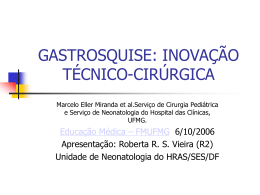
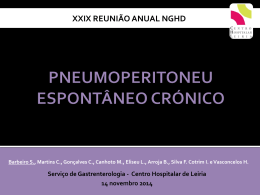
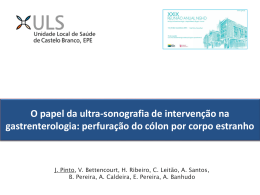
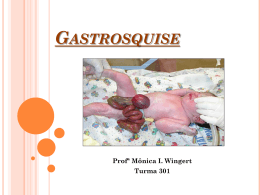
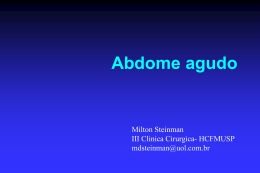
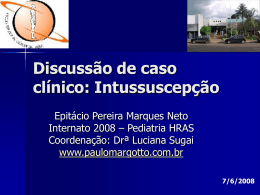
Historia da Medicina History of Medicine Barvalento Médico 2008; 1 (vol.1): 34-39 Bridas e aderências intestinais Visão histórica de um problema que se mantém actual Intra-abdominal adhesions Historical Vision of a current problem Daniel Cartucho Serviço de Cirurgia CHBA Barlavento Médico 34 1 Ellis H. The clinical significance of 2 3 4 5 6 7 8 adhesions: focus on intestinal obstruction. Eur J Surg Suppl, 1997;577: 5-9 Wilson MS, Hawkswell J, McCloy RF. Natural history of adhesional small bowell obstrution: counting the cost. Br J Surg 1998; 85: 1294-1298 Thompson JN, Ellis H, Parker MC et al. Surgical impact of adhesions following surgery in the upper abdomen. Br J Surg 1999; 86: 418-419 Herschlag A, Diamond MP, DeCherney AH. Adhesiolysis. Clin Obstet Gynecol 1991; 34:395-401 Angioli R, Barreau G. Interceed use and adhesion prevention in gynecology. Contemporary OB/GYN Archive 1998 Nov. http://obgyn.pdr.net/obgyn/public. htm?path=content/journals/g/data/1998/ gba/gba096.html 10 Van Der Krabben AA; Dijkstra FR; Nieuwenhuijzen M; Reijnen MM; Schaapveld M; Van Goor H. Morbidity and mortality of inadvertent enterotomy during adhesiotomy. Br J Surg 2000 Apr;87(4):467-71 Wiseman DM. Adhesion prevention: Past the future. In DiZerega GS (Ed.) Peritonea1 Surgery 2000 Springer-Verlag. pp:401-417 Correspondência | Correspondence [email protected] SUMÁRIO: Bridas e aderências intrabdominais são lesões já referenciadas nos papiros do antigo Egipto. Bem conhecida nos primórdios da patologia no contexto da tuberculosa ou outra doença inflamatória peritoneal, torna-se comum depois do advento da cirurgia abdominal na segunda metade do século XIX, pela obstrução intestinal que estas aderências pós-operatórias criam. É uma patologia que ainda hoje mantém importante morbilidade. O autor revê a evolução histórica desta doença e apresenta uma imagem dos primórdios do registo gráfico desta patologia. ABSTRACT: Knowledge of the existence of intraabdominal adhesions extends back to the ancient Egyptians. Well recognized by early pathologists following tuberculosis and other peritoneal inflammatory diseases, intestinal occlusion created by postoperative adhesions became a common complication after the advent of abdominal bowel surgery in the late 19th century. It still is considered to be the cause of important morbidity today. The author reviews the historical progression of this pathosis and presents a very early graphic image found. PALAVRAS CHAVE: Bridas, aderências intestinais, história KEY WORDS: Intra-abdominal adhesions, history INTRODUÇÃO INTRODUCTION Na segunda metade do século XX realizaram-se grandes avanços em praticamente todos os campos da Medicina. No entanto as consequências da patologia originada pelas bridas e aderências intra-abdominais, permaneceu praticamente inalterada. Sabemos hoje que estas membranas ou autênticos cordões de tecido fibroso que ligam vários órgãos intra-abdominais que normalmente não têm pontos fixos entre si lideram as causas de obstrução intestinal. São responsáveis por mais de 40% de todos os casos de obstrução intestinal 1 e de 60 – 70% do intestino delgado . Para além da oclusão intestinal que pode ocorrer no pós-operató2 rio imediato ou 34 anos após o acto cirúrgico , esta patologia é responsável ainda por quadros de dor abdominal, infertilidade – 15 a 20% desta é causada 3 4 5 pelas aderências – gravidez ectópica , dispareunia ou 6 isquémia intestinal . O conhecimento das adesões remonta igualmente ao antigo Egipto onde há registo de severas