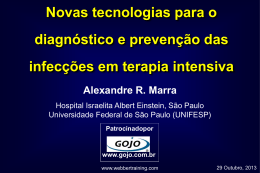
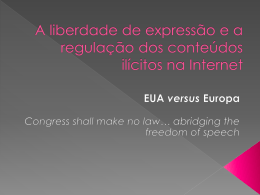
Outros exames complementares • Glicemia e eletrólitos – Descartar hipoglicemia e distúrbio metabólico • Coagulograma – Base para anticoagulação/ trombólise • HMG e plaquetas – Afastar coagulopatias • Enzimas cardíacas – Identificar IAM/ risco de cardioembolismo • Perfil lipídico – Identificar fator de risco • ECG – Arritimias/ risco de cardioembolismo • LCR Escala de Cincinnati Medidas gerais TAC/ RM de crânio ECG Testes sanguíneos ABCD2 ≥4 Terapia apropriada Articles Score ABCD2 Validation and refinement of scoresto predict very early stroke risk after transient ischaemicattack SClaiborneJohnston, Peter M Rothwell, Mai N Nguyen-Huynh, Matthew FGiles, Jacob SElkins, Allan LBernstein, Stephen Sidney Summary Background We aimed to validate two similar existing prognostic scores for early risk of stroke after transient ischaemic attack (TIA) and to derive and validate a unified score optimised for prediction of 2-day stroke risk to inform emergency management. Methods The California and ABCD scores were validated in four independent groups of patients (n=2893) diagnosed with TIA in emergency departments and clinics in defined populations in the USA and UK. Prognostic value was quantified with c statistics. The two groups used to derive the original scores (n=1916) were used to derive a new unified score based on logistic regression. Findings The two existing scores predicted the risk of stroke similarly in each of the four validation cohorts, for stroke risks at 2 days, 7 days, and 90 days (c statistics 0· 60–0· 81). In both derivation groups, c statistics were improved for a unified score based on five factors (age ≥60 years [1 point]; blood pressure ≥140/ 90 mm H g [1]; clinical features: unilateral weakness [2], speech impairment without weakness [1]; duration ≥60 min [2] or 10–59 min [1]; and diabetes [1]). This score, ABCD2, validated well (c statistics 0· 62–0· 83); overall, 1012 (21%) of patients were classified as high risk (score 6–7, 8· 1% 2-day risk), 2169 (45%) as moderate risk (score 4–5, 4· 1%), and 1628 (34%) as low risk (score 0–3, 1· 0%). Implications Existing prognostic scores for stroke risk after TIA validate well on multiple independent cohorts, but the unified ABCD2 score is likely to be most predictive. Patients at high risk need immediate evaluation to optimise stroke prevention. Introduction score was developed to predict stroke within 90 days and Lancet 2007; 369: 283–92 SeeComment page251 StrokeService, Department of Neurology, University of California, SanFrancisco, CA94143-0114, USA (SCJohnston MD, MNNguyen-Huynh MD, JSElkinsMD); Stroke Prevention ResearchUnit, UniversityDepartment of Clinical Neurology, Radcliffe Infirmary, Oxford, UK (PMRothwell MD, MFGilesMRCP); and Division of Research, Kaiser-Permanente Northern California, Oakland, CA, USA(SCJohnston, ALBernstain MD, SSidneyMD) Correspondenceto: Dr SClaiborneJohnston [email protected] Score ABCD2 • Age ≥60 1 ponto • Blood pressure 1 ponto – PS≥140mmHg – PD≥90mmHg • Baixo risco: <4 • Moderado risco: 4-5 • Alto risco: >5 • Clinical features – Hemiparesia ou 2 pontos – Distúrbio de fala sem hemiparesia 1 ponto • Duration of TIA – 10-59min 1 ponto – ≥60min 2 pontos • Diabetes 1 ponto Score ABCD2 Stroke risk •1628 (34%) – low risk (<4) – 1,0% at 2 days – 1,2% at 7 days – 3,1% at 90 days •2169 (45%) – moderate risk (4 or 5) – 4,1% at 2 days – 5,9% at 7 days – 9,8% at 90 days •1012 (21%) – high risk (>5) – 8,1% at 2 days – 11,7% at 7 days – 17,8% at 90 days Score ABCD2 Stroke risk •1628 (34%) – low risk (<4) – 1,0% at 2 days – 1,2% at 7 days – 3,1% at 90 days •2169 (45%) – moderate risk (4 or 5) – 4,1% at 2 days – 5,9% at 7 days – 9,8% at 90 days •1012 (21%) – high risk (>5) – 8,1% at 2 days – 11,7% at 7 days – 17,8% at 90 days Escala de Cincinnati Medidas gerais TAC de crânio ECG Testes sanguíneos ABCD2 ≥4 Terapia apropriada Não Investigação ambulatorial Escala de Cincinnati Medidas gerais TAC de crânio ECG Testes sanguíneos SIM Internação Testes sanguíneos Ecodoppler de carótidas Ecocardiograma RM AngioTC Holter ABCD2 ≥4 Terapia apropriada Não Investigação ambulatorial Tratamento pós fase aguda • • • • • Monitorização de dados vitais Avaliação de risco