mesa cirúrgica e o corpo alinhado axialmente, o que ajudará no correto posicionamento do componente acetabular da prótese. A borda posterior do grande trocanter é identificada e uma incisão longitudinal de 7 a 10cm é realizada. Esse tamanho de incisão é escolhido baseado na equação geométrica ia (tamanho do componente acetabular x 2) igual aproximadamente à incisão mínima necessária para que um componente acetabular de 56mm possa ser colocado sem que entre em contato com o tecido celular subcutâneo, pele e instrumental, permitindo para tal o estiramento da pele ao redor de 15%. Metade da incisão é realizada proximal ao topo do grande trocanter e a outra metade, distal (figura 1). O tecido celular subcutâneo é dissecado e a fascia lata identificada. A fascia lata é aberta conforme a incisão cutânea e pode ser ampliada por pequena extensão distal e proximal, com o objetivo de ajudar na exposição. O afastador de Charnley é posicionado no nível do grande trocanter, tendo o cuidado de não lesar o nervo ciático. Enquanto se trabalha com a coxa estendida, a mesma é ligei648 Fig. 1 – Incisão centrada no aspecto posterior do grande trocanter Fig. 1 – Incision centered at greater trochanter posterior aspect tion of body fat should also be considered. Patients who have large amounts of body fat, regardless of the BMI, but still have small amounts of fat on the hip region, are also candidates for the small incision. However, experience has also shown that extremely muscular thighs make exposure difficult, and in such cases, a larger incision may be required. Surgical technique Hypotensive epidural anesthesia is recommended for this procedure, as a surgical field with smaller amounts of blood turns viewing much easier. Antibiotic prophylaxis with 2 grams of cephalothin for patients with more than 60 kg is routinely provided. The patient is positioned onto his or her side, and the surgeon has to assure that the pelvis of the patient is secure and fixed perpendicularly to the operating table and the body axially aligned, which will help with the proper placement of the prosthetic acetabular component. The posterior edge of the greater trochanter is identified and a longitudinal 7 to 10 cm incision is performed. This size of incision is chosen based on the ia geometric equation (acetabular component size x 2), and approximately equals the minimum incision required for the placement of a 56 mm acetabular component without any contact with subcutaneous tissue, skin and instruments, creating skin tension of around 15%. Half of the incision is made proximally to the upper portion of the greater trochanter, and the other half distally (figure 1). Subcutaneous tissue is dissected and the fascia lata is identified. The fascia lata is incised following skin incision. The fascial incision can be enlarged beneath the skin incision Rev Bras Ortop _ Vol. 38, Nos 11/12 – Nov/Dez, 2003 ARTROPLASTIA TOTAL DE QUADRIL MINIMAMENTE INVASIVA Fig. 2 – Exposição do acetábulo Fig. 2 – Acetabulum exposure ramente rodada internamente. Um afastador de Hohmann curvo estreito é colocado na porção superior do colo do fêmur e outro, inferiormente. A gordura que recobre os rotadores externos é removida com um descolador tipo Cobb ou uma rugina. Os rotadores externos devem ser visualizados nesse ponto. Os rotadores externos, com exceção de parte do quadrado femoral e da cápsula posterior, são liberados de suas inserções. O piriforme e o tendão conjunto são reparados com sutura de fio inabsorvível e descolados da cápsula posterior. A cápsula é, então, incisada de maneira a formar retalho trapezoidal e suas bordas reparadas com fio inabsorvível para posterior reinserção. O quadril é luxado e o músculo quadrado femoral rebatido, o que facilita a visualização do pequeno trocanter. O corte no colo do fêmur é realizado na altura apropriada, conforme medição pré-operatória, com serra oscilatória, e a cabeça femoral removida. A perna é deixada em extensão sobre a mesa com o acetábulo exposto. Um afastador de Hohmann curvo é colocado sobre a porção superior da borda anterior do acetábulo (figura 2). Um prego de Freeman é posicionado na borda lateral do acetábulo