adesões pélvi7 cas num doente, embora não se sugira um tratamento . A descrição mais antiga de adesões em relação com lesão funcional de órgão, tanto quanto se conhece, é o registo no Talmud babilónio neste caso para adesões 8 pleurais . Ao longo do tempo, em particular na Idade Média, vai persistindo um debate acerca das adesões pleurais como causa ou consequência de perfuração. A partir de Hunter (1728-1793) temos estabelecida a rela- In the second half of the twentieth century, enormous advances were made in virtually all fields of medicine. However, on entering the twenty-first century, the graveness of the consequences of abdominal fibrosis, with its adherences and fibrotic bands, has remained practically unaltered. We know today that these membranes, or authentic fibrotic laces, bind the intra-abdominal viscera that normally do not have fixed points between each other leading to intestinal occlusion. These membranes are responsible for 60-70% of all small bowel disease and more than 40% of all the cases 1 of intestinal occlusion . Intestinal occlusion can occur in the immediate postoperative period or 34 years 2 after surgery . It is still responsible for abdominal pain, 3 infertility (15 to 20% are caused by adhesions) , ectopic 4 5 6 pregnancy , dispareunia and intestinal ischemia . The knowledge of adhesions retraces equally to ancient Egypt where a case of severe pelvic adhesions in a sick person is registered on papyrus, although there is 7 no suggestion of a treatment . The oldest description of adhesions in relation with functional organ injury, as far back as is known, is a register in the Babylonian 8 Talmud of a case of pleural adhesions . Throughout evolution, with particular reference to the Medieval Age, the debate persisted concerning pleural adhesions as a cause or a consequence of perforation. From Hunter (1728-1793), we established the relationship Fig. 1 - Um caso de gestação peritoneal retida. In Thivet M. Maladies du péritoine – Grossesse péritonéale, morte au bout de dix-huit ans. In Anatomie pathologique du corps humain. Ed. J Cruveilhier, Tome second, Livraison XXXVII, Libraire de l’Academie Royale de Medicine, 1843, Paris. A case of retained peritoneal gestation 9 Von Dembowski T (1889) Ueber die Ursachen der peritonea¬len Adhãsionen nach chirurgischen Eingriffen mit RUcksicht auf die Frage des Ileus nach Laparotomien. Langenbecks Arch Chir 37: 745 citado por Treutner KH, Schumpelick V. Adhäsionsprophylaxe – Wunsch und wirklichleit (Adhesions prevention – wish and reality) Chirurg (2000) 71: 510-517 10 Ellis H. Adhesions: the early history. Hospital Medicine, Vol. 65, Iss. 6, 10 Jun 2004, pp 328 - 329 11 Bryant T (1872) Clinical lectures on intestinal obstruction. Med Times Gaz 1: 363 citado por Treutner KH, Schumpelick V. Adhäsionsprophylaxe – Wunsch und wirklichleit (Adhesions prevention – wish and reality) Chirurg (2000) 71: 510-517 1 ção entre as adesões, peritonite e infecção . Danbarski em 1889, descreve causas de adesividade peritoneal pós-operatórias, com ênfase das localizadas ao íleo e concluiu, com base num trabalho experimental no cão, que eram induzidas tanto pelos fios de compressas, 9 como pela escarificação do intestino . Estas bridas que podem ser congénitas são normalmente secundárias a um processo intrabdominal como uma cirurgia, uma inflamação ou um trauma. Estas lesões referenciadas nos primórdios da patologia no contexto da tuberculosa ou outra doença inflamatória peritoneal, tornam-se comuns depois do advento da cirurgia abdominal na segunda metade do século XIX, pela obstrução intestinal que estas aderências pós-ope10 ratórias criam . Brant em 1897, descreve um caso de adesividade no íleo depois de exerése de quisto do ová11 rio . Payr em 1911, descreve a