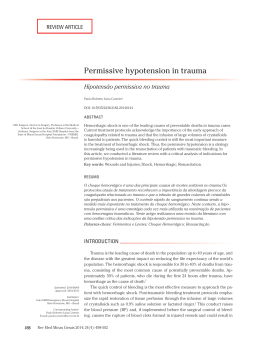
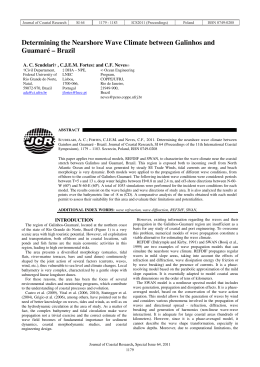
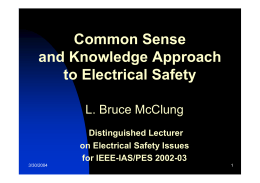
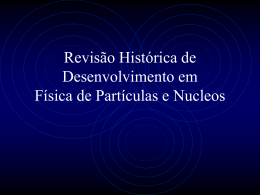
Chapter 2.fm Page 11 Tuesday, November 21, 2006 6:33 PM 2 Physical Principles and Generation of Shock Waves Ludger Gerdesmeyer, Mark Henne, Michael Göbel, Peter Diehl 17 Introduction The effect of extracorporeal shock waves on biological tissue has been known since observations were made during the second World War. At that time, castaways swimming in the water suffered lethal lung damage when water bombs were detonated in a wider radius. The impact of such extracorporeal shock waves caused lungs to tear without any visible injuries on the outside[12]. The properties of such shock waves were utilized to develop new test procedures in material research. Another area of application is signaling technology. Indeed, shock waves propagate (in water, for example) over long distances with only minor energy loss. By measuring acoustic travel time, distances can be deduced as illustrated in laser distance measurement technology[13, 18]. Since they were first used successfully by Chaussy in the treatment of kidney stones in 1980, shock waves have held their own in medicine and the number of applications has risen considerably[2]. The first gall bladder stones were treated in 1985[15]. Since the study conducted by Valchanov, who described the effect of shock waves on the healing of bone fractures, the range of indications for ESWT treatment widened significantly in the area of orthopedics[21]. Today, not only kidney and gall bladder stones but also salivary gland stones, pancreatic stones, pseudoarthrosis, lateral epicondylitis humeri radialis, heel spur and calcified shoulder are treated with varying success[5, 6, 9, 11, 15-17]. A precise description of shock waves was long thought to be unnecessary. What mattered most in the treatment of kidney stones was to be able to fragment the calculi without touch11 Chapter 2.fm Page 12 Tuesday, November 21, 2006 6:33 PM 12 EXTRACORPOREAL SHOCK WAVE THERAPY ing the patient. Side effects such as bleeding or skin lesions were thought to be acceptable. However, the situation in orthopedics is quite different. As a result of the multitude of indications, often very different clinical objectives have been defined. Changing conditions in orthopedic ESWT have brought about a greater need for information on the shock wave itself but also on the equipment to be used and on the possibilities to favor the positive effects of ESWT and to reduce even further any of the rare side effects found to be relevant. To meet such objectives, the information would allow modifying therapy parameters as well as shock wave emission technologies. What is known today about the effects of shock waves on the treatment of kidney stones does not suffice to determine the reasons for the effect of ESWT on orthopedic treatments, to describe which effects are induced on the cellular level, or to explain the shock wave’s analgesic effect[4, 7, 14]. A precise definition of shock wave-relevant parameters is therefore an indispensable requirement to be able to evaluate any observed clinical effects or findings from basic research. This chapter gives an overview of the physical parameters, the characteristic properties and the generation of extracorporeal shock waves. The definition of physical parameters and their characteristic properties is based on the international standard proposal IEC 61846 (International Electrotechnical Commission, Geneva, Switzerland) and on the work of the Shock Wave Therapy Consensus Group. They define which parameters are to be described for individual units and therefore provide utmost transparence for the user[23]. However, they do not state which of these parameters has medical relevance or which has specific biological effects. Parameters can be viewed at http:// www.ismst.org/. The hope is to define the relation between dose and effect independently of the equipment used, and to look for parameters that may be responsible for the medical efficacy of the shock wave. Shock waves are defined as transient pressure oscillations that propagate in three dimensions and typically bring about a clear increase in pressure within a very short time. In most units used in medicine, such maximum pressure is reached within few nanoseconds (ns)[10]. Besides this very rapidly rising positive pressure impulse, shock waves are also characterized by a tension phase with negative pressure following the pressure phase. Overall, shock waves are characterized by the following properties (Figure 1)[19, 22, 23]: Chapter 2.fm Page 13 Tuesday, November 21, 2006 6:33 PM PHYSICAL PRINCIPLES AND GENERATION OF SHOCK WAVES 13 Figure 1a. Illustration of a shock wave. Shock wave pressure is shown