na posição de 12 horas. Com a perna em extensão, outro afastador de Hohmann curvo é posicionado, de maneira justaóssea, na borda posterior do acetábulo. Nesse ponto, o cirurgião deve ter cuidado para não lesar o nervo ciático no momento da colocação desse afastador. Um terceiro afastador de Hohmann é colocado inferiormente, justadistal ao ligamento transverso do acetábulo. O lábrum é, a seguir, excisado em toda sua extensão. Nesse ponto, o acetábulo deve estar bem exposto. O pulvinar deve ser removido e a fresagem é, então, iniciada. Terminada a fresagem, o componente Rev Bras Ortop _ Vol. 38, Nos 11/12 – Nov/Dez, 2003 by a small distal and proximal extension to help exposure. The Charnley retractor is carefully positioned at the level of the greater trochanter, avoiding injury to the sciatic nerve. The thigh is extended, and then slightly internally rotated. A narrow bent Hohmann retractor is placed on the upper portion of the femoral neck, and another retractor is inferiorly placed. The fat covering external rotators is removed with a Cobb-like elevator or a retractor. The external rotators should be seen by now. The external rotator muscles, except for parts of quadratus femoris muscle and the posterior capsule, are released from their insertions. The piriformis muscle and the conjoint tendon are repaired with nonabsorbable suture and detached from the posterior capsule. The capsule is then incised to form a trapezoid flap with its edges repaired with nonabsorbable sutures for later reinsertion. The hip is dislocated and the quadratus femoris muscle reflected, enhancing lesser trochanter view. The femoral neck osteotomy is performed at the appropriate height according to the preoperative measurement, with an oscillating saw, and the femoral head is removed. The leg is left extended on the table with the acetabulum exposed. A bent Hohmann retractor is placed on the upper portion of the anterior edge of the acetabulum (figure 2). A Freeman nail is placed on the lateral edge of the acetabulum at a 12 o’clock position. With the leg extended, another bent Hohmann retractor is placed close to the bone at the upper edge of the acetabulum. At this moment, the surgeon must avoid injury to the sciatic nerve during retractor placement. A third Hohmann retractor is inferiorly placed, distally to the transverse ligament of the acetabulum. Next, the labrum is excised all the way. At this time, the acetabulum should be well exposed. The pulvinar pad should be removed and reaming is started. After reaming completion, the acetabular component is inserted (figure 3). Uncemented components facilitate the procedure at this stage. All retractors are removed and a wet pack is placed to protect the acetabulum. The leg is flexed and internally rotated. A retractor for the femoral neck is placed to lift the proximal portion of the femur. The femoral canal is then prepared and the trial femoral component is inserted. The trial reduction is then performed and, if satisfactory, a component of the same size is placed into the femoral canal (figure 4). Before the final reduction, two 2 mm holes are drilled on the greater trochanter. Repair sutures previously made at the capsule and piriformis muscle are passed through these holes, but are not tied. The hip is reduced and sutures are tied (figure 5). The wound is washed and a suction drain is placed deeply into the 649 L.C. BOSCHIN, M.A. TELOKEN, L.A. RUBIN, M.S. CORREA, P.M. WERLANG & C.R. SCHWARTSMANN Fig. 3 – Colocação do componente acetabular Fig. 3 – Acetabular component fitting acetabular é inserido (figura 3). Componentes não cimentados facilitam a cirurgia nesse tempo operatório. Todos os afastadores são removidos e uma compressa úmida é colocada com o intuito de proteger o acetábulo. A perna é fletida e rotada internamente. Um afastador para o colo do fêmur é posicionado para elevar a porção proximal do fêmur. O canal femoral é, então, preparado e o componente femoral de teste colocado. A prova de redução é, então, realizada e, se tudo estiver satisfatório, um componente com a mesma medida é inserido no canal femoral (figura 4). Antes da redução final, dois furos de 2mm