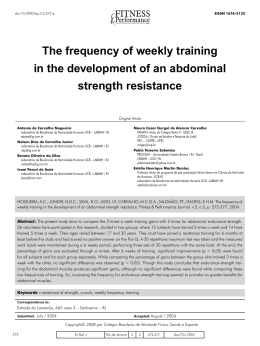
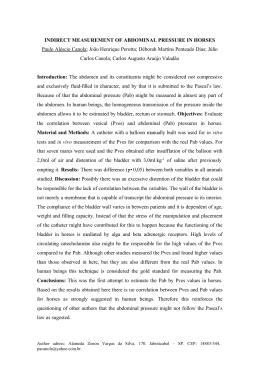
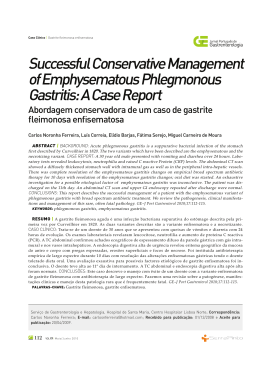
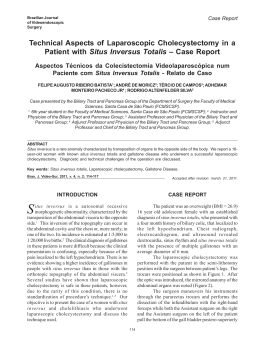
SCIENTIFIC FORUM Classification for Indications of Lipoabdominoplasty and Its Variations Wilson Novaes Matos Jr, MD; Ricardo Cavalcanti Ribeiro, MD; Ricardo Alves Marujo, MD; Rogerio Porto da Rocha, MD; Sergio Miguel da Silva Ribeiro, MD; and Fernando V. Carrillo Jiminez, MD Drs. Matos and Cavalcanti Ribeiro are Professors in the Postgraduate Course in Plastic Surgery at Santa Casa General Hospital (CESANTA) in Rio de Janeiro, Brazil. Drs. Jiminez and da Silva Ribeiro assisted Dr. Matos with the manuscript. Dr. Marujo is in private practice in São Paolo, Brazil. Dr. Porto da Rocha is Professor of Anatomy at the University of Medicine of Santos in São Paolo, Brazil. The authors are all members of the Brazilian Society of Plastic Surgery. Background: Lipoabdominoplasty, the combination of lipoplasty with classical abdominoplasty, presents new opportunities for the treatment of abdominal lipodystrophy. Objective: The author analyzed 211 patients who underwent lipoabdominoplasty from 2000 to 2004. Methods: After the preoperative physical examination, the patients were classified into 9 different groups according to the indications for the most appropriate technique in each case. Patient groups ranged from those presenting with mild fat panniculus and good quality skin to massive weight loss patients with a high degree of flaccidity. Techniques used in treating the various patient groups included lipoplasty alone, 3 variations of lipominiabdominoplasty, 4 variations of lipoabdominoplasty, and abdominoplasty alone. The surgical principles used in the variations of lipoabdominoplasty included dissection and sculpturing of the subcutaneous deep layer and superficial layer through lipoplasty, selective undermining and plication of the anterior rectus sheath, preservation of the perforator vessels, preservation of Scarpa’s fascia and deep fat, skin resection, and umbilical transposition. Results: Two hundred eleven patients were treated between January 2000 and May 2004. Results were good, with high patient satisfaction regardless of variations in technique. There was no loss of sensibility in the suprapubic region in any patients. Among patients who underwent lipoabdominoplasty, there were low complication rates of epidermolysis (1.5%), seroma (1%), hematoma (1%), and necrosis (0.1%). There was no incidence of seroma, necrosis, or hematoma in the lipominiabdominoplasty subgroups I and II; in subgroup III, there was a 2% incidence of necrosis. Seroma was noted in 2% of patients who underwent reverse lipominiabdominoplasty. Similar low complication rates were observed in other groups. Conclusions: The classification of lipoabdominoplasty indications offers good options for treatment of the abdominal region. Lipoplasty, selective undermining, and maintenance of Scarpa’s fascia help reduce surgical trauma that is the main factor affecting hematoma and necrosis rates. The learning curve for these classifications is fast because the described procedures are already familiar to most plastic surgeons. (Aesthetic Surg J 2006;26:417–431.) A bdominal plastic surgery has evolved greatly since Callia’s1 original description in 1965, in response to demands for better results, smaller scars, faster postoperative recovery and, above all, fewer postoperative complications. The introduction of lipoplasty, first reported by Illouz2 in 1980, revolutionized the treatment of lipodystrophy in all regions, and particularly in the abdominal area. Papers associating lipoplasty with abdominal plastic surgery involving a small skin resection were published by Hakme3 1985 and by Wilkinson4 in 1986. Several studies suggested clinical and therapeutic classifications for the treatment of abdominal lipodystrophy.5-7 The first description of the association between lipoplasty and full