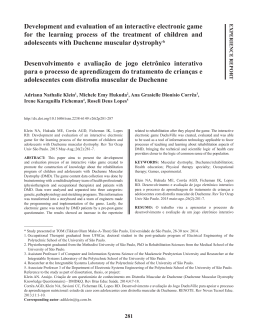
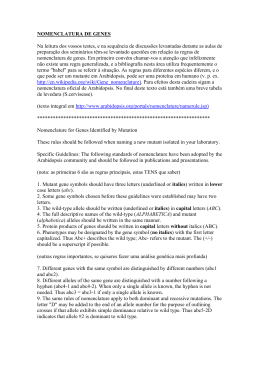
HUMAN MUTATION 25:38^44 (2005) RESEARCH ARTICLE The Most Common Mutation in FKRP Causing Limb Girdle Muscular Dystrophy Type 2I (LGMD2I) May Have Occurred Only Once and Is Present in Hutterites and Other Populations Patrick Frosk,1 Cheryl R. Greenberg,1,2 Alysa A.P. Tennese,1 Ryan Lamont,1 Edward Nylen,1 Cheryl Hirst,1 Danielle Frappier,4 Nicole M. Roslin,4 Michaela Zaik,6 Kate Bushby,5 Volker Straub,6 Mayana Zatz,7 Flavia de Paula,7 Kenneth Morgan,3,4 T. Mary Fujiwara,3,4 and Klaus Wrogemann1,2n 1 Departments of Biochemistry and Medical Genetics, University of Manitoba, Winnipeg, Canada; 2Department of Pediatrics and Child Health, University of Manitoba, Winnipeg, Canada; 3Departments of Human Genetics and Medicine, McGill University, Montreal, Canada; 4The Research Institute of the McGill University Health Centre, Montreal, Canada; 5Institute of Human Genetics, University of Newcastle upon Tyne, United Kingdom; 6Department of General Pediatrics and Neuropediatrics, University of Essen, Essen, Germany; 7Human Genome Research Center, Departamento de Biologia, Instituto de Biociências, Universidade de São Paulo, São Paulo, Brazil Communicated by Jacques Beckmann Limb girdle muscular dystrophy (LGMD) is common in the Hutterite population of North America. We previously identified a mutation in the TRIM32 gene in chromosome region 9q32, causing LGMD2H in approximately two-thirds of the 60 Hutterite LGMD patients studied to date. A genomewide scan was undertaken in five families who did not show linkage to the LGMD2H locus on chromosome 9. A second LGMD locus, LGMD2I, was identified in chromosome region 19q13.3, and the causative mutation was identified as c.826C4A (L276I), a missense mutation in the FKRP gene. A comparison of the clinical characteristics of the two LGMD patient groups in this population reveals some differences. LGMD2I patients generally have an earlier age at diagnosis, a more severe course, and higher serum creatine kinase (CK) levels. In addition, some of these patients show calf hypertrophy, cardiac symptoms, and severe reactions to general anesthesia. None of these features are present among LGMD2H patients. A single common haplotype surrounding the FKRP gene was identified in the Hutterite LGMD2I patients. An identical core haplotype was also identified in 19 other non-Hutterite LGMD2I patients from Europe, Canada, and Brazil. The occurrence of this mutation on a common core haplotype suggests that L276I is a founder mutation that is dispersed among populations of European origin. Hum Mutat 25:38–44, 2005. r 2004 Wiley-Liss, Inc. KEY WORDS: FKRP; TRIM32; limb girdle muscular dystrophy; LGMD; Hutterites; linkage mapping; linkage disequilibrium; founder effect DATABASES: TRIM32– OMIM: 602290, 254110 (LGMD2H); GDB: 9957765; GenBank: NM_012210.2 FKRP – OMIM: 606596, 607155 (LGMD2I); GDB: 4589036; GenBank: NM_024301.2 www.dmd.nl (Leiden Muscular Dystrophy Pages) www.ncbi.nlm.nih.gov/SNP/index.html (dbSNP) INTRODUCTION The limb girdle muscular dystrophies (LGMDs) are a clinically and genetically heterogeneous group of disorders characterized by weakness and wasting in the pelvic and shoulder girdles [Bushby, 1999a, 1999b]. The LGMDs are rare worldwide, with a prevalence of about 40 per million [Emery, 1991]. LGMDs have been mapped to 15 different loci; five LGMDs have an autosomal dominant mode of inheritance and 10 have an autosomal recessive mode of inheritance [Kaplan and Fontaine, 2004; Zatz et al., 2003]. Mutations in genes have been identified in three of the dominantly inherited LGMDs and for all of the recessively inherited LGMDs (see the Leiden muscular dystrophy website; r2004 WILEY-LISS, INC. Received 14 July 2003; accepted revised manuscript 9 June 2004. n Correspondence to: Dr. Klaus Wrogemann, Department of Biochemistry and Medical Genetics, University of Manitoba, 770 Bannatyne Ave.,Winnipeg, MB R3E 0W3, Canada. E-mail: K [email protected] Grant sponsor: German Research Society; Grant numbers: DFG Str 498/3^2; SPP 1086; Grant sponsors: Canadian Institutes of Health Research; Muscular Dystrophy Association; Muscular Dystrophy Association of Canada; Children’s Hospital Foundation of Manitoba; Manitoba Health Research Council; Canadian Genetic Diseases Network (Networks of Centres of Excellence Program); Krupp-Stiftung; Muscular Dystrophy Campaign. DOI 10.1002/humu.20110 Published online in Wiley InterScience (www.interscience.wiley.com). A COMMON LGMD2I FOUNDER MUTATION www.dmd.nl). Among the latter are LGMD2H (MIM# 254110) and LGMD2I (MIM# 607155). LGMD2H is a relatively mild form that was first described in the Manitoba Hutterites in 1976 [Shokeir and Kobrinsky, 1976] and has become known as the ‘‘Hutterite type’’ muscular dystrophy. We previously identified a missense mutation, c.1459G4A (D487N), in TRIM32 as the putative causative mutation, and all known Hutterite patients in families that showed linkage to chromosome region 9q32 were homozygous for this mutation [Frosk et al., 2002]. TRIM32 is a member of the tripartite-motif family of