são realizados no grande trocanter. As suturas de reparo previamente realizadas com a cápsula e o piriforme são passadas por esses furos, mas não amarradas. O quadril é reduzido e as amarras realizadas (figura 5). A cicatriz é lavada e um dreno de aspiração colocado profundamente à fáscia. O subcutâneo e a pele são suturados e um curativo compressivo aplicado. Se não ocorrer sangramento ou secreção serosa, o curativo é mantido fechado por 48 horas e só então a ferida operatória é revista. Profilaxia dos fenômenos tromboembólicos é utilizada durante a internação, bem como antibióticos por 48 horas, que correspondem ao período de permanência do dreno de aspiração. A dor, inicialmente, é manejada com analgésicos por via intramuscular, quando necessário, e gradualmente substituída por medicação via oral. Fisioterapia motora e respiratória é iniciada tão cedo quanto possível. Esta deve permitir ao paciente deambular com auxílio de andador ou muletas, antes da alta hospitalar. 650 Fig. 4 – Inserção do componente femoral Fig. 4 – Acetabular component insertion Fig. 5 – Redução dos componentes Fig. 5 – Component reduction fascia. The subcutaneous and the skin are sutured and a compressive dressing is applied. If there is no bleeding or serous discharge, the dressing is kept closed for 48 hours and only then the surgical wound is reviewed. Prophylaxis of thromboembolic phenomena is employed during hospital stay, as well as antibiotics for 48 hours, which corresponds to the period the suction drains remains in place. Pain is initially managed with IM analgesics when necessary, and gradually replaced by oral medication. Motor and respiratory physical therapy is started as soon as possible. It should enable the patient to walk with the help of a walker or crutches before hospital discharge. Rev Bras Ortop _ Vol. 38, Nos 11/12 – Nov/Dez, 2003 ARTROPLASTIA TOTAL DE QUADRIL MINIMAMENTE INVASIVA RESULTADOS A técnica minimamente invasiva vem sendo utilizada no SOT-SCPA-RS desde abril de 2002 e 21 pacientes (22 cirurgias) já foram operados dessa maneira. O tempo cirúrgico médio foi de 113 minutos e o sangramento intra-operatório, de aproximadamente 388ml. O sangramento pós-operatório medido foi de aproximadamente 581ml. Quando analisada a dor pósoperatória, obteve-se um índice aproximado de 3,14 numa escala de 0 a 10. Avaliada a cicatriz pós-operatória, o tamanho médio das incisões foi de 86mm. O tempo de seguimento dos pacientes foi, em média, de seis meses e não se evidenciou nesse período nenhum caso de infecção profunda, de luxação ou de lesão neurovascular. Até o momento nenhum caso de falência precoce ou afrouxamento dos componentes da prótese foi detectado. Um paciente (4,5%) apresentou infecção superficial da ferida operatória, sendo submetido à antibioticoterapia com resolução completa do problema; outro paciente apresentou úlcera duodenal perfurada no 40o dia pós-operatório; devido às complicações, evoluiu para óbito. Fig. 6 – Afastadores especiais Fig. 6 – Special retractors RESULTS The minimally invasive technique has been used at the SOTSCPA-RS since April 2002 and 21 patients (22 surgeries) were DISCUSSÃO Quando as condições possibilitam a realização de um procedimento com um mínimo de exposição, a abordagem por via posterior modificada descrita previamente pode permitir ao cirurgião fazer toda a cirurgia sem maiores dificuldades. Como na maioria dos procedimentos em ortopedia, existe uma curva de aprendizado e o treinamento da equipe é fundamental. Anestesia epidural hipotensiva, quando possível, é de grande auxílio na diminuição do sangramento intra-operatório, ajudando na manutenção de campo operatório exangue. A manutenção da posição do paciente durante a cirurgia é de grande importância, evitando erros no posicionamento dos implantes. O uso de afastadores apropriados para este tipo de cirurgia ajuda muito na exposição do campo operatório (figura 6). A utilização de próteses não cimentadas parece ser o ideal para este tipo de abordagem, uma vez que a própria colocação do cimento pode ser difícil, principalmente se manual (finger pack) e não com pistola. Entre as poucas comunicações sobre o tema, Crockett