as a function of time. A, first portion of the shock wave with positive pressure; B, second portion of the shock wave with negative pressure; P+, positive peak pressure; P-, negative peak pressure; Tr, rise time; Tw, impulse width; I+, standard time interval to calculate the shock wave’s so-called “positive energy”; I, standard time interval to calculate the shock wave’s so-called overall energy. • Positive peak pressure (P+): P+ is defined as the difference between maximum positive peak pressure of the shock wave and ambivalent pressure. Depending on equipment type, P+ varies from 5 mega Pascal (MPa) to 120 MPa. • Negative peak pressure (P-): P- is defined as the maximum negative peak pressure during the second phase of the shock wave. P- reaches values between 10% and 20% of P+. • Rise time (Tr): Tr is defined as the interval in which pressure rises from 10% of P+ up to 90% of P+. Depending on equipment type, Tr can vary from a few nanoseconds to milliseconds. • Impulse width (Tw): Tw is defined as the interval between the time when pressure first exceeds 50% of P+ and the time when pressure (during the exponential pressure drop within the first phase of the shock wave) is less than 50% of P+. The duration of Tw is between 200 ns and 500 ns. The term “full-width-half-maximum” (FWHM) is also used as a synonym for Tw. The duration of Tw affects directly the energy flow density of extracorporeal shock waves. Chapter 2.fm Page 14 Tuesday, November 21, 2006 6:33 PM 14 EXTRACORPOREAL SHOCK WAVE THERAPY Figure 1b. Pressure measurement of one radial shock wave impulse. The values of P+, P-, Tr and Tw of a shock wave depend to a large extent on the shock wave source and on the setting used. The tension portion of the shock wave lasts clearly longer than the pressure portion. In contrast, the value of P- is always less than the value of P+. Also, in contrast with P+, P- is limited in its amplitude due to physical principles. In the case of higher tension force, cohesion forces of the surrounding medium may be exceeded whereby gas-filled negative pressure bubbles - so-called cavitation bubbles - appear[11]. A complete shock wave lasts from a few microseconds to milliseconds; the frequency spectrum encompasses a range between 16 Hz and 20 MHz. Principle of shock wave generation Different processes have been developed to generate shock waves. Four techniques in particular are used in clinical applications. All methods so used aim to couple the generated pressure impulse to the tissue while minimizing energy loss. To this effect, several coupling media are used. The units used in medicine to generate pressure impulses rely on some techniques that are basically different[18]. Chapter 2.fm Page 15 Tuesday, November 21, 2006 6:33 PM PHYSICAL PRINCIPLES AND GENERATION OF SHOCK WAVES 15 Figure 2a. Illustration of a ballistic shock wave source One of the latest but also very common methods is the mechanical generation of shock waves. Based on ballistics, compressed air significantly accelerates a projectile which hits an applicator placed on the skin at very high kinetic energy. By using a coupling gel such as ultrasound gel or Castor oil, this impact pressure hitting the applicator can be delivered to the tissue in the form of a pressure wave. Then, the shock wave continues to propagate in the body in the form of a spherical or ball-shaped wave. This wave travels in a radial fashion, thus the descriptive term radial shock wave. The main characteristic of this type of unit is that steepening occurs much more slowly compared to focused shock wave devices. Focused technologies are required to treat deep areas. Radial technologies provide no second acoustic focus. In this type of shock wave generation, the applicator surface constitutes the geometric point of highest pressure and highest energy density and so it is called tip-of-the-applicator-focus. Due to radial expansion, the pressure and energy density of the shock wave drop steadily upon leaving the applicator. The same shock wave propagation characteristics could be found in focused technologies behind the acoustic focus. Due to theoretical considerations, they also first appear to be less appropriate for classic indications such as pseudoarthrosis or calcific tendonitis located in deeper tissue layers[23]. In contrast, there is no doubt that indications near the surface are highly appropriate for shock waves that propagate radially. In the meantime, new and improved techniques have led to a modification in applicator systems used to deliver ballistic shock waves. Special geometry and changes in applicators allow ballistic shock waves to focus on areas of higher concentration. Clinical studies will need to demonstrate whether such technical modifications would also be appropriate to treat conditions such as