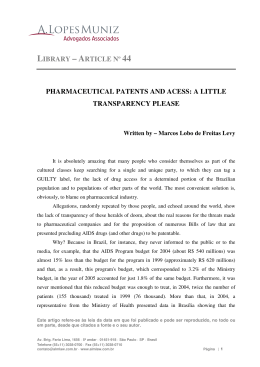
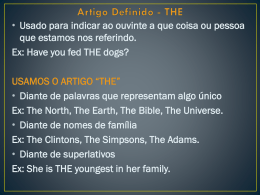
Microsporum gypseum infection in Aids patient: a case report | Anai... http://www.anaisdedermatologia.org.br/artigo_imprimir_en.php?arti... Volume 73 - Number 1 : Case Report Microsporum gypseum infection in Aids patient: a case report Infecção por Microsporum gypseum em paciente com aids: relato de caso Authorship Nurimar C. Fernandes Fabrício Lamy Tiyomi Akiti Maria da Glória C. Barreiros Abstract Report of a case of tinea corporis caused by Microsporum gypseum in a 36-year-old female Aids patient. The literature does not refer this dermatophyte as a common etiologic agent in this group of patients.The lesions were generalized,psoriasiform and refractory to treatment with ketoconazole and itraconazole. Keywords: Dermatomycoses; Microsporum; acquired immunodeficiency syndrome; tinea Resumo Relato de caso de tinea corporis por Microsporum gypseum em paciente com Aids de 36 anos. Segundo a literatura, este dermatófito não é um agente comum neste grupo de pacientes. As lesões eram psoriasiformes, generalizadas e não responderam ao tratamento com cetoconazol e itraconazol. Palavras-chave: Dermatomicose; Microsporum; síndrome de imunodeficiência adquirida; tinha INTRODUCTION In the human immunodeficency virus (HIV) infected patient, dermatophytosis usually manifests as tinea pedis or unguium and the prevalent dermatophyte is Trichophyton rubrum.1,2 Tinea pedis infection in HIV positive persons is similar in appearance to the disease in non HIV-infected persons. The incidence of dermatophytosis of the glabrous skin in HIV-positive patients is about 40%.3 Tinea cruris is frequent in any stage of HIV infection.4 The most common isolated dermatophytes are Trichophyton rubrum, Trichophyton mentographytes and Epidermophyton floccosum. 5,6 We report a patient with immunodeficiency syndrome (Aids) and extensive cutaneous fungal 1 of 5 6/5/08 12:41 PM Microsporum gypseum infection in Aids patient: a case report | Anai... http://www.anaisdedermatologia.org.br/artigo_imprimir_en.php?arti... infection due to Microsporum gypseum which failed to respond to the usual therapy. A 36 year-old white female, born in Rio de Janeiro and registered at Hospital Universitário Clementino Fraga Filho. HIV-positive since 1992, developed red scaling patches on the face and thorax, in november 1995. Direct microscopy of skin scales revealed dermatophyte hyphae; culture was negative. The clinical picture did not respond to ketoconazole (200mg daily for two months) and itraconazole (100mg daily for one month). The lesions spread slowly and in July 1996 they became generalized; they were erythematous, scaling, circinate, large, irregular and psoriasiform (Figure 1, 2). The skin scrapings did not reveal dermatophytes. Figure 1 - Large, irregular, scaling eruption on face and scalp Figure 2 - Generalized psoriasiform lesions on face and thorax The sample taken from biopsied lesion was mounted in KOH solution and cultured on Sabourand's agar.On direct examination, septated hyphae were found. 2 of 5 6/5/08 12:41 PM Microsporum gypseum infection in Aids patient: a case report | Anai... http://www.anaisdedermatologia.org.br/artigo_imprimir_en.php?arti... Microsporum gypseum was isolated on culture with the following specific features (Figure 3, 4): colonies with a flat, spreading powdery surface, cinnamon-buff to brown, scalloped and ragged edges. Microscopic morphology revealed septated hyphae and a great number of thin-walled and roughened macroconidia with 4 to 6 septa. Figure 3 - Colony with a flat, spreading, powdery surface Figure 4 - Microscopic morphology: septate byphae and macroconidia (400x) By this time a severe pneumonia was not controlled and the patient died. The prevalence of Microsporum gypseum in Rio de Janeiro makes clear that our patient is unusual not only for the psoriasiform eruption but also for the isolated dermatophyte ( Table 1). 