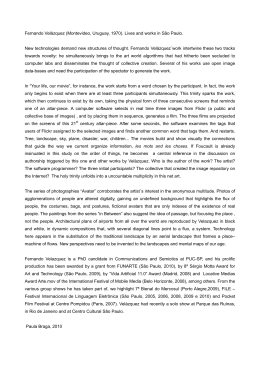
298 Nigri PZ, Orlando FM, Gava ALW, Peccin MS, Cohen M ORIGINAL ARTICLE Assessment of quality of life of patients who underwent anterior cruciate ligament reconstruction and a rehabilitation program Avaliação da qualidade de vida de pacientes submetidos à reconstrução do ligamento cruzado anterior e a um programa de reabilitação Priscila Zeitune Nigri1, Flavia Machado Orlando2, Ana Lucia Wirz Gava3, Maria Stella Peccin4, Moises Cohen5 ABSTRACT RESUMO Introduction: Quality of life can be defined as the expression of a conceptual model that tries to represent patient’s perspectives and his/her level of satisfaction expressed by numbers. The objective of this study is to evaluate the parameters of quality of life of 23 patients who underwent surgery for anterior cruciate ligament reconstruction. Methods: We adopted SF-36, a generic health-related evaluation questionnaire, to obtain information regarding several aspects of patients’ health conditions, and the Lysholm questionnaire, specific to evaluate the symptoms and function of the knee. The questionnaires were applied at two stages of the treatment: pre- and postoperatively (after the rehabilitation program). Results: Before surgery, the Lysholm questionnaire presented the following results: excellent in 4% of the cases, good in 22%, fair in 22%, and poor in 52%. After surgery (Lysholm e SF36) the correlation level was approximately 44% (p = 0.041). Discussion: The correlation between the Lysholm and the SF-36 questionnaires showed the following: the lower the level of pain, the higher the Lysholm score. The high scores presented by the Lysholm questionnaire are directly proportional to physical and emotional aspects, and to functional capacity. Conclusion: Analysis of both questionnaires, as well as of their correlation, showed some improvement in patients´ quality of life. We were also able to demonstrate the importance and usefulness of applying the two questionnaires at three different moments: before, during and after physiotherapeutic intervention. Introdução: Qualidade de vida pode ser entendida como a expressão de um modelo conceitual que tenta representar a perspectiva de um paciente ou seu grau de satisfação de forma quantificável. O objetivo deste trabalho é avaliar os parâmetros de qualidade de vida do ponto de vista de 23 pacientes submetidos à cirurgia de reconstrução do ligamento cruzado anterior do joelho. Métodos: Utilizou-se o questionário genérico de avaliação de qualidade de vida SF-36, para obter informações relacionadas a vários aspectos do estado de saúde; e o questionário Lysholm, específico para avaliar sintomas e função do joelho. Esses foram aplicados em duas etapas do tratamento: a primeira correspondente ao préoperatório e a segunda, ao pós-operatório (após acompanhamento fisioterapêutico). Resultados: Constatou-se que no pré-operatório o questionário Lysholm resultou em 4% excelente; 22% bom; 22% regular; 52% ruim. Para os dados pós-operatórios (Lysholm e SF36), o grau de correlação foi aproximadamente 44% (p = 0,041). Discussão: Ao fazer a correlação do questionário Lysholm com os domínios do questionário SF-36, observamos que quanto menor o nível álgico, maior a pontuação do Lysholm; a alta pontuação do Lysholm é diretamente proporcional à dos aspectos físicos, emocionais e capacidade funcional. Conclusão: Concluímos que houve melhora na qualidade de vida na análise dos questionários Lysholm e SF-36 e também na correlação de ambos. Demonstramos o quanto é importante e necessária a utilização desses questionários antes da, durante e após a intervenção fisioterapêutica. Keywords: Quality of life; Physiotherapy; Anterior cruciate ligament; Questionnaire; Orthopedics Descritores: Qualidade de vida; Fisioterapia; Ligamento cruzado anterior; Questionário; Ortopedia Instituition: Instituto Cohen de Ortopedia, Reabilitação e Medicina do Esporte: Av. Lineu de Paula Machado, 660 - Cidade Jardim - CEP 05601-000 - São Paulo – SP – Tel.: (11) 3093-9000. 1 Physiotherapist of the Instituto Cohen de Ortopedia, Reabilitação e Medicina do Esporte - São Paulo (SP). 2 Physiotherapist from Universidade Paulista - São Paulo (SP). 3 Master´s degree in Health Psychology from UMESP (SP). 4 Physiotherapist of the Instituto Cohen de Ortopedia, Reabilitação e Medicina do Esporte. Master’s degree in rehabilitation, Ph.D. student in Science at the Universidade Federal de São Paulo (SP). 5 Post-doctorate degree and Lecturer at the Universidade Federal de São Paulo, Chief of the Sport Trauma Center of CETE - Universidade Federal de São Paulo (SP). Corresponding author: Priscila Zeitune Nigri - Rua Tupi, 549 - apto11 – Pacaembu - CEP 01233-001 - São Paulo (SP) – Tel.: (11) 3826-4903/(11) 8182-4566 - Fax: (11) 3666-9458. Received on March 2, 2004 – Accepted on August 28, 2004 einstein. 