relação entre as adesões a fibrinólise e a importância das primeiras 48 h para a 12 formação destas aderências . Posteriormente, utilizou a expressão “problemas de adesividade peritoneal” chamando a atenção da maior relevância do problema pelo maior número de laparotomias que cirurgiões e ginecologistas praticavam. Valoriza a lesão da mucosa pelo trauma na laparotomia asséptica e a lesão do peritoneu pela falta de humidade, lesões químicas e térmicas. Ao longo dos anos vão sendo propostas uma série de soluções para evitar a formação destas aderências. Wiseman8 em 2000 dá-nos uma visão ampla do tema e 1 between the adhesions, peritonitis and infection . Danbarski, in 1889, described with basis on experimental 10 work on the dog , postoperative causes of peritoneal adhesions, emphasizing on adhesions located on the ileum, and concluded that adhesions could be induced by the gauze fibres as well as by intestinal scarifica10 tion . Brant, in 1897, described a case of adhesions 11 of the ileum after excision of an ovarian cyst . Payr, in 1911, described the relationship between adhesions, fibrinolysis and the importance of the first 48 hours 12 for the formation of these adhesions . The expression “problems of peritoneal adhesiveness” was later used by him to call attention to the great relevance of the problem through the large number of laparotomies that surgeons and gynaecologists were practising. He valued traumatic injury of the mucosa and peritoneal injury due to lack of moisture, chemical and thermal injuries in aseptic laparotomy. Congenital bands have been found to exist, but the great majority of all adhesions are secondary to some intra abdominal process such as a surgery, inflammation or intra-abdominal trauma. Adhesions following tuberculosis and other peritoneal inflammatory diseases were well recognized by early pathologists, but it was not until the advent of abdominal surgery in the 19th century that postoperative adhesions, and thus small bowel obstruction complications, became common. Through the years several proposals, for a series of solutions, were made to prevent these formations. Barlavento Médico 35 Fig. 2 - Thivet M. Maladies du péritoine – Grossesse péritonéale, morte au bout de dix-huit ans. In Anatomie pathologique du corps humain. Ed. J Cruveilhier, Tome second, Livraison XXXVII, Libraire de l’Academie Royale de Medicine, 1843, Paris. A case of peritoneal extrauterine gestation presenting an image of the embryo, restrained for 18 years, in the abdominal cavity. Barlavento Médico 36 reporta uma primeira tentativa para a resolução destas lesões motiva uma comunicação com a utilização de óleo de massagem para impedir a sua formação em 1880s. Depois, respectivamente em 1886 e 1889, tanto Muller como Malcolm, descreveram a utilização de soluções salinas para “float the intestines”. Conceito que como iremos verificar mantém toda a actualidade. Um agente chamado “fibrinolysin” (tiosinarnine e salicilato de sódio) foi introduzida em 1892, mas não teve eficácia e caiu em desuso. A goma-arábica foi recomendada como “lubricant between the viscera” em 1902, e em 1905, a Johnson and Johnson lançou no mercado uma preparação de peritoneu cecal bovino (disponível até 1993). Desde então, uma grande variedade de substâncias, algumas bem exóticas, tem sido utilizada numa tentativa de evitar a formação destas adesões pós-operatórias: intestino grosso de touro, peritoneu de tubarão, lanolina, bílis, membrana amniótica, bexiga de peixe, retalhos de epiploon e múltiplas películas. IMAGEM NOTÁVEL DE 1839 A Anatomia ciência morfológica do estudo da arquitectura do corpo baseado na dissecação, legou à História da Medicina tratados com excepcionais ilustrações. Disciplina muito tempo limitado aos dados de Galeno (129-200), iria ter um novo impulso na Idade Média a que se juntou com a dinâmica trazida pela impressa de Gutenberg, cerca de 1450. Vários autores publicam tratados de anatomia com ilustrações. De entre estes André Vesálio publica em 1543 De humani corporir fabrica, obra notável de anatomia tanto no plano conceptual com estético e chegamos ao século XIX com um corpo de excepcionais tratados de anatomia. Nessa altura com a litografia era possível publicar “sem demasiados encargos, obras iconográficas muito volumosas (…) um favor aos médicos colocar ao alcance de todos o conjunto dos trabalhos que tiveram 13 a anatomia como objecto” . Estamos nos inícios dos anos 1880s, a anatomia encontrava-se no seu apogeu e escrevia-se: “Sem a anatomia a fisiologia é apenas um tecido de fábulas mais ou menos engenhosas, a cirurgia encontra-se sem orientação e a medicina está reduzida 13 a um empirismo cego” . É patente o primado existente então da anatomia entre as disciplinas médicas e na evolução dos conceitos científicos. A anatomia patológica faz igualmente o seu percurso e entre 1828 e 1842 Léon Jean Baptiste Cruveilhier publica em Paris um memorável tratado Anatomie pathologique du corps humain. A Cruveilhier (17911874) foi conferido o título de doctor de medicina em Paris, em 1816, com uma dissertação com uma nova classificação de órgãos de acordo com suas alterações patalógicas. Em 1830 torna-se director do Hospice de la Maternité, mais tarde Salpêtrière e Charité, e em 1836 tornou-se o primeiro catedrático da cadeira de anatomia patalógica, que tinha sido estabelecida pelo 14 seu professor, Dupuytren . Dedicando sempre um A first attempt for its resolution, in 1880s, motivated a paper on the use of massage oil to hinder the formation of adhesions. In 1886, Muller spoke of the use of a saline solution and in 1889; Malcolm described the use of fluid to “float the intestines”. This concept, we go on to verify, is pertinent today. In 1892, an agent called “fibrinolysin” (sodium tiosinarnine and salicylate) was introduced, but it was not effective and fell into disuse. The gum-Arabic was recommended as a “lubricant between the viscera” in 1902, and in 1905, Johnson and Johnson launched, on the market, a preparation of bovine peritoneal cecum (available up to 1993). Since then, a great variety of substances, some quite exotic, have been used in an attempt to prevent the formation of these postoperative adhesions: large intestine from bulls, shark peritoneum, lanoline, bile, amniotic membrane, fish bladder, strips of epiploon and multiple films. A SINGULAR IMAGE FROM 1839 Anatomy, the morphologic science of the study of the architecture of the body based on dissection, bequeathed to the History of the Medicine compendiums with exceptional illustrations. Long limited to Galen’s data (129-200), anatomy would go on to have a new impulse in the Medieval age with the Gutenberg prints cerca 1450. Various authors publish illustrated compendiums of anatomy. Among them, Andres Vesálio publishes, in 1543, De humani corporir fabrica, a highly notable work on anatomy in its conception as well as aesthetically. We arrive at XIX century with a body of exceptional textbooks on anatomy. At this point, with lithography, it was possible to publish “without too much expense, voluminous iconographic compendiums (…) as a favour to doctors to place, within reach of all, the object of a set of works of anatomy”. We are at the beginnings of the 1880s, anatomy was at its epitomy and thus was written: “Without anatomy, physiology is just a weaving of more or less ingenious tales, surgery finds itself without orientation 13 and medicine is reduced to blind empirism” . The existing primacy of anatomy then is evident amongst the medical disciplines