proteins [Reymond et al., 2001] and may be an E3 ubiquitin ligase due to the presence of a RING–finger domain [Freemont, 2000; Horn et al., 2004]. To date, mutations in this gene have not been found in any patients outside the Hutterite population. LGMD2I was first described in a large consanguineous Tunisian family and mapped to chromosome region 19q13.3 [Driss et al., 2000]. Concurrent with our study, another group [Brockington et al., 2001a, b] found mutations within the fukutin-related protein gene (FKRP) in LGMD2I families, as well as in families with a severe form of congenital muscular dystrophy, MDC1C (MIM # 606612). FKRP is thought to be a glycosyltransferase that may function in the O-linked glycosylation of proteins such as a-dystroglycan [Esapa et al., 2002; Hewitt and Grewal, 2003]. Recent work has shown that LGMD2I is one of the most common forms of LGMD worldwide [Bushby and Beckmann, 2003]. The Hutterites, also called Hutterite Brethren, live on farming colonies located predominantly in the Prairie Provinces and Great Plains of North America, and constitute a religious and genetic isolate. They immigrated to North America from Europe in the 1870s and formed three subdivisions. There has been very little intermarriage between subdivisions. The ancestry of the overwhelming majority of the Hutterites can be traced back to 89 ancestors [Nimgaonkar et al., 2000]. The history and social structure of the Hutterite Brethren are described in Hostetler [1985]. Here we report that the second type of LGMD in the Hutterite population maps to chromosome 19q31–q33 and is due to homozygosity for the L276I mutation in FKRP. We also present a comparison of the clinical variability of LGMD2I and LGMD2H and evidence that the L276I mutation observed in Hutterites and other populations is inherited from a common ancestor. MATERIALS AND METHODS Patients, Families, and Controls DNA samples from 38 Hutterites, including 12 affected with LGMD, from five nuclear families, were included in a genomewide scan. Subsequent to the genomewide scan, we collected DNA from five other small Hutterite families with seven individuals affected with LGMD. The LGMD2H families referred to in this study are those reported in Frosk et al. [2002], along with one newly ascertained patient referred by Dr. Keith Brownell, University of Calgary. The clinical criteria for LGMD were essentially the same as previously used [Weiler et al. 1998a]. DNA from 19 non-Hutterite LGMD2I patients was obtained. A total of 12 are from the UK, five are from Brazil (four Caucasian, one African-Brazilian), one is from Germany, and one is GermanCanadian. A total of 14 of these patients are homozygous for the FKRP L276I mutation, and the remaining five are heterozygous for this mutation. The second mutation in four of the five compound heterozygotes is E310X, W279X, V300M, or Y307N, while no other mutation was identified in the coding sequence of FKRP for the remaining heterozygote. A control group of 111 healthy individuals from Manitoba, not known to have LGMD, was used to determine allele frequencies. Controls were obtained from the 39 Rh Laboratory, University of Manitoba, and are 90% Caucasian, with the remainder being Aboriginal, Asian, and African. This study was approved by the Health Research Ethics Board of the University of Manitoba. DNA Analysis Protocols for DNA analysis have been published previously, as follows: genotyping of microsatellite markers in candidate genes and for fine mapping [Weiler et al., 1998a], genomewide scan at the Montreal Genome Centre [Mira et al., 2003], and DNA sequencing [Frosk et al., 2002]. PCR cloning was done using a TOPO TA cloning kit (Invitrogen, www.invitrogen.com) as per the manufacturer’s instructions. A total of 18 additional markers used in this study were: D19S903, D19S918, D19S908, D19S219, DM, D19S412, FKRP52 (dbSNP rs8179080), a C4G SNP in the FKRP promoter (rs3810288), FKRP c.135C4T (rs2287717), FMS2 (rs3138636), D19S540, D19S606, D19S902, D19S596, D19S879, D19S550, D19S867, and D19S904. FKRP52 [Louhichi et al., 2003], a CA/CAA repeat found within an intron of the PRKD2 gene, was amplified by PCR with FKRP52_F (50 TCTCCAAAAAACAACAACAAC-30 ) and FKRP52_R (50 CTAGTGTTCTGGGACCTTT-30 ). FMS2, a CA repeat found within the 30 untranslated region (UTR) of SLC1A5 [Jones et al., 1994], was amplified with FMS2_F (50 -GGAGGGAATAGGGGATCTGG-30 ) and FMS2_R (50 -CACCATGCTGGT0 TATTTTGGC-3 ). FKRP c.135C4T is a silent variant within codon 45 of FKRP. It was amplified in a 702-bp fragment using FKRP_ex.4(1)F (50 -CTCAACCTTCTGGTCCTCTTC-30 ) and FKRP_ex.4(1)R (50 -CCGAGAGGTTGAAGAGGT-30 ). The fragment was then digested with NgoMIV (New England Biolabs, www.neb.com), the C allele yields two fragments (499 and 203 bp) and the T allele remains uncut. Rs3810288 in the FKRP promoter was amplified in a 118-bp fragment using rs3810288_F (50 TCCAACCTGCACCTGGCTAGG-30 ) and rs3810288_R (50 AGCTGGAGGGGTCTGGGAGAtCT-30 ). A mismatch (denoted by lowercase t) creates an Hpy188I site (New England Biolabs), the C allele yields two fragments when digested (96 and 22 bp) and the G allele