abdominoplasty was reported in 1991 by Matarasso,8,9 who performed lipoplasty of the abdominal flap with wide undermining and classified the areas that could be aspirated. In 1992, Illouz10 described an abdominoplasty without undermining after abdominal lipoplasty, naming it “mesh undermining,” with restricted indications. In 1999, Shestak11 published papers in which he associated lipoplasty, partial removal of suprapubic skin, and restricted undermining. In 1999 and 2000, Avelar12,13 proposed the overall treatment of the abdominal subcutaneous fat pad with deep lipoplasty, without undermining and without fat pad resection, using video AESTHETIC SURGERY JOURNAL ~ JULY/AUGUST 2006 417 SCIENTIFIC FORUM Table 1. Classification of lipoabdominoplasty and variations Procedure Subgroup Skin Muscles No flaccidity No diastasis I: Lipoplasty, suprapubic resection with or without lower plication Light/mild infraumbilical flaccidity With/without lower diastasis II: Lipoplasty, suprapubic resection and total or infraumbilical plication, downward traction of the umbilicus Light/mild infra- and supraumbilical flaccidity Partial or total diastasis III: Lipoplasty, suprapubic resection, plication, transposition of the umbilicus Mild infra- and supraumbilical flaccidity, high umbilicus Partial or total diastasis Lipoabdominoplasty Lipoplasty, total plication, supraumbilical resection Excessive skin over entire abdomen Total diastasis Classic abdominoplasty Dermolipectomy, herniorrhaphy, plication Excessive skin over entire abdomen Diastasis, ventral hernia Lipoplasty Lipominiabdominoplasty Figure 1. Lipoabdominoplasty classification. A, Lipominiabdominoplasty, Type I; B, Lipominiabdominoplasty, Type II; C, Lipominiabdominoplasty, Type III; D, Lipoabdominoplasty; E, Reverse lipoabdominoplasty; F, Vertical lipoabdominoplasty; G, Anchor lipoabdominoplasty; H, Postbariatric lipoabdominoplasty. 418 Aesthetic Surgery Journal ~ JULY/AUGUST 2006 Volume 26, Number 4 SCIENTIFIC FORUM A B Figure 2. Lipominiabdominoplasty Type I. A, After deep and superficial lipoplasty of the abdominal region, Scarpa’s fascia is visible, preserved with the deep fat tissue. B, An elliptical incision is made in Scarpa’s fascia for performance of the rectoabdominal muscle plication in the inferior abdominal region. A B Figure 3. Lipominiabdominoplasty Type II. A, After deep and superficial lipoplasty of abdominal region, Scarpa’s fascia is visible, preserved with the deep fat tissue in the hypogastrium. B, Umbilical suture in the midline before rectoabdominal plicature in patients with superior abdominal skin flaccidity. endoscopic diastasis suturing,14 with suprapubic and partial inframammary skin removal for the upper abdomen, without transposing the navel. And in 2001, Saldanha15,16 proposed the association of lipoplasty with classical abdominoplasty through performance of selective flap undermining, suturing of the rectoabdominal muscles, complete resection of the infra-umbilical skin, and umbilicus transposition, naming his technique “lipoabdominoplasty.” Since 2000, we have used this technique to treat the abdominal region. The varied indications were the basis for changes in surgical strategy and technique, depending Classification for Indications of Lipoabdominoplasty and Its Variations on the need for treatment of the abdominal structures. The classification of lipoabdominoplasty indications enabled us to standardize and systemize the associated lipoplasty and classic abdominoplasty techniques. It is based on 5 surgical phases: 1. Dissection and sculpturing of the subcutaneous deep layer and superficial layer through lipoplasty. 2. Selective undermining and plication of the anterior recti sheath. 3. Preservation of the perforator vessels. 