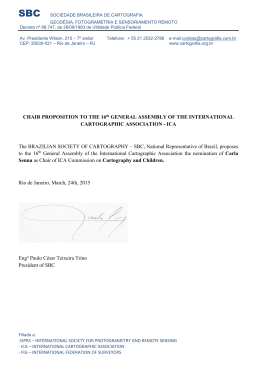
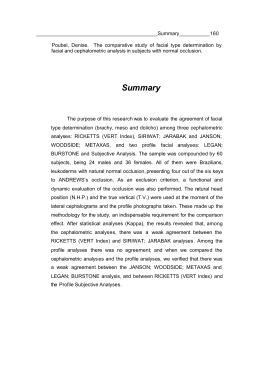
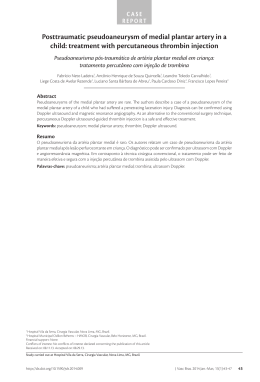
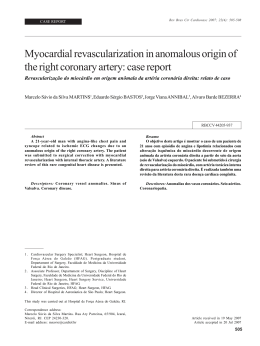
Reporte de casos Revista Chilena de Neurocirugía 38 : 2012 Endovascular treatment of iatrogenic pseudoaneurysm and delayed carotid-cavernous fistula following trans-sphenoidal surgery Tratamiento endovascular de pseudoaneurisma y fístula carótida-cavernosa iatrogénica después de la cirugía trans-esfenoidal Mário Luiz Marques Conti1, Guilherme Brasileiro de Aguiar1, José Carlos Esteves Veiga1, Américo Rubens Leite dos Santos1, Paulo Roberto Lazarini2, Maurício Jory1, Ricardo Hideo Tachibana3, José Guilherme Mendes Pereira Caldas.4 1 Department of Surgery, Division of Neurosurgery, Santa Casa Medical School, São Paulo, Brazil. 2 Otorhinolaryngology Department, Santa Casa Medical School, São Paulo, Brazil. 3 Medical student; Santa Casa Medical School, São Paulo, Brazil. 4 INRAD - Radiology Institute, Hospital das Clinicas da Faculdade de Medicina da Universidade de São Paulo - São Paulo, Brazil. Rev. Chil. Neurocirugía 38: 147 - 150, 2012 Resumen Lesiones accidentales de la arteria carótida son complicaciones poco frecuentes de diversos procedimientos diagnósticos y terapéuticos. Representan una condición grave y potencialmente mortal si el tratamiento no se realiza adecuadamente. Un paciente de sexo femenino, 45 años de edad, que ingresó en el servicio de Otorrinolaringología con queja de la disminución de la agudeza auditiva y acúfenos en el oído izquierdo. La resonancia magnética encefálica mostro una formación expansiva / infiltrativa a comprometer desde la nasofaringe izquierda hasta la base del cráneo, con la participación de la arteria carótida interna (ACI) en el mismo lado en su segmento petroso. Durante el procedimiento de biopsia, se produjo una laceración en la carótida derecha intracavernosa con sangrado abundante. Se realizó un taponamiento local y el paciente fue remitido a la angiografía cerebral que mostró un seudoaneurisma en la arteria carótida interna derecha en su segmento cavernoso. Después de una prueba de oclusión, la ACI derecha fue ocluida por 2 globos. Tres semanas después, el estado del paciente mostró empeoramiento progresivo de la agudeza visual, proptosis ocular, hiperemia conjuntival y la restricción del movimiento ocular en el ojo derecho. Una nueva angiografía fue realizada y mostró la persistencia de la oclusión de la ACI en su origen y un seudoaneurisma asociado con fístula carótido-cavernosa derecha, que se opacificado después de la inyección de contraste en la ACI izquierda, a través de la arteria comunicante anterior. El paciente fue sometido a un nuevo tratamiento endovascular con resolución de la lesión. Laceración de ACI durante la cirugía transesfenoidal es una complicación rara y potencialmente fatal. La prevención es el mejor tratamiento para cualquier lesión accidental. La utilización de técnicas endovasculares ha permitido para el tratamiento satisfactorio de esta condición. Palabras clave: Lesiones de la arteria carótida, seudoaneurismas, fístula carótido-cavernosa, tratamiento endovascular. Abstract Accidental carotid artery lesions are uncommon complications from diverse diagnostic and therapeutic procedures. It represents a grave and potentially lethal condition if treatment is not adequately performed. A female patient, 45 years old, who was admitted to the Otolaryngology service complaining of diminished auditory acuity and tinnitus in the left ear. The encephalic magnetic resonance imaging (MRI) showed an expansive/infiltrative formation compromising the left nasopharynx to the skull base, involving the ipsilateral internal carotid artery (ICA) in its petrous segment. During the biopsy procedure, there was a right intracavernous 147 Revista Chilena de Neurocirugía 38 : 2012 ICA laceration with copious bleeding. A local tamponade was performed and the patient was referred to cerebral angiography (CAG), which showed a right ICA