remains uncut. Samples for both SNPs, c.135C4T and rs3810288, were analyzed by electrophoresis on polyacrylamide gels (8 and 15%, respectively). In addition to genotyping FKRP c.826C4A/L276I (NM_024301.2) by BfaI digestion [Brockington et al., 2002], we developed a nested allele-specific PCR assay. A 2-kb PCR product was generated using primers FKRP_ex4(1)F (50 -CTGCCTTC CCTTTCGTCC-30 ) and FKRP_ex4(3)R (50 -CCAAAACTCTG CCCCTGC-30 ). This fragment contains most of exon 4 of the FKRP gene and was used as template in a secondary allele-specific amplification step using the reverse primers FKRP_826C (50 CCTTCCCAGCTCACTcG-30 ) and FKRP_826A (50 -CCTTCCC AGCTCACTcT-30 ). Each primer has an intentional mismatch at the second-to-last base pair (lowercase) to destabilize the resultant DNA duplex, and the last base pair corresponds to either the normal (C) or mutant (A) sequence. A common forward primer, FKRP_ex4(2)F (50 -CCTGGACGGAGATGCTGT-30 ) was used and amplification with the two reverse allele-specific primers was done in separate PCR reactions. Samples were analyzed by electrophoresis in 1.5% agarose. Protein Analysis Muscle proteins were extracted in treatment buffer containing 0.125 M Tris-HCl (pH 6.8), 4% SDS, 20% glycerol, 5% mercaptoethanol, and 0.0001% bromphenol blue. Soluble proteins were separated by SDS-PAGE on 3 to 10% linear gradient gels and transferred to a nitrocellulose membrane. The membrane was blocked in 3% milk powder in phosphate buffered saline (PBS), treated with anti-glycosylated a-dystroglycan antibody (IIH6C4, Upstate 1:1,000, www.upstate.com) or anti-b-dystroglycan antibody (Novocastra 1:50, www.novocastra.co.uk), and washed and 40 FROSK ET AL. incubated with horseradish peroxidase (HRP)-conjugated antimouse secondary antibodies (Dianova, www.dianova.de). Immunoreactive bands were detected using a chemiluminescence detection system (ECL, Amersham Biosciences, www.amersham biosciences.com). Skeletal muscle tissues were embedded in traganth and frozen in liquid nitrogen-cooled isopentane. Cryosections (7 mm) were immunostained with anti-glycosylated a-dystroglycan (IIH6C4; Upstate) in TBS/1% bovine serum albumin (BSA) for 90 min. After washing, sections were incubated with the appropriate Texas Red dye-conjugated secondary antibody for 30 min. Sections were observed under a Zeiss Axioplan fluorescence microscope (www.zeiss.com). RESULTS Identi¢cation of the LGMD2I Locus in Hutterites After the LGMD2H locus had been mapped, five Hutterite families did not show linkage to chromosome region 9q31–q33, two of which had been reported previously [Weiler et al., 1998b]. After excluding the known LGMD loci LGMD1A, 1B, 1D, and 2A–2G, we performed a genomewide scan, using 389 microsatellite markers with an average spacing of 9.1 cM, on 38 individuals, including 11 affected with LGMD. Single-point parametric linkage analysis with a fully penetrant autosomal recessive disease model was performed using GENEHUNTER 2.1 [Kruglyak et al., 1996; Markianos et al., 2001]. A maximum logarithmic odds (lod) score of 1.50 at D19S587 was obtained. The second highest score was 0.87 at the adjacent marker, D19S178, and the third highest score was 0.67 at D2S407. These lod scores were all at zero recombination. Using multipoint linkage analysis, the maximum multipoint lod score was 3.18 at D19S178. The region with the next highest multipoint lod score was 1.06 at D2S407. To define a candidate gene interval, families were genotyped for 18 additional markers in a 13-cM region between two genomescan markers, D19S178 and D19S246 (see Materials and Methods section). Three markers, FMS2, FKRP52, and D19S902, in a 1.3cM interval, had single-point lod scores of 5.33 at zero recombination. During our fine-mapping studies, Brockington et al. [2001a] reported that a form of congenital muscular dystrophy was caused by mutations in FKRP, a promising candidate gene for LGMD2I. The entire coding region of FKRP was sequenced in one Hutterite LGMD2I patient who was found to be homozygous for a missense mutation, c.826C4A (L276I), that results in the substitution of isoleucine for leucine. This same mutation was reported by Brockington et al. [2001b], with the patients from 15 of their 17 LGMD2I families being homozygous (five families) or heterozygous (10 families). We found that every Hutterite LGMD patient who was not homozygous for the TRIM32 D487N mutation, was homozygous for the FKRP L276I mutation. L276I was not found in our control group of 111 individuals. The majority of Hutterites who are homozygous for the L276I mutation are also homozygous for D19S412 (109 bp), FKRP52 (110 bp), rs3810288 (G allele), c.135C4T (T allele), FMS2 (142 bp), and D19S540 (184 bp) (Fig. 1). This indicates that a genomic segment of about 0.5 Mb is shared among Hutterites carrying L276I and is likely identical by descent from a common ancestor. In comparison to the allele frequencies of our 111 controls (Table 1), there is a strong association of L276I in the non-Hutterite patients with the 110-bp allele of FKRP52 (52 kb centromeric to L276I), the G allele of rs3810288 (10 kb centromeric