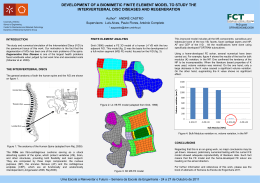
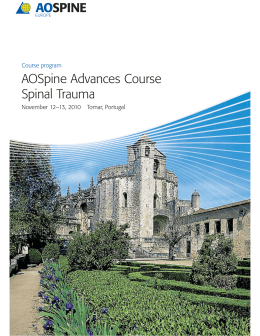
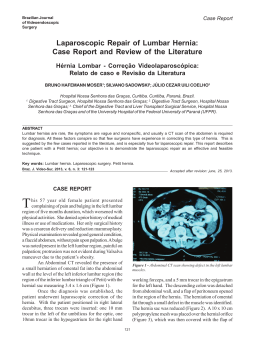
Artigo de atualização / update ARTICLE Adjacent segment disease of the lumbar spine: genetic versus biomechanical theories Síndrome transicional da coluna lumbar: teoria genética versus biomecânica Síndrome transicional de la columna lumbar: teoría genética versus biomecánica Lyonel Beaulieu Lalane1 Karen A. Weissmann Marcuson2 ABSTRACT resumo resumen KEYWORDS: Intervertebral disc/pathology; Lumbar vertebrae/surgery; transitional syndrome; Spinal fusion/ adverse effects descritores: Disco intervertebral/patologia; Vértebras lombares/cirurgia; Fusão vertebral/efeitos adversos descriptores: Disco intervertebral/patología; Vértebras lumbares/cirugía; Fusión vertebral/efectos adversos Adjacent segment disease has been considered a late complication of spinal fusion. It’s described as any degeneration that develops at mobile segments above or below a fused spinal segment. Several questions have arisen in the late years regarding this syndrome, we try to define it, describe it and determine if it’s caused by strain forces due to spinal arthrodesis or whether it’s the natural history of the degenerative spinal process. Possibilities on conservative and surgical management are discussed. Spinal degeneration is a pre – determined genetic process and therefore the involvement of unfused levels is an expected result. A doença do disco adjacente tem sido considerada como complicação tardia da cirurgia de artrodese vertebral. Ela é descrita como qualquer degeneração que ocorre nos segmentos móveis acima ou abaixo do segmento vertebral que passou pela cirurgia de artrodese. Muitos questionamentos têm sido apresentados nos últimos anos relacionados a esse problema e será apresentada e discutida a possível etiologia mecânica relacionada à realização da artrodese vertebral ou ao processo degenerativo vertebral do disco intervertebral. As possibilidades do tratamento conservador e cirúrgico são apresentadas e discutidas. A degeneração do disco intervertebral está relacionada à predisposição genética e o acometimento dos segmentos vertebrais que não sofreram cirurgia de artrodese é um acontecimento esperado. La enfermedad del disco adyacente ha sido considerada como una complicación tardía de la artrodesis vertebral. Ella es descrita como cualquier degeneración que ocurre en los segmentos movibles encima o abajo del segmento vertebral artrodesados. Muchas controversias se han presentado en los últimos años relacionados con ese problema. De esta forma será presentado y discutido la posible etiología mecánica relacionada con la formación de artrodesis vertebral y el proceso degenerativo vertebral del disco intervertebral. Las posibilidades del tratamiento conservador y quirúrgico serán presentadas y discutidas. La degeneración del disco intervertebral está relacionada con la predisposición genética, con la agresión de los segmentos vertebrales no artrodesados y una agresión esperada. Trabajo hecho no Hospital Exequeil Gonzalez Cortés e Fundación Médica San Cristoba. Santiago, Chile. MD, Instituto Traumatologico de Santiago, Chief of Spine group. Fundación Médica San Cristobal, member of the spine group. Member of the Sociedad Chilena de Ortopedia y Traumatología. Santiago, Chile. 2 MD, Hospital Exequeil Gonzalez Cortés, Staff member of the spine group. Fundación Médica San Cristoba. Santiago, Chile. 1 Recebido: 19/06/08 Aprovado: 30/09/08 COLUNA/COLUMNA. 2008;7(3)276-280 Adjacent segment disease of the lumbar spine: genetic versus biomechanical theories iNtroduction Lumbar fusion is a procedure that has been in development for more than 80 years. Adjacent segment disease or transitional syndrome has been considered a late complication of spine fusion, especially instrumented fusion. Not since the introduction of pedicle screw fixation, a device which allows a better control of intersegment mobility and higher load resistance, has this syndrome been an object of real study (Figure 1). A big metha – analysis of 101 articles documented 94.8% fusion rates in 5756 patients studied. In relation to pedicle screw fixation they described 12.5% rates of complications in which adjacent segment degeneration was included1. The incidence of this syndrome is low during the early years after surgery, but it progressively begins to increase in frequency during the late ones. It ranges in the lumbar spine between 5.6% at 2 years follow-up2 to 45% at 33 years after surgery3. No all patients are symptomatic. Actually most of findings are just X- rays ones at follow – up. Those patients that appear symptomatic may require surgery. In a study by Abla et al. 501 fusions in a period of 5 years, 