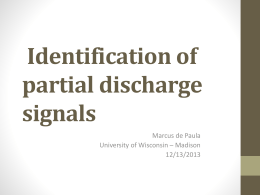
Jornal de Pediatria - Vol. 76, Nº1, 2000 65 0021-7557/00/76-01/65 Jornal de Pediatria Copyright © 2000 by Sociedade Brasileira de Pediatria ORIGINAL ARTICLE Breastfeeding in Montes Claros, Minas Gerais: a representative sample study Antônio P. Caldeira,1 Eugênio M.A. Goulart2 Abstract Objective: to evaluate the situation of breast-feeding in the city of Montes Claros, state of Minas Gerais, Brazil, among children under 2 years of age, and to determine variables associated to major risks for early weaning. Methods: in this cross-sectional study, interviews were carried out by trained personnel with 602 mothers randomly selected in the urban area of Montes Claros from September to November 1996. Survival analysis was the method used to calculate the prevalence and the median duration of breast-feeding. The chi-square test was performed to compare the proportions; significance level was set at 5%. Prevalence odds ratio was used to measure the significance of associations, with a 95% confidence interval. Logistic regression analysis was used to identify the risk factors for early weaning. Results: the average length of breast-feeding was 8.7 months; however, the median length of exclusive breast-feeding was only 27 days. Risk factors for early weaning were low birth weight (odds ratio=2.65; confidence interval 95%=1.10-6.40), mothers with difficulties to breastfeed in the first days (OR=1.86; CI 95%=1.21-2.85), and lack of postnatal medical incentive to breastfeed (OR=1.75; CI 95%=1.15-2.66). Conclusions: in general, breast-feeding is in a better situation than that showed by other national reports, although the numbers are still below what is recommended by the World Health Organization. There is a critical exclusive breast-feeding pattern. The factors related to early weaning denote a weak breast-feeding support given by maternal and infant health services. J Pediatr (Rio J) 2000; 76(1):65-72: breast-feeding, infant feeding, weaning, lactation, human milk, nutritional survey. Introduction Mother’s milk undoubtedly represents the best nourishment for the child during the first months of life. Several studies emphasize the advantages of breast-feeding in the promotion of infant health.1-3 Although breast-feeding was considered natural in the beginning of this century, today it is the result of a maternal option that involves a complex interaction of factors. National studies recently published point out an improvement in breast-feeding rates4,5 in relation to the past years.6,7 This fact reflects a world trend, and leads to 1. Assistant Professor Woman and Child Health, Universidade Estadual de Montes Claros (UNIMONTES) School of Medicine. 2. Associate Professor, Department of Pediatrics, School of Medicine, Universidade Federal de Minas Gerais (UFMG). 65 66 Jornal de Pediatria - Vol. 76, Nº1, 2000 an expressive repercussion in the health of Brazilian children in general. However, the present situation is far from ideal, and several works have aimed at presenting/testing strategies to increase breast-feeding rates.8,9 Several studies intended to define the determinant variables in the success or failure of breast-feeding,10-12 which could ease the organization of promotional strategies. Nevertheless, it is always prudent to consider that, as an eating habit, breast-feeding is intrinsically related to the development and the cultural patterns of a given population. This fact justifies the need for regional studies that allow a more efficient action in regard to intervention measures, based on knowledge of the local reality. Some authors study the local status of breast-feeding based on restricted samples, or on the clientele of inpatient and outpatient units. Despite the importance of these works, the population samples are not representative. Other studies do not define the different patterns of breast-feeding, or present an imprecise terminology. In this work, we tried to clearly define the terminology used in the study of a local representative population sample. The present study aimed at establishing knowledge about the reality of breast-feeding in the urban area of Montes Claros, state of Minas Gerais, Brazil. We also aimed at identifying the demographic and socioeconomic variables related to maternal and infant assistance that may be negatively interfering in breast-feeding practices. Breastfeeding in Montes Claros, Minas Gerais:... - Caldeira AP et alii During the interviews, we used forms with direct, easyto-answer questions. Most of these questions, already tested in previous studies,13 did not open many answering