pseudoarthrosis or calcific tendonitis reserved until now for the “classic” shock wave. Another common method to generate shock waves is using electromagnetic currents (Figure 3). Chapter 2.fm Page 16 Tuesday, November 21, 2006 6:33 PM 16 EXTRACORPOREAL SHOCK WAVE THERAPY Figure 3. Illustration of an electromagnetic shock wave source In this process, local electromagnetic currents are induced with a flat coil in a thin copper foil. Due to the Lorentz effect on charges in motion, the foil undergoes an explosion-like deflection. In the process, the associated water column is deflected in proportion to the tension. The pressure impulse so generated is then coupled and transmitted to the next medium. Additional technical features such as acoustic cutoff lenses are able to bundle the pressure waves into a defined focus to be placed in deeper regions of the body. Additional acoustic reflectors can further improve the precision of the focus. Further clinical studies will have to show whether such features would be suitable as part of orthopedic pain therapy. The electro pneumatic principle is an old method by which shock waves are generated by a spark plug located in the primary focus (Figure 4). The high temperatures reached at the time of spark discharge cause the surrounding liquid to evaporate and a plasma bubble to occur. These radial shock waves from the primary focus are then bundled into a second focus by using an elliptic acoustic mirror. By using appropriate coupling media, shock waves can be transmitted in selected regions. One of the disadvantages of this process is spark plug wear and wear-dependent shock wave energy variations. The rather costly exchange of electrodes must be repeated after a certain number of discharges. In addition, the shock wave generated with this process may fluctuate between shots in terms of energy and geometry [1] but these variations are believed to be clinically irrelevant. Another method is the piezoelectric principle[20]. A small pressure impulse is emitted in the center of a ball cup by pulse-like local electric impulses of individual piezocrystals. Since the crystals are arranged on a half shell, the individual pressure waves can be bundled in one focus (Figure 5). Chapter 2.fm Page 17 Tuesday, November 21, 2006 6:33 PM PHYSICAL PRINCIPLES AND GENERATION OF SHOCK WAVES 17 Figure 4. Illustration of an electromagnetic shock wave source As in the other methods, such focus can then be placed in the body by using appropriate localization systems. The shock wave is coupled based on the same principle as in the other emission methods mentioned earlier. In terms of shock wave generation methods, a detailed discussion about technical equipment parameters is of little use at this time from a medical point of view. Indeed, today it has not been determined which parameter is significant for possible biological effects or clinical results[8]. However, for the purpose of technical comparisons, it is useful to identify as many shock wave parameters as possible. Figure 5. Summary illustration of a piezoelectric shock wave source Chapter 2.fm Page 18 Tuesday, November 21, 2006 6:33 PM 18 EXTRACORPOREAL SHOCK WAVE THERAPY Figure 6. Illustration of a PVDF hydrophone Measuring Technique Just like technical progress has led to on-going equipment modifications and new techniques to generate shock waves, so have technical advances affected the processes involved in measuring technology. In principle, shock wave magnitude can be measured by electrical and non-electrical means. Non-electrical methods include optical methods and the defined fragmentation rate of model stones[7, 18]. However, there is general consensus that only electrical sensors, so-called hydrophones, are suitable for the quantitative measurement of shock wave magnitude. These are sensors for acoustic pressure in liquids which deliver an electric signal and which are appropriate due to the possibility of calibration for absolute measurements. Among the older hydrophones are PVDF hydrophones. The first dynamic pressure measurements of shock waves were performed with them. The hydrophone used at the time is based on a concept by Chivers and Lewin dating back to 1981 and originally designed for the low-pressure area. This measuring technique is based on the piezoelectric properties of a polyvinyl fluoride (PVDF) foil applied to a thin steel tube. At the end the generated potential is made transparent via an oscilloscope (Figure 6). A major disadvantage of this hydrophone is the fact that the tensile part of the shock wave could not be measured precisely due to local cavitation phenomena as well as the limited stability (life) of the hydrophone. The consensus therefore was to use hydrophones which do not have the PVDF hydrophones related disadvantage. Among them are