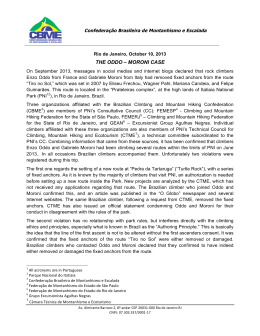
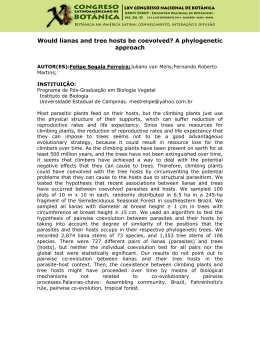
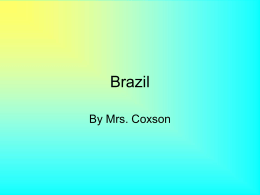
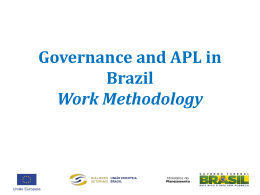
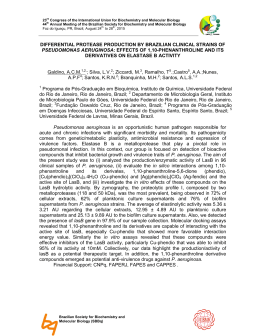
Original Paper. Physical Education and Sport, 52, 73 - 76, 2008 DOI: 10.2478/v10030-008-0015-5 Authors’ contributions: A Study design B Data collection C Statistical analysis D Data interpretation E Literature search F Manuscript preparation G Funds collection Somatic and functional profile of sport rock climbers André Padrenosso 1,2 A D, Erik S. de Godoy 1 – 5 A B D - F, Eurico César 2 E F, Ana Barreto 1,2 C E F, Vitor Reis 5 E F, Antonio Silva 5 E F, Estélio Dantas 2,5 C - F 1 Centro Universitário Celso Lisboa, Rio de Janeiro, RJ; 2 Laboratório de Biociências da Motricidade Humana, Universidade Castelo Branco, Recreio dos Bandeirantes, RJ; 3 Centro Universitário Augusto Motta, Rio de Janeiro, RJ; 4 Universidade Veiga de Almeida, Cabo Frio, RJ, Brazil; 5 Universidade de Trás-os-Montes e Alto Douro, Vila Real, Portugal Summary Study aim: To evaluate the physical fitness of rock climbers. Material and methods: A group of 21 male and 9 female climbers, mean age 30.5 ± 8.8 years, training on indoor climbing walls and on outdoor rocks participated in the study. Cardio-respiratory fitness was evaluated using the Polar OwnIndex, highly correlated with the ‡O2max. Neuromuscular fitness was evaluated by maximum repetition and maximum endurance tests for upper extremities, simulating the holding conditions specifically met by climbers. Results: Male climbers were far stronger than the female ones as evidenced by the average numbers of pull-ups (13.8 and 3.2, respectively; p<0.001) and had higher cardiorespiratory fitness (p<0.05). Moreover, women rated their climbing skills markedly lower than men (4.8 ± 0.9 and 6.3 ± 1.2, respectively). Conclusion: Cardio-respiratory fitness and dynamic strength of upper extremities seem to be the key factors in sport climbing. Key words Rock climbing – Cardio-respiratory fitness – Neuromuscular fitness Introduction Rock climbing has increased in popularity in Rio de Janeiro (Brazil), a city with many rocky mountains of easy access. Climbers look for excitement and adventure without, however, giving up safety. Nevertheless, it is usual to observe climbers who use established methods with no regard to biological individuality and specificity. It is therefore important to identify the level of physical fitness required for the safe practice of climbing, so that training regimens, whether recreational or competitive, may be adequately prescribed and a safer initiation to the sport may be provided. Physical evaluation can be performed with two main objectives: to determine the health-related physical fitness and the sport performance. According to the American College of Sports Medicine [1], cardio-respiratory fitness, one of the most important components of health-related physical fitness, refers to the ability to perform prolonged physical activity of dynamic, moderate-to-high intensity, engaging large muscle groups. Strength, localised muscle resistance and flexibility are components of neuro- muscular fitness. According to Heyward [12], these components are necessary for maintaining functional independence and for the capacity to perform physical activities without excessive fatigue and stress. These basic principles pose the question about the somatic and functional characteristics, as indicators of the training process of rock climbers. The aim of this study was thus to evaluate the anthropometric, cardio-respiratory and neuromuscular fitness measures, as well as climbingspecific muscle activity and skills in sport climbers. Material and Methods The study, based on a project [18,23] aimed at evaluating somatic and functional features of rock climbers, included 21 male and 9 female climbers training on indoor climbing walls, as well as on rocks. The subjects were members of an indoor climbing training centre in Rio de Janeiro, who practiced rock climbing for at least one year, training volume amounting to at least three sessions per week, including obligatory rock climbing. All the participants were adequately informed about the Dr Erik Salum de Godoy LABIMH UCB/RJ, Av Salvador Allende 