4. Preservation of Scarpa’s fascia and deep fat. 5. Skin resection and umbilical transposition. AESTHETIC SURGERY JOURNAL ~ JULY/AUGUST 2006 419 SCIENTIFIC FORUM A B Figure 4. Lipominiabdodminoplasty Type III. After deep and superficial lipoplasty of the entire abdomen, selective undermining was performed in the area of diastasis for plicature. Scarpa’s fascia is visible, preserved with the perforant vessels in the inferior abdomen. B, An enlarged skin incision was made in the infraumbilical region (hypogastrium), resulting in a vertical scar. Then extended elliptical resection of the suprapubic skin was performed with transposition of the umbilicus and omphaloplasty. The umbilical oriface was closed, leaving a 3- to 4-cm scar at the hypogastrium region. Based on this analysis, we propose a new clinical-therapeutic abdomen classification to indicate the best technique for each case (Table 1, Figure 1). During the physical examination, we took note of skin features, such as elasticity, laxity, wrinkles, surface irregularities, and presence of scars. The position of the navel, its distance in relation to the pubis and xyphoid appendix, and scarring in the hypogastrium were used as initial parameters to indicate the amount of skin to be removed and the future positioning of the umbilical scar. The thickness, the amount, and the disposal of the fatty tissue were evaluated to estimate the amount of fat to be aspirated. We also diagnosed the presence, degree, and localization of rectoabdominal diastasis for plication (supraumbilical or infraumbilical localization) to better determine the best technique to be used. Body contouring lipodystrophies in other areas, such as the flanks, gluteus, sacrum, and pubis, were also evaluated. loss, and previous pregnancies can result in flaccidity, stretch marks, and loss of dermis elasticity. The subcutaneous abdominal tissue is divided into 2 layers, separated by Scarpa’s fascia. The areolar or the superficial layer is composed of small, firm, and compact adipocytes. The lamellar or deep layer, composed of regular and loose globules, 17 is where the largest amount of fat is found in abdominal lipodystrophy, and is thus the main layer to be treated. The rectoabdominal muscles are involved by aponeuroses that cross the midline; at this region, we observe flaccidity and diastasis of those muscles. According to Taylor,18 80% of the abdominal wall blood supply comes from the abdominal perforating branches of the lower and upper epigastric arteries. The other 20% comes from the intercostal arteries, loin arteries, and upper external iliac arteries. The lymph vessels run to the inguinal regions and armpits. Innervation is provided by the last 6 intercostal nerves and the great and small abdominogenital nerves. Applied Anatomy Surgical Technique The skin has particular attributes with respect to elasticity, thickness, and mobility. Alteration of the cutaneous tissue by factors related to obesity, weight Saline solution and epinephrine at a concentration of 1:1,000,00017 were infiltrated. The abdomen was aspirated by the “scanner” technique, with the cannula Preoperative Evaluation 420 Aesthetic Surgery Journal ~ JULY/AUGUST 2006 Volume 26, Number 4 SCIENTIFIC FORUM A B C D Figure 5. Lipoabdominoplasty. A, Deep and superficial lipoplasty. B, Lipoplasty of the superficial layer in the inferior abdomen with Scarpa’s fascia and the fat deep tissue preserved. Selective undermining was performed with a bistoury only in the diastasis region of the rectoabdominal muscle for plication in the superior abdomen and elliptical incision of Scarpa’s fascia in the inferior abdomen for the plicature. C, Rectoabdominal plicature and Scarpa’s fascia suture. Deep fat tissue over the inferior abdomen. D, Final result before elliptical skin resection and omphaloplasty. A B Figure 6. Anchor lipoabdominoplasty. A, Marking of the skin resection before lipoplasty. B, Skin resection after lipoplasty without flap undermining. Classification for Indications of Lipoabdominoplasty and Its Variations AESTHETIC SURGERY JOURNAL ~ JULY/AUGUST 2006 421 SCIENTIFIC FORUM A B C D Figure 7. A, C, Preopererative views of a 