r{
n\
The Use of Fibrin TissueAdhesive
to ReduceBlood Lossandthe Need for
Blood TlansfusionAfter Total Knee Arthroplasty
RnNnol\4lzeo,MulrtceNtsR Sluov*
A PRosPECTtve,
M'D'I' ARIEL ORAN' M'D'T' TEL HASHOMER'
BY OFER LEVY, M.D.I, BEER.SHEVA' URI MARTINOWITZ'
HOROSZOWSKI' M'D'#' TEL HASHOMER' ISRAEL
CFIANAN TAUBER, M.D.$, REFIOVOT, AND I'IENRI
lJniversity of the Negev' Beer-Sheva;
Investigation perlorrnecl at soroka Meclical center, Ben-Gttrion
ShebaMetlicalCenter,TelHushomer;andKaplanMedicalCenter,Rehovot
Abstract
Background:Total knee arthroplastyis associated
with major postoperativeblood loss of approximately
fre'
800 to iZOO mifnliters, and blood transfusion is
the
about
quentlyrequired.With the increasedconcern
blood
of
.ist s of blood transfusion,various methods
conservationin orthopaedicsurgeryhavebeenstudied'
The most appropriatesolution, however,is to reduce
the loss of nlood during and after an operation'The
presentprospective,controlled,randomizedstudy was
i"sign"d to evaluatethe hemostaticefficacyof the use
of fif,rin tissueadhesivein patients managedwith total
knee arthroPlastY.
Methods: Fifty'eight patients who were scheduled
to have a total knee arthroplasty were randomly di'
vided into two groups:a control group' in which the
standard -uunt of hemostasiswere applied, and a
treatment group' in which the standardmeansto con'
trol local ntu"aing were applied and a fibrin tissue
adhesivewas sprayedon the internal aspectsof the
operativefield beforeskin closure'All operationswere
performedin a bloodlessfield with useof a pneumatic
iourniquet.All patientsreceivedlow'molecular'weight
heparin as thromboprophylaxistwelve hours before
the operation and every twelve hours postoperatively'
Blood lossduring the operationwasevaluatedby measuring the volume in the suction apparatusand by
estimatingthe amount of lost blood in the swabsat the
end of the operation.The apparentpostoperativelost
+Oneor moreof the authorshasreceivedor will receivebenepartyrelated
usefrom a commercial
fits foipersonalor professional
beneJlt".tiy'o, inclirectlyto the subjectof this article ln aclclition'
fiis have been or will be direitecl to a researchfund' founclation'
with which
institution,or other nonprofitorganization
eclucational
recelvedln
were
funds
No
is
associatecl'
authors
the
of
one or more
of this stttdY.
-support
"iO"pn.t.ent
Hospiof OrthopaedicSurgery,Royal-Berkshire
tal, Loion Roacl,ReaclingRCt SRN, United Kingdom'E-mail
way.co'uk'
[email protected]
address:
of OrtNationalitaemophiliaCentre(U M') and Department
Surgery(A. O.), ShebaMeclicalCenter'Tel Hashomer
thopaeclic
52621,Israel.
Surgery,KaplanMedicalCentre'
!ibepartmentof Orthopaeclic
P.O.Box 1.Rehovot76100'Israel.
#Deceased.
t
1580
blood was determined by measuring the volume in
the suction-drainbottles. Alt blood transfusionswere
recorded.
Resu/ts;The mean apparentpostoperativeblood loss
(and standard deviation) in the fibrin'tissue'adhesive
group was 360 ! 287.7millititers compared with 878 t
iOf.d mnnnters in the control groupr with a mean dif'
ferenceof 518millititers (p < 0.001).The decreasein the
level of hemoglobin was 25 t 1'0grams per liter in the
treatment group compared with 37 + 12 grams per liter
in the conirol group (p < 0.001). Sixteen patients (55
percent) in the iontrol group required a blood transfu'
sion and eight (28 percent) required two units of blood'
whereas only five (1,7 percent) of the patients in the
fibrin-tissue-adhesivegroup required a blood transfu'
=
sion and only one (3 percent) required two units (p
0.004).The number of adverseevents was comparable
between the two groups. None of the adverse events
were consideredto be related to the use of fibrin tissue
adhesive.One death, which was due to massivepulmo'
nary embolism' was reported in the control group' No
seroconversionwas reported at three and six months
after the oPeration.
Conclision: The use of fibrin tissue adhesive in
total knee arthroplasty seemsto be an effective and
safemeanswith which to reduceblood lossand blood'
transfusionrequirements.Furthermore,the importance
of thesefindings was enhancedby a significantreduc'
tion in blood loss,in the postoperativedecreasein the
level of hemoglobin,and in blood'transfusionrequire'
ments despite preoperative thromboprophylaxiswith
low-molecular-weightheParin.
Total knee arthroplastyis associatedwith major
postoperativeblood loss, which is usually underestitransfusion'Although the
mated ancloften necessitates
use of a tourniquet during the procedure may reduce
the intraoperativebloocl loss,the postoperativeblood
loss,asdeterminedby measuringthe amount of suction
clrainageand as calculatedon the basisof the decrease
Blood
in the ievel of hemoglobin,can be considerable'
to
Iossafter total knee arthroplastyoften amounts 800
to 1200milliliters, ancl blood transfusionis frequently
requireds
15'4756'
re15
TFIE JOURNAL OF BONE AND JOINT SURGERY
tral
eas
atil
re2
me
At
dil
bl(
ES
p(
m
sir
ol
t(
fl
c
f
(
I
I
1581
FIBRINTISSUEADHESIVEToREDUCEBLooDLOSSANDTHENEEDFoRBLooDTRANSFUSION
United States".Fibrin tissue adhesiveis comwith the increasedconcernabout the risks of blood in the
posedof two main components:fibrinogenand thromtransfusion,which include the transmissionof viral disof
hep- tin. wtr"n mixed together,they mimic the last step
suchasthe humanimmunodeficiencyviruso,,
eases,
fibrinogen
activates
thrombin
as well as transfusion the coagulationcascade:
and cytomegalovirus'r5'''?,
atitis2633,
clot, and factor XIII, which
unstable
an
to
polyrierize
to
new
for
reactions,there has been a co'stant search
is present in the fibrinogen concentrateand is actimethodsof blood conservationin orthopaedicsurgery.
vafed by thrombin (factor XIIIa)' stabilizesthe clot by
Among the various methods are perioperativehJmocross-linking-betweenthe fibrin molecules'
dilutiono,,intraoperativeand postoperativesalvageof catalyzing
an- Factor XiIIa also cross-linksbetween natural plasmin
of hypotensiv"e
blood and reinfusion'rzttt.u.u,theuse
(which co-purifywith fibrinogen)and the fiesthesiaor epidural anesthesia,and the transfusionof inhibitors
againstfibriHOWeVer,a brinOgenmashto enhanceclot resistance
predonatedautologous61oo6r,n.,z.*.,..3?38.s8.62.
norysii. Some products contain additional fibrinolytic
more rational approachwould be to enhancehemostainhibitors,suchasbovineaprotininor tranexamicacido"
sis and sealingof vesselsat the site of the op"rutron rn
althoughthe contribution of such additivesis controorder to prevenror reducebrood loss.
