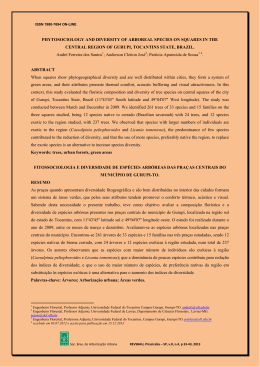
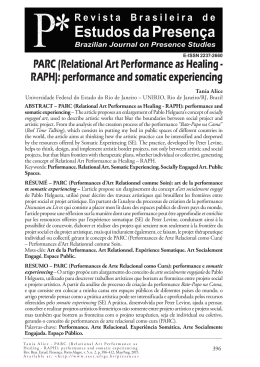
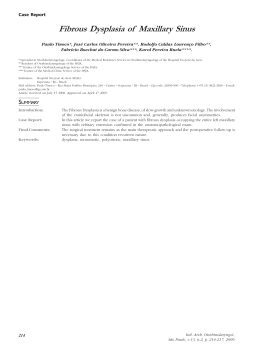
CASE REPORT Propranolol for extensive hemangiomas of infancy: two case reports Hemangiomas extensos da infância tratados com propranolol: relato de dois casos Luíza Helena dos Santos Cavaleiro1, Fernanda de Oliveira Viana1, Deborah Aben Athar Unger2, Maraya de Jesus Semblano Bittencourt3 Abstract Hemangiomas are the most common benign tumors of childhood. They show rapid growth, followed by a regression phase that culminates in the partial or total disappearance of the lesion. Therapeutic options should be evaluated for extensive cases. Systemic glucocorticoids are the therapy of choice; however, there are reports that propranolol offers better and faster results. We report two cases of large volume infantile hemangioma associated with functional limitation and aesthetic disfigurement, treated successfully with propranolol, a drug that comes as a therapeutic option providing satisfactory and maintained results, with few side effects. Keywords: Hemangioma; propranolol; therapeutics; adrenal cortex hormones. Resumo Hemangiomas são os tumores benignos mais frequentes da infância, apresentando como história natural crescimento rápido, seguido de uma fase de regressão que culmina com o desaparecimento parcial ou total da lesão. Opções terapêuticas devem ser avaliadas para casos extensos. Os glicocorticoides sistêmicos são a terapia de escolha; contudo, há relatos de que o propranolol oferece resultados melhores e mais rápidos. Este trabalho descreve dois casos de hemangioma infantil de grande volume associados à limitação funcional e desfiguração estética com significativa resposta ao propranolol, droga esta que surge como uma proposta terapêutica oferecendo resultados satisfatórios e mantidos, com poucos efeitos colaterais. Palavras-chave: Hemangioma; propranolol; terapêutica; corticosteroides. Introduction Hemangiomas are the most common benign tumors of infancy, with an incidence varying from 1% in newborns to 12% in children in the first year of life. They develop by the uncontrolled proliferation of vessels, grow fast during the first months of life and have a regression phase which ends in partial or total disappearance1,2. Although spontaneous regression makes expectant management an option, other therapies must be considered in cases of large infantile hemangiomas that cause compression of vital structures, present visceral involvement, disfigurement, or are located at a body orifice3,4. In such cases, systemic glycocorticoids are the treatment of choice: oral prednisone or prednisolone 2 to 4 mg/kg/day or pulse methylprednisolone1. However, some reports state that propanolol may provide better and faster results in the treatment of extensive hemangiomas3-5. In this paper, we describe two cases of infantile hemangioma that responded significantly to propanolol treatment. Case report Case 1 A three-month-old female infant presenting cleft lip and cleft palate. Dermatological examination showed extensive erythematous scaly lesions extending over the right hemiface, bilateral mandibular and cervical regions. Resident at the Service of Dermatology of Universidade Federal do Pará (UFPA), Belém (PA), Brazil. Master’s degree in Tropical diseases at UFPA; Adjunct Professor at Departament of Dermatology of UFPA, Belém (PA), Brazil. Master’s degree in Tropical diseases at UFPA; Physician at Fundação Santa Casa de Misericórdia do Pará, Belém (PA), Brazil. Conflit of interest: nothing to declare Submitted on: 09.01.2011. Accepted on: 28.04.2011 J Vasc Bras. 2011;10(2):173-176. 1 2 3 174 J Vasc Bras 2011, Vol. 10, Nº 2 Due to the involvement of the right periorbital region, the patient was unable to open her eye, and the lesions on the cervical region were obstructing the upper airways (Figure 1). She was treated with prednisone 1 mg/kg/day for one month, but without improvement. After cardiology assessment, propanolol 2 mg/kg every 8 hours was introduced with rigorous monitoring of arterial blood pressure, heart rate and glycemic levels. The patient presented significant improvement after one week of treatment; The lesion showed regression and became more plane, which enabled the patient to open her right eye normally (Figure 2). Despite clinical improvement of hemangioma, the patient died of septic complications. Case 2 Four-month-old female infant presenting with erythematous papules on the right preauricular regions, that had appeared at 20 days of life. The lesions had