possibilities, requiring short answers. Questions included information on demographic and socioeconomic variables of the mothers and on local maternal and infant assistance, in addition to the children’s eating habits. The mothers were also questioned about the reasons for early weaning. The studied variables were divided in four groups: Demographic variables: parity, type of delivery, birthweight, maternal age, and presence of the father in the family structure. Socioeconomic variables: family income (assessed in minimum wages), maternal education, paternal education, and the father’s type of job (specialized or not). Variables related to prenatal assistance: number of prenatal appointments, prenatal incentive to breast-feeding (mothers were questioned whether they had been oriented and motivated to breastfeed during their prenatal appointments), previous willingness and planning to breastfeed (the mothers were questioned whether they were willing to breastfeed their children and for how long they planned to breastfeed in case they were willing to do so), and previous experience with breast-feeding (for mothers who had already breastfed). Methods The city of Montes Claros is located in the northern area of the state of Minas Gerais, Brazil, and it represents the main urban center of the region. Total population is approximately 270,000 inhabitants. The city presents indices of a predominantly poor population. Variables related to postnatal assistance: stay in conjoin lodgings, hospital incentive to breastfeed (mothers were questioned whether or not they had received orientation and incentive to breastfeed during their stay in the hospital/ maternity), time elapsed between birth and first breastfeeding, initial difficulties (mothers were questioned about the difficulties with mammary ingurgitation, fissures, problems with the nipple, and mastitis on the first days), and incentive during postnatal appointments (mothers who controlled the postnatal development of their children were asked whether they had been oriented and motivated by the pediatricians in relation to breast-feeding). In this research, we sought to study a representative sample of infants under the age of 2 (about 4.5% of the total population). The sample size suggested by Barros & Víctora for similar studies is approximately 450 children.13 The EPI-Info software14 suggests a sample of 564 children, with 25% of weaning before the 6th month, 5% of standard error, and design factor equal to 2 (it constituted a conglomerate sample). A previous pilot study was performed in order to test the questionnaire and the team of interviewers. All data were collected in the months of September and October 1996. In the beginning of November, 5% of the interviews were checked for a better control of the information quality. We considered as losses the mothers who refused and those who were absent or unavailable for an interview after at least three visits (total of 17 mothers). A random sample of 602 mothers of children under 2 year of age was selected for an interview at their own homes by a team of 28 especially trained interviewers. The sampling process occurred in two different stages: initially, we drew some censual sectors to be included in our study. Later, we randomly selected a starting point (a city block) in each sector, from where the whole area began to be visited (homes were alternated). We used the maps provided by Fundação IBGE for demographic and territorial divisions, according to the latest census. The EPI-Info software (version 6.0)14 was used for processing and analyzing data. The chi-square test was applied for comparing proportions when we evaluated factors associated with early weaning; a 5% alpha error was admitted. We also calculated odds ratio for each studied variable, with a 95% confidence interval. This is usually applied in crossover studies, in which the prevalence instead of the incidence - is assessed according to the significance of the association. Its calculation is similar to the relative risk, which is the odds ratio.15 Breastfeeding in Montes Claros, Minas Gerais:... - Caldeira AP et alii Logistic regression was performed with the Multlr16 software, in order to identify the variables that in a simultaneous mathematical analysis presented an independent explanatory effect on higher risk for early weaning. For this stage of the investigation, we selected the variables that showed P<0.20 in the bivariate analysis. For analyzing the length of breast-feeding, we applied the life table technique using an electronic spreadsheet. We considered the fact of receiving mother’s milk