8.2% required an extension of the original fusion, having the time between their first and second surgery an average of 16.4 years4. Can we consider these degenerative changes as being caused or triggered by surgery? Is the transitional syndrome a late complication of surgery, or is the normal degenerative process of the spine following its course? Is it natural History? Figure 1 Adjacent segment degeneration in a 55 year old female after a posterior fusion due to spinal stenosis. One year post-op 277 to allow its mobile segments to function normally. We know the degenerative process is the normal ageing progression of the spine. So how can we help not compromise the biomechanics of an already dysfunctional spine whose mechanics are already altered, hence the need for the original surgery anyhow. So can we state that this process is caused by our surgery in the opposite of it being triggered by it? Findings at an adjacent level disease We divided these findings in four main groups: disc degeneration, instability, stenosis and fracture. Disc degeneration can manifest itself as loss of disc height, disc space narrowing6 or herniated nucleus pulposus5 (Figure 2). Instability may be considered hipermobility of the segment or listhesis, a 7% incidence has been reported of adjacent instability after 2.4 years7 and 45% after 33 years2, Chen et al. define instability of the adjacent segment as a slippage of more than 4mm, either anterior or posterior and/or an angle change of more than 10° on flexion and extension8. Lateral listhesis is not mentioned in his definition, we consider it to be a component or manifestation of instability, no studies have stated a measurable parameter, it presence is in itself diagnostic. The motion segment above the fused level is the most commonly affected7-8. May be due to hypertrophic facet arthritis, Flavum Ligament hypertrophy and/or osteophyte formation5. Fractures are rare, but may be present as either a vertebral compression fracture9 or a stress fracture of the pars interarticularis on both sides10. Any of this findings by itself or combined constitute part of the adjacent segment syndrome. Risk factors that induce or trigger changes in the adjacent mobile segments are plentiful. It has been mentioned adjacent facet injury, long arthrodesis, sagittal alignment, coronal alignement, previously degenerated segments, lumbar stenosis, PLIF, age, osteoporosis, smoking, females and post-menopausic states5. Facet violation is not uncommon. Astudy by Shah et al. of 212 top-level screws where evaluation by computed tomography scan, violation occurred in 32% of the patients with a 20% of facet involvement. This may raise the subject of adjacent instability in those patients in Definition How could we define adjacent segment disease? Park et al. describes it as any degeneration that develops at mobile segments above or below a fused spinal segment5. We define it as any radiological changes developing at an adjacent segment, not necessarily immediately next to a previously fused level at least a year after spinal fusion. These findings are not necessarily symptomatic. However a time component has been stated in our definition. We cannot consider alterations at an adjacent level as a new pathology or complication, most probably below that time lapse, those findings were already there, a year is somewhat arbitrary, just the time it takes you not to consider it a failed back surgery syndrome. If we believe it to be a late complication of our surgery, then it was, maybe, our failure to maintain the basic biomechanics of the spine in order Figure 2 Disc narrowing, disc herniation, hipermobility found adjacent to a previously fused segment. Risk factors for adjacent segment degeneration COLUNA/COLUMNA. 2008;7(3)276-280 Lalane LB, Marcuson KAW 278 whom facet damage was present11. Instrumented arthrodesis have higher incidences of transitional syndromes than non instrumented ones, a study with computed tomography showed that the facet violation with pedicle screws is around a 30%11, in the literature one can find in studies up to 50%, therefore this would contribute to the acceleration of a degenerative process but secondary to facet injury, not due to stress forces. Other studies argue against this issue but no serious studies have been made to prove why unistrumented arthrodesis has lesser incidences of transitional syndrome. The length of the arthrodesis is a subject to be treated separately as is commonly blamed. Some studies suggest that the posterior ligamentary complex is important in maintaining the stability in the non fused segments in relation to the fused ones12. Out of 31 patients that underwent lumbar arthrodesis with pedicular screws in which the indemnity of