progressive growth and similar ones appeared. Dermatological examination showed erythematous scaly lesions of smooth consistency on the right frontal, right periocular, preauricular, mandibular and inferior lip regions (Figures 3A-B). After cardiologic assessment, she was given propanolol 2 mg/ kg every 8 hours, with dosage increase one month later, to 3 mg/kg every 8 hours. The lesions disappeared after four months of treatment (Figures 4A-B). Laboratory exams did not show alterations. Discussion Figure 1 - Scaly lesion on the inferior third of the face obstructing upper airways and eye opening at the right side. Propranolol for infantile hemangiomas - Cavaleiro LHS et al. It is believed that only 10 to 20% of hemangiomas require treatment. Indication of treatment is made in case of eye, upper airways and auditory canal obstruction, as well as those that cause heart failure and hemorrhage, and those that may turn into ulcers and disfigure the patient. Systemic corticoids are the treatment of choice for extensive hemangiomas1,2. They are usually given to patients in high dosages and for long periods, which makes the patient more prone to adverse effects such as hirsutism, cushingoid facies, hypertrophic cardiomyopathy, gastrointestinal, sleep and growth disorders2,6. Propanolol, a nonselective beta-blocker, has been pointed out as an alternative in more aggressive cases3,4,5,7, for its effects include: vasoconstriction immediately perceptible as a color alteration associated with palpable softening of the lesions, decrease in vascular endothelial growth factor expression (VEGF) and basic fibroblast growth factor (bFGF) due to protein kinase inhibition, which explains the progressive improvement of hemangioma; and capillary endothelial cell apoptosis deflagration. This drug should be used in the proliferative phase, in which pro-angiogenic factors, VEGF and bFGF are involved3. There is no consensus in literature about the right dosage. It is recommended to initiate the treatment with 0.16 mg/kg every 8 hours, which may be increased to 2 mg/kg/day3. The use of this medicine is not risk-free, and the patient may hypotension, bradycardia and asymptomatic hypoglycemia, so the patient must be previously assessed as to cardiologic features and have their arterial blood pressure, heart rate and glucose levels closely monitored4. The patients of the Figure 2 - Aspect of the lesion after propanolol (fourth day). Propranolol for infantile hemangiomas - Cavaleiro LHS et al. A J Vasc Bras 2011, Vol. 10, Nº 2 175 B Figure 3 - Erythematous scaly papules of smooth consistency on the right frontal, right periocular, preauricular, mandibular and inferior lip regions (A and B). A Figure 4 - Lesion aspect after propanolol (A and B). B 176 J Vasc Bras 2011, Vol. 10, Nº 2 cases described had no adverse effects to the drug, hence it may be considered a promising alternative for extensive hemangioma treatment with fast response. References 1. Serra AMS, Soares FMG, Cunha Jr AG, Costa IMC. Abordagem terapêutica dos hemangiomas cutâneos na infância. An Bras Dermatol. 2010;85:307-17. 2. Assunção BFG. Tumores e malformações vasculares. In: Sampaio SAP, Rivitti EA. Dermatologia. São Paulo: Artes Médicas; 2007. p. 1197-225. 3. Léauté-Labrèze C, Dumas de la Roque EC, Hubiche T, Boralevi F, Thambo JB, Taïeb A. Propranolol for severe hemangiomas of infancy. N Engl J Med. 2008; 358:2649-51. 4. Jadhav VM, Tolat SN. Dramatic response of propranolol in hemangioma: report of two cases. Indian J Dermatol Venereol Leprol. 2010;76:691-4. Propranolol for infantile hemangiomas - Cavaleiro LHS et al. 5. Siegfried EC, Keenan WJ, Al-Jureidini S. More on propranolol for hemangiomas of infancy. N Engl J Med. 2008;359:2846-7. 6. Dinehart SM, Kincannon J, Geronemus R. Hemangiomas: evaluation and treatment. Dermatol Surg. 2001;27:475-85. 7. Pérez SR, Mora PC, Rodríguez JDG, Sánchez FR, Torres JDP. Tratamiento del hemangioma infantil con propranolol. An Pediatr (Barc). 2010;72:152-4. Correspondence: Maraya de Jesus Semblano Bittencourt Travessa Vileta, 1.289, apto 302 CEP: 66087-422 – Belém (PA), Brazil E-mail: [email protected] Author’s contribution: Study conception and design: LHSC, FOV, DAAU, MJSB Data analysis and interpretation: LHSC, FOV, DAAU, MJSB Data collection: LHSC, FOV, DAAU, MJSB Writing: LHSC, FOV, DAAU, MJSB Critical analysis: LHSC, FOV, DAAU, MJSB Final approval*: LHSC, FOV, DAAU, MJSB Statistical analysis: N/A Overall responsibility: MJSB *All authors have read and approved the final version submitted to J Vasc Bras.
Baixar