an assessment criterion. The introduction of water, tea, or juices was considered the final event in cases of exclusive breastfeeding; the introduction of any other food was considered the final event in cases of predominant breast-feeding. When analyzing length, the final event was usually the definitive interruption of breast-feeding. The terminology here used is proposed by the World Health Organization.17 Thus, isolated, the term breastfeeding does not define a specific behavior of giving suck. Exclusive breast-feeding refers to the use of human milk as the only source of nourishment to the child. Predominant breast-feeding is used when human milk is consumed as the main source of nutrition, allowing the consumption of other liquids (water, juices, or teas). Complementary feeding applies to the use of human milk associated with other food, either lactic or not, solid or liquid. Early weaning, in this text, refers to the introduction of complementary feeding prior to 4 months of life, with the interruption of exclusive or predominant breast-feeding before this period. Thus, for obvious reasons, only children older than 4 months of age participated in the analysis we present here. This subgroup was composed by 494 children. Jornal de Pediatria - Vol. 76, Nº1, 2000 67 The performance of this project was approved by the Department of Woman and Child Health, Medical School, Universidade Estadual de Montes Claros, and by the ethics committee of the Hospital Aroldo Tourinho. Results In our observed group, we identified a homogeneous distribution in relation to the children’s sex. The majority of the interviewed mothers was primiparous (45.7%), and only 10.4% of them had more than three children. Around 72% of the children were born by normal deliveries, and among these, 7.3% presented birthweight lower than 2,500 g. The proportion of mothers under 20 years of age was approximately 20%. In 24% of the visited homes, there was no father living with the family. Around 43% of the families had a monthly income inferior to two minimum wages, and 30.4% of the interviewed mothers informed an income between two and five minimum wages. Maternal education was evaluated: 5% of the mothers were illiterate, 25.4% had up to the 4th grade of elementary school, and less than 5% had completed college. Similar indices were observed in relation to paternal education: 7.1% of the fathers were illiterate, 23.9% had studied up to the 4th grade of elementary school, and 6.8% had completed a college program. Based on the life tables, it was possible to establish the graphic here presented (Figure 1) using the patterns of breast-feeding considered. The life table technique allows us to consider children who are still being breastfed in the moment of the interview, and also to know the proportion of Figure 1 - Survival curve for the several patterns of breast-feeding (Montes Claros, Minas Gerais, Brazil, 1996) 68 Jornal de Pediatria - Vol. 76, Nº1, 2000 children that remain being breastfed by the end of each month. So, it allows a longitudinal approach to the crosssectional data collected. In relation to exclusive breast-feeding, we observed that this is no longer a universal practice immediately after birth. By the end of the 1st month of life, only 48% of the children are being exclusively breastfed. In the following months, we noticed a continuous decline: by the end of the 2nd month of life, only 28% of the children remain being exclusively breastfed, and at 4 months, this percentage is approximately 8%. The median length of exclusive breastfeeding (age in which half of the children are receiving only the mother’s milk) was inferior to 1 month (27 days). The survival curve for exclusive breast-feeding + predominant breast-feeding reveals an early introduction of water or teas/juices. By the end of the 1st month of life, 88% of the children are included in this category. At 2 months of age, this proportion was 81%, and at 4 months of age, it was 50%. The average length observed was thus 4 months. From this age on, we observed significant frequency falls, with proportions of 27%, 18%, and 3% to 5, 6, and 7 months of age, respectively. The survival curve for general breast-feeding is also presented in the figure. We noticed that starting breastfeeding at birth is almost a universal practice among the interviewed mothers: around 96% of the children were still breastfed at the end of the 1st month, regardless of other sources of nutrition. However, weaning is frequent in the first months. At 2 months of age, the proportion of children who still receive mother’s milk is 91%; at 4 months of