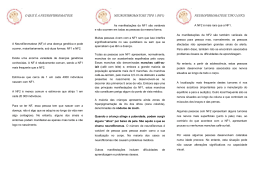
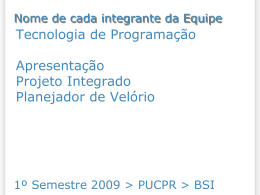
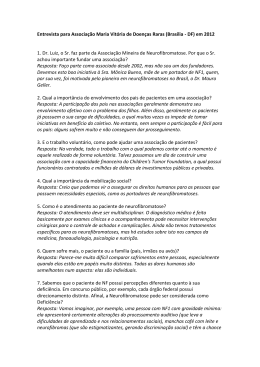
Relato de viagem: Congresso de NF em Barcelona, Seminário em Doenças Raras em Coimbra e encontro com a Associação Portuguesa de NF em Lisboa. Por Dr Luiz Oswaldo Carneiro Rodrigues Thalma e eu, representando a Amanf, comparecemos a três eventos no mês de setembro de 2014 na Europa. As três oportunidades transformaram-se em novos contatos, aprendizados importantes e estreitamento dos laços de cooperação com outras associações. Dr Luiz Oswaldo diante de um dos pôsteres apresentados em Barcelona. O Congresso Europeu de NF, este ano realizado em Barcelona, é um evento com menor número de participantes do que o congresso internacional promovido pelo Children’s Tumor Foundation nos Estados Unidos, ao qual nosso grupo do Centro de Referência em Neurofibromatoses do HC-UFMG tem comparecido anualmente e neste ano de 2014 contou com a participação de participantes do CRNF HC UFMG: Dr Nilton Alves de Rezende, Dra. Juliana Ferreira de Souza e doutorando Marcio de Souza. A principal diferença entre os dois eventos, além da maior participação de cientistas, médicos e familiares europeus, parece-me ser a maior atenção dada às associações de apoio no encontro europeu. Como geralmente ocorre, em Barcelona, alguns novos tijolos foram acrescentados à construção lenta e firme do edifício de conhecimentos sobre as neurofibromatoses, em especial o destaque à necessidade de maior prevenção do câncer de mama nas mulheres com NF1. No evento, apresentamos três temas livres (conteúdo completo dos resumos disponível abaixo), abordando a menor tolerância ao calor nas pessoas com NF1 e a documentação fotográfica comprovando cerca de 6% de incidência do segundo sinal dos dedos dos pés nas crianças com NF1. Além disso, em parceria com o Rogério Martins, fundador da Associação Maria Vitória de Doenças Raras (AMAVI), apresentamos um pôster que mostra a diferença do modo de ação das associações de NF e das associações de doenças raras, pois estas últimas parecem contar com maior interesse financeiro da indústria farmacêutica. Em Coimbra, participamos de um Seminário sobre Experiências e Trajetórias de Cuidados de Saúde: as Doenças Raras em Debate, 23 de setembro de 2014, Centro de Estudos Sociais, Universidade de Coimbra. No qual apresentei uma palestra sobre as características das NF que são compartilhadas com as demais doenças raras: DOR Desconhecimento científico – Omissão institucional – Representação social inexistente. O seminário foi muito rico nas demais participações, com destaque para o geneticista Dr. Jorge Sequeiros, que mostrou a complexa estrutura da Eurordis e as políticas internacionais para as doenças raras. Mais informação em: http://www.ces.uc.pt/eventos/index.php?id=10292&id_lingua=1&pag=10294 Final da reunião com a Associação Portuguesa de NF em Lisboa. Em Lisboa, fomos recebidos pela advogada Lucia Lemos, presidente da Associação Portuguesa de Neurofibromatoses e pela geneticista pediatra Dra. Isabel Cordeiro do Serviço de Pediatria do Hospital de Santa Maria, Lisboa. O encontro, no dia 24 de setembro de 2014, de 17.30 às 21 horas, foi denominado “À Conversa com Dr. Luiz Oswaldo”, no qual pude apresentar nossa experiência brasileira e realizamos uma proveitosa discussão sobre o enfrentamento das NF. Mais informações em: http://www.apnf.eu No retorno ao Brasil, apresentamos oralmente nossas impressões durante a reunião da Amanf de setembro, ocasião em que transmitimos nossa impressão de que as dificuldades enfrentadas pelas pessoas brasileiras com NF são bastante semelhantes àquelas encontradas por pessoas com NF de outros países. Acreditamos que as características competitivas, elitistas e injustas de uma sociedade de classes baseada na exploração do trabalho humano, agravam em muito o sofrimento natural causado pelas neurofibromatoses. A seguir, os resumos levados ao Congresso de Barcelona. Figure 1 – Some typical pictures of Second Toe