fiber-optic hydrophones which register acoustic waves as peaks and convert them to proportional output voltage. Chapter 2.fm Page 19 Tuesday, November 21, 2006 6:33 PM PHYSICAL PRINCIPLES AND GENERATION OF SHOCK WAVES 19 Due to the high cost of this technology fiber glass hydrophones have only been used for the past two years. These more recent measurements produce in part significantly higher values for the same parameters. As mentioned before, measurements performed under in vivo conditions raise particular problems[7]. It must be noted once again that until now no link has been established between measurable shock wave parameters and biological or analgesic effect. Today, it is not known whether such equipment-specific parameters are clinically relevant at all or rather serve to animate a technical discussion of lesser clinical relevance. Literature 1. Bailey MR, Blackstock DT, Cleveland RO, Crum LA (1999): Comparison of electrohydraulic lithotripters with rigid and pressure-release ellipsoidal reflectors. II. Cavitation fields. J Acoust Soc Am 106:1149-1160. 2. Chaussy C, Chaussy C, Brendel W, Schmiedt E (1980): Extracorporeally induced destruction of kidney stones by shock waves. Lancet. 13:1265-8. 3. Coleman AJ, Draguioti E, Tiptaf R, Shotri N, Saunders JE (1998): Acoustic performance and clinical use of a fiberoptic hydrophone. Ultrasound Med Biol 24:143-151. 4. Delacretaz G, Rink K, Pittomvils G, et al: Importance of the implosion of ESWLinduced cavitation bubbles. Ultrasound Med Biol 21:97-103, 1995. 5. Delius M: Lithotripsy. Ultrasound Med Biol 26 (Suppl 1):55-58, 2000. 6. Gerdesmeyer L, Wagenpfeil S, Haake M, Maier M, Loew M, Wortler K, Lampe R, Seil R, Handle G, Gassel S, Rompe JD.: Extracorporeal shock wave therapy for the treatment of chronic calcifying tendonitis of the rotator cuff: a randomized controlled trial. JAMA. 2003 Nov 19;290(19):2573-80. 7. Gerdesmeyer, L., Maier, M., Haake, M., Schmitz, C.: Physical-technical principles of extracorporeal shockwave therapy (ESWT). Orthopäde 2002, 31: 610-617 8. Haake M, Boddeker IR, Decker T, Buch M, Vogel M, Labek G, Maier M, Loew M, Maier-Boerries O, Fischer J, Betthauser A, Rehack HC, Kanovsky W, Muller I, Gerdesmeyer L, Rompe JD.: Side-effects of extracorporeal shock wave therapy (ESWT) in the treatment of tennis elbow. Arch Orthop Trauma Surg. 2002 May;122(4):222-8 9. Howell DA: Pancreatic stones: treat or ignore? Can J Gastroenterol 13:461-465, 1999. 10. Hundt E. (1974) Die Physik, Bibliographisches Institut Mannheim – Dudenverlag, S.360 11. Iro H, Zenk J, Waldfahrer F, et al: Extracorporeal shock wave lithotripsy of parotid stones. Results of a prospective clinical trial. Ann Otol Rhinol Laryngol 107:860864, 1998. 12. Krause H: Physik und Technik medizinischer Stosswellensysteme. In Rompe JD (ed). Extrakorporale Stosswellentherapie. Weinheim, Chapman and Hall, 15-34, 1997. Chapter 2.fm Page 20 Tuesday, November 21, 2006 6:33 PM 20 EXTRACORPOREAL SHOCK WAVE THERAPY 13. Lewin PA, Schafer ME: Shock wave sensors: I. Requirements and design. J Lithotr Stone Dis 3:3-17, 1991. 14. Maier M, Milz S, Wirtz DC, Rompe JD, Schmitz C. Basic research of applying extracorporeal shockwaves on the musculoskeletal system. An assessment of current status. Orthopade. 2002 Jul;31(7):667-77. 15. Mulagha E, Fromm HJ: Extracorporeal shock wave lithotripsy of gallstones revisited: current status and future promises. Gastroenterol Hepatol 15:239-243, 2000 16. Rompe JD, et al: Shock wave application for chronic plantar fasciitis in running athletes – a prospective, randomized, placebo- controlled trial. Am J Sports Med 2003; 31:268-275 17. Rompe JD, Schoellner C, Nafe B.: Evaluation of low energy extracorporeal shock wave application and treatment in chronic plantar fasciitis. J Bone Joint Surg Am. 2002; 84:335-341. 18. Schräbler S (1999): Ein abtastendes Verfahren zur Darstellung und Analyse von Stosswellen in Flüssigkeit, Shaker Verlag. 19. Staudenraus J.(1995) In Vivo Stosswellenmessung. In Chaussy C (Hrsg) Die Stosswelle in Forschung und Klinik. Attempto Verlag, S 21-26 20. Tavakkoli J, Birer A, Arefiev A, Prat F, Chapelon JY, Cathignol D (1997) A piezocomposite shock wave generator with electronic focusing capability: application for producing cavitation-induced lesions in rabbit liver. Ultrasound Med Biol 23:107-115 21. Valchanou VD, Michailov P (1991) High energy shock waves in the treatment of delayed and nonunion of fractures. Int Orthop 15:181-184 22. Ueberle F (1997) Shock wave technology. In Siebert W, Buch M (Hrsg) Extracorporal shock waves in orthopaedics. Springer, S.59-87 23. Wess O, Ueberle F, Dührssen RN, et al: Working Group Technical Developements Consensus Report. In Chaussy C, Eisenberger F, Jocham D, Wilbert D (eds). High Energy Shock Waves in Medicine. Stuttgart, Thieme, 59-71, 1997.
Baixar