age, this rate falls to 76%. At 6 months of age, the proportion of children who still receive mother’s milk is 65%, and by the end of the 1st year, it goes down to 41%. The median length of breast-feeding was 8.7 months. During the 2nd year of life, breast-feeding rates remain decreasing: at 18 months, 22% of the children still use the mother’s milk, and by the end of the 2nd year, this rate is approximately 10%. The analysis of factors associated with early weaning refers to the study of the association between exclusive breast-feeding + predominant breast-feeding and some demographic and socioeconomic variables, in addition to data regarding maternal and infant care (pre and postnatal). It was not possible to evaluate determinants of the exclusive breast-feeding pattern due to the small number of children in this group; the early introduction of water or teas/juices is very usual among the studied population. Tables 1, 2, 3, and 4 present the studied variables and their association with early weaning. Among the variables chosen for the logistic regression (Table 5), low birthweight (odds ratio=2.65; confidence interval 95%=1.10-6.40) and lack of incentive to breastfeed during postnatal care (OR=1.75; CI 95%=1.15-2.66) were the factors associated with higher risks for early weaning. The variables concerning presence of father in the family structure and length of breast-feeding experience were not selected for the logistic Breastfeeding in Montes Claros, Minas Gerais:... - Caldeira AP et alii Table 1 - Demographic variables and association with early weaning (Montes Claros, Minas Gerais, Brazil, 1996) Variable Weaning Yes No χ2 P RP CI 95% Parity Primiparous 102 Nonprimiparous 133 123 136 0.67 0.4121 0.92 0.76-1.11 Interdelivery interval <24 months 35 > 24 months 98 36 100 0.01 0.9128 1.00 0.76-1.31 Mode of delivery Operative 71 Normal 164 67 192 0.95 0.3299 1.12 0.92-1.36 Birthweight <2500 g >2500 g 25 208 10 248 7.68 0.0056 1.57 1.24-1.98 Maternal age <20 years >20 years 62 173 51 208 2.76 0.0967 1.21 0.99-1.48 Presence of the father No 61 Yes 174 52 207 2.09 0.1480 1.18 0.97-1.45 regression so that the lack of complete information would not affect the analysis. The main reason (31.8%) presented by the mothers for the introduction of other food in their children’s diet was the belief that the isolated mother’s milk was not sufficient (that “it didn’t sustain” the children). When asked about what led them to believe in this, the most frequent answers were: excessive crying (54.0%), little milk (22.0%), stable weight (9.0%), and “thinned milk” (7.5%). Table 2 - Socioeconomic variables and their association with early weaning (Montes Claros, Minas Gerais, Brazil, 1996) Variable Family income <1 m.w.* >1 m.w.* Weaning Yes No χ2 P RP CI 95% 32 196 25 228 1.60 0.2055 1.21 0.94-1.56 Maternal education <4 years 85 >4 years 150 70 189 4.37 0.0366 1.24 1.03-1.49 Paternal education <4 years 64 >4 years 108 62 144 1.83 0.1766 1.19 0.95-1.48 Father’s job Unspecialized Specialized 142 65 5.65 0.0174 1.41 1.06-1.89 * minimum wage 139 35 Breastfeeding in Montes Claros, Minas Gerais:... - Caldeira AP et alii Table 3 - Variable Variables related to prenatal care and their association with early weaning (Montes Claros, Minas Gerais, Brazil, 1996) Weaning Yes No χ2 P RP CI 95% Prenatal care <4 appointments 44 >4 appointments 191 31 228 3.86 0.0496 1.29 1.04-1.60 Prenatal incentive No 88 Yes 147 78 181 2.65 0.1037 1.18 0.98-1.43 Will to breastfeed No/Indifferent 26 Yes 209 19 240 1.64 0.2000 1.24 0.95-1.62 Breast-feeding planning <6 months 82 66 >6 months 153 193 4.76 0.0291 1.25 1.04-1.51 Previous experience <4 months 35 >4 months 86 4.10 0.0429 1.37 1.05-1.78 23 109 The second reason (11.1%) presented by the mothers for early weaning was that the milk had dried out. Mothers who gave this answer were asked whether they knew the reason for such thing to have happened. Around 46% said they did not know why. The rest of the mothers presented reasons such as the use of medication (20%), emotional reasons (11%), physical reasons (6%), and others (17%). Other reasons presented for early weaning were: medical indication (10.7%), return to work (9.6%), and lack of interest on the child’s part (5.8%). Other reasons presented summed up 31.0%. Jornal de Pediatria - Vol. 76, Nº1, 2000 69 A fact that may justify the critical situation of exclusive breast-feeding, in spite of the general improvement in general breast-feeding, is the relevant rural influence observed in the city. Due to its geographic and developmental situation, the studied area presents an important migratory flow from the