Prevenir acidente vascular encefálico grave Controlar hipertensão Iniciar terapia antitrombótica após descartar hemorragia • Tratar doença base Regime •Clopidogrel + Aspirina – 21 dias •Clopidogrel – 90 dias Superior a Aspirina isolada em •Prevenção de AVE •Sem diferença em eventos hemorrágicos fter transient ischaemicattack: and meta-analysis Articles Prognóstico y transient attack (TIA), studies ofischaemic stroke risk after TIA are Risk ofischaemic stroke early afterbut transient attack: onflicting results. However, reliable estimation of this risk is necessary for a systematic review and nical trials, and public education. Wemeta-analysis therefore did a systematic review of all Matthew FGiles, Peter M Rothwell Summary Lancet Neurol 2007; 6: 1063–72 Published Online November 12, 2007 DOI:10.1016/S14744422(07)70274-0 StrokePreventionResearch n7 days of Stroke TIA were use of electronic databases andofby hand Background is oftenidentifi precededed by by transient ischaemic attack (TIA), but studies stroke risk after areUnivers Lancet Ne urol 2007; 6: 10 Unit,TIA Oxford ity logistically difficult and abstracts. have yielded Stroke conflicting results. reliable estimation thiswere risk is necessary forof C Publis he d Online nals, and conference risks at 2However, days and 7 days after of TIA Department linic al November 12, 2007 planning effective service provision, clinical trials, and public education. We therefore did a systematic Neurology, review of all Radc liffeInfirmary, ogeneity were done, if possible, after categorisation by study method, setting, DOI:10.1016/S1474studies of stroke risk early af ter TIA. •Em pessoas com AIT •Incidência de AVE: Oxford, UK(MF4422(07 GilesD hil, )7P 0274-0 PMRothwell FRS C P) PreventionResea troke Methods All studies of stroke risk within 7 days of TIA were identified by use of electronic databases and by hand Unit, OxfordUniversity Corre sponde searches of reference lists, relevant journals, and conference abstracts. Stroke risks at 2 days and 7 days after TIA werenceDto: epartment of Clinical ncluded, which reported stroke risk in 10 126 TIA patients. The pooled stroke calculated overall and analyses for heterogeneity were done, if possible, after categorisation by study method, setting, Matthe wFGiles,Neurology, Stroke RadcliffeInfir xford, UK(MFGilesDPh ys,population, but there was substantial heterogeneity between studies (p<0· 0001), with Prevention ReseaOPrc and treatment. h Unit, Oxford MRothwell FRCP) ofnc Celinic wever, the risks reported in individual studies over different durations of UniversityDepartme Corresnt ponde to: al Findings 18 independent cohorts were included, which reported stroke risk in 10 126 TIA patients. The pooled stroke atthe wFrma Gilesry, , Stroke Neurology, RadcM liff eInfi aysrisk vswas 8–90 days, 89,5)p<0· 0001), andwas thesubstantial heterogeneity between 5· 2% (95% r=0· CI 3· 9–6· at 7 days, but there heterogeneity betweenstudies studies (p<0· 0001), with Prevention Research Unit, WoodstockRoad, Oxford risks ranging fromand 0% totreatment. 12· 8%. However, risks reported individual over different of UniversityDepartment of method, setting, Thethelowest risks inwere seenstudies in studies of durations OX26HA, UK Neurology, RadcliffeInfirm were highly correlated (0–7 days vs 8–90 days, r=0· 89, p<0· 0001), and the heterogeneity between studies WoodstockRoad, Oxford ke follow-up services (0· 9% [95% CI 0· 0–1· 9], four studies) and the highest risks in was almost fully explained by study method, setting, and treatment. The lowest risks were seen inmatthew.giles studies of @ OX26HA, UK clneuro.ox.ac t treatment (11· 0% in [8·specialist 6–13· 5], three studies). Results were forand stroke emergency treatment stroke services (0· 9% [95% CI 0· 0–1· 9], similar four studies) the highest risks in .uk matthew.giles@ – 11% na 1ª semana – 24-29% ao longo dos 5 anos seguintes population-based studies without urgent treatment (11· 0% [8· 6–13· 5], three studies). Results were similar for stroke risk at 2 days. clneuro.ox.ac.uk Prognóstico Conclusões • AIT é preditor de AVEi • Até 20% dos AVEi são precedidos por AIT • Até 30% dos pacientes não buscam auxílio médico após AIT • Mudança no estilo de vida • Tratamento da doença base OBRIGADO
Download