2004; 2(4):298-302 Assessment of quality of life of patients who underwent anterior cruciate ligament reconstruction and a rehabilitation program INTRODUCTION Quality of life can be understood as the expression of a conceptual model that tries to represent the perspective of a patient or his/her level of satisfaction expressed by numbers. This concept started to be applied in the United States after World War II aiming to describe the effect caused by the acquisition of material goods on people’s lives. Quality of life is subjective since it is a concept based on individual perspective, and it is multidimensional because it encompasses different aspects of a person’s life, such as physical and emotional aspects (psychometric aspects). Subjectivity and multidimensionality are key when quality of life is studied(1). The present paper aims to assess the quality of life of patients who were submitted to anterior cruciate ligament reconstruction and physiotherapeutic intervention. We applied two instruments: SF-36, a generic health-related quality of life questionnaire, was used to provide information related to several aspects of patients´ health, such as their functional level, their ability to perform activities of daily living, presence of pain, fatigue and their emotional conditions; and the Lysholm questionnaire, which is designed to study the clinical outcome and to evaluate only the symptoms and function of the knee. Correlations between the Lysholm and the SF-36 questionnaires were statistically significant regarding physical aspects, pain, and functional capacity, items evaluated in both questionnaires(1). It is important to emphasize that the lesion of the anterior cruciate ligament is one of the most common and disabling injuries of the knee, and it affects young adults more often, when they are engaged in more intense sports activities(2-3). It is important to stress that when describing the impairment of an individual’s quality of life or health status and when assessing them in a broader manner, it is possible to show how much that condition is important to social or health aspects(4). The main objective of this study is to assess the parameters of quality of life from the point-of-view of a group of patients in the postoperative stage of reconstruction of the knee ligament that were undergoing physiotherapeutic follow-up, and to verify the existence or absence of specific changes in the symptoms regarding the knee in the first months of the rehabilitation program. Our other objectives are to examine quality of life from the patients´ point-ofview; allowing us to assess the level of interference of their condition on activities of daily living; to examine patients´ acceptance regarding the rehabilitation program, from physical to emotional aspects, at the 299 beginning and during physiotherapeutic actions; to contribute to scientific literature since there are not enough studies regarding quality of life. METHODS This is a longitudinal study carried out by means of examining the questionnaires applied to a group of patients that were undergoing rehabilitation program at a private physiotherapy clinic located in the city of São Paulo. The sample was made up of 23 patients (17 men and 6 women, age ranging from 14 to 52 years, mean age of 31.4 years) who underwent reconstruction of the anterior cruciate ligament and were undergoing physical therapy follow-up, with diagnostics and surgery performed by the same orthopedic surgeon, a specialist in knee surgeries. The Lysholm, “Lysholm Knee Scoring Scale”, is a questionnaire originally written in English and internationally accepted, that aims to study the clinical outcome and to assess exclusively the symptoms and functions of the knee. It was described by Lysholm in 1982, and was later modified(5), validated and translated into Portuguese by Peccin (1). It contains eight questions, with maximum and minimum scores distributed as follows: “limp” (maximum: 5 points; minimum: 0 point); “support” (maximum: 5 points; minimum: 0 point); “locking” (maximum: 15 points; minimum: 0 point); “instability” (maximum: 25 points; minimum: 0 point); “pain” (maximum: 25 points; minimum: 0 point); “swelling” (maximum: 5 points; minimum: 0 point); “stair climbing” (maximum: 10 points; minimum: 0 point); “squatting” (maximum: 5 points; minimum: 0 point). Each question is objective and closed, and the final score can be expressed by concept or by numbers: excellent (95-100 points); good (84-94 points); fair (6583 points); poor (less or equal to 64 points)(1). The terms used in this questionnaire cannot be changed; therefore the technical term “claudicating” (claudicar, in Portuguese) was changed to “to limp” (mancar, in Portuguese) during the translation and validation process, so that patients could better understand the questionnaire. The term “to limp” (mancar) was used in the questionnaire and in this study. The SF-36 questionnaire – “Medical Outcomes Study 36-item Short Form Health Survey” - was developed in 1992 as a generic health-related evaluation questionnaire, easy to be understood and applied, without being too long (6) . It is a multidimensional questionnaire that evaluates 36 items, subdivided in 8 scales or components: functional capacity (10 items), physical aspects (4 items), pain (2 items), general health status (5 items), vitality (4 items), einstein. 