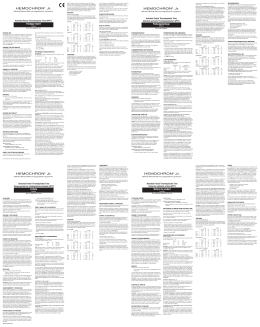
Theuseofplasmaproteinsatthesiteoftheinjuryversial(Fig.1).
Despiie numerouspublicationson the use of fibrin
to reduceblood lossdatesback to the beginningof thl
tissueaihesive in a[ fields of surgery,evidencefrom
century,when Bergel.useddry plasmaand Gre!" used
controlledtrials on the efficacyof fibrin tissueadhesive
fibrin patchesduring operations.The modein concept
also known as is lacking'Most reportslav.ebeen descriptj* 119,1-"
of treatmentwith fibrin tissueadhesives,
Recentexperrmenconsistsof the application beenbasedon uncontrolledstudies.
fibrin gluesor fibrin sealants,
that there is no
suggested
have
triars
clinical
tar and
of plasma fibrinogen mixed with thrombrn io ro.- a
of
benefit in the use of fibrin tissueadhesivefor some
fibrin clot adhesive,and it was first ,"por,"d, to our
or that there may evenbe a harmthe indications32.44.4e.54
knowledge,by cronkite et ar.,oduring world war II.
ful effect&'e.
commer-cialfibrin tissue adhesivebecame available in
we designedthe present prospective'controlled,
extensively
used
been
has
and
Europe in the late 1970s
ral-domizedituay to evaluate the hemostatic efficacy
since then for various indications,including hemostasis,
a
of fibrin tissueadhesivein patients who were having
sealing,and gluing, and as a vehicle for Jhemical and
preoperamanaged
were
and
total knee arthroplasty
biological materials{.Becausethere is a lack of solid
tively with low-molecuiar-weightheparin asprophylaxis
commost
efficacy,
and
evidenceconcerningtheir safety
againstdeep-veinthrombosis'
mercially available fibrin tissue adhesivessiill have not
Methods
and
Materiars
f:il""irffi,?iT":'"::,ti:.3fffilTf$3:::
which are much ress
Thepresentinvestigationwasamurticenter,prospecbovine thrombin concentrates,
study'
randomized,standard-treatment-controlled
tive,
extensively
used
safethan the commercialproducts,are
EllrinsigColgulatignglscrqe
(Wound)
fissuethromboplastin
IntrinsicC3g!g!!gn rQg3!9
EAiormu
o"tiuotion
*,,-L*,rr"
+
11 -#Xta
I
I
,* t
v
vrrr
vllla----|\
vIn*
vrrg
,*,
t t*'
\
\fu/
,*
---1g
vtl
/
/
Xa
v
I
Va
FulCo.nloirrlttt Q
Prothrombin
FIA-Conpoaent !
vtlthtddirton o{
$ataexnfrueocid
,tiilotto*u"'
,$rrbttbtdlr"
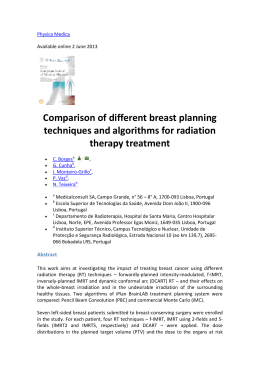
Clotformation b1t
the physiological
coagulalion
cascade as well as
Fibrin Polymer II (Cross-linked)
Ftc. 1
adhesive (FTA)'
the composition of the components of the fiblin tissue
Schernatic drawrng of the coagulation cascade and
VOL. 81-A, NO. 11, NOVEMBER 1999
1582
OFER LEVY ET AL.
TABLE I
Data oN rue Petteuts
All of the operationswere performedin a bloodless
field with use of a pneumatic tourniquet.The tourniquet was deflated after the preparationof the femur
Fibrin-TissueAdhesiveGroup
ControlGroup
and the tibia and before insertion of the prosthesisin
(N = 2e)
(N = 2e)
order to obtain hemostasisby electrocauteryof the maAge* (yrs.)
68.9+ 6.3
70.2+ 8.2
jor vessels.
Then the tourniquet cuff was inflated again,
(60-82)
(47-83)
prosthesiswas insertedwith cement.In all
before
the
Gender(F/M)
23t6
zato
patients,
of
the
the drill-hole in the femoral canal was
Mean height(crn)
160.4
t62.7
plugged
pluggingthe guide-holein the femoral
because
Mean weight (kg)
76.7
76.9
canal during knee arthroplasty has been reported to
*The values are given as the mean and the standard deviation, with
reduceblood lossso.
the range in parentheses.
After the prosthesishad been insertedwith cement
and beforeclosureof the soft tissues,
the kneejoint and
It wasapprovedby the ethicscommitteeat eachmedical the entire operativefield was thoroughlyrinsed of any
centerand by the Ministry of Health.All patientsgave debrisand was meticulouslydried.The fibrin tissueadinformedconsent.
hesive(ten to twenty milliliters of combinedproduct or
Fifty-eight patients who had osteoarthritisof the one or two kits) was then applied by topical spraying
knee and werescheduledto havea unilateraltotal knee with useof a double-syringespray-device.