to L287I), the T allele of c.135C4T (0.7 kb centromeric to L276I), and the 142-bp allele of FMS2 (19 kb telomeric to L276I). The association of L276I with the 109-bp allele of D19S412 (250 kb centromeric to L276I) and the 184 bp allele of D19S540 (250 kb telomeric to L276I) does not appear as strong (Table 1). The markers flanking this region (DM, 1 Mb centromeric and D19S606, 0.7 Mb telomeric) show no association with L276I in the patients that we studied (Table 1). Recombination appears to have occurred between L276I and FMS2 on one chromosome (Patient C11.975) and between rs3810288 and c.135C4T on another (Patient NCL-10; Fig. 1). This results in a very small common core haplotype consisting of the mutation itself and c.135C4T. The likelihood that this set of associations has occurred by chance is low and reflects strong linkage disequilibrium. Thus, L276I appears to have arisen only once and is identical by descent in most, and possibly all patients. The presence of a homozygous AfricanBrazilian individual showing these same associations (Patient C10.882; Fig. 1) raises the possibility that the mutation is not Genotypes for markers in a 1.7-Mb region £anking FKRP.The Hutterite haplotype corresponds to the most frequent haplotype in the Hutterites. Patients NCL-01 through 12 are Caucasian patients collected in the UK. Patients C6.625, C8.749, C11.975, and C17.553 are Caucasian Brazilian patients and Patient C10.882 is African-Brazilian [de Paula et al., 2003]. Patient G-01 is German and Patient G-04 is German-Canadian. Black regions indicate alleles that are consistent with the consensus Hutterite haplotype; gray shading indicates alleles that are one repeat unit di¡erent and may have arisen by slipped mispairing during DNA replication; boxed areas indicate alleles that were phased by PCR cloning. Alleles for microsatellite markers are designated by length in bp except for DM, which is reported as the number of CAG repeats. For c.135C4Tand rs3810288, alleles are designated by nucleotide and for FKRP L276I, alleles are designated by amino acid. FIGURE 1. A COMMON LGMD2I FOUNDER MUTATION TABLE 1. Marker DM D19S412 FKRP52 rs3810288 c.135C4T FKRP L276I FMS2 D19S540 D19S606 41 Frequency of Chromosome 19 MarkerAlleles Associated With the L276Ia Mutation in FKRP Allele Hutterite 276I chromosomes (%) Non-Hutterite 276I chromosomes (%) Frequency of allele in controls chromosomes (%) N=222 Physical distance from the L276I mutation (bp) b 22 repeats 109 bp 110 bp G T Ile 142 bp 184 bp 184 bp 92 c 100 97 c 100 100 100 100 100 87 c 0 70 82 97 100 100 94 79 10 nd 36 2 34 14 0 18 31 nd 986,085 248,199 52,237 10,554 691 0 +18,767 +247,548 +714,207 Inferred from the c.826C4A change identi¢ed within FKRP (NM_024301.2). UCSC Human Genome Assembly website (http://genome.ucsc.edu/index.html; April 2003 Assembly). The other observed alleles were DM/5 and 13 repeats; FKRP52/112 bp; D19S606/180 and 182 bp. a b c specific to Caucasians. However, with our limited data this cannot be conclusively determined, particularly in light of the extreme amount of admixture amongst Brazilians [Parra et al., 2003]. Of note are the discrepancies present at the FKRP52 locus. A possible mutation in FKRP52 due to slipped strand mispairing during DNA replication is present on five of the nine Brazilian chromosomes (110 bp4108 bp). This suggests a recent Brazilian mutational event in a common ancestor of three of these five Brazilian patients [de Paula et al., 2003]. In addition, within the Hutterite population there are also individuals with a 112-bp allele instead of a 110-bp allele on the same haplotype as the L276I mutation. Through cloning and sequencing, we have found a large amount of variation in FKRP52 (data not shown). There is variation in both a dinucleotide (CA) and trinucleotide (CAA) stretch between the FKRP52 primers, however, trinucleotide variation is much less common. We have found that the range of variation in the CAA stretch is limited to two possibilities (three or four CAA repeats, four being rare), whereas the range of variation in the CA stretch is much greater (13 to 31 CA repeats). The net result is allele sizes in the range of 92–128 bp, with variation in the CAA stretch showing up as odd-sized alleles within this range. A total of 17 different alleles were found to be present in our 111 control samples at frequencies ranging from 0.5 to 26.1% (data not shown). This hypervariability readily explains the discrepancies that we have detected at this locus in our patient samples. Phenotype^Genotype Correlations To date we have identified 60 Hutterite individuals from 27 nuclear families who are homozygous for either TRIM32 D487N (41 individuals from 17 nuclear families) or FKRP L276I (19 individuals from 10 nuclear families). Table 2 shows clinical details on individuals who were homozygous or heterozygous for the mutations. There is considerable clinical variability even among siblings. Serum creatine kinase (CK) levels tended to be higher in the LGMD2I than in the LGMD2H patients. Severe dilated cardiomyopathy was the presenting symptom in one LGMD2I patient