2004; 2(4):298-302 300 Nigri PZ, Orlando FM, Gava ALW, Peccin MS, Cohen M social aspects (2 items), emotional aspects (3 items), mental health (5 items), and one more assessment question comparing the current health status to that presented one year ago. It assesses both the negative (disease or illness) and the positive (well-being) aspects. This tool was translated into Portuguese and validated by Ciconelli(7). Results found are converted into a 0to-100 scale, in which “0” corresponds to the worst health condition, and “100”, to the best(4). The Lysholm questionnaire was applied in the preoperative period and for a 2-month follow-up period; the same patients (except for patient N for not living in Brazil) answered both the Lysholm and the SF-36 questionnaires(5). Patients selected for this study met the following inclusion criteria (to make the sample more homogeneous): 1– patients older than 14 years, with clinical diagnosis of anterior cruciate ligament (ACL) lesion, either isolated or combined; 2– signature of the informed consent term by the patient or the person responsible for him/her; 3– patients with the same cultural and socioeconomic level, to make the sample more homogeneous; 4 – patients operated by arthroscopy, using two surgical techniques: • ACL reconstruction with graft of the middle third of the patella tendon (8) and fixation with an interference screw, • ACL reconstruction with graft of the tendons of the semitendinosus and gracilis muscles, and femur fixation with the “trans-fix®” system, and of the tibia with interference screw and a clamp. Following the preoperative evaluation, the 23 patients were submitted to anterior cruciate ligament reconstruction and to the same rehabilitation protocol that emphasizes movement control, complete extension recovery symmetrically to the contralateral knee, early performance of the range of movement, and exercise programs for the quadriceps femoris to recover normal gait and for the posterior thigh muscles to help to protect the graft and restore normal knee biomechanics(9). SF-36 is a questionnaire in which parameters should be assessed in a comparative and individualized manner; however it was not routinely applied, and in order to minimize this absence, we tried the correlate results from SF-36 and the Lysholm questionnaires after the surgery. Data analysis was carried out using the paired t-test, aiming to check the correlation between observations. The paired t-test is adequate when we want to run a general comparison of two population means: measures taken before and after a certain intervention. einstein. 2004; 2(4):298-302 RESULTS Twenty-three patients (17 men and 6 women) who underwent reconstruction of the anterior cruciate ligament between June and September of 2003 were assessed. Results obtained in the pre- and postoperative analysis of the Lysholm questionnaire are presented in table 1. The score was classified according to the following Lysholm standardization: excellent, good, fair and poor. Table 1. Comparative results: Lysholm applied in the pre- and postoperative periods Lysholm Scale Preoperative Postoperative Excellent Good Fair Poor 4% 22% 22% 52% 14% 23% 58% 5% Analysis of the box plot (figure 1) for the pre- and postoperative Lysholm data showed that there are indications that quality of life is better in the postoperative stage since the chart is more homogeneous in that phase. Figure 1. Box-plot describing Lysholm pre- and postoperative periods Correlation analysis between the pre- and postoperative Lysholm data was approximately 60%, which is an average correlation (p = 0.04). For the postoperative data (Lysholm and SF-36), the correlation level was approximately 44%, demonstrating an correlation (p = 0.041) (alpha = 5%, t = 3.149 and p = 0.005). Values obtained in the SF-36 questionnaire (in the postoperative phase) are presented in table 2, which shows the 8 scales of this questionnaire. Assessment of quality of life of patients who underwent anterior cruciate ligament reconstruction and a rehabilitation program 301 Table 2. Comparative SF-36 (postoperative) aspects Patient A B C D E F G H I J K L M O P Q R S T U V W Functional capacity 35 60 95 45 70 65 95 45 55 65 40 60 90 55 70 95 60 65 95 85 90 65 Physical aspects 25 100 25 0 25 25 100 25 50 100 25 25 