6700, 22780-160, Recreio dos BandAuthor’s address eirantes, RJ, Brazil [email protected] 74 A. Padrenosso et al. objectives of the study and the procedures they would be submitted to, and signed an informed consent according to the guidelines for research with human participants [5,20,24]. The following variables were measured: anthropometric (body mass and height, body composition [10,11, 15,19], cardio-respiratory fitness (by using Polar OwnIndex, highly correlated with ‡O2max; r = 0.97; [13]), neuromuscular fitness (by applying a maximum repetition test consisting of pull-ups on a bar [4]) and maximum endurance (straight-arm hang). Neuromuscular tests were conducted with the use of resin holds, specific for indoor climbing walls. A 5-min interval was allowed between the tests. The participants were requested to restrict their physical activities for 48 h before the tests and to drink at least 2 l of water on the day preceding the tests, so they were properly hydrated for evaluation of body composition with use of electrical bioimpedance. A Body height was determined with a portable stadiometer (Cescorf, Brazil), body mass with a portable digital scale (Plena, Brazil), relative body fat content with a bipolar bioimpedance device (Techline, Brazil) cardio-respiratory fitness with a heart rate monitor (Polar, model M52, Finland); symmetrical holds (Wall type, VDoze, Brazil), attached to an artificial wall, and a manual digital chronometer (Polar, model S120, Finland) were used to assess neuromuscular fitness; rating scale adopted by FMERJ (Rio de Janeiro´s Mountain Sports Federation) was applied to rate climbing skills (FMERJ: 1-11a). Details of the tests and equipment are shown in Fig. 1. The data were described by using means, standard deviations, ranges and coefficients of variability [17,22]. The distributions of all variables proved normal by the Kolmogorov-Smirnov’s test, SPSS v.10 software being used. B C D Fig. 1. Equipment used in assessing the fitness of climbers A – VDoze holds; B – System Wall model Attachment of the holds to the artificial climbing wall; C – Performance of the maximum repetition test; D – Performance of the maximum endurance test Table 1. Somatic and functional characteristics of male (n = 21) and female (n = 9) climbers Gender Variable Mean ± SD Age (years) 28.7 ± 5.1 Body height (cm) 173.9 ± 9.2 Body mass (kg) 67.0 ± 8.1 Lean body mass (kg) 61.6 ± 6.4 Body fat content (%) 8.3 ± 4.4 Climbing experience (months) 90.6 ± 61.6 Training frequency (days/wk) 3.5 ± 1.2 CRF (ml/kg/min) 46.9 ± 8.4 Isometric force (s) 96.5 ± 27.0 Dynamic force (n) 13.8 ± 5.1 Self-rated climbing skills 6.3 ± 1.2 Men Range 21 - 40 155 – 187 55,5 – 80,7 52,0 - 74,2 4,7 – 18,3 6 – 228 1–6 37 – 68 58 – 153 5 - 24 4–8 CV 18 5 12 10 53 68 33 18 28 38 19 Mean ± SD 34.8 ± 13.7 160.2 ± 3.8*** 53.3 ± 5.3*** 43.0 ± 4.1*** 18.8 ± 7.9*** 32.7 ± 26.4*** 3.3 ± 1.4 38.0 ± 10.5* 90.3 ± 28.3 3.2 ± 4.7*** 4.8 ± 0.9** Women Range 23 – 68 152,3 – 165,5 45 – 59 33,6 – 47,5 7,5 – 30,4 1 – 84 1–6 21 – 53 53 - 142 0 – 11 4–6 CV 39 2 10 9 49 81 42 28 31 144 19 Legend: CRF – Cardio-respiratory fitness; Self-rated climbing skills – Scale 1-11a; Significantly different from the respective value in men: * p<0.05; ** p<0.01; *** p<0.001 75 Somatic/functional profile of sport climbers Results Mean results (± SD and ranges) of the studied variables are presented in Table 1. Body height of the subjects was rather average and body mass in relation to height was low and they were very lean. Men were far stronger than women as evidenced by the average numbers of pull-ups (13.8 and 3.2, respectively; p<0.001) and had higher cardio-respiratory fitness (p<0.05). Moreover, women rated their climbing skills also markedly lower than men (4.8 ± 0.9 and 6.3 ± 1.2, respectively). Discussion Bertuzzi et al. [2] suggested that some somatic features, e.g. body composition, were of importance: climbers having low body fat performed better than those more fatty. More frequent trainings and a longer experience had a positive effect on somatic features. In this study, high training frequency, long experience and high skill/ technique ratings tended to be associated with low body fat. On the other hand, Mermier et al. [14] reported different results and concluded