and has subsequently been found in another three patients. Calf hypertrophy with proximal muscle wasting reminiscent of that seen in patients with Becker muscular dystrophy has been observed in the LGMD2I patients in our study, but is not a constant feature. No other muscular hypertrophy, including macroglossia, was noted. Two children presented with reactions to inhalation anesthetics (succinylcholine/halothane) during dental surgery, one with a masseter spasm and the other with severe rhabdomyolysis. Both of these patients recovered post- operatively. They showed persistently elevated resting CK levels and muscle biopsies with dystrophic features. Both were subsequently found to be L276I homozygotes. Recently, a German LGMD2I patient (compound heterozygote for L276I and V121E) was reported to also have had a malignant hyperthermia-like episode subsequent to inhalation anaesthetic [Walter et al., 2004]. This suggests that LGMD2I patients, in general, are at risk for reactions to inhalation anaesthetic. Unlike LGMD2I, to our knowledge, LGMD2H patients have shown none of the following characteristics: muscle hypertrophy, reaction to general anesthetics, or development of cardiomyopathy. In addition, none of the LGMD patients of either type that we have studied have shown signs of facial weakness or any respiratory symptoms; however, subtle respiratory difficulties cannot be ruled out [Dohna-Schwake et al., 2004]. Among the Hutterite LGMD families that we studied, there was one individual who was homozygous for FKRP L276I and heterozygous for TRIM32 D487N. This individual has proximal muscle weakness and a highly elevated CK level of 9,190 U/L. There were also six individuals who were homozygous for TRIM32 D487N and heterozygous for FKRP L276I, representing two families (a father and daughter from one family and a set of four siblings from another family). The father is ambulatory but has proximal muscle weakness, a dystrophic muscle biopsy, and a CK level of 669 U/L. The daughter is asymptomatic at this time and her CK level is 267 U/L. In the remaining family, all four siblings have CK levels Z10 maximum normal (range 1,700–2,960 U/ L), one has had a clearly dystrophic muscle biopsy, and two show proximal weakness but they are all ambulatory. Within both of these families, there are eight individuals who are heterozygous for both mutations. Seven of these individuals were available for study and were clinically normal (as examined by C.R.G.). CK values for these individuals ranged from 35–294 U/L. DISCUSSION We have demonstrated unexpected locus heterogeneity for LGMD in the Hutterite population, and have identified patients who are homozygous for a missense mutation (D487N) in TRIM32 or homozygous for a missense mutation (L276I) in FKRP. This provides another example of genetic heterogeneity of an autosomal recessive disease in a genetically isolated population. Both locus and allelic heterogeneity were found for LGMD in the Amish, another Anabaptist isolate [Duclos et al., 1998]. At this time, there is no evidence for a third locus causing LGMD in this population. 1 1 52^411 35^294 1 33 44^1,460 322^26,087 Six of these are also heterozygous for LGMD2I with no obviously di¡erent phenotype. One of these is also heterozygous for LGMD2H with no obviously di¡erent phenotype. b a 23 8 Both Heterozygote Double Heterozygote na na Absent (23) Absent (7), not studied (1) Not studied (49) Dilated cardiomyopathy (4), normal (10), not Studied (5) Not studied (23) Not Studied (8) Absent (49) Absent (8), Borderline (2), Present (9) 49 19b LGMD2I/ FKRP L276I Heterozygote Homozygote na 2^25 mean=12 10 81^5,556 Normal (13), not studied (28) 41a Homozygote LGMD2H/ TRIM32 D487N 9^42 mean=24 Absent (41) Mean Multiples of Max Normal Highest Resting CK (U/litre) Cardiac Status Di¡erences Between LGMD2H and LGMD2I in the Hutterites Calf Hypertrophy Status Mutation Age of Onset (years) Number of Individuals TABLE 2. Clinical 13 Asymptomatic (7^42), 4 Assisted ambulation (42^47), 3 Wheelchair bound (60^66), 21 Ambulatory (13^53) 49 Asymptomatic (6^77) 1 Deceased/congestive heart failure (40), 1 Assisted ambulation (40), 17 Ambulatory (5^50) 23 Asymptomatic (6^70) 7 Asymptomatic (12^47), Not studied/Deceased (1) FROSK ET AL. Current status (age range in years) 42 LGMD2H appears to be more frequent in the Schmiedeleut subdivision of the Hutterites, whereas LGMD2I appears to be more frequent in the Dariusleut. Currently, we do not have an accurate estimate of the relative frequencies of the two mutations in each of the subdivisions. Overall, we have ascertained 58 Canadian Hutterite LGMD patients and the Canadian Hutterite population is estimated to be 28,020 (Statistics Canada; www.statcan.ca). Thus, the estimated prevalence of LGMD in this population is at least 1 in 483. This is very much higher than the highest prevalence reported to date of 1 in 14,493 (69 per million) in the Guipúzcoa population in Spain [Urtasun et al., 1998]. There is considerable clinical heterogeneity for both LGMD2H and LGMD2I in spite of a uniform communal lifestyle and only one mutation for each of