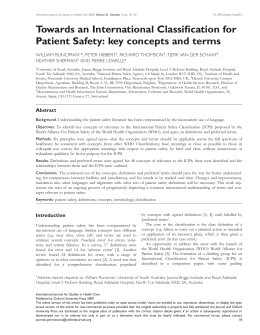
Introdução à Medicina I/II Class 9 Adviser: Alberto Freitas What are PQIs? IntroMedI - class 9 - PQIs QIs • Not definitive measures • Use hospital discharge inpatient data •Based on readily available data IntroMedI - class 9 - PQIs PQIs • Primary Healthcare •Ambulatory Care Sensitive Conditions Prevention starts here. • “avoidable hospitalization rates are a sensitive indicator for assessing quality of primary ambulatory care”IntroMedI (Niti et al,9 2003) - class - PQIs Source: Ansari Z. Laditka JN. Laditka SB. Access to Health Care and Hospitalization for Ambulatory Care Sensitive Conditions. Med Care Res Rev. 2006;IntroMedI 63:719-742 - class 9 - PQIs When were they first introduced? IntroMedI - class 9 - PQIs Studies of the kind in other countries • United States • Australia (Ansari et al., 2003, 2006) • New Zealand • Canada • Italy (Sheerin et al., 2006) (Roos et al., 2005, Porter et al., 2007) • Singapore • Spain (Starfied et al.,1991, Sanderson et al., 2000, Kozak et al., 2001) (Niti & Ng, 2003) (Sánchez et al., 2004) (Rizza et al., 2007) IntroMedI - class 9 - PQIs Source: Agency for Healthcare Research and Quality. Guide to Prevention Quality Indicators: Hospital Admission for Ambulatory Care Sensitive Conditions. Version 3.1. Rockville, MD: Agency for Healthcare Research and Quality; March 2007. IntroMedI - class 9 - PQIs This kind of studies • evaluate the quality of the healthcare conditions • establish patterns • allow comparison with past and future works inside and outside the sampling area. IntroMedI - class 9 - PQIs Key-words • Ambulatory Care •Primary Care •Quality of Healthcare •Portugal •Delivery of Healthcare •Prevention Quality Indicators IntroMedI - class 9 - PQIs Aim IntroMedII - class 9 - PQIs RESEARCH QUESTION What is the status of the primary health care system in Portugal and how does it compare to past years and among its regions? IntroMedI - class 9 - PQIs AIMS • Assessment of the primary healthcare system quality, in an outpatient setting. • Compare different level 2 NUTS*, trends 2000-2005 • Lay hypotheses for the observed differences. *except for Azores and Madeira. IntroMedI - class 9 - PQIs Participants and Methods IntroMedII - class 9 - PQIs PARTICIPANTS • 6199102 patients’ discharge data from national database (ACSS) • 94 Acute Care Public Hospitals (continent) IntroMedI - class 9 - PQIs DATA COLLECTION • Data collected from acute care hospital database • Variables of interest present in the database or calculated from others • INE (Instituto Nacional de Estatística) provides populational and other statistical data IntroMedI - class 9 - PQIs • Division in NUTS II 2000 2002 2001 2004 2003 2005 IntroMedI - class 9 - PQIs INCLUSION • Diagnosis according to PQI EXCLUSION • Age <18 • MDC = 14 or 15 • Transferred from • Related non-evaluative conditions IntroMedI - class 9 - PQIs IntroMedI - class 9 - PQIs IntroMedI - class 9 - PQIs IntroMedI - class 9 - PQIs Source: Agency for Healthcare Research and Quality. Guide to Prevention Quality Indicators: Hospital Admission for Ambulatory Care Sensitive Conditions. Version 3.1. Rockville, MD: Agency for Healthcare Research and Quality; March 2007. IntroMedI - class 9 - PQIs INVALID • Address codes missing. non-existent or belonging to the Azores or Madeira. • Absurd age (below 0; over 150) • Undetermined Sex (3) IntroMedI - class 9 - PQIs STRATIFICATION • NUT II (Norte, Centro, Lisboa, Alentejo, Algarve) • Year (2000-2005) • Gender • Age (0-17; 18-24; 25-34; 35-44; 45-54; 55-64; 65-74; 75+) IntroMedII - class 9 - PQIs IntroMedII - class 9 - PQIs RESULTS OVERVIEW IntroMedII - class 9 - PQIs * * 9 Overall PQI = Sum of all PQIs except for 2 and IntroMedI - class 9 - PQIs IntroMedI - class 9 - PQIs IntroMedII - class 9 - PQIs IntroMedII - class 9 - PQIs IntroMedII - class 9 - PQIs IntroMedII - class 9 - PQIs Country PQI1 PQI2 PQI3 PQI5 PQI7 PQI8 PQI9 M 20.04 23.62 89.23 155.77 18.94 156.45 5.24 F 29.27 18.95 89.25 80.84 25.38 190.29 6.01 M 56.24 31.18 135.41 208.1 37.27 463.64 6.00 F 53.31 28.93 118.71 251.39 61.44 512.08 6.53 PQI12 PQI13 PQI14 PQI15 PQI16 PT Gender USA PQI10 PQI11 PT USA M 17.75 324.81 58.43 71.37 19.64 11.37 31.38 F 25.35 263.99 107.27 49.79 27.82 27.83 19.34 M 98.72 398.89 101.03 43.74 21.37 67.99 51.22 F 154.39 436.39 249.26 47.97 23.07 170.22 27.64 IntroMedII - class 9 - PQIs Significant Associations • Life Quality • GIP per Capita • Life Expectancy at Birth • Healthcare Facilities • Number of Health Centers per 100.000 pop. • Medical visits per inhabitant • Number of doctors per 1000 pop. • Education • Literacy Index • Proportion of active population with minimum education (“3º Ciclo”) • Proportion of active population with secondary education or higher • Neonatal • Age of first pregnancy IntroMedII - class 9 - PQIs Significant Associations •Overall PQI •Acute PQI •Diabetes PQI No significant associations found IntroMedII - class 9 - PQIs Diabetes short-term complication Doctors (N) r= -0,70 Nurses (N) r= -0,81 Health Centres r= 0,74 Lit. Index r= -0,67 Life exp. r= -0,61 Hospital Distance r= 0,76 Med. Visits r= -0,59 IntroMedII - class 9 - PQIs Perforated Appendix Pop. Density r= -0,96 Med. Visits r= -0,76 Doctors (N) r= -0,53 Hospital Distance r= 0,37 Life Exp. r= -0,43 Lit. Index r= - 0,40 IntroMedII - class 9 - PQIs Diabetes Long-term complication NONE COPD Med. Visits r= 0,71 Life Exp. r= 0,60 Hospital Distance r= 0,53 Min. Education r= -0,39 Hypertension Sec. Education r= -0,36 Min. Education r= -0,35 IntroMedII - class 9 - PQIs Congestive Heart Failure Health Centres r= 0,70 Doctors (N) r= -0,68 Hospital Distance r= 0,56 Lit. Index r= -0,68 Dehydration Hospital Distance r= 0,78 Lit. Index r= -0,64 Life Exp. r= -0,40 Health Centres r= 0,73 IntroMedII - class 9 - PQIs Bacterial Pneumonia Life Exp. r= -0,51 Urinary Tract Infection Sec. Education r= 0,49 Min. Education r= 0,52 Med. Visits r= -0,51 GDP r= 0,37 IntroMedII - class 9 - PQIs Angina without Procedure GDP r= 0,54 Minim. Education r= 0,44 Life Exp. r= -0,50 Sec. Education r =0,42 Lower-extremety amp. in Diabetics Hospital Distance r= 0,74 Health Centres r= 0,63 Minim. Education r= 0,33 Lit. Index r= -0,62 Uncontrolled Diabetes Med. Visits r= 0,50 Adult Asthma GDP r= 0,50 Min. Education r= 0,47 Med. Visits r= 0,57 Sec. Education r =0,46 Lit. Index r= 0,38 IntroMedII - class 9 - PQIs Low Birth Weight per 100 neonates GDP r= 0,70 Mean Age 1st Pregnancy r= 0,64 Fig.6 Mean age of first child vs LBW Linear Regression IntroMedII - class 9 - PQIs Cost Analysis IntroMedII - class 9 - PQIs IntroMedII - class 9 - PQIs Discussion IntroMedII - class 9 - PQIs Prevention • There are different levels of prevention 1. Preventing the onset of the condition 2. Preventing the rampage development of symptoms; i.e controling the condition IntroMedII - class 9 - PQIs Variable North Centre Lisbon Alentejo Algarve Population Ageing Index 90,9 140,1 105,9 170,8 126,2 Cities 51 41 17 19 11 Pop. Density(N/Km2) 175,6 84,5 946,9 24,3 83,4 SEDI CO2 emissions/Km2 0,775 0,767 620,131 361,722 0,854 9029,576 0,747 232,786 0,791 360,295 Sources: INE, 2005; Cónim C. População e Desenvolvimento Humano- Uma Perspectiva de Quantificação -1970-1999; Marques JL, Martins JM, Castro EA. Análise input-output rectangular inter-regional - emissões de CO2 em Portugal e o protocolo de Quioto Fig.9 Overall PQI per NUT II IntroMedII - class 9 - PQIs Self-Perception of Health NUT II Good/Very Good Total