☰
Explorar
Assinar em
Inscrever-se
Envio
×
Baixar
Sem categoria
Einstein On line vol2_n4.p65 - Hospital Israelita Albert Einstein
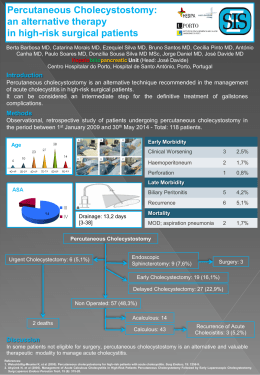
an alternative therapy in high
Resumos Artigos HA
Fungal spondylodiscitis due to Candida albicans: an atypical
Pressão interna ruptura ligação teto
e muito mais que a soma das gotas do mar
Fratura Ipsilateral do Colo e Diáfisedo Fêmur
Prevalence of hip and lower limb fracture in the city of Aracaju, Brazil
Inglês - Revista de Odontologia da UNESP
English