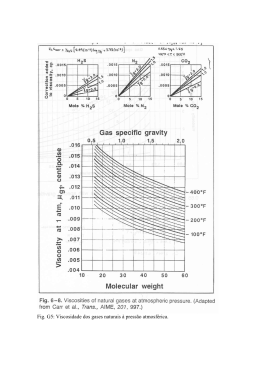
Preparação para o parto com um novo dispositivo de treino R. Schuchardt, J. Hillebrenner, S. Hoffman, W. Horkel, M. Schelling, KTM Schneider Frauenlinik der TU-Munchen; Klinikum rechts der Isar, Abteilung für Perinatalmedizin; Praxis Starnberg Introdução Os cursos de preparação para o parto realizados por enfermeiras ou fisioterapeutas são regularmente frequentados por um elevado número de mulheres grávidas, a partir da 24ª. semana até ao dia do parto. Estes servem para preparar mentalmente todas as grávidas primíparas para o nascimento do seu primeiro filho, desenvolver um conhecimento de todas as fases de entrega e mecanismos de nascimento, bem como aprender diferentes exercícios de respiração e de relaxamento. Neste caso em particular, as mães primíparas têm mais dificuldade em imaginar como será o parto, o período das contracções, associando o medo e a dor à penetração da cabeça do bebé. O dispositivo de treino para o parto aqui apresentado foi desenvolvido como uma possibilidade de adaptar gradualmente a vagina e o períneo a grandes volumes de penetração e treinar as sensações de pressão adequadas. Este estudo pretende investigar até que ponto é possível influenciar positivamente o processo de nascimento, através da ajuda deste dispositivo de treino e simultaneamente prevenir lesões a nível do períneo. Material e métodos Segundo a perspectiva de um estudo piloto realizado a 80 mulheres grávidas (50 das quais primíparas e 30 multíparas) foram examinadas em oposição a um grupo de controlo com bebés com o mesmo perímetro cefálico e peso de nascimento (pacientes que não realizaram o treino) no que diz respeito a infecções do períneo e respectivo processo de preparação para o parto. O dispositivo de treino para o parto EPI NO (fig. 2) é composto por um balão cónico e anatómico, ligado a um manómetro através de um tubo com aproximadamente 70 cm. Desde a 38ª. semana até ao final da gravidez, o balão é introduzido pela grávida na sua vagina uma vez por dia, de forma gentil e gradual, podendo ser enchido até atingir um máximo de 10 cm de diâmetro. Após 15 a 20 minutos, o balão é expelido pela grávida, tendo em conta de que o limite de dor não deva ser excedido em nenhuma das circunstâncias (fig. 1). Para um maior rigor do estudo, diariamente são documentados parâmetros, tais como, o tamanho do balão, a capacidade de pressão, a ansiedade do parto e algum tipo de problemas técnicos. Fig. 1 Fig. 2 Resultados No que respeita à ansiedade do nascimento (muito medo = 4; sem medo = 1), registou-se uma significativa redução deste medo no decurso do treino (fig. 3). No grupo de mulheres grávidas que usaram o dispositivo de treino para o parto, a toma de analgésicos (PDA-rate: p=0.038; Dolatin: p=0.01) ficou muito abaixo comparativamente ao grupo de controlo (fig. 4). Fig. 3 A fase do parto, dentro do grupo de formação, teve a duração média de 28.8 minutos. Uma duração significativamente mais baixa do que o grupo de controlo, com uma média 53.7 minutos (p=0.014) (fig. 5). No grupo de grávidas primíparas foi possível registar uma significativa redução da taxa de episiotomia de 78%, no controlo colectivo, para 42%, sem observar um aumento considerável das lesões do trabalho de parto (danos do períneo, de grau I –III). Em 48% dos partos espontâneos, as mães primíparas do grupo de treino experienciaram um parto com “períneo intacto”, considerando que no controlo colectivo, apenas 8.5% dos partos espontâneos ocorreram sem recurso a uma episiotomia ou danos no períneo (fig. 6). Fig. 4 Os valores do Índice de Apgar foram significativamente mais elevados após o 1º. e 5º. minuto no grupo de treino, comparativamente ao grupo de controlo (fig. 7). Discussão e consequências Através do treino diário com o dispositivo de preparação para o parto EPI NO é possível reduzir significativamente a ansiedade, reduzir o período de recuperação pós-parto assim como o uso de analgésicos. Isto pode ser explicado pelo facto da inibição das contracções uterinas, no âmbito da ansiedade do parto, serem impedidas através deste efeito energético. Um curto período de parto traz menos stress para o feto e por conseguinte um índice de Apgar mais favorável. Lenta e gentilmente, os mecanismos de pré-expansão da vulva e a vagina são regulados pela própria mulher, sendo deste modo possível reduzir significativamente infecções da vulva, assim como da vagina, influenciar positivamente o próprio parto e consequentemente a situação do próprio feto. Mais ainda, pode ser esperada uma redução das micro-lesões que desempenham um papel considerável num possível micro-trauma que possa vir a ocorrer, mais tarde, nos músculos da pélvis. * Publicado: “8. kongress der Deutschen Gesellschaft für Pränatal – und Geburtsmedizin, Nürnberg, 18 – 20.05.2000” Birth preparation with a novel birth training device R. Schuchardt, J. Hillebrenner, S. Hoffmann, W. Horkel*, M. Schelling, KTM Schneider Frauenklinik der TU-München; Klinikum rechts der Isar, Abteilung für Perinatalmedizin; * Praxis Starnberg Introduction Material and methods: In a prospective and single blinded pilot study 80 pregnant women (50 primiparae and 30 pluriparae) were examined as against a control group with comparable baby’s head circumference and birth weight (patients who did not perform the training) with regard to perineal injuries and the birth process itself. The Birth Trainer EPI•NO (fig. 2) consists of a pumpable conical balloon which is connected to a manometer via an approx. 