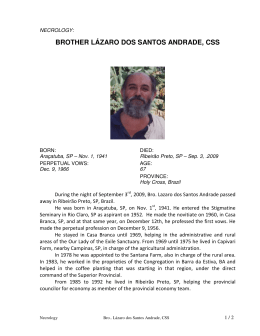
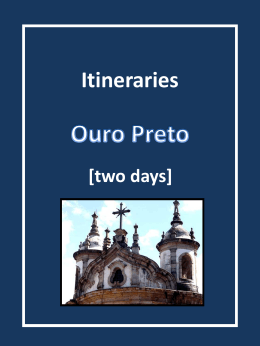
Titanium Membranes in Prevention of Alveolar Collapse After Tooth Extraction Márcia N. Pinho, MS,* Virgı́lio M. Roriz, MS,* Arthur B. Novaes, Jr., DDS, PhD,† Mário Taba, Jr., DDS, PhD,‡ Márcio F. M. Grisi, DDS, PhD,‡ Sérgio L. S. de Souza, DDS, PhD,‡ and Daniela B. Palioto, DDS, PhD‡ he resorption of alveolar bone following tooth extraction results in a narrowing and shortening of the residual ridge. Alveolar bone resorption is a common finding following tooth extraction, and it poses a problem for the clinician in 2 distinct manners: (1) it creates an esthetic problem for the fabrication of conventional or implantsupported prostheses, and (2) it can make the placement of endosseous implants difficult or even impossible. These patterns of resorption reduce the bone volume available for implant therapy.1-4 There are many techniques available to improve alveolar ridge collapse after tooth extraction, including connective tissue grafts, acellular dermal matrix grafts, and guided bone regeneration with or without the association of different bone grafts.5-8 The alveolar ridge preservation procedures are recommended at the extraction to prevent loss of tissue, reduce the number of surgeries, and increase the predictability of esthetic reconstruction.9 Guided bone regeneration is used to prevent alveolar ridge resorption or enlarge the alveolar ridge.10 The membrane acts as a mechanical barrier, the blood clot is protected from the overlying tissue, and bone promoting cells are the only cells allowed to repopulate the bone defect. The amount of T *Graduate student of Periodontology, School of Dentistry of Ribeirão Preto, University of São Paulo, Ribeirão Preto, São Paulo, Brazil. †Chairman of Periodontology, School of Dentistry of Ribeirão Preto, University of São Paulo, Ribeirão Preto, São Paulo, Brazil. ‡Professor of Periodontology, School of Dentistry of Ribeirão Preto, University of São Paulo, Ribeirão Preto, São Paulo, Brazil. ISSN 1056-6163/06/01501-053 Implant Dentistry Volume 15 • Number 1 Copyright © 2006 by Lippincott Williams & Wilkins DOI: 10.1097/01.id.0000202596.18254.e1 Background and Purpose: The resorption of alveolar bone following tooth extraction results in a narrowing and shortening of the residual ridge, which leads to esthetic and restorative problems, and reduces the bone volume available for implant therapy. The aim of this study was to evaluate the prevention of alveolar collapse after tooth extraction, using titanium membrane (Frios Boneshield; DENTSPLY Friadent, Mannheim, Germany), associated (or not) with autologous bone graft. Materials and Methods: A total of 10 nonsmoking healthy subjects, ranging from 35 to 60 years old, were selected for this study. Each patient had a minimum of 2 uni-radicular periodontally hopeless teeth, which were scheduled for extraction. After the procedure, 2 titanium pins were fixed on the vestibular bone surfaces that were used as references for the initial measures (depth, width, and height) of the socket. Of the sockets,1 was randomly chosen to be filled with autologous bone graft (test) removed from superior maxillary tuber, and the other one did not receive the graft (control). A titanium membrane was adapted and fixed, covering the sockets, which remained for at least 10 weeks. After a 6-month healing, the final measures were performed. Results: There was exposure of the membrane in 5 of the 10 treated subjects. Average bone filling (⫾standard deviation) among the 10 subjects was 8.80 ⫾ 2.93 mm (range 4-13) in the control group and 8.40 ⫾ 3.35 mm (range 4-13) in the test group. Average bone loss in width in both group was 1.40 ⫾ 1.97 mm (range ⫺4-1) in the control group and 1.40 ⫾ 0.98 mm (range ⫺4-0) in the test group. There was no significant statistical difference between groups considering the evaluated standards. Conclusion: The use of titanium membrane, alone or in association with autogenous bone, favored the prevention of alveolar ridge after tooth extraction. This membrane seems to be a possible and safe alternative to other nonresorbable membranes when the prevention of alveolar ridge resorption is the objective. (Implant Dent 2006;15:53– 61) Key Words: prevention, alveolar ridge resorption, bone graft, bone resorption, titanium membrane, guided bone regeneration regenerated bone is limited by the space available under the membrane. Autogenous