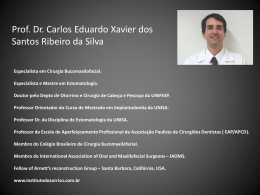
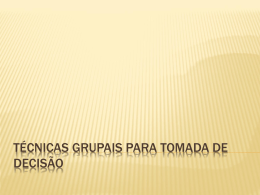
Necessidade de cirurgia urgente Francisco Moscoso Costa • 14H00 – Urgência Interna • Chamada do Serviço de Cirurgia Geral • “ … tenho aqui uma senhora de 67 anos que precisa ser operada mas está a fazer anticoagulante novo, Dabigatrano 110mg …” 1ª Questão Qual a melhor atitude ? 1. A doente pode ser já operada, o Dabigatrano 110mg mostrou melhor perfil de segurança vs varfarina 2. A cirurgia está contraindicada nas próximas 24horas 3. Vou avaliar o risco-benefício 4. A doente não tem queixas do foro cardiovascular logo não está indicada avaliação pela Cardiologia 3 História Clínica • ML, Sexo feminino com 67 anos de idade • FRCV: HTA / Diabetes tipo 2 • AP: Fibrilhação auricular paroxistica diagnosticada em Agosto/2012 por episódio de palpitações Sem outros antecedentes relevantes • Medicação habitual: – – – – Metformina 850mg 3xdia Ramipril 5mg 1xdia peq. almoço Amlodipina 5mg 1xdia jantar Dabigatrano 110mg 2xdia ( aprox. 10h e 22h ) 4 História Clínica • Recorreu ontem ao SU por quadro de dor abdominal difusa com início apos o almoço. • Em observação durante a tarde- melhoria sintomática alta sem diagnóstico conclusivo- indicação para vigilância e reavaliação de agravamento dos sintomas. 5 História Clínica • Recorreu novamente ao hospital hoje ao final da manhã por agravamento das dor abdominal associada a náuseas e vómitos. • Apresentava-se prostrada; TA:143/85mmHg; FC:85/min; ACP inocente Empastamento abdominal com dor à descompressão . 6 História Clínica • Rx de abdomen- ar na cavidade peritoneal • Rotura intestinal - Cirurgia urgente 7 História Clínica • Avaliação analítica: – Hb 13,4g/dl, Htc 42,4%, VGM 93,4fl – Leucócitos 12,4x10 9, N 85% – Creatinina 1,2mg/dl, ureia 67mg/dl (Cl Creat 45ml/min, MDRD) Na+ 143mmol/L, K+ 4,67 mmol/L – ALT 55 U/L, – PCR 10 mg/dl 8 História Clínica ECG 9 2ª Questão Qual a melhor atitude ? 1. Ecocardiograma para avaliar a dimensão da auricula esquerda e estimar o risco trombótico 2. As melhores ferramentas para avaliar o risco são o score CHADSVASC2 e HAS-BLED 3. Se a doente está estável, sem hemorragia ativa não necessito mais exames, não vale a pena atrasar a cirurgia 4. As melhores ferramentas para avaliar o risco são o score CHADS2 e HEMORR2HAGES 10 Avaliação do risco 1. Avaliação do risco trombótico de parar a medicação CHA2DS2-VASc Total score N Adjusted stroke rate (%/year)* 0 1 0.0 1 1 422 1.3 2 2 1230 2.2 3 1730 3.2 4 1718 4.0 5 1159 6.7 6 679 9.8 CHA2DS2-VASc criteria Score Congestive heart failure/ left ventricular dysfunction 1 Hypertension Age 75 years Diabetes mellitus 1 Stroke/transient ischaemic attack/TE 2 Vascular disease (prior myocardial infarction, peripheral artery disease or aortic plaque) 1 7 294 9.6 8 82 6.7 Age 65–74 years 1 9 14 15.2 Sex category (i.e. female gender) TE = thromboembolism 1 *Adjusted for warfarin use. Theoretical rates without therapy; assuming that warfarin provides a 64% reduction in stroke risk, based on Hart RG et al. 2007. Lip G et al. Chest 2010;137:263–72; Lip G et al. Stroke 2010;41:2731–8; ESC guidelines: Camm J et al. Eur Heart J 2010;31:2369–429; Hart RG et al. Ann Intern Med 2007;146:857–67 13 The 2012 ESC guidelines recommend oral anticoagulation in patients with ≥1 risk factors for stroke CHA2DS2-VASc score Recommended therapy 0 Either Aspirin 75–325 mg daily or no antithrombotic therapy Preferred choice is no antithrombotic therapy 1 Either OAC* or Aspirin 75–325 mg daily Preferred choice is OAC 2 OAC* *OAC, such as a VKA, adjusted to an intensity range of INR 2.0–3.0 (target 2.5). New OAC drugs, which may be viable alternatives to a VKA, may ultimately be considered (e.g. dabigatran etexilate). ESC = European Society of Cardiology; INR = international normalized ratio; OAC = oral anticoagulation; VKA = vitamin K antagonist ESC guidelines: Camm J et al. Eur Heart J 2010;31:2369–429 Disclaimer: Dabigatran etexilate is now approved for clinical use in stroke prevention in atrial fibrillation in certain countries. Please check local prescribing information for further details. 