the LGMDs. A wide spectrum in clinical severity has been previously reported for LGMD2I and ascribed to the various mutations found in compound heterozygotes [Mercuri et al., 2003]. We have observed similarly large clinical variation, although all our patients are homozygous for the FKRP L276I mutation. This was also seen in a recent study by Walter et al. [2004] in which 13 out of 20 patients from nonconsanguineous matings were homozygous for this mutation and showed similar clinical variability. Our impression is that patients with LGMD2I present earlier, follow a more severe course with possible cardiomyopathy (Poppe et al., submitted manuscript), and have higher serum CK levels than LGMD2H patients, although we may be underascertaining more mildly affected LGMD2I patients. A comprehensive ascertainment of LGMD in the Hutterites is needed to provide accurate information on the prevalence, penetrance of the genotypes, and clinical variability of LGMD. In addition, there is no indication of any interaction between the two loci as individuals with mutations at both loci are indistinguishable from those with mutations at only one locus (Table 1). This is not surprising due to the apparently different mechanisms by which these genes appear to cause muscular dystrophy [Esapa et al., 2002; Frosk et al., 2002]. Presumably, the only situation that might result in a more severe phenotype would be a double mutation homozygote. It appears that all Hutterite LGMDs are of either type 2H or type 2I. This will make it possible to provide accurate noninvasive diagnostic and carrier testing for LGMD in Hutterites. Specific tests for these two mutations are currently being established in the molecular diagnostic laboratory at the Health Sciences Centre, Winnipeg, Manitoba. Such a DNA-based approach is not yet practical for the non-Hutterite LGMD population because of the marked locus and allelic heterogeneity. Given the high incidence of LGMD2I carriers in the Hutterite population, and the risk of cardiomyopathy and anaesthetic reactions in this group, we would suggest that genetic testing of at-risk individuals even below the normal age of consent for such testing should be considered and discussed with the families. The FKRP L276I mutation appears to be common worldwide, with respect to LGMD-causing mutations. Carrier frequency is estimated to be 1 out of 306 on the basis of controls typed for L276I [Brockington et al., 2001b; de Paula et al., 2003; Walter et al., 2004; this study]. In addition, patients homozygous for L276I from 28 nonconsanguineous families have been reported [Brockington et al., 2001b; Poppe et al., 2003; Walter et al., 2004]. Our analysis indicates that L276I may be a founder mutation, as all Hutterite and non-Hutterite disease chromosomes tested to date carry the low frequency T allele (14%) at an intragenic SNP (c.135C4T) and the G allele at rs3810288 in the putative A COMMON LGMD2I FOUNDER MUTATION promoter of FKRP (with one exception). The L276I mutation with the C allele at rs3810288 (Patient NCL-10; Fig. 1) is consistent with being a recombinant chromosome but due to the lack of phase information for most of the genotypes this cannot be firmly established. The T allele of c.135C4T and the G allele of rs3810288 have been shown to be associated with a further 26 L276I chromosomes from German patients [Walter et al., 2004], strengthening the evidence for a founder mutation. Markers as far away from the L276I mutation as 0.25 Mb in each direction show readily detectable linkage disequilibrium; however, markers 0.75– 1.0 Mb away show very little linkage disequilibrium in the samples used in this study. This is strong evidence that L276I has arisen only once. The small common core haplotype is an indication that the mutation may have occurred long ago. Further analysis of SNPs in and around FKRP and additional patients will be needed to confirm that most, if not all, copies of L276I in the contemporary population are identical by descent and to accurately estimate the age of the mutation. The relative frequency of L276I in Caucasians, compared to other LGMD-causing mutations, and the high likelihood that it is a founder mutation, are readily explained by genetic drift. However, given the postulated function of FKRP, it is tempting to speculate that a selective advantage may also be contributing to the maintenance of this allele. FKRP is thought to be a glycosyltransferase, and its mutations affect the glycosylation of a-dystroglycan, an essential component of muscle cell membranes [Durbeej et al., 1998a; Esapa et al., 2002; Hewitt and Grewal, 2003]. An immunoblot of muscle from an L276I homozygote shows a decreased level of fully glycosylated a-dystroglycan (Fig. 2). Two other groups have recently reported variably decreased levels of a-dystroglycan in patients homozygous for L276I as well [Brown et al., 2004; Walter et al., 2004]. a-Dystroglycan is known to be expressed in numerous tissues and has been shown to be the receptor for the entry of two different types of pathogens [Cao et al., 1998; Durbeej et al., 1998b; Rambukkana et al., 1998]. It is FIGURE 2. Immunodetection of glycosylated a-dystroglycan. Immuno£uorescence staining of skeletal muscle from a control individual (a) and from LGMD2I Patient G-01 (b) with antiglycosylated a-dystroglycan antibody (IIH6C4, Upstate). c: Reduction of a-dystroglycan expression in skeletal muscle of a patient (lane 2) compared to control muscle (lane 1) by immunoblot. No reduction is apparent in b-dystroglycan. Equal loading determined by Ponceau S staining (not shown). 