bone or bone substitutes have been suggested as space maintainers under the membrane, and are considered the gold standard because there is the possibility of retaining cell viability, faster graft revascularization, and there is no possibility of disease transmission.11-13 Using autogenous bone, Becker et al14 observed the presence of osteocytes inside empty spaces, blood vessels, and secondary bone formation, proving its superiority in relation to lyophilized human bone grafts. Considering that both nonresorbable membranes and absorbable membranes tend to collapse into the defects, IMPLANT DENTISTRY / VOLUME 15, NUMBER 1 2006 53 more rigid membranes in association with grafts are required. The use of titanium membranes has been suggested instead of absorbable or expanded polytetrafluoroethylene (e-PTFE) membranes, with or without the association with grafts. The titanium membranes have micro-porosities small enough to prevent the penetration of cells and fibers but that allow the diffusion of interstitial fluid.11 Because of their rigidity, these barriers promote better space maintenance, favoring the formation and stability of the blood clot that is essential for cell proliferation and tissue regeneration. This article proposes a clinical, randomized controlled comparison of the use of titanium membranes associated with, and not associated with, autogenous bone grafts in the prevention of alveolar ridge resorption after extraction. MATERIALS AND METHODS After the Universities Human Research Committee approved the study protocol, 10 healthy subjects, ranging from 35 to 60 years old (average age 46.3), were selected. Each subject presented with at least 2 anterior maxillary teeth or premolars for extraction as a result of advanced periodontal disease (Fig. 1). The lost teeth were to be replaced following the healing period by osseointegrated implants. A temporary removable partial prosthesis was made for each subject to replace the missing teeth during the healing phase. Systemic antibiotics were given for 10 days (500 mg amoxicillin, 3 times/ day), beginning 24 hours before the surgical procedures. After local anesthesia, an intrasulcular incision with 2 vertical releasing incisions at the proximal angles of the teeth were made, and a mucoperiosteal flap was raised. A partial thickness flap was raised up to the mucogingival junction to guarantee the flexibility of the flap that is essential to cover the membranes without tension. The teeth were extracted as atraumatically as possible, without damaging the cortical bone using the Periotome (DENTSPLY Friadent, Mannheim, Germany). After the procedure, 2 membrane fixating tacks were placed on the buccal bone surfaces to be used as references 54 TITANIUM MEMBRANES IN Fig. 1. Teeth 11, 21, and 23 selected for extraction. Fig. 2. Illustration showing the socket measurements: internal vertical measurement (IVM), horizontal measurement (HM), and external vertical measurement (EVM). Fig. 3. Internal vertical measurement (IVM). Fig. 4. Horizontal measurement (HM). marks for the initial measurements, which were made with a periodontal probe to the nearest millimeter: (1) internal vertical measurement, distance from most apical end of the socket and the coronal border of the buccal bony wall (Figs. 2 and 3); (2) horizontal measurements, distance from the coronal border of the buccal bony wall to the coronal border of the lingual or PREVENTION OF Fig. 5. External vertical measurement (EVM). Fig. 6. Filling the test socket with the autogenous bone graft. Fig. 7. Test socket filled with the autogenous bone graft. Fig. 8. Titanium membrane adapted and fixed onto the alveolar ridge. palatal bony wall (Figs. 2 and 4); and (3) external vertical measurement, distance from the most coronal aspect of the pin to the coronal border of the buccal bony wall (Figs. 2 and 5).15 Of the sockets, 1 was randomly chosen to be filled with an autogenous bone graft (test), which was removed from superior maxillary tuberosity, while the other one remained as a control and did not receive a graft (Figs. 6 ALVEOLAR COLLAPSE AFTER TOOTH EXTRACTION Table 2. Vertical Bone Fill (N ⫽ 10 sites) Fig. 9. Flaps sutured using nonresorbable interrupted suture. Fig. 10. Six months after titanium membrane placement. Patient No. Control (mm) Test (mm) 1 2 3 4 5 6 7 8 9 10 Mean (SD) 12 9 10 11 4 7 9 13 5 8 8.80 (2.93) 13 9 7 10 4 5 8 10 11 7 8.40 (3.35) using a similar design to the one