The glue was
arthroplastywith cement were enrolled in the study. sprayedover the tissues,into the joint itself,on the raw
There were forty-six women and twelve men.Twenty- surfacesof the bones,on the musclesand tendons,and
nine patients w'ere randomized to receive treatment around and on the subcutaneoustissueswhile all of the
with fibrin tissueadhesive(the treatmentgroup),and so-calledhidden pouchesof the joint were exposedin
twenty-ninewere randomizedto be managedwith the order to cover as much surfacearea as possiblewith a
standardmethod of hemostasis(the control group).
film of glue. Drains were used in the joint and were
All implantswere of the posteriorcruciate-sparing connectedto a high-vacuum-suction-drain
bottle. The
type,and all were insertedwith cement.
kneejoint wasthen closedin layers.Thesestagesof the
The randomizationwasdeterminedaccordingto pa- procedurewere identicalfor both groups,exceptfor the
tient number,whichhad beenassigned
with a computer- applicationof the fibrin tissueadhesive.
generatedrandomizationlist. The randomizationwas
The operationswere performed by eight different
centralized,and the study monitor informed the sur- surgeonsin three medical centers.All of the surgeons
geon of the patient'sallocatedtreatmentgroup during performedoperationswith and without the fibrin tissue
the operation,just before the applicationof the glue, adhesivein patientsincludedin the presentstudy.
if the patient was in the fibrin-tissue-adhesive
group.
The AGC total knee prosthesis(Biomet, Warsaw,
This procedure was used to eliminate the possibility Indiana) was used in twenty-one patients (eleven in
of bias,as the surgeonmight have deviatedfrom stan- the control group and ten in the treatmentgroup);the
dard hemostatictechniquesand practicesas a result of press-fitcondylar total knee prosthesis(PFC; Johnson
awarenessof the patient'sstudy cohort.The fibrin tis- and JohnsonOrthopaedics,Raynham,Massachusetts),
sue adhesiveusedin the presentstudy wasoctacolF15 in five patients(two in the control group and three in
(Quixil; Omrix Biopharmaceuticals
SA, Nes-Ziona,Is- the treatment group); the Insall-BursteinII (Zimmer,
rael). It consistsof a cryoprecipitate-based
fibrinogen Warsaw,Indiana),in twenty-eightpatients(fourteen
at a concentrationof fifty milligramsper milliliter and in each group); the Rotoglide total knee prosthesis
a high concentrationof humanthrombin (1000interna- (Corin Medical, Cirencester,Gloucestershire,
United
tionalunitsper milliliter)dissolved
in a solutionof forty Kingdom),in two patients(one in eachgroup);and the
millimolesof calciumchlorideper liter. An antifibri- Howmedicatotal kneeprosthesis
(Howmedica,
Ruthernolytic agent,tranexamicacid (ninety-five milligrams ford, New Jersey),in two patients(one in each group).
per milliliter), is addedto the fibrinogenas a stabilizer. The two study groups were comparablewith respect
Both componentsundergo double viral-inactivation to all other parameters,
suchas age,gender,height,and
steps:treatmentwith solventdetergentfollowedby pas- weight(TableI).
teurization(at 60 degreesCelsiusfor ten hours)for the
Hemoglobin and hematocrit values were deterfibrinogenand nanofiltrationfor the thrombin.
mined preoperativelyand on the first, second,third,
fifth, and seventhpostoperativedays.The preoperative
OperativeProcedure
plateletcount,prothrombintime,and activatedpartial
In order to control the variablefactors,all of the thromboplastintime were determinedfor all patients.
surgeonsdiscussedand agreedon the operativeproto- The prothrombin time and the activatedpartial thromcol and the sequenceof the operativeproceduresbefore boplastin time also were evaluatedimmediately after
the study and they performedall of the operationsin a the applicationof the glue.The lossof blood at the end
uniform manner.
of the operationwasrecordedby measuringthe volume
THE JOURNAL OF BONE AND JOINT SURGERY
FOR BLOOD TRANSFUSION
BLOOD LOSS AND THE NEED
FIBRIN TISSUE ADHESIVE TO REDUCE
1583
the amount the supervisionof a physiotherapist'
assessed
in the suctionapparatusand by estimating
Ttre satetyof thafibrin tissueadhesivewas
porilf"ruriu"
laboratory
of rost brood in the swabs.The apparen,
and
signs,
vital
events,
volumein the by monitoringadverse
blood losswasrecordedby measuringthe
SerJlogicaltestsfor the human immunodefithat fina119-s
however,
suction-drainbottles.It ii well known,
andthe hepatitis-B'c' and
cjen.cyvirus,cytJmegalovirus,
postoperainapparent
of
amount
substantial
there is a
and were reor ,n" A virusesweie perfotmedpreoperatively
extravasaiion
by
caused
is
which
loss,
tive blood
months postoperativelyto en""u"uur"o uv peated at three and six
brood into the tissuesand thereforeis not
had occurred'
no serocol'lversion
Thus,total Ulooa,tosswas also iure that
the suctiondrainage"3n.
this study with regard
Th";;il"y9nd^.Po:"l.of adhesivewasa reduccatcutatedwitli a formuia,desiiibeil5y Cfaltt;liiaf'
tissue
ritrin
j, .t a r-,";;to the "fii.u"y or trre
of
usbsthe maximumposiopeialivedecibase
u:L^tl blood loss' as determinedby measurement
"iif'"
rteigitt
"ta rr
*"igf,t
wcttsIrtdr:u
' tt
use
after
globin value adjust"d-i;;irt"
percent
30
least
at
of
postoperativebleeding,
patient.
with that in the
]"^"
bt tt " fibrin tissueadhesivecompared
crinicar
a
Determining the need for transfusionis
with statistical
chosen
was
lteattt, con- "ont,ot g,oup.This criterion
were the
challenge.In 1988'tr'eNationalInstitutesoi
parameters
efficacy
Secondary
oi.ea consiaeiations.
and hesensusconference""on perioperativetransfusion
hemoglobin
the
in
criteria -ugrrit,rJ" of the reduction
requireblood ce's addressedttris issueand established
brood-transfusion
in
as
the need for matocrit reuersas weil
and guidelinesfor trre determination of
of hematoma'
the basisfor mentsand the development
blood replacement.These guidelinesare
patientand the range
ofthe
The functionalrecovery
at our
examinations'
the regurarpractice"on""rrlng ulood transiusion
foilo*-up
th"
ui
in ou, ,tuay ot rnotron*"re recorded
medicarcenters,and they were follow"a
to the applias well. As the surgeoncannotbe blinded
StatisticalMethods
d""i.;:;;J";;rhe
adhesive,
cation of fibrin tissue
ingpostoperativeutooa-transfusionr"qulr"rn"ntscouldDemographicdataandotherbaselineparameters
statistically check the comparability
-'#
bias,the sur- *"r" ""itire'd
.to
also
have been biased.In order to preventthis
study groups.statistical analyseswere
tir"
of
""nt"rr)ugr""a
three
(at
all
Safety
geonsinvorvedin this study
parameters'
p"rtor-"J on the iafety and efficacy
i"{"ir"that the decisionsregarding brood-transfusi."