43 possible that an FKRP L276I heterozygote with a mild defect in glycosylation may have a partial resistance to these or other pathogens. Over long periods this advantage would then increase the prevalence of the FKRP L276I allele in areas where the pathogen is endemic. On the basis of the data presented here, it appears that the frequent occurrence of L276I is not the result of multiple de novo mutations as was previously thought [Bushby and Beckmann, 2003]. Instead, our findings suggest this mutation has occurred once and became prevalent through either genetic drift, selective advantage, or some combination of both. ACKNOWLEDGMENTS We are indebted to the patients and their families for their participation in this study. We thank Drs. T. Bree, F. Booth, C. Bourque, K. Brownell, A. Hoke, W. Ilse, T. Ladd, N. Lowry, C. Toth, and S. Weizman for patient samples, and Dr. T. Zelinski for control samples. We thank Dr. T. Hudson and A. Verner for facilitating the genomewide scan in the Montreal Genome Centre (McGill University and Genome Quebec Innovation Centre), J. Crumley for maintaining the genealogical database for many years and for the XBase computer programs, J. Loredo-Osti for helpful discussions, and L. Cree and M. Buddles for mutation analysis in the Newcastle patients. V. Straub and M. Zaik were supported by the German Research Society (DFG Str 498/3–2, SPP 1086) and the Krupp-Stiftung. The Newcastle Muscle Centre receives financial support from the Muscular Dystrophy Campaign. REFERENCES Brockington M, Blake DJ, Prandini P, Brown SC, Torelli S, Benson MA, Ponting CP, Estournet B, Romero NB, Mercuri E, Voit T, Sewry CA, Guicheney P, Muntoni F. 2001a. Mutations in the Fukutin-related protein gene (FKRP) cause a form of congenital muscular dystrophy with secondary laminin alpha2 deficiency and abnormal glycosylation of alpha-dystroglycan. Am J Hum Genet 69:1198–1209. Brockington M, Yuva Y, Prandini P, Brown SC, Torelli S, Benson MA, Herrmann R, Anderson LVB, Bashir R, Burgunder JM, Fallet S, Romero N, Fardeau M, Straub V, Storey G, Pollitt C, Richard I, Sewry CA, Bushby K, Voit T, Blake DJ, Muntoni F. 2001b. Mutations in the fukutin-related protein gene (FKRP) identify limb girdle muscular dystrophy 2I as a milder allelic variant of congenital muscular dystrophy MDC1C. Hum Mol Genet 10:2851–2859. Brockington M, Blake DJ, Torelli S, Brown SC, Muntoni F. 2002. The gene for a novel glycosyltransferase is mutated in congenital muscular dystrophy MDC1C and limb girdle muscular dystrophy 2I. Neuromuscul Disord 12:233–234. Brown SC, Torelli S, Brockington M, Yuva Y, Jimenez C, Feng L, Anderson L, Ugo I, Kroger S, Bushby K, Voit T, Sewry C, Muntoni F. 2004. Abnormalities in alpha-dystroglycan expression in MDC1C and LGMD2I muscular dystrophies. Am J Pathol 164:727–737. Bushby KM. 1999a. Making sense of the limb-girdle muscular dystrophies. Brain 122:1403–1420. Bushby KM. 1999b. The limb-girdle muscular dystrophies-multiple genes, multiple mechanisms. Hum Mol Genet 8:1875–1882. Bushby KM, Beckmann JS. 2003. The 105th ENMC sponsored workshop: pathogenesis in the non-sarcoglycan limb-girdle muscular dystrophies, Naarden, April 12-14, 2002. Neuromuscul Disord 13:80–90. 44 FROSK ET AL. Cao W, Henry MD, Borrow P, Yamada H, Elder JH, Ravkov EV, Nichol ST, Compans RW, Campbell KP, Oldstone MB. 1998. Identification of alpha-dystroglycan as a receptor for lymphocytic choriomeningitis virus and Lassa fever virus. Science 282:2079–2081. de Paula F, Vieira N, Starling A, Yamamoto LU, Lima B, de Cassia PR, Vainzof M, Nigro V, Zatz M. 2003. Asymptomatic carriers for homozygous novel mutations in the FKRP gene: the other end of the spectrum. Eur J Hum Genet 11:923–930. Dohna-Schwake C, Ragette R, Mellies U, Straub V, Teschler H, Voit T. 2004. Respiratory function in congenital muscular dystrophy and limb girdle muscular dystrophy 2I. Neurology 62:513–514. Driss A, Amouri R, Ben Hamida C, Souilem S, Gouider-Khouja N, Ben Hamida M, Hentati F. 2000. A new locus for autosomal recessive limb-girdle muscular dystrophy in a large consanguineous Tunisian family maps to chromosome 19q13.3. Neuromuscul Disord 10:240–246. Duclos F, Broux O, Bourg N, Straub V, Feldman GL, Sunada Y, Lim LE, Piccolo F, Cutshall S, Gary F, Quetier F, Kaplan JC, Jackson CE, Beckmann JS, Campbell KP. 1998. Beta-sarcoglycan: genomic analysis and identification of a novel missense mutation in the LGMD2E Amish isolate. Neuromuscul Disord 8:30–38. Durbeej M, Henry MD, Campbell KP. 1998a. Dystroglycan in development and disease. Curr Opin Cell Biol 10:594–601. Durbeej M, Henry MD, Ferletta M, Campbell KP, Ekblom P. 1998b. Distribution of