countryside to the city and its surrounding communities. It is well known that rural communities have more traditional habits: although they frequently start breastfeeding and sustain it for longer periods, they usually introduce other foods very early.7,20 Another factor that may be contributing to an early interruption of exclusive breast-feeding is the weak performance of maternal and infant services. The indices closest to the ideal ones were found, for example, in the city of Guarujá, São Paulo, as the result of an intense work of the lactation centers.21 Another example that must be mentioned is the town of Feira de Santana, state of Bahia, where very high indices can also be found due to a strong work developed by the healthcare units.22 In relation to the variables involved in breast-feeding, this study assessed, for the first time, the factors associated with a higher risk for early weaning, here understood as the introduction of foods other than water or tea/juices prior to 4 months of life. This approach took into consideration the fact that the introduction of water and tea in the studied population is a widely spread habit. Probably, the mothers who gave their children water or tea were not concerned with the nutritional aspect, but did so out of ignorance, or because they believed it could be helpful in solving their infants’ colic. Doctors are also commonly tolerant with such conduct.23 Table 4 - Discussion This study showed a relatively better situation for the urban area of Montes Claros when compared to general breast-feeding in other regions of Brazil.4,5 Almost all mothers started to breastfeed (98%), and the average length observed (8.7 months) was higher than the length found in previous studies. However, we identified a critical situation in regard to exclusive breast-feeding, which presented an average length inferior to 1 month (27 days). These data are compatible with the recent national literature: the National Research on Demography and Health,4 carried out in several regions of the country, showed a 92.3% rate for initial breast-feeding, with an average length of 7.0 months for breast-feeding, and 1.1 month for exclusive breast-feeding. So, a return to the breast-feeding practice has been seen in our country over the last years, especially after the creation of the Programa Nacional de Incentivo ao Aleitamento Materno; this has been registered in previous studies.18,19 Variable Variables related to postnatal care and their association with early weaning (Montes Claros, Minas Gerais, Brazil, 1996) Weaning Yes No χ2 P RP CI 95% Conjoin lodging No 142 Yes 93 147 112 0.54 0.4623 1.08 0.90-1.31 Hospital incentive No 78 Yes 157 72 187 1.45 0.2287 1.14 0.94-1.38 First breast-feeding >6 hours 164 <6 hours 62 161 97 5.19 0.0227 1.29 1.04-1.62 Initial difficulties Yes 119 No 116 89 170 12.73 0.0004 1.41 1.17-1.69 Postnatal incentive No 138 Yes 97 127 132 4.27 1.23 1.02-1.49 0.0388 Breastfeeding in Montes Claros, Minas Gerais:... - Caldeira AP et alii 70 Jornal de Pediatria - Vol. 76, Nº1, 2000 The majority of studies that deal with factors associated with breast-feeding establish associations with the breastfeeding total length, and do not take into consideration the different patterns of suckling.10 This fact incurs the mistake of considering extreme situations in one only category, such as the child who receives exclusively mother’s milk, and one who receives it only now and then. Naturally, the ideal approach to this matter would be a survey with the mothers who exclusively breastfeed their infants. However, as previously mentioned, the introduction of water and teas in the newborns’ diet is very usual, thus reducing the number of children classified in the exclusive breast-feeding category. Generally, demographic variables (Table 1) are not very likely to be relevant to the breast-feeding pattern. A review performed by Losch et al.11 points out several works with different results in relation to these variables. The present study showed low birthweight as a risk factor for early weaning, even after the logistic regression. This result is in agreement with other national study,24 although the literature stresses diverging results.25 These unmatched results can possibly be justified by the complexity of factors involved in the birth of an underweight child. The bivariate analysis of socioeconomic factors (Table 2) showed that the return of the breast-feeding practice has been more common among socially privileged families (greater maternal education and “specialized” paternal work). Nevertheless, this observation was not confirmed by the