by comparingthe two groupswith respect
and not was assessed
ments would be made by a team of surgeons
events and the outcome
*-unr of sur- to the frequency of adverse
by the operating surgeonalone.The .u-"
hematoma'and deeprrion comptications(wound infections'
was evalgeonsmade the deciiions concerningutooo-irunrt
u"in-tttto*uosis) after the operation' Efficacy
control group
the conrror
th me
tt":u '*Jrhe treatdifferences
requirements for both
the
of
uated bj Jetermining the.significance
menr group.
after the treatbetweenthe resultsfor the two groups
The team decisionwas basedon the recommendawere usedfor descripconsensus ment perioo.Graphicalmethods
Health
of
Institutes
Nationar
the
of
tions
of normality'The
tive piesentationand for assessment
ctinic;r
good
on
iuJg*"nt.
and
lggg
in
conferenceou
as the nonparametricMannbasis of the ,*o-ru*pi" t test as well
the
on
prescribed
was
transfusion
the two groups'
Each
whitneyu test were ut"q.Jo compare
,h" d".r"u.,
status,
present
the
history,
cardiovascular
w'coxon signed-ranktestwere
ioss,and the Thepaiied t testandthe
blood
"'":'
of
severity
severrtt
ihe
tne
I'
level,
in hemoglobin
of changeswithin the groups'
used for the assessment
patient.
the
age of
for comparisonof
:'
of Analysisof covariancewas applied
formation
the
such^as
complications,
wound
Any
to adjust the postwound or the groupswhen it rilas necessary
ttre
from
drainage
prolonged
a hematoma,
levelsof the same
infection treatmenileversto the pretreatment
of
signs
any
and
dehiscence,
wound
tests for
drain site,
putu."i"tr. For the qualitative parameters,
recorded.
were
hearing,
or delayed
chi-squarestatis"onti,,ge,,"ytables,,u"h u. Pearson
injection
a
subcutaneous
received
patients
All of the
A two-tailedp
tics ani Fisher'sexacttest'were applied'
n"purin
low-mot""rrtur-*"igrrt
a
of
of forty milrigrams
to be significantfor
twelve valueof 0.05or lesswasconsidered
thromboprop'yil"is
as
(enoxaparin[clexane])
to re- all analysesperformed'
hours before trre of"iation, and they cbniinued
hours'
twelve
Results
feive thirty milligramsof enoxaparinevery
andcontinuing
*r;ru***:#ffiii:fnerativelY
werecomparable
andcontrol
sroups
rhetreatment
(TableI)'
of the patients
in terris of the characteristics
Doppler ultrasound'studies(duplex ultrasonograwassimilar for the two
loss
blood
The intraoperative
limbi1or
phy) were p"rtor*"J to examine tt," fo*"i
":H;
h:r,;,"*;*fn';"1"|;:i,Hil:,J,il",1JiT.ff[
werea'owed to get out of bed on the
The patients
"rJprry.i"secondday afterthe operativ"pro""aur"i
*"r"
p"ii"rri,
rrr"
a"v.
therapywasstarteJo'it".u-"
il;;
tJrJriiJi,
u,
exercis",
and
encouragedto walk
vol.
81-A, NO. 11, NOVEMBER 1999
(and
ross
brood
p^osroperative
apparent
mean
in the
*"na"to-a"uiutio't; was 360x zg'1.7'rilliliters
with 878t 403'0
groupcompared
fibrin-tissue-adhesive
of 518
difference
The
gio,rp.
mittititersin the contiol
2)'
(Fig'
<
0'001)
(p
*iniil,"t. wassignificant
1584
OFER LEVY ET AL
@
2000
1800
1600
1400
1200
1000
800
600
400
200
0
FTA Group
Control
(p < 0.001)
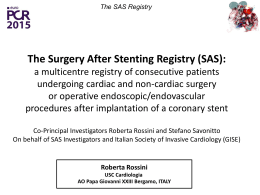
Frc. 2
(FTA)groups.
andcalculated2s
bloodlossin thecontrolandfibrin-tissue-adhesive
theapparent
Graphshowing
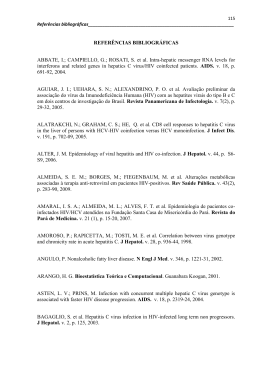
The mean decrease(and standarddeviation)in hemoglobinconcentrationafter the operationwas25 + 10
group comgramsper liter in the fibrin-tissue-adhesive
pared with 37 ! 12 gramsper liter in the control group,
suggestinga larger blood loss than was demonstrated
by the volume of drainedblood. The differencein the
hemoglobinvaluesbetweenthe two groupswas found
to be significant(p < 0.001)(Fig.3).
The calculatedblood loss^wasgreaterthan the observedloss in both groups,but it was found to be significantly lower in the fibrin-tissue-adhesivegroup
(1063.0t 481.95milliliters) than in the control group
(1768.0t 61.4.60
milliliters) (p < 0.001)(Fig.2).
The blood-transfusion requirements in the fibrintissue-adhesivegroup also were found to be significantly lower than thosein the control group.Only five
group
patients(17 percent)in the fibrin-tissue-adhesive
required a blood transfusionand only one (3 percent)
required two units of blood, whereassixteen patients
(55percent)in the control grouprequireda blood transfusion and eight (28 percent) required two units (p =
0.004)(Fig.a).
AdverseEvents
The frequency of adverseeventswas comparable
between the two groups:twenty-sixpatients (90 pergroup and twentycent) in the fibrin-tissue-adhesive
seven(93 percent)in the control group had an adverse
event.There were fifty-two adverseeventsin the fibringroup, and thirty-nine (75 percent) of
tissue-adhesive
these eventswere consideredmild. There were fortynine adverseevents in the control group, and thirtythree(67percent)of theseeventswereconsideredmild.
Fever was the most common adverseevent associated
with the operation,with no differencein frequencybetween the two groups (twenty-threepatients [79 per-
40
35
30
I
r:
u
)<
€ 2 0
OI
u l s
t0
FTA Group
(p < 0.001)
Control
Frc. 3
Graph showing the postoperative decreasein the hemoglobin levels in the control and fibrin-tissue-adhesive(FIA)
groups.