used in the initial surgical procedures. Comparisons between control and experimental sites at baseline and the 6-month postoperative period were performed using the Mann-Whitney test with the significance level set at 5% (P ⫽ 0.05). RESULTS and 7). A titanium membrane (Frios Boneshield; DENTSPLY Friadent) was adapted to cover the sockets and fixed with membrane fixating tacks (Fig. 8). Buccal and lingual flaps were approximated to achieve complete wound closure over the membranes. In some cases, cutback incisions were made into the periosteum of the buccal mucosa to eliminate tension present at the suture line. Flaps were sutured using nonresorbable single U-shaped interrupted sutures (Fig. 9). Subjects were prescribed the aforementioned medication plus oral antiseptics (10 mL rinses of 0.12% chlorhexidine gluconate for 2 minutes for 15 days). Subjects were also instructed not to wear any type of prosthesis, which could come in contact with the surgical area for 2 weeks following the surgical procedure. Sutures were removed 2 weeks after the surgery. After 6 months of membrane placement (Fig. 10), the final measurements were made during the reentry surgical procedures performed to remove the membranes. Buccal and lingual full-thickness flaps were elevated The subjects tolerated the surgical procedures well, and there were no postoperative complications, or clinical signs of inflammation or infection. There was exposure of the membrane in 5 of the 10 treated subjects between the sixth and tenth week of the placements. Patients were instructed to apply a daily a solution of 0.12% chlorhexidine to the exposed membrane until removal 30 days after the exposure. In addition, patients with membrane exposure came in for weekly appointments for bacterial plaque control and to verify the status of the clinical healing. The titanium tacks were left in place for the final measurements in the sixth postoperative month. Regardless of membrane exposure (or not), all 10 subjects were submitted to a reentry procedure after 6 months of membrane placement. Vertical Bone Fill The reentry procedures revealed that when the amount of existing bone tissue in the areas of the sockets was compared, before the placement and after the removal of the membranes, Table 1. Bone Fill (N ⫽ 10 sites) Control Group Test Group 8.80 ⫾ 2.93 mm (range 4-13) 8.40 ⫾ 3.35 mm (range 4-13) Data are presented as mean ⫾ SD. bone fill was observed but without statistical significance. In the control group, mean relative bone fill (⫾standard deviation [SD]) was 8.80 ⫾ 2.93 mm (range 4-13) and in the test group, 8.40 ⫾ 3.35 mm (range 4-13) (Tables 1 and 2). These values were relative, considering the tacks in the buccal surfaces of the bone as reference. Socket Depth In relation to socket depth, all sockets showed complete fill, so that at the measurement, the result was zero. Ridge Width Considering the width, both groups presented the same mean values of bone fill after 6 months of healing, 1.40 ⫾ 1.97 mm (range ⫺4-1) in the control group and 1.40 ⫾ 0.98 mm (range ⫺4-0) in the test group (Tables 3, 4). Although there was no difference between groups, there was statistical intra-group differences before and after the titanium membrane placements, but only in the test group, presenting the values: initial mean 8.3 ⫾ 1.41 mm (range 7-11) and final mean 6.9 ⫾ 1.85 (range 4- 11) (P ⫽ 0.04). Vertical Bone Fill and Horizontal Bone Loss The amount of new bone formation in each site was calculated by taking the socket (depth), adding or diminishing the bone height, depending on an increase or decrease in bone height 6 months after membrane placement (Tables 2, 4, and 5). DISCUSSION The deformities of the alveolar ridge in the anterior maxillary area caused by extraction normally leads to functional and esthetic problems, and can be difficult to solve. Considering the results of this study, the titanium membranes can be used to preserve the alveolar ridge with minimum bone remodeling after tooth extraction. In the present, and apparently first controlled randomized, clinical study using titanium membranes, the autogenous bone graft did not favor bone formation in height or width in the subjects that had no membrane exposure.15-20 When the values of ridge width were compared IMPLANT DENTISTRY / VOLUME 15, NUMBER 1 2006 55 Table 3. Bone Loss (width) Control Test 1.40 ⫾ 1.97 mm (range ⫺4-1) 1.40 ⫾ 0.98 mm (range ⫺4-0) Data are presented as mean ⫾ SD (N ⫽ 10 sites). Table 4. Horizontal Bone Loss Patient No. Control Test 1 ⫺2 ⫺1 2 ⫺3 0 3 1 ⫺1 4 ⫺4 ⫺3 5 0 ⫺1 6 0 ⫺1 7 ⫺1 ⫺1 8 0 0 9 ⫺1 ⫺2 10 ⫺4 ⫺4 Mean (SD) ⫺1.40 (1.97) ⫺1.40 (0.98) Data are presented in mm ⫾ SD (Sinal –: bone loss) (N ⫽ 10 sites). before and after membrane placement, the bone loss observed was statistically significant in the test group. One explanation for this result is that the titanium membranes were rigid enough to favor space maintenance, protecting the blood clot from the overlying tissue and allowing only bone promoting cells to repopulate the bone defect. In this situation, the additional use of grafting materials may not be necessary. According to Becker et al,14 the association is needed only when the selected membrane does not maintain space well. Therefore, autogenous bone, or bone substitutes, has been suggested as space maintainers Table 5. Relative Bone Fill: Initial and Final Measurements Initial and Final Measures of the 10 Subjects Control Patient No. 1 1 1 2 2 2 3 3 3 4 4 4 5 5 5 6 6 6 7 7 7 8 8 8 9 9 9 10 10 10 Measures Initial SD RW RH SD RW RH SD RW RH SD RW RH SD RW RH SD RW RH SD RW RH SD RW RH SD RW RH SD RW RH Test Final Difference Initial Final Difference 0 7 10 0 7 6 0 9 7 0 5 4 0 7 5 0 9 7 0 6 8 0 12 5 0 7 3 0 4 6 11 2 ⫺1 10 3 1 10 ⫺1 0 13 4 2 5 0 1 5 0 ⫺2 8 1 ⫺1 13 ⫺1 0 6 1 1 11 4 3 9 7 6 9 7 7 8 9 6 10 9 4 6 7 6 6 7 7 7 8 6 10 11 4 12 10 8 9 8 6 0 6 10 0 7 7 0 8 5 0 6 4 0 6 4 0 6 6 0 7 7 0 11 4 0 8 7 0 4 4 9 1 ⫺4 9 0 0 8 1 1 10 3 0 6 1 2 6 1 1 7 1 ⫺1 10 0 0 12 2 1 9 4 2 11 9 9 10 10 7 10 8 7 13 9 6 5 7 6 5 9 5 8 7 7 13 11 5 6 8 4 11 8 9 Control indicates membrane; final, 6 months; initial, time 0; RH, ridge height (mm); RW, ridge width (mm); SD, socket depth (mm); Test, membrane ⫹ bone graft. 56 TITANIUM MEMBRANES IN PREVENTION OF under the membrane to ensure adequate space for regeneration and promote bone growth. Autogenous bone grafts are considered the gold standard because there is the possibility of retaining cell viability, faster graft revascularization, and there is no possibility of disease transmission.11-13 Using autogenous bone, Becker et al14 observed the presence of osteocytes inside empty spaces, blood vessels, and secondary bone formation, proving its superiority in relation to lyophilized human bone grafts. Mean bone loss in width in both groups (1.40 mm) was similar to values found by Lekovic et al15 when absorbable membranes were used. When our results were compared to another study by Lekovic et al,16 in which e-PTFE membranes were used, 30% more bone loss in width (1.80 mm) was found in their study. This finding is relevant and significant because of the fact that using e-PTFE membranes, 3 of 10 cases were exposed, and, in this study, 5 of 10 were exposed. Although membrane exposure in this study was more frequent, the mean value of bone loss in width was smaller. This fact could be explained by the lower contamination of the titanium membranes.21-25 The comparison of our findings in bone fill to other studies is difficult because our results are reported using the membrane fixating tacks as references.15-17 Therefore, relative bone formation was measured and not absolute bone gain in terms of millimeters. However, the present results show maintenance of alveolar ridge and prevention of resorption after extraction. Titanium membranes are not as flexible as other membranes, and this could favor its increased exposure.11,26 The value of exposure (50%) of this study is similar to studies in which absorbable membranes were used.16,19 Another factor that could contribute to the exposure is the suturing technique, and in this study, a simple, interrupted suturing technique was used. Maybe a more elaborate technique could reduce the exposure. Absorbable membranes have the advantage over nonresorbable ones of not needing a second procedure for removal but, similar to e-PTFE membranes, require the association with bone ALVEOLAR COLLAPSE AFTER TOOTH EXTRACTION grafts because, in some cases, space maintenance can be a problem. In addition, e-PTFE membranes are highly contaminated when exposed, and, considering the results of this study, titanium membranes may be a good alternative for ridge preservation. CONCLUSION Based on these findings, it can be concluded that titanium membranes associated (or not) with bone grafts can prevent resorption of the alveolar ridge following tooth extraction,. This membrane can be used as a safe alternative to other membranes in guided bone regeneration. Disclosure The author claims to have no financial interest in any company or any of the products mentioned in this article. ACKNOWLEDGMENT The authors thank DENTSPLY Friadent Brazil for supplying the membranes. REFERENCES 1. Johnson K. A study of the dimensional changes occurring in the maxilla following tooth extraction. Aust Dent J. 1969; 14:241-244. 