dystroglycan in normal adult mouse tissues. J Histochem Cytochem 46:449–457. Emery AE. 1991. Population frequencies of inherited neuromuscular diseases—a world survey. Neuromuscul Disord 1:19–29. Esapa CT, Benson MA, Schroder JE, Martin-Rendon E, Brockington M, Brown SC, Muntoni F, Kroger S, Blake DJ. 2002. Functional requirements for fukutin-related protein in the Golgi apparatus. Hum Mol Genet 11:3319–3331. Freemont PS. 2000. RING for destruction? Curr Biol 10:R84–R87. Frosk P, Weiler T, Nylen E, Sudha T, Greenberg CR, Morgan K, Fujiwara TM, Wrogemann K. 2002. Limb-girdle muscular dystrophy type 2H associated with mutation in TRIM32, a putative E3-ubiquitin-ligase gene. Am J Hum Genet 70:663–672. Hewitt JE, Grewal PK. 2003. Glycosylation defects in inherited muscle disease. Cell Mol Life Sci 60:251–258. Horn EJ, Albor A, Liu Y, El Hizawi S, Vanderbeek GE, Babcock M, Bowden GT, Hennings H, Lozano G, Weinberg WC, KuleszMartin M. 2004. RING protein Trim32 associated with skin carcinogenesis has anti-apoptotic and E3-ubiquitin ligase properties. Carcinogenesis 25:157–167. Hostetler JA. 1985. History and relevance of the Hutterite population for genetic studies. Am J Med Genet 22:453–462. Jones EM, Menzel S, Espinosa R, III, Le Beau MM, Bell GI, Takeda J. 1994. Localization of the gene encoding a neutral amino acid transporter-like protein to human chromosome band 19q13.3 and characterization of a simple sequence repeat DNA polymorphism. Genomics 23:490–491. Kaplan JC, Fontaine B. 2004. Neuromuscular disorders: gene location. Neuromuscul Disord 14:85–106. Kruglyak L, Daly MJ, Reeve-Daly MP, Lander ES. 1996. Parametric and nonparametric linkage analysis: a unified multipoint approach. Am J Hum Genet 58:1347–1363. Louhichi N, Triki C, Quijano-Roy S, Richard P, Makri S, Meziou M, Estournet B, Mrad S, Romero NB, Ayadi H, Guicheney P, Fakhfakh F. 2003. New FKRP mutations causing congenital muscular dystrophy associated with mental retardation and central nervous system abnormalities. Identification of a founder mutation in Tunisian families. Neurogenetics 5:27–34. Markianos K, Daly MJ, Kruglyak L. 2001. Efficient multipoint linkage analysis through reduction of inheritance space. Am J Hum Genet 68:963–977. Mercuri E, Brockington M, Straub V, Quijano-Roy S, Yuva Y, Herrmann R, Brown SC, Torelli S, Dubowitz V, Blake DJ, Romero NB, Estournet B, Sewry CA, Guicheney P, Voit T, Muntoni F. 2003. Phenotypic spectrum associated with mutations in the fukutin-related protein gene. Ann Neurol 53: 537–542. Mira MT, Alcais A, Van Thuc N, Thai VH, Huong NT, Ba NN, Verner A, Hudson TJ, Abel L, Schurr E. 2003. Chromosome 6q25 is linked to susceptibility to leprosy in a Vietnamese population. Nat Genet 33:412–415. Nimgaonkar VL, Fujiwara TM, Dutta M, Wood J, Gentry K, Maendel S, Morgan K, Eaton J. 2000. Low prevalence of psychoses among the Hutterites, an isolated religious community. Am J Psychiatry 157:1065–1070. Parra FC, Amado RC, Lambertucci JR, Rocha J, Antunes CM, Pena SD. 2003. Color and genomic ancestry in Brazilians. Proc Natl Acad Sci USA 100:177–182. Poppe M, Cree L, Bourke J, Eagle M, Anderson LV, Birchall D, Brockington M, Buddles M, Busby M, Muntoni F, Wills A, Bushby K. 2003. The phenotype of limb-girdle muscular dystrophy type 2I. Neurology 60:1246–1251. Rambukkana A, Yamada H, Zanazzi G, Mathus T, Salzer JL, Yurchenco PD, Campbell KP, Fischetti VA. 1998. Role of alphadystroglycan as a Schwann cell receptor for Mycobacterium leprae. Science 282:2076–2079. Reymond A, Meroni G, Fantozzi A, Merla G, Cairo S, Luzi L, Riganelli D, Zanaria E, Messali S, Cainarca S, Guffanti A, Minucci S, Pelicci PG, Ballabio A. 2001. The tripartite motif family identifies cell compartments. EMBO J 20:2140–2151. Shokeir MH, Kobrinsky NL. 1976. Autosomal recessive muscular dystrophy in Manitoba Hutterites. Clin Genet 9:197–202. Urtasun M, Saenz A, Roudaut C, Poza JJ, Urtizberea JA, Cobo AM, Richard I, Garcia BF, Leturcq F, Kaplan JC, Marti Masso JF, Beckmann JS, Lopez dM. 1998. Limb-girdle muscular dystrophy in Guipuzcoa (Basque Country, Spain). Brain 121:1735–1747. Walter MC, Petersen JA, Stucka R, Fischer D, Schroder R, Vorgerd M, Schroers A, Schreiber H, Hanemann CO, Knirsch U, Rosenbohm A, Huebner A, Barisic N, Horvath R, Komoly S, Reilich P, Muller-Felber W, Pongratz D, Muller JS, Auerswald EA, Lochmuller H. 2004. FKRP (826C4A) frequently causes limb-girdle muscular dystrophy in German patients. J Med Genet 41:e50. Weiler T, Greenberg CR, Zelinski T, Nylen E, Coghlan G, Crumley MJ, Fujiwara TM, Morgan K, Wrogemann K. 1998a. A gene for autosomal recessive limb-girdle muscular dystrophy in Manitoba Hutterites maps to chromosome region 9q31-q33: evidence for another limb-girdle muscular dystrophy locus. Am J Hum Genet 63:140–147. Weiler T, Sudha T, Brunham L, Nylen E, Patel L, Halliday W, Greenberg CR, Wrogemann K. 1998b. Genetic heterogeneity of limb girdle muscular dystrophy in Manitoba Hutterites. Am J Hum Genet 63(Suppl):A392–A392. Zatz M, de Paula F, Starling A, Vainzof M. 2003. The 10 autosomal recessive limb-girdle muscular dystrophies. Neuromuscul Disord 13:532–544.
Baixar