the posterior ligamentary complex was maintained only two developed adjacent segment disease over the fused segments in comparison with 24% of the ones where the ligamentary complex was not preserved. Out of the caudal segments none of the patients with ligamentary complex indemnity developed any degenerative changes in relation to 5.6% in which it was not preserved12. The effect of PLIF was studied on adjacent segment changes, no correlation was found between radiological degeneration and clinical results, no risk factor were determined, only it was suspected that the horizontalization of the lamina and the facet tropism were one of the risk factors for secondary neurological deterioration in the adjacent segment13. Aging people have segment degeneration as a base, will see that this really does not explain the pathology, this people also have absence of other support structures, osteoporosis, especially in post – menopausal patients and they have little physical activity which also helps instability7. This is the core of genetic theory, that is why older patients are more prone to develop adjacent instability and why our interventions should be to stimulate spine stability through physiotherapy and exercise, we may prevent in a small percentage its development but not avoid it altogether. Segments above or below a previous fusion In 1950 Kellgren and Lawrence described that 50% of the population would develop degenerative changes by the age of 504. What is it that triggers increased changes in the segments above or below a fusion and why it that cranial segments are affected more often is? Studies performed both in dogs and human cadaveric specimens show increased mobility in the adjacent segments5,14, Chow et al. described that adjacent segments to fused ones must work more frequently towards the extremes of their functional ranges of motion15 especially after a multilevel fusion, therefore there is a transference of motion from the fused segments to the free ones that overload them. Cunningham et al.16 also described that there is a considerable increase of up to 45% in the intradiscal pressure of adjacent disc segment, the torque produced at the segment above is greater than the one below, and therefore this transfer of movement and load affect primarily the cranial one. Immediately next to and adjacent fused segment or supradjacent to it Transitional syndrome usually develops in the immediately next to a fusion. Instability requiring surgical stabilization commonly COLUNA/COLUMNA. 2008;7(3)276-280 develops in spine’s most mobiles segments. Therefore it’s expected that this same process develops in the levels around fusion, it’s impossible to determine whether the symptomatic changes that develop in a patient were due to the natural progression of degenerative changes or induced by fusion17. A short term study was developed at two years follow-up, where adjacent segments were studied with magnetic resonance, important degenerative changes in the immediately adjacent segments in relation to remote segments were present in up to 75% of the patients18 (Figure3). Figure 3 Supraadjacent segment disease in a 75 - years woman, 10 years after surgery. Notice how the immediately adjacent segment remains perfectly normal, while the supraadjacent disc has undergone severe degenerative changes Genetic versus biomechanical theories Fifty percent % of the population develops degenerative changes by the age of 5019, if a patient underwent surgery for spondylotic changes in a segment; the highest probability is that they develop the same pathology in the adjacent segments6. The radiological changes in the transition zones in asymptomatic fusions at ten years have the same frequency as the changes observed in control patients that haven’t undergone surgery20. However there is the feeling that the mechanical stress under which the immediately adjacent segment to an arthrodesis are submitted, suffer an accelerated degenerative process20. From a biochemical perspective Cole found considerable changes in the metabolism and composition of the adjacent disc to a fused segment21-22. Has adjacent segment disease a short or long termed etiology As previously mentioned, degenerative changes may appear as early as two years after the intervention19. We defined the presence of adjacent segment disease after a year of surgery, but if we believe in the genetic theory, those changes being the normal progression can either be there before surgery or evolve rapidly after it independent on time. As age is a prognosis factor for its development, older patients should be more predisposed to early and higher rates of segment instability. So though Abla et al. report 16 years average appearance of these