pseudoaneurysm in its intracavernous segment. After a balloon occlusion test, the right ICA was occluded by 2 balloons. Three weeks after, the patient’s condition showed progressive worsening of visual acuity, occular proptosis, conjuctival hyperemia and occular movement restriction in the right eye. A new CAG was performed and showed persistence in the right ICA occlusion in its origin and an intracavernous pseudoaneurysm associated with ipsilateral carotidcavernous fistula, which became opacified after contrast injection in left ICA, through the anterior communicating artery. The patient was submitted to a new endovascular treatment with lesion resolution. ICA laceration during transsphenoidal surgery is a rare and potentially fatal complication. The prevention is the best treatment for any accidental lesion. Utilization of endovascular techniques has allowed for satisfactory treatment of this condition. Key words: Carotid Artery Injuries, Pseudoaneurysms, Carotid-Cavernous Sinus Fistula, Endovascular Treatment. Introduction Accidental lesions in the carotid artery are uncommon complications from various procedures1. During transsphenoidal surgeries the internal carotid artery (ICA) lesion constitutes a rare event, albeit grave and potentially lethal if treatment is not adequately performed1,2,3,4. It may manifest itself in peri- or postoperative bleeding, formation of internal carotid artery pseudoaneurysm or carotidca-vernous fistula (CCF)2,3,4,5, necessitating prompt diagnosis and treatment. This case study describes a case of right ICA laceration with the formation of a pseudoaneurysm, during a transsphenoidal surgery on a skull base tumor which was treated with ICA occlusion. A few days after the occlusion, the patient presented with occular symptoms. The cerebral angiography confirmed the right carotid occlusion and showed an ipsilateral carotid-cavernous fistula which opacified via the anterior communicating artery (ACoA). The patient was submitted to a new endovascular treatment with lesion resolution. Furthermore, we made a brief revision of the literature. Case report This female patient, 45 years old, was admitted to the Otolaryngology service complaining of diminished auditory acuity and tinnitus in the left ear. An encephalic magnetic resonance imaging (MRI) was performed which showed an expansive/infiltrative formation, compromising the left nasopharynx to the skull base, involving the ipsilateral internal carotid artery in its petrous segment. Transsphenoidal lesion biopsy was suggested. During the procedure, there was a right intracavernous ICA laceration with copi- 148 Figure 1: A – Right internal carotid artery angiography (lateral view), showing a pseudoaneurysm in the right intracavernous internal carotid artery (arrow). B and C - cerebral angiography of the left internal carotid artery during the right ICA balloon occlusion test (frontal view), not showing delay in angiographic times. D – placement of the balloons following the right ICA occlusion (lateral view). E – final angiographic control from the right common carotid artery (lateral view), showing right internal carotid artery occlusion (arrowheads). Reporte de casos ous bleeding. A local tamponade was performed and the patient was referred to cerebral angiography (CAG), which showed a right ICA pseudoaneurysm in its intracavernous segment (Figure 1A). Following the occlusion test (Figure 1 B-C), the right ICA was occluded by means of two Goldball 2 balloons (Balt Extrusion, Montmorency, France), which were deployed in the right ICA (Figure 1D) petrous and cervical segments. The final angiographic control showed a complete occlusion of the right ICA (Figure 1E). Three weeks after the initial procedure, the patient’s condition showed progressive worsening of visual acuity, occular proptosis, conjuctival hyperemia and occular movement restriction in the right eye (Figure 2A). A new CAG was performed and it showed persistence in the right ICA occlusion in its