Signal Phenotype in (at least) three criteria NF1 individuals – European NF Meeting Barcelona 2014 CODE 0269 Photographic prevalence of the Second Toes Signal phenotype in Neurofibromatosis Type 1 (NF1) Authors : Rodrigues LOC MD PhD; Diniz LM MD PhD; Cunha KGS PhD; Darrigo-Junior LG MD PhD; Passos RLF MSc; Geller M MD PhD; Rezende NA MD PhD. Institution/University: Neurofibromatosis Outpatient Reference Center, Federal University of Minas Gerais, Belo Horizonte, Brazil Background – Early seven-consensus criteria NF1 diagnosis is useful for clinical management of complications and genetic counseling. Any other specific congenital NF1 signal could help to assure NF1 diagnose. Our group previously reported a questionnaire prevalence of 12% of a new NF1 phenotype (1), which consists of the up righting of second toes of both feet, which we have nominated Second Toes Signal (STS). Aim – To verify the prevalence of STS by photographic recording in the first 200 NF1 individuals attained to an outpatient reference center compared to 200 random unaffected controls. Methods – A 187 NF1 volunteers (presenting at least three NIH diagnostic criteria) and 194 unaffected random volunteers controls have had their feet photographed and evaluated for STS presence, which was verified by four separated clinical doctors. Data was presented as positive frequency and it was compared using qui-squared test. Significance was set at P<0.05. Results – The mean four examiners consensus results were: STS was positive in 5.8% in NF1 volunteers and zero in unaffected controls (P<0.05). Conclusion – Photographic documentation and four examiners evaluation indicate that STS is probably a specific and congenital NF1 signal that could be useful to help early diagnosis through clinical examination. Granting agencies: FAPEMIG, CAPES e CNPQ Figure 4 – Heat thermoregulatory autonomic responses model. EC: environmental conditions; TS: thermal stimulus; SR: sweat rate; TT: tympanic temperature used as an indirect measurement of central nervous system temperature; CT: cutaneous temperature; HR: heart rate used as an indirect measurement of cardiac sinus rhythm; AP: arterial pressure (systolic: used as an indirect measurement of cardiac contractility – diastolic: used as an indirect measurement of active vasodilation); HTC: Hypothalamic and other temperature modulator centers; PR: peripheral resistance. Arrows in red: sympathetic autonomic pathways responses to heat stimuli involves: 1) venous constriction; 2) increased heart rate; 3) increased cardiac contractility; 4) increased arterial vasoconstriction; 5) increased sweat rate (cholinergic); 6) increased arterial vasodilation (cholinergic/NO mediated). European NF Meeting 2014 – CODE 0268 Neurofibromatosis type 1 individuals have reduced heat tolerance. Authors: Luiz OC Rodrigues MD PhD, Luciana G Madeira MS; Juliana F Souza MD PhD; Renata LF Passos MS; Nilton A de Rezende MD PhD; Nilo RV Lima PhD. Institution/University: Neurofibromatosis Outpatient Reference Center, Federal University of Minas Gerais, Belo Horizonte, Brazil. Email: [email protected] Background: During increased environmental temperature and body metabolism, human internal temperature is maintained within a short-range through heat dissipation by sweat evaporation and cutaneous vasodilation. Some diseases impair thermoregulation, which increases the risk of heat injuries and death. Neurofibromatosis type 1 (NF1) skin lesions, neural dysplasia and lower aerobic capacity could influence both sweat and vascular responses to thermal stress. However, NF1 individuals’ heat tolerance is not known. Aims – To compare heat tolerance of NF1 with non-NF1 individuals. Methods – Volunteers were 14 males (M) and 11 females (F) with NF1, aged 16-57 years with 23 non-NF1 individuals (control group – CG) matched by sex, age, height and weight. Sweat was experimentally induced twice: 1) by pilocarpine 1% iontophoresis (PILO) and 2) by passive heating (HEAT), using lower-leg immersion into 