2. Johnson K. A study of the dimensional changes occurring in the maxilla following closed face immediate denture treatment. tooth extraction. Aust Dent J. 1969;14:371-376. 3. Seibert JS, Cohen DW. Periodontal considerations in preparation for fixed and removable prosthodontics. Dent Clin North Am. 1987;31:529-538. 4. Allen EP, Gainza CS, Farthing GG, et al. Improved technique for localized ridge augmentation. A report of 21 cases. J Periodontol. 1985;56:195-199. 5. Abrams L. Augmentation of the deformed residual edentulous ridges for fixed prosthesis. Compend Contin Educ Dent. 1980;1:205-209. 6. Jonck LM, Grobbelaar CJ. A glass ionomer for reconstructive surgery. Ionogran-Na ionomeric micro implant. A biological evaluation. Clin Mater. 1992;9: 85-103. 7. Dahlin C, Lekholm U, Linde A. Membrane-induced bone augmentation at titanium implants. A report of 10 fixtures followed from 1 to 3 years after loading. Int J Periodontics Restorative Dent. 1991;11: 273-281. 8. Simion M, Dahlin C, Trisi P, et al. Qualitative and quantitative comparative study on different filling materials used in bone tissue regeneration. A controlled clinical study. Int J Periodontics Restorative Dent. 1994;14:199-215. 9. Sottosanti J. Aesthetic extractions with calcium sulfate and the principles of guided tissue regeneration. Pract Periodontics Aesthet Dent. 1993;5:61-69. 10. Fugazzotto PA. Report of 302 consecutive ridge augmentation procedures: Technical considerations and clinical results. Int J Oral Maxillofac Implants. 1998; 13:358-368. 11. Watzinger F, Luksch J, Millesi W, et al. Guided bone regeneration with titanium membranes: A clinical study. Br J Oral Maxillofac Surg. 2000;38:312-315. 12. Proussaefs P, Lozada J, Kleinman A, et al. The use of titanium mesh in conjunction with autogenous bone graft and inorganic bovine bone mineral (Bio-Oss) for localized alveolar ridge augmentation: A human study. Int J Periodontics Restorative Dent. 2003;23:185-195. 13. Goldberg VM, Stevenson S. Natural history of autografts and allografts. Clin Orthop. 1987;225:7-16. 14. Becker W, Becker BE, Caffesse R. A comparison of demineralized freezedried bone and autologous bone to induce bone formation in human extraction sockets. J Periodontol. 1994;65:1128-1133. 15. Lekovic V, Camargo PM, Klokkevold PR, et al. Preservation of alveolar bone in extraction sockets using bioabsorbable membranes. J Periodontol. 1998;69:10441049. 16. Lekovic V, Kenney EB, Weinlaender M, et al. A bone regenerative approach to alveolar ridge maintenance following tooth extraction. Report of ten cases. J Periodontol. 1997;68:563-570. 17. Dies F, Etienne D, Abboud NB, et al. Bone regeneration in extraction sites after immediate placement of an e-PTFE membrane with or without a biomaterial. A report on 12 consecutive cases. Clin Oral Implants Res. 1996;7:277-285. 18. Fowler EB, Breault LG, Rebitski G. Ridge preservation utilizing an acellular dermal allograft and demineralized freeze-dried bone allograft: Part I. A report of 2 cases. J Periodontol. 2000;71:1353-1359. 19. Zubillaga G, Von Hagen S, Simon BI, et al. Changes in alveolar bone height and width following post-extraction ridge augmentation using a fixed bioabsorbable membrane and demineralized freeze-dried bone osteoinductive graft. J Periodontol. 2003;74:965-975. 20. Fugazzotto PA. GBR using bovine bone matrix and resorbable and nonresorbable membranes. Part 2: Clinical results. Int J Periodontics Restorative Dent. 2003;23:599-605. 21. Lundgren AK, Sennerby L, Lundgren D. Guided jaw-bone regeneration using an experimental rabbit model. Int J Oral Maxillofac Surg. 1998;27:135-140. 22. Simion M, Baldoni M, Rossi P, et al. A comparative study of the effectiveness of e-PTFE membranes with and without early exposure during the healing period. Int J Periodontics Restorative Dent. 1994;14: 166-180. 23. Nowzari H, Slots J. Microbiologic and clinical study of polytetrafluoroethylene membranes for guided bone regeneration around implants. Int J Oral Maxillofac Implants. 1995;10:67-73. 