100 100 100 100 0 50 50 100 0 25 Pain 25 100 25 0 25 25 100 25 50 100 25 25 100 100 100 100 0 50 50 100 0 25 General health score 87 90 82 90 100 87 80 77 87 82 87 87 100 92 62 100 87 87 85 77 87 72 DISCUSSION The term quality of life has had several definitions throughout the years, and it can be based on four key principles: functional capacity, socioeconomic level, satisfaction(10) and self-protection regarding health(11). It can include a larger variety of potential conditions that can affect the perception of individuals, their feelings and behaviors related to their daily functioning; including, but not limiting, their health status and the medical interventions(12). It can also be understood as a subjective concept, based on the perspective of the individual. The patient is the person who can better define his/her own quality of life and relate his/her expectations, satisfaction and well-being(13). In contrast to the piece of information given above, other authors stated it is difficult to define quality of life, as well as to measure it, since it can be affected by cultural, ethical and religious values, as well as by personal values and perceptions (14) . This is a consequence of the lack of clear and unanimous definition of this concept, given the different meanings of the term, and little information about the assessment tools available, which have generated disagreement regarding the most appropriate methods to measure it(15). According to most of the literature, we show that quality of life is affected by several factors related to: strategies of psychosocial adaptation(16), traits of an individual’s personality, the person’s history and expectations towards life(17), their self-concept and self- Vitality 40 70 65 90 90 80 80 25 65 65 45 25 75 100 30 80 45 65 80 90 60 75 Social aspects 50 100 100 38 100 75 100 75 75 88 75 63 88 100 88 100 50 88 50 100 38 100 Emotional aspects 0 67 67 67 33 100 100 100 100 100 100 0 100 100 100 100 0 100 33 100 100 100 Mental health 44 80 80 84 96 84 96 60 88 72 60 44 96 84 32 80 52 76 88 100 80 80 efficiency(10), social support received from people who are important to them, their locus of control(16), and the perception of crisis’ control. The rehabilitation program applied in the postoperative period shows important concept-related changes, compared to the current protocols. The main landmark in physiotherapeutic management of ligament reconstruction started in 1986, with the development of fast protocols, and better knowledge of the biomechanical behavior of the graft(4). In our study, the application of the Lysholm tool before surgery showed that most patients presented poor results; but these improved in the postoperative period as shown by the increased amount of fair results indicating that the two-month treatment had been effective. We should consider it was just the beginning of the treatment (a six-month follow-up according to the protocol performed) and, at that stage, the treatment changed because the range of movement was complete. From that moment on, great improvement in quality of life, mainly in relation to the independence of the patient (such as driving, walking and working) is observed. This is also confirmed by the pain score of SF-36 in which it is possible to observe that for most patients, the lower the level of pain, the higher the Lysholm score. This shows that the correlation is effective because patients with few symptoms of the knee present low level of pain; therefore improving the patient’s quality of life both in the physical and emotional einstein. 2004; 2(4):298-302 302 Nigri PZ, Orlando FM, Gava ALW, Peccin MS, Cohen M aspects. These two latter aspects are closely related since physical problems affect the availability and willingness of patients to carry on their activities of daily living; therefore changing the emotional aspects. In this study, this correlation shows that most patients with deficit in physical aspects also present changes in the emotional field; however, according to the response of few patients, this correlation is not true. On the other hand, it is possible to see that, when compared to Lysholm, the correlation is correct since its high score is directly proportional to physical and emotional aspects. In relation to functional capacity, it was possible to observe the existing correlation among patients since the best Lysholm scores correspond to an increasing development of the functional capacity, which is in accordance with our expectations since after two months of treatment, the functional capacity begins to reach the level presented before the lesion in the anterior cruciate ligament. When other SF-36 scales such as mental health, vitality, general aspects of life and social aspects are related to the Lysholm applied in the same date, they show how differently each