14 2. Avaliação do risco Hemorrágico HAS-BLED HAS-BLED risk criteria Hypertension (SBP >160 mmHg) Abnormal renal or liver function (1 point each) Score 1 1 or 2 HAS-BLED total score N Number Bleeds per 100 of bleeds patient-years* 0 798 9 1.13 1 1286 13 1.02 2 744 14 1.88 Stroke 1 3 187 7 3.74 Bleeding 1 4 46 4 8.70 5 8 1 12.5 6 2 0 0.0 7 0 – – 8 0 – – 9 0 – – (history or predisposition) Labile INRs 1 Elderly 1 (e.g. age >65 years) D rugs† or alcohol (1 point each) 1 or 2 *P value for trend = 0.007; †Antiplatelets and non-steroidal anti-inflammatories; INR = international normalized ratio; SBP = systolic blood pressure 16 Pisters R et al. Ches. 2010;138:1093–100; ESC guidelines: Camm J et al. Eur Heart J 2010;31:2369–429 HAS-BLED • HAS-BLED – Melhor preditor que os scores mais antigos (ATRIA / HEMORR2HAGES) • Melhor preditor de hemorragia intracraneana 17 “ patients with non–end-stage chronic kidney disease had an increased risk of stroke or systemic thromboembolism (hazard ratio, 1.49; 95% confidence interval [CI], 1.38 to 1.59; P<0.001)” 18 RISCO trombótico e hemorrágico • CHADSVASC2 = 4 - 4% AVC/ano • HAS-BLED = 1 - 1,02 hemorragias por cada 100 dts • Disfunção Renal – Cl. Creatinina 45ml/min (MDRD) 3ª Questão Qual a melhor opção? 1. Só se pode avançar para cirurgia quando INR<2 2. É sempre seguro 12 horas após a última toma 3. Pode avançar para cirurgia desde que efetuada ponte com HBPM 4. Nenhuma das anteriores 20 Qual a urgência cirurgica? Hipótese 1 A cirurgia pode ser protelada > 12h Hipótese 2 A cirurgia não pode ser protelada Como avaliar o efeito anticoagulante do dabigatrano? 4ª Questão Qual a melhor opção? 1. Avaliar o INR 2. Não há maneira de avaliar esta terapêutica 3. Se a cirurgia é urgente não vale a pena avaliar 4. O aPTT pode ajudar nesta situação 5. Nenhuma das anteriores 24 Avaliar a anticoagulação Avaliar a anticoagulação • aPTT – avaliação qualitativa • TT (Tempo Trombina) e Dabigatran calibrated Hemoclot thrombin inhibitor assay • ECT (Ecarin clotting time) Interpretation of Point-of-care INR Results in Patients Treated with Dabigatran ,Joanne van Ryn, et al. AJM 2012 Pharmacotherapy Dabigatran in Clinical Practice Rangadham Nagarakanti et al. aPTT • Prático e disponível no SU • Útil para determinar um efeito anticoagulante excessivo (aPTT >80s , 2 a 3 x LSN) • Valor dentro dos valores de referência – exclui a presença de efeito anticoagulante ( Compliance?) • A maioria dos doentes sob dabigatrano terão aPTT 1,5 a 2x (45 a 60s) embora este método não deva ser utilizado para avaliação quantitativa da coagulação aPTT e ralação com a concentração plasmatica de Dabigatrano Interpretation of Point-of-care INR Results in Patients Treated with Dabigatran ,Joanne van Ryn, et al. AJM 2012 TT / Dabigatran calibrated Hemoclot thrombin inhibitor assay • Não disponível na maior parte dos centros • Teste calibrado para calcular a concentração de dabigatrano (quantificação precisa) • Risco hemorrágico acrescido para concentrações > 200ng/ml antes da toma seguinte • Um valor normal indica ausência de efeito anticoagulante ECT • Avaliação actividade do inibidor direto da trombina • Pouco disponível na pratica clínica • Um resultado 3 a 4 x o LSN representa um risco hemorrágico acrescido TP e INR • Sem correlação com o efeito anticoagulante • Valores falsos positivos • Sem indicação na prática clínica Dosear o aPTT! Avaliação analítica - aPTT 63seg - Plaquetas- 235x10(3) Efeito anticoagulante presente Que medidas tomar? 5ª Questão Qual a melhor opção? 1. Vitamina K é eficaz 2. Com aPTT 60 é seguro avançar para a cirurgia 3. Concentrado de plaquetas é sempre a primeira opção 4. Pedir o antidoto ao serviço de sangue (Antidaxa ®) 5. Nenhuma das anteriores 36 Alternativa se a cirurgia poder ser protelada por 4 a 6 horas Hemodialise / hemodiafiltração • Dabigatrano é uma molecula de relativo baixo peso molecular e que circula maioritariamente livre no plasma • Remoção de aprox. 