changes4, earlier changes are not to be excluded. Traumatic versus degenerative etiologies to transitional syndrome If degenerative changes were due to overstress in adjacent segments, then there would be no difference in the incidence between traumatic or degenerative surgery, however this is not the case, traumatic surgery has very little incidence of transitional syndrome in comparison to degenerative surgery, this mainly supports a degenerative surgery over a biomechanical one. Adjacent segment disease of the lumbar spine: genetic versus biomechanical theories Previously engaged levels versus healthy ones in adjacent degeneration It’s reasonable to consider that a previously degenerated disc is prone to develop adjacent instability faster than a healthy level, even if this last one is submitted to shear stress forces. The biomechanical theory considers that the stress forces applied to the unfused disc are higher with more fused segments, due to a longer lever effect; healthy disc should be more resilent to this effect. Throckmorton et al. did a retrospective study, with a two year follow- up were they reviewed the clinical outcomes of this two groups, validated with the SF-36 scores and Magnetic Resonance. Twenty patients where fused adjacent to a degenerative level, five to a normal one, no adverse impact was detected in the adjacent degenerated level group, with a power analysis that validated this data with a 98% certainty, therefore it’s not a matter of stress forces, for this are equally well tolerated in a degenerated level23. Short versus long fusions. Does it matter? Long fusions imply a larger lever, so they are expected to produce more stress on the non fused segments, the longest fusions are made in scoliosis, for those patients whose fusion ended at L5 level a follow-up was made for up to 14 years, it concluded that 61% of the patients developed disc degeneration in the L5 – S1 level, this was associate with a significant forward shift in sagital balance and revision surgery24. We believe than more the length of the fusion is the last level involved that matters. Rinella et al. studied the effect of age and distal fusion levels comparing fusions ending in T11L2 to those ending L3-L4, higher rates of transition syndrome where found in the more distal arthrodesis25. Management Based in the radiographic evaluations, Transitional syndrome apparently does not correlate with a poor prognosis4. This is why it doesn’t necessarily need a surgical treatment. Conservative treatment may be considered with emphasis in pain control and optimizing quality of life. In order to consider surgery we must consider that the problem is being caused by the instability or the secondary spinal stenosis in the lumbar spine, in the cervical spine. Chen et al. described instability in transitional syndrome as a listhesis of more than 4mm or an angular variation higher than 10°7-8, Schlegel et al. defined instability as a listhesis in continuity to a fused segment or significant malalignement whether in the coronal or sagittal plane without specifying measurements26. What consideration should we take when we think surgery, we should asses what kind of involvement there is in order to chose the best treatment, is there compression or instability. How many levels are involved and how long was the previous arthrodesis, which was the last level fused and what option do we have of extending this fusion, of course things we must consider for any patient are age, bone quality and co morbidities. And of course we must never forget to try and explain the physiopathology of the disease, why did this happen and how could I have avoided it. In order to solve the problem we have three alternatives, decompression without fusion, arthrodesis whether instrumented or not and in the future we might consider using a disc arthoplasty. We can consider only decompressing in those patients with no proven 279 instability, in the presence of a single unilateral radiculopathy, lateral disc herniations or single level foraminal stenosis due to osteophyte formation. This would be the minimal useful surgery we could offer a patient, its advantages are a shorter surgical time and therefore the co morbidities associated and the preservation of the segment mobility, however we cannot predict whether instability will develop in the segment after laminoforaminotomy4. It would be mandatory to respect the respective facets, eventual fusion may occur. To approach the patient considering fusion without instrumentation is a mistake, Whitecloud et al. observed an 80% of non union in non instrumented patients27. Satisfactory results have been obtained with the instrumented extension of fusion and decompression, the same Whitecloud et