24. Fritz ME, Eke PI, Malmquist J, et al. Clinical and microbiological observations of early polytetrafluoroethylene membrane exposure in guided bone regeneration. Case reports in primates. J Periodontol. 1996;67:245-249. 25. Arpak MN, Alkan A, Nergiz I. A case of localized ridge augmentation from using a titanium membrane: a pilot study. J Oral Sci. 2000;42:133-138. 26. Jovanovic SA, Schenk RK, Orsini M, et al. Supracrestal bone formation around dental implants: An experimental dog study. Int J Oral Maxillofac Implants. 1995;10:23-31. Reprint requests and correspondence to: Arthur B. Novaes, Jr., DDS, PhD Faculdade de Odontologia de Ribeirão Preto Universidade de São Paulo Av. do Café S/N 14040-904, Ribeirão Preto, SP, Brazil Fax: (5516) 633-0999 E-mail: [email protected] IMPLANT DENTISTRY / VOLUME 15, NUMBER 1 2006 57 Abstract Translations [German, Spanish, Portugese, Japanese] AUTOR(EN): Márcia N. Pinho, MS*, Virgilio M. Roriz, MS**, Arthur B. Novaes Jr., DDS, PhD***, Mário Taba Jr., DDS, PhD#, Márcio F. M. Grisi, DDS, PhD##, Sérgio L. S. de Souza, DDS, PhD###, Daniela B. Palioto, DDS, PhD⫹. *Student mit Graduiertenstatus im Bereich der Parodontologie, zahnmedizinische Fakultät von Ribeirão Preto, Universität von São Paulo, Ribeirão Preto, São Paulo, Brasilien. **Student mit Graduiertenstatus im Bereich der Parodontologie, zahnmedizinische Fakultät von Ribeirão Preto, Universität von São Paulo, Ribeirão Preto, São Paulo, Brasilien. ***Leiter des Parodontologie, zahnmedizinische Fakultät von Ribeirão Preto, Universität von São Paulo, Ribeirão Preto, São Paulo, Brasilien. #Professor für Parodontologie, zahnmedizinische Fakultät von Ribeirão Preto, Universität von São Paulo, Ribeirão Preto, São Paulo, Brasilien. ##Professor für Parodontologie, zahnmedizinische Fakultät von Ribeirão Preto, Universität von São Paulo, Ribeirão Preto, São Paulo, Brasilien. ###Professor für Parodontologie, zahnmedizinische Fakultät von Ribeirão Preto, Universität von São Paulo, Ribeirão Preto, São Paulo, Brasilien. ⫹Professorin für Parodontologie, zahnmedizinische Fakultät von Ribeirão Preto, Universität von São Paulo, Ribeirão Preto, São Paulo, Brasilien. Schriftverkehr: Arthur B. Novaes Junior, DDS, PhD, Faculdade de Odontologia de Ribeirão Preto, Universidade de São Paulo, Av. do Café S/N, 14040-904, Ribeirão Preto, SP, Brasilien. Fax: ⫹5516 633-0999, eMail: [email protected] 58 TITANIUM MEMBRANES IN Titanmembrane im Einsatz zur Verhütung eines der Zahnextraktion folgenden alveolären Kollapses ZUSAMMENFASSUNG: Hintergrund und Zielsetzung: Die Resorption des Alveolarknochens nach einer Zahnextraktion führt zu einer Verringerung und Verkürzung des verbleibenden Kamms, was wiederum in ästhetischen sowie Wiederherstellungstechnischen Problemen resultiert und eine Verringerung des für eine Implantierung zur Verfügung stehenden Knochenvolumens nach sich zieht. Die vorliegende Studie zielte darauf ab, die Möglichkeiten der Verhütung eines alveolären Kollapses nach Zahnextraktion durch Einsatz von Titanmembranen /Frios Boneshield, Dentsply Friadent, Mannheim, Deutschland) zu erheben, sowohl in Verbindung mit wie auch ohne autologes Knochengewebstransplantat. Materialien und Methoden: Insgesamt wurden 10 gesunde, nicht rauchende Teilnehmer im Alter von 35 bis 60 Jahren für diese Studie ausgewählt. Jeder dieser Patienten hatte mindestens 2 einwurzelige Zähne, die aus parodontaler Sicht nicht mehr zu retten und daher für eine Zahnextraktion vorgesehen waren. Nach dem Eingriff wurden zwei Stifte auf der Oberfläche des vestibulären Knochens angebracht, um als Referenz für die Ursprungsmessungen (Tiefe, Weite, Höhe) der Pfanne zu fungieren. Eine der Höhlen wurde nach dem Zufallsprinzip zur Füllung mit autologem, aus dem oberen Tuber maxillare gewonnenem Knochentransplantat (Testgruppe) ausgewählt, während die andere ohne Transplantat blieb (Kontrollgruppe). Eine Titanmembran wurde zur Abdeckung der Pfannen angepasst und befestigt und für mindestens 10 Wochen dort belassen. Nach einer 6-monatigen Membranplatzierungszeit wurden die abschließenden Maßnahmen durchgeführt. Ergebnisse: Eine Exposition der Membran war in 5 von 10 Fällen der behandelten Patienten zu beobachten. Die durchschnittliche Anfüllung mit Knochen für die 10 Patienten lag bei 8,80 ⫾ 2,93 (im Bereich von 4 bis 13 mm) für die Kontrollgruppe und bei 8,40 ⫾ 3,35 mm (im Bereich von 4 bis 13 mm) für die Testgruppe. Der durchschnittliche Knochengewebsverlust in der Breite