62% em 2 horas F. Wagner, H. Peters, S. Formella et al., “Effective elimination A cirurgia é impreterível em < 4h Como minimizar o risco? • Suspender a medicação • Fluidos para acelerar a excreção renal • Carvão activado se ultima toma <2h • Concentrado de plaquetas, plasma fresco congelado (especialmente se uso concomitante de antiagragantes) Complexo Protrombina (ex: Octaplex 40U/kg, máx. 3000U) Complexo Protrombina activada ou inactivada Eerenberg E S et al. Circulation 2011;124:1573-1579 “CONCLUSIONS: In this animal study, PCC showed potential as an agent for reversing the effects of dabigatran. Further investigation is warranted.” Factor VIIa recombinante (20-40mcg/kg,) • Risco trombotico • Não é um antidoto do Dabigatrano • Melhora a hemostase local DECISÃO - Última toma Dabigatrano aprox 5h - aPTT – 63sec - Necessidade de cirurgia urgente • Apoio Serviço Sangue • CCP – 2800 U (40U/kg ) pré cirurgia • Durante a cirurgia foi necessário efectuar 2UCE (Queda de 3gr Hb) + 1 pool plaquetas • Pós cirúrgico sem complicações • 24h após cirurgia Hb 11,5g (estável, sem evidencia de perdas) Reinicio da terapêutica antitrombótica 45 Disclaimer: Dabigatran etexilate is now approved for clinical use in stroke prevention in atrial fibrillation in certain countries. Please check local prescribing information for further details. 6ª Questão Qual a melhor opção? 1. O reinicio da terapêutica deve ser ponderado após a alta e pelo médico assistente 2. Deve fazer AAS + Clopidogrel em vez de ACO até reavaliação pelo elevado risco hemorrágico da doente no período pós cirúrgico 3. Devo reiniciar ACO assim que garantida a hemostase 4. Nenhuma das anteriores 46 Reinicio de terapêutica antitrombotica • 2012 ESC- reinício da ACO na dose habitual (sem dose de carga) ao final do dia ( ou manhã seguinte) da cirurgia, desde que garantida a hemostase. 1 • 2010 Canadian Cardiovascular Society guidelines- Reinício da ACO assim que garantida a hemostase (aprox. 24horas) 2 ESC = European Society of Cardiology 1. ESC guidelines: Camm J et al. Eur Heart J 2012;31:2369–429; 2. CCS guidelines: Cairns JA et al. Can J Cardiol 2011;27:74–90 47 DECISÃO • HBMP 24h • Switch para Dabigatrano 110mg 2xdia 48 Disclaimer: Dabigatran etexilate is now approved for clinical use in stroke prevention in atrial fibrillation in certain countries. Please check local prescribing information for further details. RE-LY® • Dabigatran 150 mg twice daily1,2 – In RE-LY®: superior efficacy to well-controlled warfarin with a similar risk of major bleeding • Dabigatran 110 mg twice daily1,2 – In RE-LY®: similar efficacy to well-controlled warfarin with a lower risk of major bleeding • • • Low potential for drug–drug interactions3 Predictable and consistent pharmacodynamic effects4,5 No requirement for routine anticoagulation monitoring6 1. Connolly SJ et al. N Engl J Med 2009;361:1139–51; 2. Connolly SJ et al. N Engl J Med 2010;363:1875–6; 3. Blech S et al. Drug Metab Dispos 2008;36:386–99; 4. Stangier J et al. Clin Pharmacokinet 2008;28:47–59; 5. Stangier J. Clin Pharmacokinet 2008;47:285–95; 6. Stangier J et al. Br J Pharmacol 2007;64:292–303 Disclaimer: Dabigatran etexilate is now approved for clinical use in stroke prevention in atrial fibrillation in certain countries. Please check local prescribing information for further details. 