and in the evolution of scientific concepts. Pathological anatomy equally follows suit between 1828 and 1842. Léon Jean Baptiste Cruveilhier publishes, in Paris, a memorable compendium on Anatomie pathologique du corps humain. Cruveilhier (1791-1874) was conferred with the title of Doctor of Medicine, in Paris in 1816, for his dissertation on a new classification of organs according to pathological alterations. In 1830 he became physician-in-chief and director of the Hospice de La Maternité, later Salpêtrière and the Charité, and in 1836, he became the first Professor to hold the chair of pathological anatomy, which had been established by his Professor, 14 Dupuytren . Always dedicating great interest to DISCUSSÃO 12 Payr E (1924) Biologisches zur Ents- 13 14 15 16 tehung, Rtickbildung und Vorbeugung von Bauchfel lverwachsungen. Zentralbl Gyniikol 14: 718 citado por Treutner KH, Schumpelick V. Adhäsionsprophylaxe – Wunsch und wirklichleit (Adhesions prevention – wish and reality) Chirurg (2000) 71: 510-517 Bourgery JM, Jacob NH. Traité complet de l’anatomie de l’homme. Na Edição Taschen Gmbh 2006 http://www.whonamedit.com/doctor. cfm/892.html http://www.cosmovisions.com/Cruveilhier.htm Thivet M. Maladies du péritoine – Grossesse péritonéale, morte au bout de dix-huit ans. in Anatomie pathologique du corps humain. Ed. J Cruveilhier, Tome second, Livraison XXXVII, Libraire de l’Academie Royale de Medicine, 1843, Paris. O peritoneu com uma superfície de 10,000 cm2 no adulto, quase igual à superfície da pele, diminui a fricção entre as vísceras abdominais permitindo o seu movimento livre. Apresenta à superfície células mesoteliais altamente diferenciadas e é a este nível que, após um factor desencadeante, por exemplo um acto cirúrgico, ocorre aquela cascata de eventos que pode confluir para a formação de bridas e aderências. Estas podem ser responsáveis por um cortejo de sintomatologia que pode ir da dor abdominal à oclusão intestinal. O seu diagnóstico é em larga medida confirmado intra-operatoriamente, já que não dispomos de exames complementares de diagnóstico para a sua identificação. Pela sua natureza não visualizamos estas lesões, só identificamos o seu rebate. No século XX a maior parte de tipos de materiais actualmente em utilização ou em desenvolvimento foram propostos para prevenção das aderências: líquidos, geles, barreiras, drogas fibrinolíticos, polímeros hidrossoluveis e polímeros orgânicos. No entanto após um período inicial de algum entusiasmo a prática não consagrou a sua utilização. E voltamos mesmo assumir uma referência prévia com o conceito “flot the intesti- Anatomy, his days were spent within the school pavilion laboratories, gathering material for the works on Anatomie Pathologique du Corps Humain (1828-1842) and the Traité D’Anatomie Pathologique Générale (1849-1864). Cruveilhier’ s claims fame for his remarkable illustrations, even today, and establishes a first and magnificent attempt to popularize anatomo-pathological science through its accessibility of loyal images of 15 the lesions . This chapter shows a truly notable image 1. The author describes a case of peritoneal extrauterine gestation presenting an image of the embryo, restrained 16 for 18 years, in the abdominal cavity . Shown are 3 adhesions, using the expressions adhesions and tacks. It describes the neovascularization observed in the membranes presents an image of the great severity of these injuries. “on voit qu’il est encore recouvert de ses envelopes primitives, qui, après s’ètre appliquées etroitement sur lui, se porolongent sous forme de brides, et vont se fixer aux colons ascendant et transverse, en se continuant insensiblement avec le péritoine (…) La partie médiane et occipitale de la tête donne insertion à un grand