☰
Explorar
Assinar em
Inscrever-se
Envio
×
Baixar
Sem categoria
000697070
EVALUATION OF THE EXPRESSION OF MexY EFFLUX
Abstract
Abstract
Detection of antimicrobial-resistant gram-negative
897-2 - Sociedade Brasileira de Microbiologia
220-1
Trabalho
Author(s) Fernanda Santos Freitas , Cristiane Carneiro Thompson
28ª REGEM Reunião de Genética de Microrganismos Exoproteome
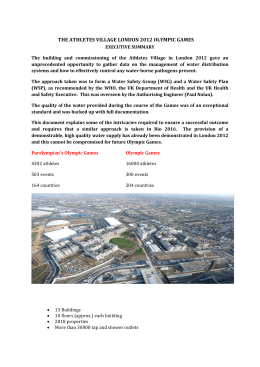
THE ATHLETES VILLAGE LONDON 2012 OLYMPIC GAMES