49 The 2010 Canadian Cardiovascular Society guidelines and 2011 ACCF/AHA/HRS update guidelines recommend dabigatran • 2010 Canadian Cardiovascular Society guidelines for patients with AF:1 – CHADS2 score ≥2: Warfarin (INR 2.0–3.0) or dabigatran (preferred option) – CHADS2 score = 1: Warfarin (INR 2.0–3.0) or dabigatran (preferred option) – CHADS2 score = 0: Aspirin (75–325 mg/day) • 2011 ACCF/AHA/HRS focused update guidelines recommend dabigatran as an alternative to warfarin in patients with paroxysmal to permanent AF2 ACCF = American College of Cardiology Foundation; AHA = American Heart Association; HRS = Heart Rhythm Society; INR = international normalized ratio 1. CCS guidelines: Cairns JA et al. Can J Cardiol 2011;27:74–90; 2. ACCF/AHA/HRS focused update guidelines: Wann LS et al. J Am Coll Cardiol 2011;57:1330–37 Disclaimer: Dabigatran etexilate is now approved for clinical use in stroke prevention in atrial fibrillation in certain countries. Please check local prescribing information for further details. 50 ® RE-LY IN PERSPECTIVE Meta-analysis of ischaemic stroke or systemic embolism Warfarin vs. placebo Warfarin vs. low dose warfarin Warfarin vs. ASA Warfarin vs. ASA + clopidogrel Warfarin vs. ximelagatran Warfarin vs. dabigatran 150 mg BID 0 0.3 0.6 Favours warfarin 0.9 1.2 1.5 1.8 2.1 Favours other treatment ASA = acetylsalicylic acid. Dabigatran etexilate is not approved for clinical use in stroke prevention in atrial fibrillation outside the US and Canada. Camm J. Oral presentation at ESC on 30 Aug 2009 http://www.escardio.org/congresses/esc-2009/webcasts/pages/sunday.aspx Dabigatran 150 mg bid prevents 1 3 out of 4 AF-related strokes Warfarin prevents 64% of strokes.2 Dabigatran prevents an additional 35% of the remaining strokes or systemic embolisms3,4 1. Roskell NS et al. Thromb Haemost 2011; 102: Epub ahead of print. 2. Hart RG et al. Ann Intern Med 2007; 146:857–867. 3. Connolly SJ et al. N Engl J Med 2009; 361:1139–1151. 4.Connolly SJ et al. N Engl J Med 2010; 363:1875–1876 (letter to editor). New Oral Anticoagulant Targets New Oral Anticoagulant Targets 55 Disclaimer: Dabigatran etexilate is now approved for clinical use in stroke prevention in atrial fibrillation in certain countries. Please check local prescribing information for further details. 56 Disclaimer: Dabigatran etexilate is now approved for clinical use in stroke prevention in atrial fibrillation in certain countries. Please check local prescribing information for further details. 57 Disclaimer: Dabigatran etexilate is now approved for clinical use in stroke prevention in atrial fibrillation in certain countries. Please check local prescribing information for further details. Conclusão 58 Disclaimer: Dabigatran etexilate is now approved for clinical use in stroke prevention in atrial fibrillation in certain countries. Please check local prescribing information for further details. PATIENT RECEIVING DABIGATRAN THERAPY: EMERGENCY SURGERY PROTOCOL STOP: Dabigatran Contact Surgeon / Anaesthetist / Haematologist Coagulation screen to include APTT (consider thrombin time) ,+/- DTI assay if available [Important to document time of last dose of dabigatran] Full blood count and renal function / eGFR APTT prolonged Dabigatran anticoagulant effect maybe present (consider oral charcoal if dabigatran ingestion <2 hours and anaesthetist / surgeon agrees) APTT normal NO dabigatran anticoagulant effect present NO requirement to consider delaying surgery Maintain BP and Urine Output (dabigatran 80% renal excretion) IF ACTIVE BLEEDING Optimise tissue oxygenation Control of haemorrhage – Compression – Surgical intervention – Tranexamic Acid (1g i.v.) Red Cell transfusion – Aim Hb > 7 g/dl Platelet transfusion – Aim Plt > 50 x 109/l or – If CNS bleed aim Plt > 100 x 109/l Discuss with surgeon feasibility of delaying surgery SURGICAL DELAY ≥12 HOURS Refer to elective surgery table 1 Risk of bleeding dependent on – Time since last dabigatran dose – Type of surgery – Renal function / eGFR SURGICAL DELAY ≥4–12 HOURS IMMEDIATE SURGERY Consider Haemodialysis Or CONSIDER potential need for haemostatic agent peri / post-op Regional anaesthesia (spinal / epidural) is considered to be contra-indicated FEIBA / rFVIIa / PCC OBRIGADO! Necessidade de cirurgia urgente Francisco Moscoso Costa
Download