70 cm long tube. From the 38th week of pregnancy on it is fed into the vagina by the pregnant women once per day and gently and gradually pumped up to a maximum diameter of 10 cm. After 15 to 20 min the balloon is pressed out by the pregnant women, whereby the threshold of pain must not be exceeded under any circumstances. (fig. 1). In a special patient’s protocol the balloon size, pressing capacity, anxiety of birth and technical problems are documented daily. Length of parturition phase 54 60 P=0,014 50 in min Birth preparation courses by midwives or physiotherapists are regularly attended by a large number of pregnant women from the 24th week of gestation on. They serve above all to mentally prepare primiparae for the oncoming birth, to develop an understanding of the phases of delivery and birth mechanism and to learn breathing and relaxing exercises. In particular primiparae have difficulty in imagining what the parturition phase and the pressing period will be like and fear the pain associated with the penetration of the baby’s head. The Birth Trainer presented here was developed as a possibility to gradually adapt the vagina and perineum to greater penetration volumes and to train a feeling for sufficient pressing. This study intends to investigating to what extent it is possible to influence the birth process positively with the help of this training device and to additionally prevent perineal injuries. 29 40 30 20 10 0 Fig. 2 EG EPI-NO group Results: Anxiety of birth 60% p<0,0001 78% p<0,0001 48% 42% 40% p=0,078 8,50% 20% p=0,12 9,30% 8% 2% 4,20% 0% Intact Episiotomy perineum EPI-NO group perineal tear 1 perineal tear 2 Control group Fig. 6 Apgar score after 1 minute p=0,003 80% 6 40% Control group EPI-NO group EPI-NO group Control group 5 6 7 8 9 10 0,0% 0,9% 4,0% 0,9% 4,0% 6,2% 10,0% 34,5% 66,0% 55,8% 16,0% 1,8% Apgar score after 5 minutes p=0,011 80% 40% Control group EPI-NO group 5 6 7 8 9 10 0,0% 0,0% 0,0% 0,0% 0,0% 0,0% 2,0% 5,3% 20,0% 37,2% 78,0% 57,5% Discussion and consequences: 2,7 Anxiety of birth before training Anxiety of birth after training Fig. 3 Analgesics requirements p=0,01 42% p=0,038 29% 40% 14% 16% 20% 10% PDA rate EPI-NO group Dolantin requirements Control group Fig. 1 Published: 8. Kongress der Deutschen Gesellschaft für Pränatal - und Geburtsmedizin, Nürnberg, 18.-20.05.2000 0% 0% Fig. 7 3,3 minimum 0% 80% p< 0,001 minor 30% 100% EPI-NO group Control group great 50% Fig. 5 Delivery injuries In the subjective assessment of anxiety of birth (great fear = 4; no fear = 1) a significant reduction of this fear (p<0.001) was registered within the course of training (fig. 3). In the group of pregnant women taking part in delivery training with the birth trainer the analgetics requirements (PDA-rate: p=0.038; Dolantin: p=0.01) were significantly below the analgesic required by the control group (fig. 4). The parturition phase within the training group lasting an average of 28.8 min was significantly lower than in the control group with an average of 53.7 min (p=0.014) (fig. 5). In the group of primiparae it was possible to significantly reduce the episiotomy rate from 78% in the control collective to 42%, without observing any major increase in other labor injuries (perineal tears, degrees I- III). In 48% of the spontaneous deliveries primiparae of the training group experienced delivery with „intact perineum“, whereas in the control collective only 8.5 % of the spontaneous delivery were without episiotomy or perineal tear (p<0.0001) (Fig. 6). In comparing the Apgar scores significantly higher rates where achieved after 1 and 5 minutes in the training group than in the control group (1-min-Apgar: p=0.003; 5-min-Apgar: p=0.011; 10-min-Apgar: not significant.) (fig. 7). none NEG Control group Fig. 4 By daily training with the Birth Trainer EPI•NO it is possible to reduce the anxiety of birth significantly. By reducing anxiety of birth it is also possible to shorten the parturition period as well as the analgesics requirements. This may be explained by the fact that the inhibition of uterine contractions within the scope of birth anxiety is prevented on the grounds of the ßadrenergic effect. A shorter parturition period means less stress for the foetus and therefore leads to more favourable „Outcome Parameters“ e.g. the Apgar Score. By a slower, more gentle mechanical pre-expansion of vulva and vagina regulated by the woman herself, it has been possible to reduce injuries to the vulva as well as vagina significantly and simultaneously positively influence the birth itself positively, in addition to the situation of the foetus. Moreover there can also be expected a reduction in microlesions which play a considerable role in later micro-trauma of the pelvis muscles can also be expected. Bibliography: contact the author for more information
Baixar