al. saw that their rate of non-union fell to 17% with the use of instrumented fusion27, Chen et al. reported a 5.1% of non union in his prolonged fusion using this technique7 but adjacent segment disease may then develop in the next adjacent level. A new possibility is to consider the use of disc arthoplasty, it was published a case report concerning the use of a Bryan disc in the two altered levels above a previous fusion on the cervico – thoracic junction, it had a good result at short term follow-up, but we must wait and see how it actually performs28. The down part of surgery is that this is a very complex surgery in an already involved segment, complication described for this surgery are persistent pain, CSF leakage, fracture of the osteosinthesis instrumentation, non union, higher infection risk, excessive blood loss and higher risk of neurological damage5. There is evidence that the percentage of complications is higher in patients that require fusion of multiple segments as opposed to those that only require a one level fusion4. The outcome of surgery is not good, Park et al. considered that post – operative pain is the only predictor of a poor result in patients submitted to decompression by a transitional syndrome5, but Abla et al. observed that the affectivity of surgery is 30 to 70% in different series, other than pain, other aetiologies for failed back surgery syndrome must be under consideration4. Medicine is moving towards prevention more than treatment, so how could we prevent transitional syndrome. If we favour the degenerative theory, the only solution we might offer our patient is gene therapy to treat any predetermined degenerative changes, this is still under research and as yet nothing has been proved concerning this matter. If we go with the biomechanical theory there are some things we could do, dynamic stabilization, whether with disc arthroplasty or dynamic instrumentation is an option. Guyer et al. published 63 to 85% of good results with disc arthoplasty, however for the moments indications are limited29, An 8.6 year follow-up (7 to 10 years) of “ProDisc I” showed a 26% of transitional syndrome at 34 studied levels30, so under a degenerative perspective arthroplasty does not prevent adjacent instability, under a biomechanical perspective, disc arthoplasty does not modify degenerative changes of the posterior spinal complex, where degenerative disease may begin either in the operated segment or the ones adjacent to it. However the presence of a disc does not interfere with intradiscal pressure in the segments above it, a study by Dmitriev et al. was performed in the cervical spine it was a human in vitro study of 10 cadavers concerning the C5- C6 junction, the bodies where COLUNA/COLUMNA. 2008;7(3)276-280 Lalane LB, Marcuson KAW 280 classified as either control, undergoing disc arthoplasty, allograft and plating plus allograft, the spines where submitted to axial rotation, flexo-extension and bending. The intradiscal pressure was not altered in either the arthoplasty or the control groups, this was most significant in flexo-extension where fused subjects had significantly higher intradiscal pressure than both the arthoplasty and control group. Range of movement though less than the control group was maintained in the arthoplasty group30. Perhaps the absence of strain in the adjacent segments will somehow prevent adjacent segment disease, there is not enough follow up to conclude either way. Hashimoto et al. compared the incidence at five years follow-up of adjacent segmented disease and revision surgery in posterolateral fusion and those fused with the artificial Graf ligament. At the first group between 25 and 43% of the patients where affected, of those 18.5% required surgery, in the second group six to 18% presented adjacent instability and of those 5.6% required revision surgery32. So there is a degree of prevention in dynamic stabilizations. Sengupta et al. published 19% of revision surgery with the use of dynamic stabilization33, this would avoid the strain over the above segment but wouldn’t prevent the natural history of the pathology. REFERENCES 1. Dickman CA, Yahiro MA, Lu HT, Melkerson MN. Surgical treatment alternatives for fixation of unstable fractures of the thoracic and lumbar spine. A meta-analysis. Spine. 1994; 19(20 Suppl):2266S-2273S. 2. Kuslich SD, Danielson G, Dowdle JD, Sherman J, Fredrickson B, Yuan H, Griffith SL. Four-year follow-up results of lumbar spine arthrodesis using the Bagby and Kuslich lumbar fusion cage. Spine. 2000; 25(20):2656-62. 3. Lehmann TR, Spratt KF, Tozzi JE, Weinstein JN, Reinarz SJ, el-Khoury GY, Colby H. Long-term follow-up of lower lumbar fusion patients. Spine. 1987; 12(2):97-104. 