patient reacts to the same question and to the same concept since the questionnaire was applied in the same manner (notinduced) to all patients; therefore it is not possible to have data correlation probably because the Lysholm questionnaire does not have a specific question to evaluate non-physical/functional states(18). Our findings support those mentioned in the literature and prove the importance of looking at the individual considering every biopsychosocial aspect. It also reinforces the importance of applying a generic questionnaire in order to have a more truthful profile of the general state of the individual’s health status (1) when specific questionnaires are used to assess a disease. CONCLUSIONS The assessment of quality of life of patients submitted to reconstruction of the anterior cruciate ligament and physiotherapeutic treatment allowed us to conclude that: 1. The quality of life of patients that had undergone ACL reconstruction improved in all parameters assessed, when the specific knee score, the Lysholm, was used. 2. The assessment of post-operative quality of life measured by SF-36 showed that most values are above the mean in all scales. REFERENCES 1. Peccin MS. Questionário específico para sintomas de joelho “Lysholm Knee scoring scale” - tradução e validação para a língua portuguesa [tese]. São Paulo: Universidade Federal de São Paulo; 2001. 2. Harter RA, Osternig LR, Singer KM, James SL, Larson RL, Jones DC. Long-term evaluation of knee stability and function following surgical reconstruction for anterior cruciate ligament insufficiency. Am J Sports Med. 1988; 16(5):434-43. 3. Amatuzzi MM, Albuquerque RFM. Tratamento cirúrgico das lesões agudas do ligamento cruzado anterior: devemos reformular nossa conduta. Rev Bras Ortop.1991; 26(1/2):4-10. 4. Cohen M. Reconstrução do ligamento cruzado anterior com o terço central do ligamento da patela: avaliação dos resultados com seguimento de dez a quinze anos [tese]. São Paulo: Universidade Federal de São Paulo; 2001. 5. Lysholm J, Gillquist J. Evaluation of the knee ligament surgery results with special emphasis on use of a scoring scale. Am J Sports Med. 1982; 10(3): 150-3. 6. Ware JE Jr, Sherbourne CD. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med Care.1992;30(6):473-83. 7. Ciconelli RM. Tradução para o Português e validação do questionário genérico de avaliação de qualidade de vida “medical outcomes study 36-item short-form health survey (SF-36) [tese]. São Paulo: Universidade Federal de São Paulo; 1997. 8. Camaho GL, Olivi R, Camanho LF, Munhoz MAS, Moura MC. Tratamento de lesão aguda do ligamento cruzado anterior. Rev Bras Ortop.1997;32(5):347-52. 9. Peccin MS. Reabilitação após reconstrução do ligamento cruzado anterior [online]; 2001; São Paulo. Pós-graduação na Universidade Sta. Cecília.[citado 2003,Ago 20]. Disponível em URL http://www.institutocohen.com.br 10. González NM. Symposium de calidad de vida: generalidades, mediciones utilizadas en medicina, elementos que la componen. Arch Reumatol. 1993(1); 4:40-2. 11. Hornquist JO. Quality of life: concept and assessment. Scand J Soc Med. 1990;18(1):69-79. IMPLICATIONS As a practical application of this study, we observed that it is necessary to use objective parameters to assess the quality of life in the pre- and postoperative periods; therefore, we suggest its application to be performed before, during, and after the physiotherapeutic intervention. On assessing its implication for research, we found out that further studies – evaluating parameters of quality of life of patients with anterior cruciate ligament lesion conservatively or surgically-treated – are necessary, using different objective and subjective methods to assess the results, especially by carrying out randomized clinical trials. einstein. 2004; 2(4):298-302 12. Bullinger M, Anderson R, Cella D, Aaronson N. Developing and evaluating cross-cultural instruments from minimum requirements to optimal models. Qual Life Res.1993; 2(6): 451-9. 13. Souza EAPD. Questionário de qualidade de vida na epilepsia: resultados preliminares. Arq Neuropsiquiatr.2001;59(3-A):541-4. 14. Gaíva MAM. Qualidade de vida e saúde. Rev Enf UERJ.1998; 6(2):377-82. 15. Cella DF, Tulsky D. Measuring quality of live today: methodological aspects. Oncology.1990;4(5):29-38. 16. Kempen PRD, Ormel J, Brilman I, Relyveld J. Adaptative responses among Dutch elderly: the impact of eight chronic medical conditions on health related quality of life. Am J Public Health.1997;87(1):38-44. 17. Calman, KC. Quality of life in cancer patients an hypothesis. J Med Ethics.1984; 10(3): 124-7. 18. Shapiro ET, Richmond JC, Rockett SE, McGrath MM, Donaldson WR. The use of generic, patient-based health assessment (SF-36) for evaluation of patients with anterior cruciate ligament injuries. Am J Sports Med. 1996, 24(2): 196-200.
Download