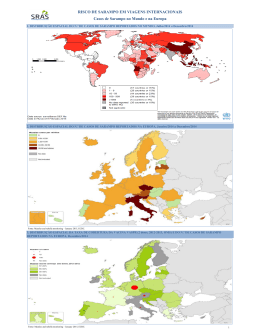
Controle de Doenças e Imunizações Sarampo Mariângela Ribeiro Resende Disciplina de Moléstias Infecciosas e Parasitárias Faculdade de Ciências Médicas da Unicamp Sarampo • Porque o sarampo ainda não foi eliminado se é evidentemente imunoprevinível? • Quais as dificuldades para atingir o controle e a eliminação ? • Quais as ações propostas pela OMS e as experiências nacionais? 2014: 3000 2014: 730 Porque o sarampo ainda não foi eliminado se é evidentemente imunoprevinível? África Sudeste asiático Pacifico oriental Porque o sarampo ainda não foi eliminado se é evidentemente imunoprevinível? Cobertura vacinal sarampo, 2013 Porque o sarampo ainda não foi eliminado se é evidentemente imunoprevinível? Transmissibilidade 5 antes e 5 após o exantema Sarampo Definição de caso suspeito de sarampo: “Todo paciente que, independente da idade e da situação vacinal, apresentar febre e exantema maculopapular, acompanhados de um ou mais dos seguintes sinais e sintomas: tosse e/ou coriza e/ou conjuntivite; ou todo indivíduo suspeito com história de viagem ao exterior nos últimos 30 dias ou de contato, no mesmo período, com alguém que viajou ao exterior” Frente ao caso suspeito de sarampo - Notificação imediata - Coleta de espécimes clínicos (sangue, secreção nasofaríngea e urina) para a realização do diagnóstico laboratorial - Medidas de controle (bloqueio vacinal seletivo frente aos casos suspeitos e sua ampliação na presença de sorologia reagente) - Precauções para aerossóis Porque o sarampo ainda não foi eliminado se é evidentemente imunoprevinível? Complicações da doença • Otite média: 7-9% • Pneumonia : 1-6% • Diarreia: 8%, • Encefalite: 1/ 1.000 - 2.000 • Panencefalite esclerosante subaguda Porque o sarampo ainda não foi eliminado se é evidentemente imunoprevinível? B3: Filipinas Sarampo: distribuição genótipos 2014 696 730 Sarampo no Estado de São Paulo 2000: ausência de circulação endêmica 2014: 7 casos GVE – Santo André (um caso), Sudeste Asiático GVE – Campinas (um caso) Ceará MSP – 5 casos (2 isolados e 3 familiar) Europa, sem registro viagem em 4 Não vacinados ou sem vacina Quais as ações propostas pela OMS? Cobertura uniforme de 95% para garantia de eliminação! Vacinar, vacinar, vacinar Quais as ações propostas pela OMS? Mitos e realidades sobre a vacina •Vacina de vírus vivos cultivada em fibroblasto embrião de galinha • Sorbitol, gelatina e neomicina NÃO CONTEM TIMEROSAL • Eficácia (90-95%) – falha primária 5% • Recomendação de duas doses • Imunidade longo prazo • Estudos demonstrando segurança SCR (MMR) crianças alérgicas a ovo Quais as ações propostas pela OMS? Mitos e realidades sobre a vacina Grupos prioritários 2 doses: - cças e adolescentes - profissionais/voluntários Saúde Educação Turismo - viajantes para áreas de risco No mínimo 1 dose: - adultos nascidos após 1960 (Ex. oportunidade puerpério) Editor's Choice The fraud behind the MMR scare BMJ 2011; 342 The original paper has received so much media attention, with such potential to damage public health, that it is hard to find a parallel in the history of medical science. Many other medical frauds have been exposed but usually more quickly after publication and on less important health issues. I am struck by Deer’s comparison, in an accompanying blog, between Wakefield’s fraud and Piltdown man, the paleontological hoax that led people to believe for 40 years that the missing link between man and ape had been found. Science is based on trust. Without trust, research cannot function and evidence based medicine becomes a folly. Journal editors, peer reviewers, readers, and critics have all based their responses to Wakefield’s small case series on the assumption that the facts had at least been honestly documented. Such a breach of trust is deeply shocking. And even though almost certainly rare on this scale, it raises important questions about how this could happen, what could have been done to uncover it earlier, what further inquiry is now needed, and what can be done to prevent something like this happening again.. doi: http://dx.doi.org/10.1136/bmj.d22 (Published 06 January 2011) Quais as ações propostas pela OMS? Mitos e realidades sobre a vacina Studies looking at measles, mumps, and rubella (MMR) vaccine: No Evidence for Measles, Mumps, and Rubella Vaccine-Associated Inflammatory Bowel Disease or Autism in a 14-year Prospective Study Peltola H et al. Lancet. 