4. Abla AA, El Kadi H, Bost J, Maroon JC, Wert M, Abla A. Degenerative changes above and below lumbar fusion. Contemp Spine Surg. 2006;7(2):1-5. 5. Park P, Garton HJ, Gala VC, Hoff JT, McGillicuddy JE. Adjacent segment disease after lumbar or lumbosacral fusion : review of the literature. Spine. 2004; 29(17): 1938-44. Review. 6. Miyakoshi N, Abe E, Shimada Y, Okuyama K, Suzuki T, Sato K. Outcome of one-level posterior interbody fusion for spondylolisthesis and postoperative intervertebral disc degeneration adjacent to the fusion. Spine. 2000; 25(14):1837-42. 7. Chen WJ, Lai PL, Niu CC, Chen LH, Fu TS, Wong CB. Surgical treatment of adjacent instability after lumbar spine fusion. Spine. 2001; 26(22):E519-24. 8. Chen WJ, Lai PL, Chen LH. Adjacent instability after instrumented lumbar fusion. Chang Gung Med J. 2003; 26(11):792-8. COLUNA/COLUMNA. 2008;7(3)276-280 Conclusion Adjacent segment disease is a difficult and controversial pathology, its diagnosis and treatment are complicated and unfortunately it seems we cannot yet prevent it. However we do not consider it as previously described a late complication of spine fusion. Most of the literature reviewed support that degenerative changes are already present or developing when we decide to fix a segment. Seventy five percent (75%) of degenerative changes at mobile segments at only two years follow up are described, despite the average 16 years in the development of adjacent instability. So we cannot blame stress forces for what nature is responsible. Adjacent segment degeneration is the natural progression of the patient’s spine, we believe that with our interference we trigger or accelerate the process but we do not produce it, that is why dynamic stabilization aids in diminishing the probability of transitional syndrome, it does not eliminate it. When we figure out how to stop, avoid or treat the normal degenerative process, aging as we more commonly know it, we will prevent this disease. Gene therapy is our next step. 9. Etebar S, Cahill DW. Risk factors for adjacent-segment failure following lumbar fixation with rigid instrumentation for degenerative instability. J Neurosurg. 1999; 90(2 Suppl):163-9. 10.Brunet JA, Wiley LJ. Acquired spondylolysis after spinal fusion. J Bone Joint Surg Br. 1984; 66(5):720-4. 11.Shah RR, Mohammed S, Saifuddin A, Taylor BA. Radiologic evaluation of adjacent superior segment facet joint violation following transpedicular instrumentation of the lumbar spine. Spine. 2003; 28(3):272-5. 12.Lai PL, Chen LH, Niu CC, Fu TS, Chen WJ. Relation between laminectomy and development of adjacent segment instability after lumbar fusion with pedicle fixation. Spine. 2004; 29(22):2527-32; discussion 2532. 13.Okuda S, Iwasaki M, Miyauchi A, Aono H, Morita M, Yamamoto T. l Risk factors for adjacent segment degeneration after PLIF. Spine. 2004; 29(14): 1535-40. 14.Bastian L, Lange U, Knop C, Tusch G, Blauth M. Evaluation of the mobility of adjacent segments after posterior thoracolumbar fixation: a biomechanical study. Eur Spine J. 2001; 10(4):295-300. 15.C how DH, Luk KD, Evans JH, Leong JC. Effects of short anterior lumbar interbody fusion on biomechanics of neighboring unfused segments. Spine. 1996; 21(5):549-55. 16.Cunningham BW, Kotani Y, McNulty PS, Cappuccino A, McAfee PC. The effect of spinal destabilization and instrumentation on lumbar intradiscal pressure: an in vitro biomechanical analysis. Spine. 1997; 22(22):2655-63. 17.Emery SE, Bohlman HH, Bolesta MJ, Jones PK. Anterior cervical decompression and arthrodesis for the treatment of cervical spondylotic myelopathy. Two to seventeen-year follow-up. J Bone Joint Surg Am. 1998; 80(7):941-51. 18.Kulkarni V, Rajshekhar V, Raghuram L. Accelerated spondylotic changes adjacent to the fused segment following central cervical corpectomy: magnetic resonance imaging study evidence. J Neurosurg. 2004;100(1 Suppl Spine):2-6. Comment in: J Neurosurg. 2004; 100(1 Suppl Spine):1; discussion 1. 19.Kellgren JH, Lawrence JS. Osteo-arthrosis and disc degeneration in an urban population. Ann Rheum Dis. 1958;17(4):388-97. 20.Hambly MF, Wiltse LL, Raghavan N, Schneiderman G, Koenig C. The transition zone above a lumbosacral fusion. Spine. 1998; 23(16):1785-92. 21.Cole TC, Burkhardt D, Ghosh P, Ryan M, Taylor T. Effects of spinal fusion on the proteoglycans of the canine intervertebral disc. J Orthop Res. 1985; 3(3):277-91. 22.Cole TC, Ghosh P, Hannan NJ, Taylor TK, Bellenger CR. The response of the canine intervertebral disc to immobilization produced by spinal arthrodesis is dependent on constitutional factors. J Orthop Res. 1987; 5(3):337-47. Correspondência Lyonel Beaulieu Lalane Luis Pasteur 5292, Vitacura, Santiago, Chile Tel.: + 56-2 7549500 E-mail: [email protected] [email protected]
Download