nombre de cês brides (…) et qui vont s’insérer d’autre au cólon ascendent; elles m’ont paru organisées, car j’ai pu y constater la presénce de vaisseaux et de petits paquets graisseux de la grosseur d’une noisette (…) Tous ces prolongemens que nous retrouverons encore aux pieds AF, servaient de moyens de suspension à l’enfant dans la cavité abdominale.” DISCUSSION The peritoneum with a surface area of 10,000 cm2 in the adult, almost equal to the surface of the skin, reduces the friction between abdominal viscera permitting its free movement. On the surface are highly differentiated mesothelial cells. It is on this level that, a surgical act sets off a cascade of events that flows toward the formation of membranes and adhesions. These can be responsible for a parade of symptoms which can go from abdominal pain to intestinal occlusion. Its diagnosis is, in wide measure, confirmed on surgery since there are no diagnostic procedures available for its identification. Due to the nature of these formations we cannot see them, unless directly due to their effect. In the XX century, most of the types materials in use or under development currently considered for prevention of adhesions: liquids, gels, barriers, fibrinolytic drugs, water soluble polymers and organic polymers. However, after some initial enthusiasm, experience did not consecrate its use. We go back to assume a previous reference on the concept of “floating the intestines”. In fact if we maintain the intestines and abdominal organs in a solution that keeps them in movement, the injured peritoneal surfaces cannot adhere to form membranes and adhesions. For this purpose, a solution used in dialysis is being proposed 37 Barlavento Médico grande interesse à Anatomia passava os seus dias nos pavilhões da Escola prática, recolhendo os materiais para as obras Anatomie Pathologique du Corps Humain (1828-1842) e o Traité D’Anatomie Pathologique Générale (1849-1864), Cruveilhier assenta a sua fama nas suas illustrações, notáveis ainda hoje, bem como o estabelecimento do que constituí a primeira e magnifica tentativa de vulgarização da ciência anatomo-patolo15 gica pela acessibilidade da imagem fiel das lesões . De entre as “diversas alterações mórbidas susceptíveis de ocorrer no corpo humano”, apresenta-nos em 1839, no segundo tomo da obra, um capítulo por Thivet M. com o título: Maladies du péritoine – Grossesse péri16 tonéale, morte au bout de dix-huit ans . Neste texto o autor descrevendo um caso de gestação peritoneal, apresenta uma imagem verdadeiramente notável do feto retido, durante 18 anos, na cavidade abdominal por gestação extra-uterina. Exibem-se várias aderências nesta estampa de grande rigor destas lesões. “on voit qu’il est encore recouvert de ses envelopes primitives, qui, après s’ètre appliquées etroitement sur lui, se porolongent sous forme de brides, et vont se fixer aux colons ascendant et transverse, en se continuant insensiblement avec le péritoine (…) La partie médiane et occipitale de la tête donne insertion à un grand nombre de cês brides (…) et qui vont s’insérer d’autre au cólon ascendent; elles m’ont paru organisées, car j’ai pu y constater la presénce de vaisseaux et de petits paquets graisseux de la grosseur d’une noisette (…) Tous ces prolongemens que nous retrouverons encore aux pieds AF, servaient de moyens de suspension à l’enfant dans la cavité abdominale.” Barlavento Médico 38 nes”. De facto se mantivermos os intestinos e órgãos intra-abdominais com uma solução que os mantenha com movimento não permitimos a junção de duas superfícies peritoneais lesadas que possam levar à formação de bridas. Para este fim vem sendo proposto o uso de solução utilizada na diálise que se mantém no abdómen por um período de cerca de 5 dias, antes