36-year-old woman with 1 previous pregnancy, mild abdominal lipodystrophy, and a flaccid inferior abdominal region. B, D, Postoperative views 8 months after lipominiabdominoplasty Type I and lipoplasty of the flanks and legs. 422 Aesthetic Surgery Journal ~ JULY/AUGUST 2006 Volume 26, Number 4 SCIENTIFIC FORUM A B Figure 8. A, Preoperative view of a 48-year-old woman with 2 previous pregnancies, previous breast augmentation, and inferior diastasis of the rectoabdominal muscles. B, Postoperative view 13 months after lipominiabdominoplasty Type I with plicature. Her breast implants were also replaced with round, high-profile silicone gel implants placed under the muscle. holes turned laterally, using short circular movements into the superficial and deep layers rather than conventional undermining. Infra-umbilical skin resection, plication of the rectoabdominal muscles, and mobilization of the umbilicus were performed, depending on the circumstances of each case. Scarpa’s fascia was always preserved, except in the classic abdominoplasty, to keep the superficial fatty layer flat, preserving lymphatic drainage and suprapubic sensibility. Aspirative drainage was used postoperatively, with the closed suction drain placed into the selected undermining region and removed by the third to fifth postoperative day in all cases in which lipoplasty was performed. Lipominiabdominoplasty I This technique was considered for patients who presented with light or mild skin flaccidity in the infraumbilical region, with or without inferior diastasis. After lipoplasty of the abdomen and surrounding areas was performed, an elliptical fuse of skin located in the suprapubic area,19 as well as the entire superficial fatty layer, was removed in such a way that the flap was advanced over the preserved Scarpa’s fascia (Figure 2, A). When inferior abdominal diastasis was present, Scarpa’s fascia was removed at the medial line to perform the rectoabdominal muscle plication in the inferior region and suture the superficial fascia borders (Figure 2, B). Lipominiabdominoplasty II Lipoplasty Lipoplasty was indicated exclusively for those patients who presented with a light or mild fat panniculus and good quality skin. Classification for Indications of Lipoabdominoplasty and Its Variations This procedure was indicated for patients with light or mild skin flaccidity at the upper and lower abdomen in whom partial or total diastasis and high positioning of the umbilical scar were present. After lipominiabdomino- AESTHETIC SURGERY JOURNAL ~ JULY/AUGUST 2006 423 SCIENTIFIC FORUM A B C D Figure 9. A, C, Preoperative views of a 45-year-old woman with 1 previous pregnancy, an inferior scar, abdominal lipodystrophy, excessive skin, and diastasis of the rectoabdominal muscles. B, D, Postoperative views 1 year after lipominiabdominoplasty Type II and lipoplasty of the waist. 424 Aesthetic Surgery Journal ~ JULY/AUGUST 2006 Volume 26, Number 4 SCIENTIFIC FORUM A B C D Figure 10. A, C, Preoperative views of a 42-year-old woman with 2 previous pregnancies, an inferior scar, abdominal lypodistrophy, excessive skin, and diastasis of the rectoabdominal muscles. B, D, Postoperative views 1 year after lipominiabdominoplasty Type III, breast augmentation, and lipoplasty of the waist. Classification for Indications of Lipoabdominoplasty and Its Variations AESTHETIC SURGERY JOURNAL ~ JULY/AUGUST 2006 425 SCIENTIFIC FORUM A B C D Figure 11. A, C, Preoperative views of a 45-year-old woman with 3 previous pregnancies, an inferior abdominal scar, excessive skin, and diastasis of the rectoabdominal muscles. B, D, Postoperative views 1 year after lipoabdominoplasty and associated mastopexy. 