logistic regression. Other studies are necessary in order to better define the role of socioeconomic variables, considering that there are some studies remarking a positive association between early weaning and low maternal education, for instance.12 On the other hand, we can not forget that different studies set different cutoff points; as an Table 5 - Tables 3 and 4 emphasize (already in the bivariate analysis) the lack of association between the studied breastfeeding pattern and variables classically considered as supportive of breast-feeding: prenatal incentive, stay in conjoin lodging, and incentive during postnatal care, for instance. Two hypotheses were raised to justify such situation. The first was the existence in the town of a reference center for breast-feeding: the Banco de Leite Humano, of Hospital Aroldo Tourinho, recently certified as Hospital Amigo da Criança. Such fact could have been acting as homogenizing factor, since the studied population was not divided according to the place of prenatal or postnatal care. Another justification for such findings would be a generally unsatisfactory performance of maternal and infant care in health services concerning the promotion of breast-feeding. This hypothesis should not be disregarded, since after the logistic regression (Table 5), the variables that remained able to predict a higher risk for early weaning (low weight, initial difficulties in breast-feeding, and lack of incentive in postnatal care) were directly or indirectly associated with the quality of maternal and infant care. Breast-feeding is a maternal option that involves a complex interaction of socioeconomic, cultural and psychological factors, among others. However, as a “socially recreated” habit, the role of maternal and infant services in the promotion of breast-feeding should by no means be disregarded. The proportion of mothers who did not stay in conjoin lodgings and presented late first suckling, or that mentioned not having received any information about breastfeeding in prenatal appointments or during their stay in the hospital/maternity is noteworthy. Logistic regression analysis for some variables related to higher risk for early weaning (Montes Claros, Minas Gerais, Brazil, 1996) Variable Birthweight Maternal age Maternal education Paternal education Father’s job (status) Prenatal appointments Prenatal incentive Breast-feeding planning Late first breast-feeding Initial difficulties Postnatal incentive * P< 0.05 example, in our approach, we established early weaning as the introduction of other foods prior to 4 months of life. Coefficient (ß) Standard deviation Odds Ratio CI 95% 0.9749 - 0.1229 0.2423 - 0.0695 0.4655 0.3466 - 0.1068 0.4808 0.3695 0.6201 0.5608 0.4497 0.2967 0.3045 0.2985 0.2793 0.3391 0.2504 0.2590 0.2313 0.2181 0.2143 2.651* 0.884 1.274 0.933 1.593 1.414 0.899 1.617 1.447 1.859* 1.752* 1.098-6.400 0.499-1.582 0.702-2.314 0.520-1.675 0.921-2.754 0.728-2.749 0.550-1.468 0.979-2.686 0.920-2.277 1.212-2.851 1.151-2.667 Breastfeeding in Montes Claros, Minas Gerais:... - Caldeira AP et alii Certainly, there is a complex relationship between the determinants of a well-succeeded breast-feeding practice, and this work did not aim at discussing it deeply. The authors believe that when defining the breast-feeding pattern in a certain region, it is important that all intervening variables be considered, allowing a global knowledge of the situation, and ensuring a greater potential for interventions. The main reasons presented by the mothers for the early introduction of other foods are similar to those already presented in previous studies, and denote insecurity and absence of knowledge.26 The considerable rate of mothers who informed early weaning as a medical indication is a reason for concern: 10.7%! This work demonstrated that, despite the return of the breast-feeding practice, permanent incentive and support are necessary, since we still observe an unsatisfactory behavior, particularly in relation to exclusive breast-feeding. The results here presented stress the need for prioritizing activities for the promotion and improvement of maternal and infant services. The variables here studied naturally present a complex interaction with others not yet studied. Future studies are necessary to approach the interrelations among these several variables and also other psychological and anthropological questions (not covered by this study) that certainly interfere in the breast-feeding practice. References 1. Cunningham AS, Jelliffe DB, Jelliffe EFP. Breast-feeding and health in the 1890s: a global epidemiologic review. J Pediatr 1991; 118:659-66. 