et (*) al demonstraram que não houve diferença significativa na relação tempo cirúrgico versus incidência de complicações entre as diferentes abordagens. Swanson e Hanna(**) bem como Goldstein e Gordon(***) apresentaram dados semelhantes, em relação à diferença no tempo cirúrgico, mas relataram sangramento intra-operatório ao redor de 280ml para a artroplastia minimamente invasiva e de 450ml para as artroplastias Rev Bras Ortop _ Vol. 38, Nos 11/12 – Nov/Dez, 2003 already operated with this procedure. Mean surgical time was 113 minutes and mean perioperative bleeding was around 388 ml. Mean postoperative bleeding was around 581 ml. Postoperative pain was approximately 3.14 in a scale from 0 to 10. According to a postoperative wound measurement, mean incision size was 86 mm. Mean patient follow-up was six months, and no deep infection or neurovascular lesion appeared during this period. To date, no case of early failure or loosening of the prosthetic components has occurred. One patient (4.5%) showed superficial infection on the surgical wound, receiving antibiotics, with complete resolution of the problem. Another patient presented a perforated duodenal ulcer at the 40th postoperative day and eventually died due to complications. DISCUSSION Whenever conditions allow a minimum exposure procedure, the previously described modified posterior approach enables the surgeon to perform the procedure without much difficulty. As in most orthopedics procedures, there is a learning curve, and training of the staff is crucial. Hypotensive epidural anesthesia, whenever possible, is important to decrease perioperative bleeding, helping to keep blood out of the operative field. The stability of the patient position during surgery is of paramount importance, avoiding implant misplacement. The use 651 L.C. BOSCHIN, M.A. TELOKEN, L.A. RUBIN, M.S. CORREA, P.M. WERLANG & C.R. SCHWARTSMANN tradicionais. Em nossa caof proper retractors for this suística encontramos um vakind of surgery greatly enlor intermediário ao relatado hances the exposure of operpor esses autores (388ml) ative field (figure 6). The use referente ao sangramento inof uncemented prostheses tra-operatório, talvez por esta seems to be the ideal choice ser uma técnica nova e ainda for this kind of approach, as estarmos na curva de aprencementing can be difficult, dizado. Já o tamanho médio particularly if performed with das incisões que praticamos finger packing technique, – aproximadamente 86mm – without a cement gun. parece estar em sintonia com Among the few communias relatadas por diversos aucations on that subject, tores, como Right et al(7), Crockett et al(*) showed that (**) Fig. 7 – Aspecto cosmético da incisão Swanson e Hanna e Goldthere was no significant difFig. 7 – Incision cosmetic aspect stein e Gordon(***). ference in relation to surgical O mesmo parece acontetime versus incidence of comcer com o tempo cirúrgico, plications among different uma vez que inicialmente precisávamos de até duas horas e approaches. Swanson and Hanna(**), as well as Goldstein et 30 minutos para fazer a cirurgia; atualmente, a cirurgia é reaal(***), presented similar data related to surgical time difference, lizada no mesmo tempo que necessitamos para uma artrobut reported perioperative bleeding of approximately 280 ml plastia convencional. for minimally invasive arthroplasty, and 450 ml for convenQuando observada a dor pós-operatória, não encontramos tional arthroplasty. In our series, we have found an intermedinenhuma fonte na literatura que tenha analisado esta questão, ate amount of perioperative bleeding in comparison to the valmas a impressão que temos é de que esses pacientes parecem ues reported by those authors (388 ml), maybe because this is a necessitar menos de substâncias analgésicas no pós-operatónew technique and we are still in the learning curve. Considerrio imediato, comparado com a artroplastia realizada através ing average size of incisions – approximately 86 mm – it seems das incisões tradicionais. O índice médio de intensidade de to overlap those reported by several authors like Right et al(7), Swanson et al(**) and Goldstein and Gordon(***). dor – 3,14 pontos – obtido nesta casuística deve ser consideThe same seems to apply to surgical time, as we needed rado como um valor baixo, mas reconhecemos que são necesinitially up to two hours and 30 minutes to perform the sursários outros estudos comparativos para confirmar nossa imgery, and today the procedure is performed in the same time pressão em relação à intensidade da dor no pós-operatório we need to perform a conventional arthroplasty. com a técnica minimamente invasiva. When assessing postoperative pain, we have not found any O uso desta técnica não é para todos os pacientes, mas é mention in literature assessing this issue, but our impression segura e eficaz quando utilizada com as indicações e os mateis that the patients seem to need less analgesic drugs during riais adequados, sendo que a cicatriz cutânea proporciona um immediate postoperative period, when compared with arthroresultado cosmético bem satisfatório (figura 7). A diferença plasty through conventional incision. The average pain intenem relação às outras técnicas tradicionais pode ser nada mais sity index – 3.14 – of those patients should be considered low, que estética e a própria percepção do paciente e do médico. but we recognize that other comparative studies are required before we confirm our impression concerning postoperative pain intensity using minimally invasive technique. **(*) Crockett H., Wright J., Bonner K.: Mini-incision for total hip arthroplasty. Scientific Exhibit. AAOS, Annual Meeting, New Orleans, 1998. Not all patients are eligible, but this technique is safe and *(**) Swanson T., Hanna R.: Advantages of cementless total hip arthroplasty effective when advocated for the proper indications and mausing minimally invasive surgical technique. AAOS, Annual Meeting, New terial, and the cosmetic result of skin wound is rather satisOrleans, 2003. factory (figure 7). The difference in comparison to other con(***) Goldstein W., Gordon A.: Minimal incision total hip artroplasty. AAOS, Annual Meeting, New Orleans, 2003. ventional techniques can be just esthetic, and the perception 652 Rev Bras Ortop _ Vol. 38, Nos 11/12 – Nov/Dez, 2003 ARTROPLASTIA TOTAL DE QUADRIL MINIMAMENTE INVASIVA Um viés de seleção por pacientes magros ou não obesos é inquestionável. Um estudo prospectivo e randomizado será a melhor maneira de comparar e averiguar a abordagem minimamente invasiva do quadril. by the patient and by the surgeon. A selection bias for either slim or non-obese patients is undisputed. A prospective, randomized trial will be the best way to compare and investigate the minimally invasive approach of the hip. COMENTÁRIO FINAL FINAL REMARK O objetivo deste artigo não é encorajar os cirurgiões a realizarem todas as suas artroplastias de quadril através de uma incisão de 5-10cm de comprimento. Cada cirurgião deve, obviamente, utilizar a abordagem com a qual está mais familiarizado e que permite a ele realizar uma boa cirurgia. The purpose of this study is not to encourage surgeons to perform all their hip arthroplasties through a 5-10 cm incision. Every surgeon should obviously use the approach with he or she is more familiar, yielding a satisfactory surgery. REFERÊNCIAS / REFERENCES 1. Charnley J.: Arthroplasty of the hip: a new operation. Lancet 1: 1129-1132, 1961. 2. Amstutz H.C., Maki S.: Complications of trochanteric osteotomy in total hip replacement. J Bone Joint Surg [Am] 60: 214-216, 1978. 3. Watson-Jones R.: Fractures of the neck of the femur. Br J Surg 23: 787, 19351936. 4. Hardinge K.: The direct lateral approach to the hip. J Bone Joint Surg [Br] 64: 17-19, 1982. Rev Bras Ortop _ Vol. 38, Nos 11/12 – Nov/Dez, 2003 5. Langenbeck B von: Über die Schussverletzungen des Huftgelenks. Arch Klin Chir 16: 263, 1874. 6. Moore A.T.: Moore self-locking vitallium prosthesis in fresh femoral neck fractures: a new low posterior approach. AAOS Instr Course Lect 16: 309, 1959. 7. Right J.M.W., Rockett H.C.C., Sculco T.C.: Mini-incision for total hip arthroplasty. Orthop Espec Edit 7: 18-20, 2001. 8. Bray G.: Overweight is risking fate. Definition, classification, prevalence and risks. Ann N Y Acad Sci 499: 14-28, 1987. 653
Baixar