THE JOURNAL OF BONE AND JOINT SURGERY
FOR BLOOD TRANSFUSION
FIBRIN TISSUE ADHESIVE TO REDUCE BLOOD LOSS AND THE NEED
1585
No. of patients
9
I Unit of Blood
2 Units of Blood
(p < 0'001)
Flc. 4
(FTA) groups'
Graph showingthe blood-transfusionrequirementsin the control and fibrin-tissue-adhesive
cent] in the treatmentgroup and twenty-four [83 percentl in the control group). Qgpgt!igt"l-.99!gg&9qqlt
was suspectedin two patients (7 percent) in the fibrincrlg p€tiqul (3 percent)
tissue-adhesivegroup al{jl
-ii thc-.=cpntplgroup AII of these infections were controlled with antibiotic treatment'
Two patients in the fibrin-tissue-adhesivegroup had
clinical iigns of deep-veinthrombosis,with negative
findings on Doppler ultrasound scans,and one patient
in the control group died of massivepulmonary embolism three weeksafter the operation.
None of the adverseeventswere consideredto be
related to the study treatment.With the numbersavailable,no significant differencewas detectedbetweenthe
groups with respectto the postoperativerange of motion or the progressof the rehabilitation.
for viruseswas reportedat three
No seroconversion
and six months after the operation.
Discussion
The amount of blood lossafter a total knee arthroas was shown in the
plasty is usually underestimated3"
presentstudy by the differencesbetweenthe apparent
and the calculatedsblood loss.
The volumesof blood lossand the need for transfusion in the control group in our series were similar to
the data reported in previousstudieson blood loss ass'te':o'rs':oas'eo'
sociated with total knee arthroplastyz':
A significant reduction was detected in both the
apparent and the calculatedtotal blood loss resulting
fiom total knee arthroplasty in the group treated with
fibrin tissueadhesivecomparedwith those valuesin the
control group (p < 0.001).The treatmentgroup had a far
smallerpostoperativedecreasein the hemoglobinlevel
VOL. 81.A. NO. 11, NOVEMBER 1999
than the control group, and the difference was significant (p < 0.001).Theseeffectsmay play a beneficial role
in the achievementof early and better postoperative
rehabilitationro.
The resultsof our study suggestthat the useof fibrin
tissue adhesivein total knee arthroplasty reduces the
postoperativeextravasationof blood into the tissuesas
well as the apparentblood loss,thereby preventing the
formation of hematoma.Theoretically,this may reduce
the rate of infection and promote healing. Our results
are supported by the findings of Marmor et al'3e,who
demonstratedthat fibrinogen concentratesreduce the
inapparentblood loss;however,in our study,the apparerrt blood losswas found to be significantlyreduced
as well (p < 0.001).
The use of fibrin tissue adhesivewas found to significantly reduce the total number of units of blood
transfusedpostoperativelyto one-fourth of that in the
control group (six compared with twenty-four units of
blood;p < 0.001).It also significantlyreducedthe number of patients requiring blood transfusion (five compared with sixteen;p = 0.004)'In addition, only one
patient in the treatment group received two units of
blood comparedwith eightpatientsin the control group'
Total knee arthroplastyis associatedwith a high risk
Most deep-vein
of postoperativethromboembolism"222niu.
the operaduring
formed
to
be
thought
thiombosesare
thromboprophypreoperative
tive procedure;therefore,
laxis with low-molecular-weightheparin is superior to
It is a well
postoperativethromboprophylaxisalone22''n'02'
the
United
outside
countries
accepiedpracticein most
preoperatively'
Statesto usethromboprophylaxis
Hull et al." showedthat preoperativeadministration
of low-molecular-weightheparin before a total hip re-
1586
OFER LEVY ET AL
placementreducesthe rate of deep-veinthrombosis having a total knee arthroplasty.The fact that the fibrinby approximately50 percentcomparedwith postopera- tissue-adhesive
group in our study had a significant
tive thromboprophylaxisonly. In their study,8.8 per- reduction in blood loss and blood-transfusionrequirecent (forty-four) of 499patientswho had beenmanaged mentsafter total knee arthroplastycomparedwith that
preoperativelywith low-molecular-weight
heparinwere in the control group (p < 0.001) despite preoperafound to havedeep-veinthrombosison bilateralvenog- tive thromboprophylaxiswith forty milligrams of lowraphy performedpostoperatively,
whereas15.6percent molecular-weightheparin enhancesthe importance of
(102) of 652 patientswho had receivedonly postop- thesefindings.
erativethromboprophylaxiswith low-molecular-weight
The use of the fibrin tissueadhesivewas found to
heparinhad deep-veinthrombosispostoperatively(p < significantly reduce the apparent blood loss, the de0.001).Similarresultshavebeenreportedfor total knee creasein the level of hemoglobin,the total calculated
replacements'0.
blood loss,and the blood-transfusionrequirements(p <
Total knee arthroplastyis associatedwith major 0.001for all) (Figs.1,2, and 3).
postoperativebleeding.Furthermore,there have been
The preventionof blood loss,includingthe prevenconcerns that preoperativethromboprophylaxiswith tion of concomitantcompartmentalshiftsin body fluid,
low-molecular-weightheparin may substantiallyin- is definitelysuperiorto the replacementof blood lossto.
creasepostoperativebleedingand bleedingcomplica- It is much safer for a patient to receive a multidonor
tions as well as increasethe need for postoperative viral-inactivatedblood product (fibrin tissueadhesive)
blood transfusions":s.
than to receivehomologousblood that cannot be viralThe intraoperativeblood loss associatedwith total inactivateda.The effectiveness
of the fibrin tissueadheknee arthroplastydoesnot imposea substantialprob- sive in reducing blood loss may be explained by its
lem, as most of theseproceduresare performed in a ability to sealand plug the bone-marrowsinusoidsand
bloodlessfield obtainedwith use of a pneumatictour- consequentlyto prevent oozingof blood.Furthermore,
niquet. The bulk of the blood loss occurs after the as extravasationof the fibrinolytic agentsfrom the cut
operationat30''5.
There are severalexplanationsfor post- edgesof tissues(bone and soft tissues)is prevented,
operative bleeding associatedwith total knee arthro- fibrin tissueadhesivemay suppressthe enhancedfibriplasty.After any operation,the fibrinolytic systemis nolytic state.
transientlyactivateds2,
and this phenomenonis greater
The very high concentrationof thrombin in the parafter osteotomyu.