lag für die Kontrollgruppe bei 1,40 ⫾ 1,97 mm (im Bereich von ⫺2 bis 4 mm) und für die Testgruppe bei 1,40 ⫾ 0,98 mm (im Bereich von ⫺4 bis 0 mm). Bezüglich der bewerteten Standards konnten keine bedeutenden Unterschiede zwischen den Studiengruppen festgestellt werden. Schlussfolgerung: Der Einsatz einer Titanmembran, entweder allein oder in Verbindung mit autologem Knochengewebe, begünstigt die Erhaltung des Aleolarkamms nach Zahnextraktion. Diese Membran scheint eine realistische und sichere Alternative zu anderen nicht resorbierbaren Membranen darzustellen, wenn es darum geht, eine Resorption des Alveolarkamms zu verhindern. SCHLÜSSELWÖRTER: Verhinderung, Resorption des Alveolarkamms, Knochentransplantat, Knochengewebsresorption, Titanmembran, geleitete Knochenregeneration PREVENTION OF ALVEOLAR COLLAPSE AFTER TOOTH EXTRACTION AUTOR(ES): Márcia N. Pinho, MS*, Virgı́lio M. Roriz, MS**, Arthur B. Novaes Jr., DDS, PhD***, Mário Taba Jr., DDS, PhD#, Márcio F. M. Grisi, DDS, PhD##, Sérgio L. S. de Souza, DDS, PhD***. Daniela B. Palioto, DDS, PhD†. *Estudiante graduado de Periodontologı́a, Facultad de Odontologı́a de Riberão Preto, Universidad de San Pablo, Riberão Preto, San Pablo, Brasil. **Estudiante graduado de Periodontologı́a, Facultad de Odontologı́a de Riberão Preto, Universidad de San Pablo, Riberão Preto, San Pablo, Brasil. ***Jefe de Periodontologı́a, Facultad de Odontologı́a de Riberão Preto, Universidad de San Pablo, Riberão Preto, San Pablo, Brasil. #Profesor de Periodontologı́a, Facultad de Odontologı́a de Riberão Preto, Universidad de San Pablo, Riberão Preto, San Pablo, Brasil. ##Profesor de Periodontologı́a, Facultad de Odontologı́a de Riberão Preto, Universidad de San Pablo, Riberão Preto, San Pablo, Brasil. ###Profesor de Periodontologı́a, Facultad de Odontologı́a de Riberão Preto, Universidad de San Pablo, Riberão Preto, San Pablo, Brasil. †Profesor de Periodontologı́a, Facultad de Odontologı́a de Riberão Preto, Universidad de San Pablo, Riberão Preto, San Pablo, Brasil. Correspondencia a: Arthur B. Novaes Junior, DDS, PhD, Faculdade de Odontologı́a, Riberão Preto, Universidade de São Paulo, Av. Do Café S/N, 14040-904, Ribeirão Preto, SP, Brazil. Fax: 5516 633-0999, Correo electrónico Las membranas de titanio en la prevención del colapso alveolar luego de la extracción de un diente ABSTRACTO: Antecedentes y Propósito: La reabsorción del hueso alveolar luego de la extracción de un diente resulta en el angostamiento y acortamiento de la cresta residual lo que lleva a problemas estéticos y restaurativos y reduce el volumen de hueso disponible para la terapia de implantes. El objetivo de este estudio fue evaluar la prevención del colapso alveolar luego de la extracción del diente, usando una membrana de titanio (Frios Boneshield, Dentsply Friadent, Mannhein, Alemania) asociado (o no) con un injerto de hueso autólogo. Materiales y Métodos: Se seleccionaron un total de 10 sujetos saludables que no fumaban, con una variación de 35 a 60 años de edad para el estudio. Cada paciente tenı́a un mı́nimo de 2 dientes uniradiculares sin esperanza periodóntica que fueron programados para su extracción. Después del procedimiento, se colocaron dos clavijas de titanio en las superficies del hueso vestibular que se usaron como referencias para las mediciones iniciales (profundidad, ancho, alto) de la cavidad. Una de las cavidades fue elegida al azar para ser llenada con un injerto de hueso autólogo (prueba) sacado de la tuberosidad del maxilar superior y el otro no recibió el injerto (control). Se adaptó y fijó una membrana de titanio, cubriendo los receptáculos que se mantuvieron por lo menos durante 10 semanas. Luego de la colocación de la membrana durante seis meses, se completaron las mediciones finales. Resultados: Ocurrió una exposición de la membrana en cinco de los 10 sujetos tratados. El promedio de rellenado de hueso entre los 10 sujetos fue 8,80 ⫾ 2,93 (variación de 4 a 13 mm) en el grupo de control y 8,40 ⫾ 3,35 mm (variación de 4 a 13 mm) en el grupo de prueba. El promedio de pérdida de hueso en anchura en ambos grupos fue 1,40 ⫾ 1,97 mm (variación de ⫺4 a 1 mm) en el grupo de control y 1,40 ⫾ 0,98 mm (variación de ⫺4 a 0 mm) en el grupo de prueba. No existió una diferencia estadı́sticamente significativa entre los dos grupos considerando las normas evaluadas. Conclusión: El uso de una membrana de titanio, sola o asociada al hueso autógeno, favoreció la prevención de una cresta