42°C water during one hour in environmental temperatures 28-30°C. Paper filters were used to measure sweat rate (SR) in forearm, chest, back and tight and the number of active sweat glands (GSA) was counted using iodine-paper technique. Tympanic (TT) and mean skin (ST) temperatures, heat storage rate (HSR), heart rate (HR), and arterial pressure were recorded. Data are presented in mean ± SD, and significance was set at p<0.05. Results – NF1 groups displayed lower SR during PILO (forearm: MNF1=0.42±0.16 versus MCG=0.71±0.31 mg.cm-2.min-1) and during HEAT (forearm: MNF1=1.77±0.70 versus MCG=2.57±0.68 mg.cm-2.min-1); GSA was similar in PILO, but lower in NF1 in HEAT (MNF1=77±16 versus MCG=70±22 gland.m-2). NF1 showed larger increased TT (MNF1=0.75±0.33 MCG=0.32±0.13°C) during HEAT protocol. HSR was higher in NF1 (MNF1=3211.6±236.2 versus MCG=93.0±1171.4 J.min-1.m²) and there was a smaller diastolic pressure decrease in NF1 (MNF1=-1.69±4.29 versus MCG=-6.73±4.43 mmHg). This abstract contains only male data, but females results were identical in both NF1 and control individuals. Conclusion – NF1 individuals presented markedly reduced sweat response to pilocarpine and heating and impairment in thermal vasodilation response, which caused a higher heat storage and 0.6°C increased tympanic temperature. The results suggest that NF1 causes reduced thermoregulatory response (autonomic central and/or peripheral dysfunction?), which can lead to higher risk of heat illnesses during heat stress and/or exercise. Grant Acknowledgement: CAPES, CNPQ. Industry RD Associations Rare diseases Social mobilization/ knowledgment Politics NF ? NF Associations Society Title: Differences between the behavior of associations: Rare Disease versus Neurofibromatosis Authors : Rogério Lima Barbosa1;Oswaldo Luiz Carneiro Rodrigues2 Institutions : 1Center for Social Studies, University of Coimbra, Coimbra, Portugal, Fellow of CAPES BEX 10006-13/3; 2Neurofibromatosis Outpatient Reference Center, Federal University of Minas Gerais, Belo Horizonte, Brazil. Background: The growing movement to disclosure of rare diseases (RD) in the worldwide involves associations dealing with some particular rare disease, such as Neurofibromatosis (NF). It is not known whether these associations accompany similarly actions for promotion the information about diseases, mobilizing society and awareness of the political class realized by rare diseases associations (RDA). Aim: To compare the typical activities of associations of NF (ANF) with those developed by the RDA. Method: Data collection through interviews with leaders of ANF in Brazil and analysis in exposed sites of ANF and RDA in Brazil, Portugal and England. Results: The ADR working as an "umbrella" model, in order to address matters of various diseases. Financial resources are, almost entirely, the pharmaceutical and biotechnology industry. In contrast, the ANF have maintained by donations from individuals and / or entities and in the Brazilian reality; do not receive financial support from pharmaceutical or biotechnology industries. Possible causes for these differences of resources are RDA: 1) the perform advocacy work with the Government tends to favor the diseases that have drug treatments available; 2) the multiplicity of RD under the same conditions attains a larger number of individuals. For the ANF: 1) the focus of attention on a specific group of diseases, which do not have available medicines; 2) the lack of a common factor that can unite the ANF. There seems to be a certain gap between ANF and industry whose causes need further studies. As a hypothesis is that the interests of industry in research to study other matrix of disease, in particular cancer and the interest to building Bio banks. For greater inclusion of ANF in the movement of RDA is required convergence of actions to care beyond medication. Conclusion: There are important differences in mode of action between the ANF and RDA due to the low economic interest in NF.
Baixar