da sua reabsorção. No texto que descrevia o caso da gestação intraperitoneal retida verificamos que há cerca de 180 anos atrás se utilizava uma nomenclatura, bridas e aderências, que se mantém actual. Por outro lado a noção de maturidade das bridas, já está igualmente presente nesse texto. Sabemos hoje que a maturidade pode condicionar a sua classificação Histológica e Macroscópica. A neovascularização que o autor tão bem assinala é factor de verificação na classificação Histológica das bridas de 17 Zuhlke . De acordo com a sua classificação Macroscópica que se refere à facilidade com que se liberta as aderências, desde uma película que se separa com facilidade por dissecção romba (grau I) ou onde a sua lise só é possível por dissecção com tesoura ou bisturi e onde a libertação do órgão previsivelmente acarreta a sua lesão (grau IV) a maturidade proporcionada pelo tempo que já levam desde a sua formação, deixa antever uma consistência que está de acordo com a sua observação:”serviam de meios de suspensão da criança na cavidade abdominal”. São lesões que tal como então ainda hoje nos confrontamos quotidianamente. Na imagem 3 verificamos a ansa do delgado atingida, depois da lise de brida unica, numa operação de Janeiro de 2007. Este é um campo que vem merecendo a atenção de muitos investigadores. Utilizando duas citações poderemos dizer, em conclusão, que nesta patologia oscilamos hoje entre uma constatação e um desejo. Por um lado “as aderências desde sempre fizeram parte da vida de um doente cirúrgico bem como do cirurgião. O cirurgião aceita a formação destas aderências como uma lesão inevitável, assim como algo que pode ser controlado tão facilmente como o tempo que fará 18 amanhã” . Por outro “as feridas convivem com a humanidade desde o seu início. A evolução na cura não pode ser deixada em paz com a moderna tecnologia. O grau de inflamação e fibrose necessária em tempos 19 pré-históricos pode ser excessiva hoje” . which remains in the cavity for a period of five days before being absorbed. In the text which described the case of the retained intra peritoneal gestation, 180 years ago, we verified the use of the nomenclature, adhesions and membranes, still used today. On the other hand, the notion of the maturity of membranes is equally present in that text. We understand today that maturity can condition its histological and macroscopic classification. In the second half of the twentieth century enormous advances were made in virtually all fields of medicine. Nevertheless, we have entered the twenty-first century and the situation concerning the gravity of the consequences of abdominal fibrosis, with its adherences and fibrotic bands, has remained practically unaltered. Neovascularization, which the author so well remarks, is a factor which is verified in the Zuhlke histological classification of membranes. In agreement with his macroscopic classification which refers to the ease with which the membranes are freed, from the membrane which is separated with ease through rhombus dissection (grade I), or its lysis only possible through dissection with scissors or scalpel blade where the freeing of the organ will provoke its lesion (grade IV). The maturity proportioned by time evolved from its formation allows the foresee all of a consistency in accordance with its observation: “the use of the means of suspension of the child in the abdominal cavity” Lesions, which just as before, still confront us today. In image 3, we verify that the small intestine segment affected, after lysis of the only membrane, in an operation in January of 2007. This is an area which has received the attention of several investigators. Citing two quotes, we could say that, in conclusion, in this pathology we swing today between