that specific somatic patterns had no direct effect on rock climbing performance. Body fat content we found in male climbers was quite low, while in many female ones was above average according to the classification of Pollock and Wilmore [16]. The method of electrical bioimpedance used in this study was easy and sufficiently reliable as the technique does not depend on evaluators skills and/or expertise [11,12]. Cardio-respiratory fitness and upper body isometric and dynamic strength represent the functional aspects of sport climbing [17]. These influence blood pressure, a vital factor to be considered for the safe practice of this sport. With the Polar Ownindex, cardio-respiratory fitness can be evaluated at rest, relating anthropometric variables, age, gender and level of physical activity to measurements of heart rate and variability, obtained with a heart rate monitor. In spite of some criticism, the method has been recently validated by studies showing that the results are highly correlated with ‡O2max [6,7,13]. Sheel [17] showed that oxygen consumption by sport climbers was relatively low on trails classified as “easier”, suggesting that the contribution of aerobic capacity was not essential for the success at that level of difficulty. However, competitive climbers who were climbing at or near their maximum ability in trails classified as “harder”, e.g. levels 5.12a - 5.14c or 8a - 11b in the Brazilian system, ‡O2 was also higher, suggesting a significant contribution of aerobic metabolism. Those results point to possible adaptation, as suggested by Sheel [17]. Billat et al. [3], however, observed that the contribution of aero- bic metabolism depends more on the degree of perceived difficulty than on the actual one, which still seems to support the idea of functional adaptation. Climbers adapted to higher and more intense grades of difficulty tend to have improved functional performance, as expected for any other type of activity. Other factors, e.g. competition stress, weather conditions, interpersonal relations among the climbers, quality of equipment used etc., were not considered either in this study or in other literature reports. Table 2. Climbing rating scales used in different countries USA – 5.10a 5.10b 5.10c 5.10d 5.11a 5.11b 5.11c 5.11d 5.12a 5.12b 5.12c 5.12d 5.13a 5.13b 5.13c 5.13d 5.14a 5.14b Europe – 6a – 6b – 6c – 7a – 7b – 7c – 8a – 8b – 8c – Brazil 5c 6a 6b 6c 7a 7b 7c 8a 8b 8c 9a 9b 9c 10a 10b 10c 11a 11b 11c Standardised 0.75 1.00 1.25 1.50 1.75 2.00 2.25 2.50 2.75 3.00 3.25 3.50 3.75 4.00 4.25 4.50 4.75 5.00 5.25 The rating system of trails and climbers differs a little from country to country, but the ratings in relation to difficulty are alike. The systems used in the US, Europe and Brazil are presented in Table 2. It ought to be emphasised that rating scales were based on expert assessments and their validity was verified for an empirical internal stability only [9]. Generally, the following factors are being considered in those rating systems: type of climb, slope, type of hold, rest points, time needed to climb, physical difficulties, exposure risk (risk to fall and the severity of its consequences), manoeuvres and resources needed. The procedure to rate a new trail, a climbing that have never had been done, involves the assessment contributed by the first climber who completed it without a fall, and that assessment then has to be validated by other experts. The standardisation of 76 such a system, based on rating the difficulty of the climbing pattern, is not an easy task as it is subjective and factors like the physical and psycho-emotional fitness of the climber may affect the judgement [12]. The scale of self-rating climbing skills was identical with that used in external rating on a climb performed without falls on a not too difficult a trail. Female climbers had a considerably lower climbing experience than the male ones and that was associated with a significantly lower self-rating and cardio-respiratory fitness, the latter being similar to that reported by others [8,14,16]. The gender-related difference in climbing performance was associated with the strength of upper extremities; inasmuch no significant difference was found in the isometric strength, the female climbers