426 Aesthetic Surgery Journal ~ JULY/AUGUST 2006 Volume 26, Number 4 SCIENTIFIC FORUM A B Figure 12. A, Preoperative view of a 68-year-old woman with 2 previous pregnancies, 7 scars from previous surgery, excessive skin, and diastasis of the rectoabdominal muscles. B, Postoperative view 16 months after anchor lipoabdominoplasty. plasty as described previously, the umbilicus was “floated” by cutting it free from the underlying fascial attachments. Selective upper undermining at the region of diastasis for the plication was performed, and the umbilicus was repositioned 2 to 5 cm lower and sutured20 (Figure 3). Excessive skin at the lower region was removed by means of a suprapubic elliptical fuse. This technique could only be used in patients whose umbilicus position was originally high in relation to the pubis. Its goal was to treat the light or mild upper abdominal skin flaccidity that might occur after lipoplasty. Lipominiabdominoplasty III A lipominiabdominoplasty III was performed in patients with relevant skin flaccidity at the supra- and infra-umbilical region who lacked sufficient excess skin to enable flap traction to the pubic region because of a high umbilicus position. After lipoplasty, selective undermining at the midline, and partial or total plication, an Classification for Indications of Lipoabdominoplasty and Its Variations extended elliptical resection of suprapubic skin was performed, followed by transposition of the umbilicus and omphaloplasty. The umbilical orifice was closed, leaving a 3- to 4-cm scar at the hypogastrium region (Figure 4). Lipoabdominoplasty Lipoabdominoplasty was indicated for the patients with skin flaccidity over the entire abdomen and light to severe lipodystrophy with or without abdominal muscle diastasis.21 After aspiration of the deep and superficial abdomen and flanks layer, the umbilicus was isolated and the infraumbilical skin was resected as in a traditional abdominoplasty, preserving Scarpa’s fascia, the venous, arterial, and lymphatic vessels, and the innervation. Selective undermining at the medial diastasis area was performed close to the internal rectus abdominis muscle borders, preserving the abdominal perforating vessels. The partial resection of Scarpa’s fascia at the mid infra-umbilical line exposed the aponeurosis for conventional plication of the entire muscle AESTHETIC SURGERY JOURNAL ~ JULY/AUGUST 2006 427 SCIENTIFIC FORUM A B C D Figure 13. A, C, Preoperative views of a 42-year-old woman with 3 previous pregnancies and 60-kg weight loss. B, D, Postoperative views 1 year after lipoabdominoplasty, mastopexy, and lipoplasty of the waist. 428 Aesthetic Surgery Journal ~ JULY/AUGUST 2006 Volume 26, Number 4 SCIENTIFIC FORUM diastasis. The navel was transposed to achieve the “starshaped” omphaloplasty.15,16,23 Closing of the abdomen was performed in 3 planes: the superficial fat, deep dermis, and superficial skin (Figure 5). In cases of difficult traction, it was possible to complete the procedure with a small inverted “T” scar at the lower region.24,25 Lipoabdominoplasty in the atypical abdomen In patients with atypical abdominal variations related to the presence of pre-existing scars in the abdomen or to massive weight loss, we adapted the techniques in the previously described categories to the individual needs of each case. Table 2. Incidence of the indications Surgical technique % of indications Lipoabdominoplasty Lipoabdominoplasty in atypical abdomen Lipominiabdominoplasty I Lipominiabdominoplasty III Lipominiabdominoplasty II Classic abdominoplasty–herniorrhaphy 79.65 9.95 4.73 2.84 1.89 0.94 Results Reverse lipoabdominoplasty and anchor or vertical abdominoplasty In treating patients who had undergone massive weight loss, in whom great skin excess and adipose tissue were present, we performed the lipoabdominoplasty, using lipoplasty to undermine and thin out the flap, removing the skin according to the need of each case. A fuse of Scarpa’s fascia and deep fatty layers may be removed from the midline. The borders were sutured, even in those cases when there was no need to expose the aponeurosis for the plication. In this group of patients, we found atypical individual variations. Physical examination and abdominal