acknowledgement and desire. On the one hand “adhesions have always been part of the life of the surgical patient and of the surgeon. The surgeon accepts the formation of these adhesions as inevitable, something so easily controlled as the weather 18 tomorrow” . On the other hand “wounds are familiar to humanity since the beginning. The evolution of healing has not kept up with modern technology. The degree of inflammation and fibrosis necessary in pre 19 historic times can be excessive today” . Fig. 3 - Imagem II. Ansa do intestino delgado atingida, depois da lise de brida única. Vídeo - wwww.chbalgarvio.min-saude.pt/barlavento_medico Referências | References 39 Barlavento Médico 1.Ellis H. The clinical significance of adhesions: focus on intestinal obstruction. Eur J Surg Suppl, 1997;577: 5-9 2. Wilson MS, Hawkswell J, McCloy RF. Natural history of adhesional small bowell obstrution: counting the cost. Br J Surg 1998; 85: 1294-1298 3. Thompson JN, Ellis H, Parker MC et al. Surgical impact of adhesions following surgery in the upper abdomen. Br J Surg 1999; 86: 418-419 4. Herschlag A, Diamond MP, DeCherney AH. Adhesiolysis. Clin Obstet Gynecol 1991; 34:395-401 5. Angioli R, Barreau G. Interceed use and adhesion prevention in gynecology. Contemporary OB/GYN Archive 1998 Nov. http://obgyn.pdr.net/obgyn/public.htm?path=content/journals/g/ data/1998/gba/gba096.html 6. 10 7. Van Der Krabben AA; Dijkstra FR; Nieuwenhuijzen M; Reijnen MM; Schaapveld M; Van Goor H. Morbidity and mortality of inadvertent enterotomy during adhesiotomy. Br J Surg 2000 Apr;87(4):467-71 8. Wiseman DM. Adhesion prevention: Past the future. In DiZerega GS (Ed.) Peritonea1 Surgery 2000 Springer-Verlag. pp:401-417 9. Von Dembowski T (1889) Ueber die Ursachen der peritonea¬len Adhãsionen nach chirurgischen Eingriffen mit RUcksicht auf die Frage des Ileus nach Laparotomien. Langenbecks Arch Chir 37: 745 citado por Treutner KH, Schumpelick V. Adhäsionsprophylaxe – Wunsch und wirklichleit (Adhesions prevention – wish and reality) Chirurg (2000) 71: 510-517 10. Ellis H. Adhesions: the early history. Hospital Medicine, Vol. 65, Iss. 6, 10 Jun 2004, pp 328 - 329 11. Bryant T (1872) Clinical lectures on intestinal obstruction. Med Times Gaz 1: 363 citado por Treutner KH, Schumpelick V. Adhäsionsprophylaxe – Wunsch und wirklichleit (Adhesions prevention – wish and reality) Chirurg (2000) 71: 510-517 12. Payr E (1924) Biologisches zur Entstehung, Rtickbildung und Vorbeugung von Bauchfel lverwachsungen. Zentralbl Gyniikol 14: 718 citado por Treutner KH, Schumpelick V. Adhäsionsprophylaxe – Wunsch und wirklichleit (Adhesions prevention – wish and reality) Chirurg (2000) 71: 510-517 13. Bourgery JM, Jacob NH. Traité complet de l’anatomie de l’homme. Na Edição Taschen Gmbh 2006 14. http://www.whonamedit.com/doctor.cfm/892.html 15. http://www.cosmovisions.com/Cruveilhier.htm 16. Thivet M. Maladies du péritoine – Grossesse péritonéale, morte au bout de dix-huit ans. in Anatomie pathologique du corps humain. Ed. J Cruveilhier, Tome second, Livraison XXXVII, Libraire de l’Academie Royale de Medicine, 1843, Paris. 17. Zuhlke HV, Lorenz EMP, Straub EM, Savvas V. Pathophysiologie und klassifikation von adhasionen. Langenbecks Arch Chir Suppl II (Kongressbericht 1990): 1009-1016. citado por Luijendijk RW, Foreign material in postoperativa adhesions. Ann Surg 1996; 223: 242-248 18. Wolff B G. Invited Commentary to Parker MC, Ellis H, Moran BJ, et al. Postoperative Adhesions: Ten-Year Follow-Up of 12,584 Patients Undergoing Lower Abdominal Surgery. Dis Colon Rectum 2001 Jun; 44(6):822-830 19. Robson MC, Steed DL, Franz MG. Wound healing: Biologic features and approaches to maximize healing trajectories. Current Problems in Surgery February 2001; Vol.38. Number 2
Baixar