origin andA an intracavernous pseudoaneurysm measuring approximately 30 mm, associated with ipsilateral carotid-cavernous fistula (CCF), which became opacified after contrast injection in left ICA, through the ACoA (Figure 3A). The patient was then submitted to a new endovascular procedure in which a left ICA selective catheterism was performed, with lesion microcatheterism through the ACoA (Figura 3B) and embolization with coils (Figure 3C). The final angiographic control showed absence of pseudoaneurysm and CCF opacification (Figure 3D). The procedure was performed without complications and the patient’s condition progressed to the regression of symptoms (Figure 2B), save a discrete visual deficit to the right. Revista Chilena de Neurocirugía 38 : 2012 Figure 2: A – Patient’s ocular appearance previous to the second procedure, showing mydriasis, occular hyperemia and proptosis in the right eye. B – final aspect, following treatment, showing regression of occular signs. Discussion Diverse diagnostic and therapeutic procedures can determine an accidental carotid artery injury, such as: anterior cervical column surgery, central venous catheter insertion, chiropractic cervical manipulation, cerebral angiographies, middle ear surgery, percutaneous procedure for trigeminal neuralgia treatment, skull base surgeries, tracheostomy and transsphenoidal surgery1. Specifically in transsphenoidal surgeries, the incidence of carotid artery laceration is 0.3 to 0.4%1,6,7. These lesions represent well-documented complications and can have catastrophic results if not adequately treated. In the majority of cases, it is caused by direct surgical trauma to the intracavernous artery seg- Figure 3: A – Left internal carotid artery angiography (frontal view), showing a pseudoaneurysm in the intracavernous segment of the right ICA, associated with an ipsilateral carotidocavernous fistula (arrow), which became opacified through the ACoA. B and C - Lesions microcatheterism and coiling performed through the left internal carotid and anterior communicating arteries. D – final angiographic control of the left internal carotid artery, in frontal view, showing complete occlusion of the fistula and pseudoaneurysm. 149 Revista Chilena de Neurocirugía 38 : 2012 ment3. As a consequence, there may be bleeding, vascular spasms, arterial thrombosis, embolism and the formation of pseudoaneurysms and carotidcavernous fistulas2,3,4,5. In most cases of iatrogenic CCF, the accidental injury causes the formation of a pseudoaneurysm that ruptures immediately to the cavernous sinus. In this case, by contrast, was initially formed a pseudoaneurysm that was treated with occlusion of the vessel. Fistula formation occurred later, and through the cross flow from the other carotid artery. This makes this case even more different. The predisposing factors for the ICA iatrogenic lesion during transsphenoidal surgery most cited in the literature are: large invasive adenomas, reoperations, previous radiotherapy in the sellar region, previous prolonged use of dopaminergic agonists and radical surgeries for tumors which invade the cavernous sinus3. ICA anatomical variations, its proximity to the medial line2 and adjacent structures can also be predisposing factors for ICA lesions during transsphenoidal surgery. Renn and Rhoton8 demonstrated that in 71% of the cases, the ICA projects itself into the sphenoid sinus and in 4% it is covered exclusively by the cavernous sinus duramater and sphenoid sinus mucosa, favoring a lesion in the same during transsphenoidal sur- gery2. In this way, a detailed preoperatory anatomical assessment by imaging (MRI and computed tomography - CT) becomes imperative in order to minimize the risk of iatrogenic arterial lesion, especially in patients with aforementioned risk factors2,3. Other methods of evaluating the sellar region, such as the sellar 3D angiotomography, the paranasal region osseal window CT, the encephalic angioresonance and Doppler ultrasound (MicroDoppler Ultrasound), have already been described in the literature as being utilized in cases in which the MRI is not sufficient to detail its anatomy3,4. The ICA lesion must be rapidly diagnosed and treated. The initial measures include local tamponade, direct repair of the lesion or even surgical occlusion of the lesioned artery1,2,5, until the patient is stabilized, in order to procede with the cerebral angiography. Traditionally, the surgical or endovascular occlusion has been used for the definitive treatment of these lesions. As the surgical occlusion is associated with a larger incidence of complications, the endovascular treatment has been more amply employed2,5,8. In the case that the CAG shows an arterial lesion, endovascular occlusion of the vessel should be considered once the occlusion test has been performed2, as in the present case. In cases in which the occlusion test shows that the patient would not withstand the lesioned artery occlusion, bypass surgery prior to its occlusion should be considered9. Curren-tly, the employment of stents has been shown to be useful in situations in which the occlusion is contraindicated2,10. In addition to preserving the ICA flow, it allows for a rapid interruption of the bleeding and stabilization of the patient2. There are some case series describing the successful use of stents with preservation of flow in treatment of carotid-cavernous fistulas, however a larger follow-up and further studies are needed to establish definitive conclusions9,10. In this way, ICA laceration during transsphenoidal surgery is a rare complication, but when it occurs it can be fatal. The prevention is the best treatment for any accidental lesion, the different imaging methods being fundamental for this. Hopefully, accumulated knowledge and experience will reduce this type of complication in the future. Utilization of endovascular techniques has allowed for satisfactory treatment of this condition and new studies are necessary for the consolidation of endovascular methods which maintain the arterial flow. Recibido: 13.08.12 Aceptado: 11.09.12 References 1. Inamasu J, Guiot BH. Iatrogenic carotid artery injury in neurosurgery. Neurosurg Rev 2005; 28 (4): 239-47. 2. Park YS, Jung JY, Ahn JY, et al. Emergency endovascular stent graft and coil placement for internal carotid artery injury during transsphenoidal surgery. Surg Neurol 2009; 72 (6): 741-6. 3. Berker M, Aghayev K, Saatci I, et al. Overview of vascular complications of pituitary surgery with special emphasis on unexpected abnormality. Pituitary 2010; 13 (2): 160-7. 4. Ahuja A, Guterman LR, Hopkins LN. Carotid cavernous fistula and false aneurysm of the cavernous carotid artery: complications of transsphenoidal surgery. Neurosurgery 1992; 31 (4); 774-9. 5. Kocer N, Kizilkilic O, Albayram S, et al. Treatment of iatrogenic internal carotid artery laceration and carotid cavernous fistula with endovascular stent-graft placement. Am J Neuroradiol 2002; 23 (3): 442-6. 6. Fukushima T, Maroon JC. Repair of carotid artery perforations during transsphenoidal surgery. Surg Neurol 1998; 50 (2): 174-7. 7. Laws ER Jr. Vascular complications of transsphenoidal surgery. Pituitary 1999; 2 (2): 163-70. 8. Renn WH, Rhoton AL Jr. Microsurgical anatomy of the sellar region. J Neurosurg 1975; 43 (3): 288-98. 9. Kobayashi N, Miyachi S, Negoro M, et al. Endovascular treatment strategy for direct carotid-cavernous fistulas resulting from rupture of intracavernous carotid aneurysms. Am J Neuroradiol 2003; 24 (9): 1789-96. 10. Morón FE, Klucznik RP, Mawad ME, et al. Endovascular treatment of high-flow carotid cavernous fistulas by stent-assisted coil placement. Am J Neuroradiol 2005; 26 (6): 1399-404. Corresponding author: Guilherme Brasileiro de Aguiar, MD. Department of Surgery, Division of Neurosurgery, Santa Casa Medical School. São Paulo, Brazil. Rua Cesário Motta Jr., 112 - Vila Buarque. 01221-900. São Paulo - SP. Brazil. Tel: 55 11 21767000 Email: [email protected] 150
Baixar