The useof a tourniquetalsomay con- ticular preparationof fibrin tissueadhesiveusedin the
tribute to the considerablepostoperativebleedingbe- presentstudy createsa fibrin tissueadhesivethat clots
causereactive hyperemiamay develop secondaryto very fast. In this preparation,the fibrin clot is already
prolongedischemiain the limb, with an increasein the created at the aerosol state and therefore immediate
fibrinolytic activity after releaseof the arterial tour- hemostasis
is inducedwhen it arriveson the tissues.
This
niquet2'.In severalstudies,continuousbleeding from featurepreventsextravasationof fibrinolytic agentsand
venoussinusesof the cut cancellousbone45.6r
wasimpli- polymorphonuclearcellsfrom the edgesof the cut bone
cated as the major sourceof blood loss.Someauthors and tissueand hencemay reducethe inflammatory rehaveshownthat bleedingmay be potentiatedby suction action at the operative site. A high concentrationof
drainage5r.
thrombin createsa fine fibrin network with small pores,
Surgeonshave a conflict betweenthe need to pro- which act as a mechanicalbarrier for polymorphoro\.
vide optimum thromboprophylaxis(preoperatively) clear cells and reduce inflammation and adhesio6.$ll)
and the need to addressthe high risk of bleeding.In The addition of tranexamicacid to the fibrin tissueadthe United States,the current recommendedpractice hesiveas a fibrinolytic inhibitor may play an additive
for the administrationof low-molecular-weight
heparin role in the stability of the gluex3q4r.
to prevent deep-veinthrombosisis to start thromIn conclusion,we found that the useof fibrin tissue
boprophylaxistwelve hours postoperatively,with no adhesiveis an efficient means with which to reduce
preoperative thromboprophylaxis.The present study blood loss and blood-transfusionrequirementsin pashowedthat the useof fibrin tissueadhesivemay allow tientshavinga total kneearthroplasty
who are managed
the use of full-dosepreoperativethromboprophylaxis preoperativelywith low-molecular-weight
heparin.
with low-molecular-weightheparin, thereby reducing
No rr: The authors gratefully acknowledge the assistanceof Dr. N. Liberman, Dr. M. Salai,
Dr. A. Vindzberg, Dr. A. Chechik, and Dr. E. Shoshani in the
the risk of deep-veinthrombosiswithout increasing Dr. A. lsraeli, D.. Y. Amit,
'fhe
completion of this study.
authors dedicate this paper to the mcmory of their triend, teilcher,
the risk of postoperativebleedingin patientswho are and colleague, the late Protessor Flenri Lloroszowski, who could not see his work comDleted.
References
Amrani, D. L.; DiOrio' J. P.;Delmotte,Y.; Krack, G. F.; and White, R.: In vitro characterizationand structuralbasisfor in vivo efficacy
of fibrin sealantin preventingformationof surgicaladhesionsIabstract].Thromb.and tlcemost.,OC-790Sr-rpplement,
June 1997.
Benoni, G., and Fredin,H.: Fibrinolytic inhibition with tranexamicacid reducesblood loss and blood transfusionafter knee arthroplasty.A prospective,
randomised,
double-blindstudyof 86 patients.,/.Bone und Joint Surg.,78-B(3):434-440,1996.
THE JOURNAL OF BONE AND JOINT SURGERY
LOSSAND THE NEED FOR BLOOD TRANSFUSION
FIBRIN TISSUEADHESIVETO REDUCE BLOOD
1'587
replacement']Ilare.fual't'131:462-464'536'1996'
3. Berenfcld,B.; Kligman,M.; and Roffman,M.: [Total knee
4.Bergel,S.:UberWirkungendesFibrins'Deutschcnted'Wochenschr''35]l633'19O9'
1988.
losswith total knee arlhroplasty.CI,in.orthop.,234:137.138.
5. Berrnan'A. T.; Geisse|e,A. B.; arrdBosacco,S.J.: Blood
l.M.:Denonstrationofafibrinolyticaclivatot'inredbonert"tarrow'AclaHoentalol"26:2'13-280'1961'
6. Bjiirkman,s.E.,andNilsson,
preoperativeautotlansfusionfol tltat hip proslheses'Acla Anacstlt'Bclgica'3o:1'75-182'1919'
7. Blaise,G., and Jackmuth,R.:
on the healingof
D'; and buschieri'A'r Adverseinfluetrceof fibrin sealant
8. Byrne, D. J.; Hardy,J.;Wood,R. A.; Mclntosn,n.; Hop'nood,
Edinburglt' 37:394-398'1992'
high-r-isksuturedcolonicanastomoses.J.Royalcoll. surgectns
Mcd'
patients.A reviewof blood replacementmethods'J' Florida
j;in;replacemcnt
total
rly
elde
in
9. cain, J. L.: Autologoustransfusion
Assn"66:35-38'1979'
and
R'; Noveck' H'; and strom' B' L': Effect of anaenia
' D^'^' D rir' Rorlin t
Spence'R' K'; Tr9^u-t'10. Carson,J. L.; Duff, A.; Poscs,R' M'; Berlin, J' A';
LanceL348:1055-1060,1996'
cardiovasculardiseaseonsurgicalnror.talityandrrrolbidity.
1 1 . c o l w e l l , c . w . , J r . ; s p i r o , T . E . ; T r o w b r i d g e , . l . a ' ; s r " p r ' " n s , J ' W ' G ' ; G a r dfor
i n eprevention
r ' G ' A " J r ' of
; a ndeep
d R i tvenous
t e r ' M ' thrombosis
A ' f o r t h e E afler
n o x aelective
parinclinical
un{ractionatedheparin
Trial Group: Efficacy and safetyof enoxaparinversus
'1995'
knee artlrroplasry.Ctin. Orthop' 321:19-27
July 1974'
56-4: 908-912'
in childre''s orthopaedics.J'Bttr'rcand 'loint surg''
12. cowclf, H. R., and swickard,J. w.: Autotransfusion
1987'
Malch
69-A:319'
blood for transfuslon'/' Bonc and Joittt Surg'''
13. Cowefl, H. R.: Editorial. Prior depositof autologous
Ant'Med'Assn''
t h r o ' , - , b i n a n d f i b r i n o g e n i n s k i n g r a fPt irnegl i m i n a r y r e p o r ' l ' J
14.cronkite,B.p.;Lozner,E.L.;andDeaver,J.M.:Useof
124:976-978,1944.