2. Habicht JP, Da Vanzo J, Butz WP. Does breastfeeding really save lives, or are apparent benefits due to biases? Am J Epidemiol 1986; 123:279-90. 3. Victora CG, Vaughan JP, Lombardi C, Fucks SMC, Gigante LP, Smith PG, et al. Evidence for protection by breast-feeding against infant deaths from infectious diseases in Brazil. Lancet 1987; 2:319-22. 4. BEMFAM. Pesquisa Nacional sobre Demografia e Saúde. Rio de Janeiro: UNICEF, 1997. Jornal de Pediatria - Vol. 76, Nº1, 2000 71 5. UNICEF - Fundo das Nações Unidas para a Infância. Saúde e nutrição das crianças nordestinas. Pesquisas estaduais, 1987 1992. Brasília: UNICEF, 1995. 6. Barros FC, Victora CG, Vaughan JP. Breastfeeding and socioeconomic status in southern Brazil. Acta Paediatr Scand 1986; 75:558-62. 7. Leão MM, Coitinho DC, Recine E, Costa LAL, Lacerda AJ. O perfil do aleitamento materno no Brasil. In: Monteiro MFG, Cervini R, orgs. Perfil estatístico de crianças e mães no Brasil: aspectos de saúde e nutrição de crianças no Brasil 1989. Rio de Janeiro. FIBGE/UNICEF/INAN; 1992.p.97-109. 8. Barros FC, Halpern R, Victora CG, Teixeira AMBB, Beria JU. Promoção da amamentação em localidade urbana da região sul do Brasil: estudo de intervenção randomizado. Rev Saúde Públ 1994; 28:277-83. 9. Susin LRO, Giugliani ERJ, Kummer SC, Maciel M, Benjamin ACW, Machado DB, et al. Uma estratégia simples que aumenta os conhecimentos das mães em aleitamento materno e melhora as taxas de amamentação. J Pediatr (Rio J) 1998; 74:368-75. 10. Forman MR. Review of research on the factors associated with choice and duration of infant feeding in less-developed coutries. Pediatrics 1984; 74:667-94. 11. Losch M, Dungy CI, Russell D, Dusdieker, LB. Impact of attitudes on maternal decisions regarding infant feeding. J Pediatr 1995; 126:507-14. 12. Giugliani ERJ, Issler RMS, Justo EB, Seffrin CF, Hartmann RM, Carvalho NM. Risk factors for early termination of breast feeding in Brazil. Acta Paediatr Scand 1992; 81:484-7. 13. Barros FC, Vítora CG. Epidemiologia da saúde infantil: um manual para diagnósticos comunitários. São Paulo, Hucitec, 1991. 14. Dean AG, Burton AH, Dicker RC. Epi Info, Version 6: a word processing, database and statistics program for epidemiology on micro-computers. Atlanta: Centers for Disease Control; 1994. 15. Wagner MB, Callegari-Jacques SM. Medidas de associação em estudos epidemiológicos: risco relativo e odds ratio. J Pediatr (Rio J) 1998; 74:247-51. 16. Campos-Filho N, Franco EL. A microcomputer program for multiple logistic regression by unconditional and conditional maximum likelyhood methods. Am J Epidemiol 1989; 129:439-44. 17. World Health Organization. Indicators for assessing breastfeeding practices. Update. Programme for Control of Diarrhoeal Disease. 1992; 10:1-4. 18. Figueiredo LMH, Goulart EMA. Análise da eficácia do programa de incentivo ao aleitamento materno em um bairro periférico de Belo Horizonte (Brasil):1980/1986/1992. J Pediatr (Rio J) 1995; 71:203-8. 19. Rea MF. The brazilian national breastfeeding program: a success story. Int J Gynaecol Obstet 1990; 31:79-82. 20. Assis AMO, Prado MS, Freitas MCS, Silva RCR, Ramos LB, Machado AD. Prática do aleitamento materno em comunidades rurais do semi-árido baiano. Rev Saúde Pbl (S Paulo) 1994; 28:380-4. 21. Barros FC, Semer TC, Tonioli Filho, S. Tomasi E, Victora CG. The impact of lactation centres on breasfeeding patterns, morbidity and growth: a cohort study. Acta Paediatr Scand 1995; 84:1221-6. 22. Vieira GO, Glisser M, Araújo SPT, Sales AN. Indicadores do aleitamento materno na cidade de Feira de Santana, Bahia. J Pediatr (Rio J) 1998; 74:11-6. 23. César JA, Kuhn D, Devens ES, Martins Jr. E, Aguiar MRC, Holthausen RS, et al. Prescrição de chás para menores de seis meses: a opinião dos médicos de uma cidade de porte médio no sul do Brasil. J Pediatr (Rio J) 1996; 72:27-31. 72 Jornal de Pediatria - Vol. 76, Nº1, 2000 24. Barros FC, Victora CG, Vaughan JP, Smith PG. Birth weight and duration of breast-feeding: are the beneficial effects of human milk being overestimated? Pediatrics 1986; 78:656-61. 25. Verronen P. Breast feeding of low birthweight infants. Acta Paediatr Scand 1985; 74:495-9. 26. Siqueira R, Durso N, Almada, AGP, Moreira MT, Massad GB. Reflexões sobre as causas do desmame precoce observadas em dinâmicas de grupo de incentivo ao aleitamento materno. J Pediatr (Rio J) 1994; 70:16-20. Breastfeeding in Montes Claros, Minas Gerais:... - Caldeira AP et alii Correspondence: Dr. Antônio Prates Caldeira Rua Santa Helena, 136 CEP 39400-369 – Montes Claros, MG, Brazil Phone: + 55 38 222.3879 E-mail: [email protected]
Download