alveolar luego de la extracción de un diente. Esta membrana parece ser una alternativa segura y posible a otras membranas no reabsorvibles cuando el objetivo es la prevención de la reabsorción de la cresta alveolar. PALABRAS CLAVES: prevención, reabsorción de la cresta alveolar, injerto de hueso, reabsorción del hueso, membrana de titanio, regeneración guiada del hueso. IMPLANT DENTISTRY / VOLUME 15, NUMBER 1 2006 59 AUTOR(ES): Márcia N. Pinho, Mestre em Ciência*, Virgı́lio M. Roriz, Mestre em Ciência**, Arthur B. Novaes Jr., CirurgiãoDentista, PhD***, Mário Taba Jr., CirurgiãoDentista, PhD#, Márcio F. M. Grisi, Cirurgião-Dentista, PhD##, Sérgio L. S. de Souza, Cirurgião-Dentista, PhD###, Daniella B. Palioto, Cirurgião-Dentista, PhD⫹. *Estudante de Pós-Graduação em Periodontologia, Faculdade de Odontologia de Ribeirão Preto, Universidade de São Paulo, Ribeirão Preto, São Paulo, Brasil. **Estudante de Pós-Graduação em Periodontologia, Faculdade de Odontologia de Ribeirão Preto, Universidade de São Paulo, Ribeirão Preto, São Paulo, Brasil. ***Chefe de Periodontologia, Faculdade de Odontologia de Ribeirão Preto, Universidade de São Paulo, Ribeirão Preto, São Paulo, Brasil. #Professor de Periodontologia, Faculdade de Odontologia de Ribeirão Preto, Universidade de São Paulo, Ribeirão Preto, São Paulo, Brasil. ##Professor de Periodontologia, Faculdade de Odontologia de Ribeirão Preto, Universidade de São Paulo, Ribeirão Preto, São Paulo, Brasil. ###Professor de Periodontologia, Faculdade de Odontologia de Ribeirão Preto, Universidade de São Paulo, Ribeirão Preto, São Paulo, Brasil. ⫹Professor de Periodontologia, Faculdade de Odontologia de Ribeirão Preto, Universidade de São Paulo, Ribeirão Preto, São Paulo, Brasil. Correspondência para: Arthur B. Novaes Júnior, DDS, PhD, Faculdade de Odontologia de Ribeirão Preto, Universidade de São Paulo, Av. do Café s/n, 14040-904, Ribeirão Preto, SP, Brasil. Fax: ⫹55 16 6330999, E-mail: novaesjr@forp. usp.br 60 TITANIUM MEMBRANES IN Membranas de Tita nio na Prevenção de Colapso Alveolar após Extração de Dente RESUMO: Antecedentes e Propósito: A reabsorção de osso alveolar em seguida à extração de dente resulta num estreitamento e encurtamento do rebordo residual que leva a problemas estéticos e de restauração e reduz o volume do osso disponı́vel para terapia de implante. O objetivo deste estudo era avaliar a prevenção de colapso alveolar após a extração de dente, usando membrana de tita nio (Frios Boneshield, Dentsply Friadent, Mannheim, Alemanha), associada (ou não) a enxerto ósseo autólogo. Materiais e Métodos: Um total de 10 indivı́duos saudáveis não-fumantes, entre 35 e 60 anos de idade, foram selecionados para este estudo. Cada paciente tinha um mı́nimo de 2 dentes uni-radiculares periodontalmente inúteis que foram escalados para extração. Após o procedimento, dois pinos de tita nio foram fixados nas superfı́cies do osso vestibular que foram usados como referências para as medidas iniciais (profundidade, largura, altura) do alvéolo. Um dos alvéolos foi escolhido aleatoriamente para ser obturado com enxerto ósseo autólogo (teste) removido da tuberosidade maxilar superior, e o outro não recebeu o enxerto (controle). Uma membrana de tita nio foi adaptada e fixada, cobrindo os alvéolos, que permaneceram por pelo menos 10 semanas. Depois de seis meses de colocação da membrana, as medidas finais foram tomadas. Resultados: Houve exposição da membrana em cindo dos 10 indivı́duos tratados. A média de obturação óssea entre os 10 indivı́duos foi de 8,80 ⫾ 2,93 (de 4 a 13 mm) no grupo de controle e de 8,40 ⫾ 3,35 (de 4 a 13 mm) no grupo de teste. A média de perda óssea em largura em ambos os grupos foi de 1,4 ⫾ 1,97 (de – 4 a 1 mm) no grupo de controle e de 1,4 ⫾ 0,98 (de – 4 a 0 mm) no grupo de teste. Não houve diferença estatı́stica significativa entre os grupos, considerando os padrões avaliados. Conclusão: O uso de membrana de tita nio, sozinha ou em associação com osso autógeno, favoreceu a prevenção de rebordo alveolar após a extração de dente. Esta membrana parece ser uma alternativa possı́vel e segura a outras membranas não-reabsorvı́veis quando a prevenção de reabsorção do rebordo alveolar for o objetivo. PALAVRAS-CHAVE: prevenção, reabsorção do rebordo alveolar, enxerto ósseo, reabsorção óssea, membrana de tita nio, regeneração óssea guiada. PREVENTION OF ALVEOLAR COLLAPSE AFTER TOOTH EXTRACTION IMPLANT DENTISTRY / VOLUME 15, NUMBER 1 2006 61
Download