had markedly lower dynamic strength and repetitive isometric contractions of the forearm musculature are known to increase blood pressure and oxygen consumption which, in turn, may represent a key factor in the performance of highlevel competitive climbers [12,16,21]. As the studied group was markedly non-homogenous, a reliable somatic and functional profile of sport climbers could not be established due to smaller than planned number of subjects but some conclusions and recommendations could be formulated. One of the key factors seems to be the cardio-respiratory fitness and dynamic strength of upper extremities. Other factors, like flexibility, co-ordination, balance and psycho-emotional features should be considered in future studies. References 1. American College of Sports Medicine. Guidelines for Exercise Testing and Prescription (1991) 4th ed., Williams & Wilkins, Baltimore. 2. Bertuzzi R.C.M. J.F.L.Gagliardi, E.Franchini, M.A.P.D. Kiss (2001) Características antropométricas e desempenho motor de escaladores esportivos brasileiros de elite e intermediários que praticam predominantemente a modalidade indoor. Rev.Bras.Ciênc.Mov. 9:7-12. 3. Billat V., P.Palleja, T.Charlaix, P.Rizzardo, N.Janel (1995) Energy specificity of rock climbing and aerobic capacity in competitive sport rock climbers. J.Sports Med.Phys.Fitness 35:20-24. 4. Boldori R (2002) Aptidão física e sua relação com a capacidade de trabalho dos bombeiros militares do estado de Santa Catarina. M.S. thesis, Post-Graduation Programme in Production Engineering, Universidade Federal de Santa Catarina, SC, Brazil. A. Padrenosso et al. 5. Conselho Nacional de Saúde (1996) Resolução 196 de 10 de outubro de 1996, dispondo sobre as diretrizes e normas regulamentadoras das pesquisas envolvendo seres humanos. Brazilian Health Ministry, Brasília, DF, Brazil. 6. Crouter S.E., C.Albright, D.R.Bassett Jr. (2004) Accuracy of polar S410 heart rate monitor to estimate energy cost of exercise. Med.Sci.Sports Exerc. 36:1433-1439. 7. Crumpton S., H.N.Williford, S.O'Mailia, M.S.Olson, L.E. Woolen (2003) Validity of the polar m52 heart rate monitor in predicting ‡O2max. Med.Sci.Sports Exerc. 35(Suppl.1):S193. 8. Dantas E. (2003) A Prática da Preparação Física. 5ª ed., Editora Shape, RJ. 9. Delignières, D. J.P.Famose, C.Thápaut-Mathieu, P.Fleurance (1993) A psychophysical study of difficulty rating in rock climbing. Int.J.Sport Psychol. 24:404-416. 10. FEMERJ - Federação de Esportes de Montanha do Estado do Rio de Janeiro, Rio de Janeiro (2000) Banco de dados. www.femerj.org/documentos%5Csistema_graduacao.pdf 11. Fernandes F.J. (2003) A Prática da Avaliação Física. Shape, RJ. 12. Graydon D., K.Hanson (1997) Mountaineering: the freedom at the hills (6th ed.) The Mountaineers, CA. 13. Godoy E.S.G., P.Barroso (1999) Manual de Avaliação Funcional do Projeto Esporte & Saúde. Secretaria de Ação Social Esportes e Lazer do Governo do Estado do Rio de Janeiro. 14. Heyward V.H. (1997) Advanced Fitness Assessment and Exercise Prescription. 3rd ed., Human Kinetics, Champaign, IL. 15. Laukkanen R (1999) Exercise and heart rate. Research and Development: Information about heart rate and exercise. www.polar.fi. 16. Mermier, C.M., J.M.Janot, D.L.Parker, J.G.Swan (2000) Physiological and anthropometric determinants of sport climbing performance. Br.J.Sports Med. 34:359-365. 17. Morrow, J.R.A.W.Jackson, J.G.Dish, D.P.Mood (2000) Measurement and Evaluation in Human Performance.2nd ed. Human Kinetics, Champaign, IL. 18. Nieman D.C. (1999) Exercício e Saúde. São Paulo. Editora Manole. 19. Pinto J.R. (1977) Cadernos de Biometria das FICAB. FICAB, RJ. 20. Pollock M., J.H.Wilmore (1993) Exercícios na saúde e na doença: avaliação e prescrição para prevenção e reabilitação. 2nd ed., MEDSI, RJ. 21. Sheel A.W. (2004) Physiology of sport rock climbing. Br.J.Sports Med. 38:355-359. 22. Shimakura, S. E. (2005) Coeficiente de Variação. Disponível em.www.est.ufpr.br/~silvia/CE055/node26.html.Acesso em 14 out. 2005. 23. Thomas, J.R., Nelson J.K. (1996) Research Methods in Physical Activity. Human Kinetics, Champaign, IL. 24. World Medical Organization. Declaration of Helsinki (1966) Br.Med.J. 313:1448-1449. Received 14.01.2008 Accepted 1.03.2008 © University of Physical Education, Warsaw, Poland
Baixar