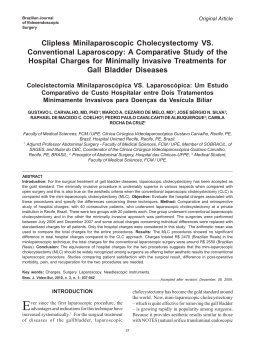
Close this window to return to IVIS www.ivis.org ABSTRACTS ISCFR 2012 July 26‐29, Whistler, Canada th 7 International Symposium on Canine and Feline Reproduction In a joint meeting with EVSSAR 2012 15th Congress of the European Veterinary Society for Small Animal Reproduction Editors: Gary England, Michelle Kutzler, Pierre Comizzoli, Wojciech Nizanski, Tom Rijsselaere and Patrick Concannon Reprinted in IVIS with the permission of the ISCFR Organizers Reprinted in IVIS with the permission of the Organizers Close window to return to IVIS Video-assisted ovariohysterectomy in domestic cats (Felis catus) using two portals Tavares, DC1; Souza, FF2; Quarterone, C2; Rodrigues, V2; Pereira, LF2 and Toniollo, GH1 1 Departamento de Medicina Veterinária Preventiva e Reprodução Animal da Universidade Estadual Paulista (FCAV/UNESP), Via de Acesso Prof. Paulo Donato Castellane s/n, Postal Code 14884-900, Jaboticabal, SP, Brasil. 2 Hospital Veterinário, Universidade de Franca – UNIFRAN, Av. Dr. Armando Sales de Oliveira, 201, Postal Code 14404600 - Franca, SP, Brasil. [email protected] OBJECTIVES AND METHODS: The laparoscopic surgery as well video-assisted surgery are not novel surgical modalities, but additional options to conduct a surgical procedure, thereby requiring an adaptation phase (1). The major disadvantage of laparoscopy is the high cost of equipment; require more than one surgeon to perform; and the progress in the learning curve (2). The search for techniques to facilitate laparoscopy and is suitable for the animal size has been the subject of several studies. Thus, the objective of this study was to evaluate the feasible of video-assisted ovariohysterectomy in cats using two portals. Fifty two healthy queens, weighing more than 2.0 Kg and aged 1.5 years were used. All procedures were performed by the same surgeon. The females were anesthetized and the abdomen was insufflated to a maximum pressure of 8 mmHg with CO2 gas using a 5 mm cannula with valve (first trocar), which was positioned in the cranial region to umbilical scar (Figure 1). Then, the endoscope (5 mm, 0°) was introduced in first trocar. The second trocar was placed in the midline of pre-pubic region. The female was turned to lateral position to show the uterine horn and right ovary. A Babcock forceps was introduced in the second trocar to elevate and to fix (transcutaneous external suture) the uterine horn and ovary up to lateral region of abdominal wall. The ovary suspensory ligament was disrupted with Babcock forceps and the ovarian pedicle was cauterized on three parallel points with a bipolar electrocautery forceps. Pedicle was sectioned in the middle cauterized portion. The same procedure was carried out in left pedicle. The queen was repositioned in dorsal supine and ovaries pulled through the second trocar. The uterine body exposed was transfixed using mononylon and sectioned. The two incisions were sutured. RESULTS: The mean and standard deviation of total surgical time was 41.4 14.2 minutes. All females had adequate recovery from anesthesia, without excitement or complications. We have found the following complications: hemorrhage (1.9%), hypotension (7.7%), subcutaneous emphysema (7.7%), dehiscence (1.9%), hematoma (1.9%) and conversion to laparotomy (13.5%). CONCLUSION: The complications were similar to findings of Solomon et al. (3), which reported decrease of the surgical time, and complications after the first 10 procedures, remaining stable in next. The conversion of the videosurgery to laparotomy was a major complication and according to Adikibi et al. (5) should not be considered a complication but an attribute to the learning curve. In this study was used only two trocars because the abdomen of the cats is small, which justifies the reduction in the portal numbers (5). The transcutaneous external suture dispensed the third trocar, a technique previously shown in dogs (6). The video-assisted surgery using two portals, described in this study was adequate and safe for performing ovariohysterectomy and it can be an additional option to domestic cats. (1) Buess G, Creuz O. Treinamento em cirurgia vídeo-endoscópica. In: Creuz O. Manual de Cirurgia Vídeo Endoscópica. Rio de Janeiro: Revinter, 1993:53-69. (2) Brun MV, Beck CAC. Aplicações clínicas e experimentais da laparoscopia em cães – artigo de revisão. Uruguaiana: Revista FZVA 1998/1999; 1:5-11. (3) Solomon D, Bell RL, Duffy AJ, Roberts KE. Single-port cholecystectomy: small scar, short learning curve. Surg Endosc, 2010; 24:2954-57. (4) Adikibi BT, Mackinlay GA, Munro FD, Clarck C. Is Conversion a Complication of Laparoscopic Surgery? J Laparoendosc Adv Surg Tech Null, 2008; 0:1-4. (5) Costa Neto JM, Teixeira RGA, Baraúna ALI, Gordilho Filho AO, Baraúna LCRI. Ovarisalpingohisterectomia laparoscópica em cadelas. Uberlândia: Vet Not, 2006; 12:79-86. (6) Ataíde MW, Brun MV, Barcellos LJG, Bortoluzzi M, Feranti JPS, Santos FR, Tomazzoni F, Brambatti G, Zílio PP, Oro G, Sartori LW, Monteiro AR, Zanella R. Ovariosalpingohisterectomia video-assistida ou convencional em cadelas com o uso de ligase atlas®, Ciência Rural, 2010; 40:1974-79. Proceedings of the 7th International Symposium on Canine and Feline Reproduction - ISCFR, 2012 - Whistler, Canada Reprinted in IVIS with the permission of the Organizers Close window to return to IVIS Figure 1: Video-assited ovariohysterectomy in a queen. A. First trocar with a valve to insufflate the abdomen (black arrow) and guided incision to insert the second trocar (red arrow). B. Transcutaneous external suture (white arrow) to fix the horn and ovary in abdominal wall. C. Transcutaneous internal suture (yarn in black arrow). D. Bipolar electrocautery forceps cauterizing ovarian pedicle. E. Section of the ovarian pedicle. F. Exposed uterine body/horns/ovaries by second trocar (black arrow). Proceedings of the 7th International Symposium on Canine and Feline Reproduction - ISCFR, 2012 - Whistler, Canada
Baixar