ultrasound may diagnose hernias and scar adherences in the abdominal wall, which would contraindicate lipoplasty. Two hundred eleven patients underwent lipoabdominoplasty, lipominiabdominoplasty, or classical abdominoplasty between January 2000 and May 2004. Patient ages ranged from 28 to 69 years; all but one were female. We observed good results and high patient satisfaction with respect to abdominal profile appearance (Figures 7-13). Regardless of variations in technique, the abdomen was better modeled due to the use of lipoplasty to decrease the thickness of the adipose tissue. In the lipominiabdominoplasty subgroups Types I and II there was no incidence of seroma, necrosis, or hematoma. In the lipominiabdominoplasty subgroup Type III there was a 1% incidence of necrosis. Low complication rates for epidermolysis (1.5%), seroma (1%), hematoma (1%), and necrosis (0.1%) were noted for patients who underwent lipoabdominoplasty.31 We observed that the final scar is smaller than with classical abdominoplasty. There was no loss of sensibility in the suprapubic region in any patients. Overall, patients were able to return to their routine activities approximately 15 days postoperatively. We also found a low complication rate among patients with an atypical abdomen who underwent lipoabdominoplasty. Seroma was noted in 2% of patients who underwent reverse lipoabdominoplasty. Among patients who underwent anchor lipoabdominoplasty, epidermolysis was observed in 1.8% of cases, seroma in 1%, and hematoma in 0.1%. Among postbariatric patients, complications included epidermolysis (2.5%), seroma (1%), and hematoma (0.1%) (Table 3). Abdominoplasty Discussion Lipoplasty was contraindicated in the presence of abdominal wall hernias. In such cases, the traditional flap undermining, herniorrhaphy, abdominal muscle plication, and conventional dermolipectomy were performed.28-30 A thorough preoperative evaluation of the abdominal region is essential to diagnosis, classification, and selection of the technique most appropriate to each case. The principles and foundations of this classification system are In patients in whom a high degree of flaccidity of the inframammary fold was present, the excessive skin was removed through the inframammary reverse approach and, if necessary, selective undermining with diastasis plication was performed.26 It was possible to associate the suprapubic resection without transposing the umbilicus in cases of lower region flaccidity, as described by Avelar,12,13 Hakme,3 and Shestack.11 The same strategy was used with skin resection in a vertical or anchor lipoabdominoplasty, 27 depending on the position and location of the scars, and preserving the irrigation through the undermining by lipoplasty (Figure 6). Postbariatric lipoabdominoplasty Classification for Indications of Lipoabdominoplasty and Its Variations AESTHETIC SURGERY JOURNAL ~ JULY/AUGUST 2006 429 SCIENTIFIC FORUM Table 3. Percentage of complications Procedure % Seroma % Hematoma % Epidermolysis % Necrosis 0 0 0 1 2 1 1 0 0 0 0.1 0 0 0.1 0 0 0 1.5 0 1.8 2.5 0 0 1 0.1 0 0.5 0 Lipominiabdominoplasty I Lipominiabdominoplasty II Lipominiabdominoplasty III Lipoabdominoplasty Reverse lipoabdominoplasty Anchor lipoabdominoplasty Postobesity lipoabdominoplasty based on preservation of the anatomy of the vascular, lymphatic, and nervous systems of the abdominal wall, involving the two layers of the adipose tissue and the muscular groups. Through superficial and deep lipoplasty, the basic lipoabdominoplasty techniques, we can dissect the two layers of the abdominal fat and reach the abdominal flap with less trauma compared with dissection using a bovie, which splits up the perforator vessels emerging from the rectoabdominal muscles. Currently, this principle is used in 99.06% of our cases (Table 2). Even in those cases in which the adipose tissue is thin (4% of cases), we prefer to perform divulsion with lipoplasty suction cannulas without vacuum for flap undermining. Selective undermining performed with a bistoury only in the diastasis region of the rectoabdominal muscle for plication does not reach the perforator arteries, which are located 2 cm from the rectoabdominal muscle edge. Dissection by means of lipoplasty and selective undermining for plication replace the large-scale dissections of conventional abdominoplasty and lipectomy. 