J Florida Med' Asstt' 66"
trlood salvagein spinal defo'rrity surgeryi' children'
15. csencsitz,T. A., and Flynn, J. c.: lntraoperatrve
39-41, 19't9.
'1991'
total knee arthroplasty'Clin' orthop ' 269:98-101
16. Cushner,E I),, and Friedman,R. J.: tslood lossin
appliedasa sp'ayedglue o'film
sealant
fib'in
of
p.;
efficacy
vivo
I'
R.:
white,
and
17. Dermotte,y.; Krack, G. E; Amrani, D. L.; Diorio, J.
'
1997
ne
Ju
and Hae ntost',OC-791Supplement'
in preventingpo* ,urgi.^i uanesions[abstract\ Throntib1g. Eckardt,J.J.;Gossett,T.c.;andAmstutz,u.c.rauiotogoust'ansfusionandtotalliiparthroplasty'Ctin.'orthop''132:39-45'1978'
coll' surgeons
protheroe,i.; u# w"lk"r, I. D.: Blood losswith kneeioint replace'rent"/ Royal
1g. Erskine,J. G.; Fraser,c.; simpson,R;
""1::i:'{,i[J]l;H;iZrtjuu"
report ln Proceedingsor the scoliosisResearch
"u,o,runsfusionin surseryfor scoliosis:a pretiminarv
,r.
Society.J. Bone and Joint Slrg', 56-,{: 1764'Dec'.1974'
21.Fahmy,N.R.,andPate|,D'G.:Hemostalic.hung*andpostoperativedeep-veinthrombosisassociatedwithuseofapneumattc
,, ff;l:;i
ti.:{:3::i:::::ff?fi:fl,i"1,i:1#TlJi::r,"cemenr: areview
(Supprement):
orrhopedics,l8
rriars.
crinicar
orrecenl
10-11,1995.
Jeffersonorthop l''
pr-esentstatus of intraoperativeblood recoveryduring orthopaedicsurgery'
23. Flynn, J. c., and csencsitz,T. A.:
'i7"f;.Yrh",rg"r,
(rAT) in spinal lurqery. spine, 7" 432-435,1982'
c. R.; and csencsitz,T. A.: rntraoperative aurorransfusion
,
B' N'; Ayers' D' c'; Rosenberg'
A. D., Jr.;lVlarder,v. J.;iiebert, Ii' M'; stumttg,
25. Francis,c. w.; peltegrini, v. D., Jr.; Totterman, ,..'j;4 j""p-u"in
comparison of warfarin and
arthroplasty'
hip
total
after
prevention
thronrbosis
oi
A.; Kessler,c.; and Johanson,N. A.:
1997'
' ,e
daiteparin..L Bone and Joittt Surg',79-A:1365-1372'Sept'
study.J. Ant. Med.
hepatitisin the united states'A prospeclrv cooperative
postlransfusion
of
Rlst<
r.-:
.1.
Bennett,
and
F.,
26. Grady,G.
Assn., 220: 692-701' 197Z'
surg.,Gynec..andobstet',2I:452-454'1915' "'
27. Grey,E.G.: Fibrin asa haemostaticin cereblalsulgely.
58:277-280'1983'iilution' '4ncsthesiology'
for
"orr"lt"d
loss:
Estimati'g allowableblood
/Nlpross,J.B.:
Llons' R'; and the-Ardeparin Arthroplasty Study Group:
t-,8. Heit,J.A.; Berkowitz, S.D.; Bona, R.; C"U"nas,V.; Corson,J. D.; Elliott,.C' G';
preventionof venousthrombo(a'deparinsodium)."onrpur"aio warfa'i' for the
Efficacy and safetyof low molecularweight i,"p"iin
Haentost''7'7:32-38'199'7'
siudy'Throntb'-and
embolismafter total kneereplacementsu'gery:I aouut"-utlna,dose-ranging Niemelli, H': Tianexamic acid (cyklokapron) r'educes
rvrantvre,r; Ylinen, J.';and
30. Hiippala, S.; Strid, L.; wennerstrand, M.; Arvcla,i
Britishl. Anaestlt.'.74:110
aith,'opiasty.
knee
rotal
with
associated
loss
blood
perioper.arive
]ll:1131: "
effectivetlran postoperattve
R' E: Preoperativeenoxapal.inis.nrore
n'",,,,
una
v.'
31. Hu||, R. D.; Pineo, G. F.; Va|entine,K. A.; s,"gg,
(THR): a pooled analysis
replacement
total'hip
uni"rgolng
(Dvr) irr patients
enoxaparinin trre pr.eventio'of deep vein thr.olibosis
OC-1578Supplenrent'p' 381'June 199f'
[abstract].Tfuontb.and Hoctt'tost"
of topical hemostaticagentsin elective
Taniura,H.; Yarnanoi,A'1 and Nakamura'T': Comparison
Y.-C,;
32. Kohno, H.; Nagasue,N.; chang,
966-9'10,1992'
16:
J.
s,ry.,
lrial.worltl
lrepaticresectio'r:aclinicalprJspectiverandomized
shoup' R J'; Krakauer'H';
J' C'; Solomon,R' E'; Purcell'R' H'; Hudson' L'M';
33. Koziol, D. E.; Holland, P. v.; Alling, D. W.; Melpolder,
in donatedblood' Ann'
agents
hepatitis
non-B
non-A,
for
nrarker
paradoxical
as a
and Alter, H. J.: Antibody to hepatitisB "or" un'tig"n
,^. i:;:.{;.t,tfl;-ii
,,
bloodrecoverv
autologous
withani'traoperative
K. D.;andBrink,M. A.: Experie'ce
iii;1,1,*f.*., Leatherman,
'#fi];]i:[:ffi:$.T|6fi:,Til
and
rerease
ortourniquet
Errects
k'eerepracemenr.
rorar
arrer
lili tf ':.* ross
Yili f;1'J.i.1';
c o n t l n u o u s p a s s t v e m o t i o n ' J ' B o n e a n d J o i n t S u r g " 1 3 - A : 1 0 3 7 - 1 0 4 0 ' A u gthtombosis
'1991'
i' the lower extremity after total joint
Sig'ificance of deep venous
36. Lotke, p. A.; steinberg,M. E.; and Ecker, M.-i.:
,r. il:iil:r:Tlf/j|].?:Hll;:,il.3ii:,tt"T
r17:254-257
're'|6'
ctin.orrhop',
surserv.
hiprepracemenr
i' rorar
brood
aurorogous
,anked
hip replacerne't'Surg'
i' total
r'; "ni Meeske,X' e': sanked autologousblood
38. Marmor, L.; Berkus, D.; Robertson,J. D.; Wiis-on,
,,. fl::#i.,'j*#:i:::"T#?3;0",
c/rrr'orthop''273:
onbloodlossin totalkneearthroplastv'
conceDtrares
".: Errecrorribrinogen
136-138,1991.