3 of 5 6/5/08 12:41 PM Microsporum gypseum infection in Aids patient: a case report | Anai... http://www.anaisdedermatologia.org.br/artigo_imprimir_en.php?arti... DISCUSSION Table 1 - Prevalence os Microsporum gypseum in Rio de Janeiro Geophilic organisms are adapted for soil habitation. The fungi sporadically infect humans and when they do the resulting disease is usually inflammatory. Microsporum gypseum is the most common geophilic fungus isolated in human infections. Although soil isolates of Microsporum gypseum are of low virulence, strains cultured from humans are more virulent and account for epidemic spread of the infection under appropriate conditions.7 Human infection due to geophilic species often originates from infected animals; the infection by direct contact is not common.8 Microsporum gypseum causes tinea capitis and tinea corporis. Lesions are usually inflammatory, impetiginous and sometimes bullous with rapid development and resolution.8 Invasion of hair is of the ectothrix type and spores are sparsely arranged in chains. Microsporum gypseum produces suppuration, kerion and favus-like crusts on the scalp.8 The infection is common in South America. Penneys 9 described a HIV positive case with large plaques with silvery scales on the trunk: resembling psoriasis; Microsporum species were isolated. Bakos 10 described a favus like eruption on glabrous skin in a patient with Aids. Microsporum gypseum was isolated and the infection did not respond to oral ketoconazole. Seventy-one cases of human dermatophytoses caused by Microsporum gypseum were diagnosed in the hinterland of Rio Grande do Sul (Brazil) during 1960- 1990.11 An outbreak by Microsporum gypseum was described in Brazil 12 although the human infections are usually sporadic. REFERENCES 1. BergerTG. Treatment of bacterial fungal and parasitic infections in the HIV - infected host. Semin Dermatol 1993;12(4):296.300. 2. Conant MA. Fungal infections in AIDS and other inmunnocompromised patients. J Am Acad Dermatol 1994;31: S47-S50. 3. Elmets CA. Management of common superficial fungal infections in patients with AIDS. J Am Acad Dermatol 1994;31:S60-S3. 4. Petri V. Indicadores dermatológicos de redução da competência imune induzida pelo vírus da imunodeficência humana. In: Lacaz CS, Martins JCC, Martins EL, eds. AIDS SIDA. São Paulo: Sarvier, 1990;209-17. 4 of 5 6/5/08 12:41 PM Microsporum gypseum infection in Aids patient: a case report | Anai... http://www.anaisdedermatologia.org.br/artigo_imprimir_en.php?arti... 5. Terssander J, Karlsson A, Morfeldt Manson L. Putkonen PO, Wasserman J. Dermatophytosis and HIV infection. Acta Derm Venereol (Stockh) 1988:68:53-6. 6. Kaplan MH, Sadick N, Me Nutt S. Meltzer M. Sarngadharan MG. Pahwa S. Dermatologic findings and manifestations of acquired immunodeficiency syndrome. J Am Acad Dermatol 1987;16:485-506. 7. Rippon JW. Medical Mycology. Philadelphia: WB Saunders, 1974:108. 8. Kwon-Chung KJ. Bennett JE. Medical Mycology. Philadelphia: Lea & Febiger;l992;113:138. 9. Penneys NS. Skin manifestation of AIDS. London: Martin Dunitz, 1990:8-18. 10. Bakos L, Bonamigo RR. Pisani AC. Mariante JC, Mallman R. Scutular favus-like tinea cruris et pedis in a patient with AIDS. J Am Acad Dermatol 1996;34:1086-7. 11. Lopes JO, Alves SH, Benevenga JP. Dermatofitose humana por Microsporum gypseum no interior do Rio Grande do Sul: estudo clínico. An bras Dermatol 1992;67(2):71-2. 12. Severo LC. Conci LMA, Amaral AA. Microsporum gypseum - Relato de surto de infecção e isolamento do solo. An bras Dermatol 1984;64(2):119-20. 13. Wankc NCF, W ankc B. Prevalência de micoses superficiais em comunidade fechada do Estado da Guanabara. Rev Soc Bras bled Trop 1974;8(2):100-5. 14. Wanke NCF. Fraga S. O teste da tricofitina como subsídio diagnóstico nas dermatofitoses. An bras Dermatol 1977;52:7-24. 15. Towersey L. Contribuição ao estudo clínico-laboratorial e à epidemiologia da dermatofitose e afecções similes. Tese de Mestrado. Niterói: Universidade Federal Fluminense. 1987. 16. Wanke NCF, Wanke B, Gomes CLN, Perez MA. Demtatofitose e atópia. Med Cut ILA 1988;16:373-5. 17. Costa EF. Micoses superficiais e cutâneas. Estudo comparativo entre duas populações- Rio de Janeiro e Aracaju. Tese de Mestrado. Rio de Janeiro: Instituto de Microbiologia, UFRJ. 1989. 18. Wanke NCF, Monteiro PCF, Wanke B. Nogueira CM. Perez MA. Dermatofitoses no Rio de Janeiro. Estudo dos fatores de risco em população adulta. An bras Dermatol 1991;66(4):171-4. 19. Wanke NCF, Avé BR. Wankc B, et al. Fungal infections in the feet of diabetic patients. J Mycol Méd 1992;2:144-7. 20. Fernandes NC, Monteiro PCf, Perez MA. Dermatophytosis in children: risk factors study. J Mycol Med 1995;5:188-9. MAILING ADDRESS Nurimar C. Fernandes Rua Alexandre de Gusmão 28/201 Rio de Janeiro RJ 20520-120 An bras Dermatol. Rio de Janeiro. 73(1):39-41.jan/fev.1998. 5 of 5 6/5/08 12:41 PM
Baixar