32 Since 2000, when we began using these techniques, we have found that they result in a broadened vascularized flap and decrease the incidence of complications, such as hematoma, epithelioisis, and necrosis. The preservation of Scarpa’s fascia and of the lower abdominal deep fat is important for the superior flap accommodation, and it is another important foundation of the technique, because anatomically and histologically speaking, the lymphatic vases are more numerous in this region.33 We believe that maintenance of the lymphatic system through this method is the main factor in the decrease in the incidence of seroma in the patient subgroup treated according to these principles. In those lipoabdominoplasty cases in which Scarpa’s fascia of the suprapubic region was removed completely, exposing the aponeurosis, we encountered seroma and observed a difference in elevation of the lower abdomen in relation to 430 Aesthetic Surgery Journal ~ JULY/AUGUST the pubis. Another important result was the lack of any sensibility loss in the lower abdomen in any of the cases. We routinely associate lipoabdominoplasty and its variations with lipoplasty of the flanks and outer thigh and lipografting in the gluteal-trocanterian regions, which allows for global harmonization of the body contour. In patients who have undergone great weight loss, lipoabdominoplasty enables thinning of the skin flap, prevents wide undermining, improves the final result, and reduces the complication rate. We can also apply this technique in cases of secondary abdominoplasty, when it is necessary to remove the fatty tissue and remaining excessive skin. Conclusion The preoperative evaluation and the correct indication of lipominiabdominoplasty, lipoabdominoplasty, and variations offer good options for abdominal region treatment, resulting in a more youthful appearance to the abdomen with less scarring and a lower incidence of major complications than traditional abdominal aesthetic surgery. Resection of adipose tissue through the lipoplasty cannula, selective undermining, and maintenance of the scarpa fascia and deep fat permit a better preservation of the vascular, lymphatic, and nervous systems associated with the abdomen. The resulting decrease in surgical trauma is the main factor in the decrease of hematoma and necrosis rates. The learning curve is fast because the described procedures utilize techniques and methods already familiar to most plastic surgeons. ■ References 1. Callia W. Contribuição para o estudo da correção cirúrgico do abdome pêndulo e globoso—Técnica original [dissertation]. Faculty of the Medical University of São Paulo, 1965. 2. IIlouz YG. Une nouvelle technique pour lês lipodystrophies localisées. Rev Chir Esth Franc 1980;April:6. 2006 Volume 26, Number 4 SCIENTIFIC FORUM 3. Hakme F. Technical details in the liposuction associated with abdominoplasty. Rev Bras Cir 1985;75:331. 27. Carreirão S, Pitanguy I, Correa WE, Caldeira MC. Abdominoplastia vertical. Uma técnica a ser lembrada. Ver Bras Cir 1983;79:184-194. 4. Wilkinson TS, Swartz BE. Individual modification in body contour surgery: the limited abdominoplasty. Plast Reconstr Surg 1986;779784. 28. Baker TJ, Gordon HL, Mosiouku PA. A template (pattern) method of abdominal lipectomy. Aesthetic Plast Surg 1997;21:167. 5. Bozola AR, Psillakis JM. Abdominoplasty: a new concept and classification for treatment. Plast Reconstr Surg 1988;82:983-993. 29. Nahas FX, Ishida J, Gemperli R, Ferreira MC. Abdominal wall closure after selective aponeurotic incision and undermining. Ann Plast Surg 1998;41:606-613. 