40.Martinowitz'U.'andSaltz,R.:Fibrinsealant.Curr.Opin.Henlatol.,3.:395-402'1996.
'
Throntb'and Haentost''78:66I-666'199'7
adiresives'
41. Martinowitz, U., and Sforoitt, W O.: Fibrin tissue
vol-. 81-A, NO. 11,NOVEMBER 1999
1588
oFER LEVy Er AL.
42. Maynard,M. J.; Scrrlco,T. P.; and Ghelman,B.: Progressionand regressionof deepvein thrombosisafter total knee arthroplasty.CIin.
O rthop., 273: 125- 130,1991.
43. Messmer,K.: Hemodilution.Sarg.Clin. North America,55:659-678,1975.
44. Milne' A. A.; Murphy,W. G.; Reading,S. J.; and Ruckley,C. V.: Fibrin sealantreducessuture line bleedingdr.rringcarotid endarterectomy;a randomisedtrial. EuropeanJ. Vasc.and Endovasc.
Sarg.,10:9l-94, 1995.
45. Mylod' A. G., Jr.; France,M. P.; Muser, D. E.; and Parsons,J. R.: Perioper:rtiveblood loss associatedwith total knee arthroplasty.
AcomparisonofproceduresperformedwithandwithoutcemeB
n toi n g
e .a"nLd J o i n t S u r g . , 7 2 -l 0
Al:0 - 1 0 1 2 , A u g . 1 9 9 0 .
46. NationallnstitutesofHealthConsensusConference:Perioperativeredbloodcelltransfusion.J.Am.Med.Assn.,260:2700-2703,1988.
47. Pattison'E.; Protheroe,K.; Pringle,R. M.; Kennedy,A. C.; and Dick, W. C.: Reductionin haemoglobinafter knee joint surgery.Ann.
Rheumat.Dis.,32:582-584.1973.
48. Peterman,T. A,; Jaffe, H. W.; Feorino, P. M.; Getchell, J. P.; Warfield, D. T.; Haverkos, H. W.; Stoneburner,R. L.; and Curran, J. W.:
Transfusion-associated
acquiredimmunodeficiency
syndromein the United States.
"/.Am. Med. Assn.,254..2913-2917,1985.
49. Podoshin'L.; Fradis'M.; Ben-David,J.; and Malatskey,S,:Resultsof sr.rrgery
for chronicotitis media:a S-yearstudy.Rev.Laryngol.Otol.
Rhinol. ( Bonleau.r),l16: 109-113,
1995.
50. Raut, V. V.; Stone,M. H,; and Wroblewski,B. M.: Reductionof postoperativeblood lossafter press-fitcondylarknee arthroplastywith
useof a femoralintramedullaryphtg.J. Boneand JointSurg.,75-A: 1356-l357,Sept.1993.
5 l. Reilly' T. J.; Gradisar,I. A., Jr.; Pakan,W.; and Reilly,M.: The use of postoperativesuction drainagein total knee arthroplasty.C/in.
O r thop., 208:238-242,1986.
52. Risberg'8.:Theresponseof
thefibrinolyticsystemintrauma.Acla
Chir.Scanclinavica,Supplementum522,pp.245-271,1985.
53. Schreiber'G. B.; Busch'M. P.;Kleinman,S. H.; and Koreliiz,J. J. for the RetrovirusEpidemiologyDonor Study:The risk of transfusiontransmittedviral infections.New EnglandJ. Med.,334:1685-1690,
1996.
54. Schwarz,N.; Redl, H.;Zeng; L.; Schlag,G.; Dinges,H. P.;and Eschberger,
J.: Early osteoinductionin rats is not alteredby fibrin sealant.
CIin. O r thop., 293:353-359,1,993.
55. Sfoand,E, M.: Viral risksassociated
with blood transfusion.
Prhotochem.trntlPhotobiol.,65:428-431.1997
.
56. Surgenor,D. M.; Wallace,E. L.; Churchill,W. H.; Hao, S. H.; Chapman,R. H.; and Poss,R.: Red cell transfusionsin total knee and total
hip replacementsurgery.Trnnsfusion,
3l: 531-537
, 1991.
57. Stevens,C. E.; Aach, R. D.; Hollinger, F. B.; Mosley,J. W.; Szmuness,lY.; Kahn, R.; Werch,J.; and Edwards,V.: Hepatitis B vrrus
antibody in blood donors and the occurrenceof non-A, non-B hepatitis in transfusionrecipients.An analysisof the transfusiontransmittedvirusesstudy..4nn. I ntern. M ed., l0l: 733-738,1984.
58. Thomson,J. D.; Callaghan,J. J.; Savory,C. J.; Stanton,R. P.; and Pierce,R. N.: Prior deposition of autologousblood.in elective
orthopaedicsurgery.l Boneand Joint Surg.,69-A:320-324,
March 1987.
59. Van der Ham, A. C.; Kort, W. J.; Weijma,I. M.; van den Ingh, H. R; and Jeekel,H.: Effect of fibrin sealanton the integrity of colonic
anastomoses
in ratswith faecalperitonitis.EuropeanJ. Surg.,1,59:425-432,1993.
60. Veikkolin, T.; Korkala,O.; Niskanen,R.; and Liesjarvi,S.: Autotransfusionof drained blood after total knee arthroplasty.Ann. Chir
Gy naeco1.,84:28l -284,1995.
61. Wittmann,E W.' and Ring, P.A.: Blood lossassociated
with Ring uncementedtotal knee replacement:comparisonbetweencontinuous
and intermittentsuctiondrainage../.
RoyalSoc.Med.,77:556-558,
1984.
62. Woolson,S. T.; Marsh,J. S.; and Tannet,J. B.: Transfusionof previously depositedautologousblood for patients undergoing hrpreplacementsurgery.-/.
Bone and Joint Surg.,69-A:325-328,
March 1987.
THE JOURNAL OF BONE AND JOINT SURGERY
Baixar