1998; 351:1327-8 Prospective study of 3 million adverse events in temporal relation to MMR vaccine. A form was filled and posted to the data collectors, followed by another form with further information 2-3 weeks later. Researchers traced subjects who developed gastrointestinal symptoms or signs lasting 24 hours or more at any time after MMR vaccination (apart from within the first hour). Researchers also checked hospital and health center records or interviewed the local public-health nurses. AUTHOR CONCLUSION: Over a decade’s effort to detect all severe adverse events associated with MMR vaccine could find no data supporting the hypothesis that it would cause pervasive developmental disorder or inflammatory bowel disease. http://www.freenetpages.co.uk/hp/gingernut/lancet/Finland%20May%201998.pdf Quais as ações propostas pela OMS? Mitos sobre a vacina Autism and Measles, Mumps, and Rubella Vaccine: No Epidemiological Evidence for a Causal Association Taylor B et al. Lancet. 1999;353 (9169):2026-9 Researchers looked for a change in trend in incidence or age at diagnosis associated with the introduction of measles, mumps and rubella (MMR) vaccination to the United Kingdom in 1988. The study identified 498 cases of autism (261 of core autism, 166 of atypical autism, and 71 of Asperger syndrome) in children born in the UK since 1979. There was a steady increase in cases by year of birth with no sudden “step-up” or change in the trend line after the introduction of MMR vaccination. There was no difference in age at diagnosis between the cases vaccinated before or after 18 months of age and those never vaccinated. There was no temporal association between onset of autism within 1 or 2 years after vaccination with MMR. Developmental regression was not clustered in the months after vaccination. AUTHOR CONCLUSION: Data do not support a causal association between MMR vaccine and autism. If such an association occurs, it is so rare that it could not be identified in this large regional sample. http://tinyurl.com/5bgvwg Quais as ações propostas pela OMS? Mitos e realidades sobre a vacina Measles-Containing Vaccines and Febrile Seizures in Children Age 4 to 6 Years Klein N, et al., Pediatrics. 2011; 129(5): 809-14 715,484 children Researchers chose to perform cohort study and included aged 48-83 months of age who received a dose of MMRV, a dose of MMR on the same day as a dose of Varicella injected separately, or MMR alone or Varicella alone to determine the risk of post-vaccination seizure in these groups. Results showed that more fevers and seizures did occur in children who had received the MMRV vaccine, compared with children who had received MMR + Varicella, or MMR or Varicella separately, though this finding was not statistically significant. The study did not find any peak in seizure or fever activity in any of the study groups in the 7-10 post-vaccination period. Of the 4 febrile seizures observed in the 7-10 days in the post-vaccination period for children receiving MMRV, only one febrile seizure could be confirmed, resulting in authors claiming the rate of febrile seizure after MMRV to be 1 in 86,750 doses. AUTHOR CONCLUSION: Overall researchers found the study groups within 6 weeks of vaccination. no increased risk of febrile seizures in any of http://pediatrics.aappublications.org/content/129/5/809 Imunidade presumida • Documentação escrita de vacinação adequada • Evidência laboratorial de imunidade (sorologia) • DN < 1960 • Confirmação laboratorial da doença (sorologia ou PCR +) Medidas Estado de São Paulo Campanha de intensificação novembro de 2014 não atingiu a meta de 95%. Monitoramento rápido da cobertura vacinal (MRC) pós-campanha de intensificação: RESGATAR OS NÃO VACINADOS, no sentido de ampliar e fortalecer a cobertura e sua homogeneidade em todo território paulista. Documento elaborado e atualizado pela Equipe Técnica da DDTR/CVE/CCD/SES-SP, em 30 de março de 2015, São Paulo, Brasil. Metas da OMS 2020 Eliminação em cinco regiões da OMS Alta cobertura vicinal com duas doses de vacinas SR Vigilância efetiva, avaliação programática das atividades de vacinação Preparo para resposta rápida e controle de epidemias Comunicação e engajamento público demanda por imunização Pesquisa ações custo-efetivas para aprimorar a vacinação e os métodos diagnósticos Obrigada pela atenção!
Baixar