6. Matarasso A. Abdominolipoplasty: A system of classification and treatment for combined abdominoplasty and suction assisted lipectomy. Aesthetic Plast Surg 1991;15:111-121. 30. Psillakis JM. Plastic surgery of the abdomen with improvement in the body contour. Physiopathology and treatment of the aponeurotic musculature. Clin Plast Surg 1984;11:465-467. 7. Pitanguy I, Salgado F, Murakami R, Radwanski HW, Manad R Jr. Abdominoplasty: classification and surgical techniques. Rev Bras Cir 1995;85:23-44. 31. Matarasso A. Awareness and avoidance of abdominoplasty complications. Aesthetic Plast Surg 1997;17:256-261. 8. Matarasso A. Liposuction as an adjunct to a full abdominoplasty. Plast Reconstr Surg 1995;95:829-836. 32. Dillerud E. Abdominoplasty combined with suction lipoplasty: a study of complication, revision, and risk factors in 487 cases. Ann Plast Surg 1990;25:333-338. 9. Matarasso A. Liposuction as an adjunct to a full abdominoplasty revisited. Plast Reconstr Surg 2000;106:1197-1206. 33. Lockwood T. High lateral-tension abdominoplasty with superficial fascial system suspension. Plast Reconstr Surg 1995;96:603-608. 10. Illouz YG. A new safe and aesthetic approach to suction abdominoplasty. Aesthetic Plast Surg 1992;16:237-245. 11. Shestak KC. Marriage abdominoplasty expands the miniabdominoplasty concept. Plast Reconstr Surg 1999;103:120-135. 12. Avelar JM. Uma nova técnica de abdominoplastia—sistema vascular fechado de retalho subdérmico dobrado sobre si memo combinado com lipoaspiração. Ver Brás Cir 1999;13:3-20. 13. Avelar JM. Abdominoplasty: a new technique without undermining and fat layer removal. Arq Catarinense de Méd 2000;29:147-149. Accepted for publication March 17, 2006. Presented at the ASAPS/ASERF/ISAPS International Symposium, New Orleans, Louisiana, May 4, 2005. Reprint requests: Wilson Novaes Matos Jr, MD, Av. Ana Costa, 151 – conj.74, Santos, São Paolo 11060, Brazil. Copyright © 2006 by The American Society for Aesthetic Plastic Surgery, Inc. 1090-820X/$32.00 doi:10.1016/j.asj.2006.05.003 14. Corrêa M. Videoendoscopic subscutaneous techniques for authentic reconstructive surgery. Plast Reconstr Surg 1995;96:446-453. 15. Saldanha OR, De Souza Pinto EB, Matos WN Jr, Lucon RL, Magalhaes FF, Bello EML. Lipoabdominoplasty without undermining. Aesthetic Surg J 2001;21:518-526. 16. Saldanha OR. Lipoabdominoplasty with selective and safe undermining. Aesthetic Plast Surg 2003;27:322-327. 17. Souza Pinto EB, de Erazo IPJ, Muniz A C, Prado Filho FSA, Salazar GH. Superficial liposuction. Aesthetic Plast Surg 1996;20:111-122. 18. Taylor GI. The superiorly based rectus abdominis flap: predicting and enhancing its blood supply based on an anatomic and clinical study. Plast Reconstr Surg 1988;81:721. 19. Uebel CO. Miniabdominoplasty—a new approach for body contouring. Presented at the 9th Annual Congress of the International Society of Aesthetic Surgery, New York, October 1987. 20. Delerm A. Refinements in abdominoplasty with emphasis on reimplantation of the umbilicus. Plast Reconstr Surg 1982;70:632-637. 21. Marques A, Brenda E, Pereira MD, De Castro M, Abramo AC. Abdominoplasty with two fusiform plications. Aesthetic Plast Surg 1996;20:249-251. 22. Abramo A, Viola JC, Marques A. The H approach to abdominal muscle aponeurosis for the improvement of body contour. Plast Reconstr Surg 1990;86:1008-1013. 23. Matos WN Jr. Onfaloplastia em forma de estrela. Arq Catarinense de Méd 2000;29:147-149. 24. Baroudi R, Moraes M. A “bicycle-handbar” type of incision for primary and secondary abdominoplasty. Aesthetic Plast Surg 1995;17:307-320. 25. Cardoso De Castro C, Marica Branco Cupello A, Cintra H. Limited incisions in abdominoplasty. Ann Plast Surg 1987;19:436-447. 26. Rebelo C, Franco T. Abdominoplasty with inframammary scar. Rev Bras Cir 1972;62:249. Classification for Indications of Lipoabdominoplasty and Its Variations AESTHETIC SURGERY JOURNAL ~ JULY/AUGUST 2006 431
Baixar