Male Female Continent 31,3 38,5 27,1 North 31,4 38,1 27,6 Centre 26 32,4 22,1 Lisbon 34,3 42,8 49,1 Alentejo 33,2 40 28,3 Algarve 31,5 38,8 27,2 Total 42,9 42,2 44,1 43,3 42,5 41,7 Average Male Female 41,6 43,7 40,8 43,1 44 44,2 40,7 44,9 43 42,2 39,3 43,1 Bad/Very Bad Total Male Female 25,8 19,9 29,3 26,4 21,1 29,3 27,9 23,6 30,5 22,4 16,5 26 24,3 17 28,5 26,9 22 29,7 Source: National Health Survey, 1999 Overall PQI IntroMedII - class 9 - PQIs Patient Profile • Male • Elderly (75 years old +) • Living in areas not densely populated IntroMedII - class 9 - PQIs Studies supporting this association: Lockwood et al .Stress-associated preterm delivery: the role of corticotropin-releasing hormone. IntroMedII - class 9 - PQIs Variable USA Portugal Year Source Human Development Index (HDI) 0,951 (ranked 12th) 0,897 (ranked 29th) 2005 UNDP report 2007/2008 Obesity 32,0% 14.2% 2004 Health 2007 (USA) Overweight and obesity in Portugal: national prevalence in 2003– 2005 Smoking prevalence 23.9% 35.8% 2005 WHO CO2 emissions (ton per capita) 20,6 5,6 2004 UNDP report 2007/2008 Hypertension 30,2% 20,0% 2004/5 National Health Survey (PT) Health 2007 (USA) Diabetes 7,0% 6,5% 2005 National Institute of Diabetes National Health Survey (PT) IntroMedII - class 9 - PQIs Variable USA Access to drinking water 99% 99% 2006 WHO Life expectancy at birth (years) 77,9 77,7 2005 UNDP report 2007/2008 Climate Dfa/b, Cfa, BSh/k, Csb, BWk. Csb (north), Csa (south) 2006 Kottek et al, World map of Koppen-Geiger climate classification update. Ethnies Heterogeneous N/A 2006 US Census Bureau. Male/Female 49%/51% 48,4% 51,6% 2005 US Census Bureau INE >65 y 12,4% 17,0% 2005 US Census Bureau INE Wet all seasons: Dfa – snow, fully humid, hot summer ; Dfb – snow, fully humid, warm summer Portugal Year Dry arid BWk – arid, desert, cold arid Mediteranean Csb – warm temperature, summer dry, warm summer Csa – warm temperature, summer dry, hot summer. Source Humid subtropical: Cfa – warm temperature, flly humid, hot summer Dry semiarid BSk – arid, steppe, cold arid BSh – arid, steppe, hot arid IntroMedII - class 9 - PQIs 250 200 150 Portugal Spain Espanha 100 50 UT I De CH hy F dr at at Hy io pe n r te ns io n An gi na As th m a DP O C 0 IntroMedII - class 9 - PQIs Study Limitations • Socioeconomic factors: • gender • age • Income • Propensity to seek care according to perceived health needs • Hospital bed availability • Regular source of care or continuity of care • Differences in healthcare service (Public/Private healthcare; Insurances) • Coding Issues • Lack in Epidemiological Studies (or inconsistent) • Intra-regional variations IntroMedII - class 9 - PQIs Conclusions •From 55 years old on: •There is a clear increase in avoidable hospitalizations •Males present higher avoidable hospitalizations rates •Differences among years are not significant •Norte presents the best quality/cost ratio •Portugal shows a more efficient primary healthcare system than USA or Spain. •Some heterogeneity among regions points to uneven primary healthcare supply •Further study is required to evaluate yearly trends and precise factors which influence PQ. IntroMedII - class 9 - PQIs Future Research • Multivariate analysis of correlations • Litoral/Interior Analysis • Wider timespan (Pre and Post SNS restructuration) • Careful analysis of economical indexes and prevalence of analysed conditions • Further International Comparison IntroMedII - class 9 - PQIs IntroMedII - class 9 - PQIs REFERENCES PQI Info • Agency for Healthcare Research and Quality. Guide to Prevention Quality Indicators: Hospital Admission for Ambulatory Care Sensitive Conditions. Version 3.1. Rockville (MD): Agency for Healthcare Research and Quality; March 2007. • Farquhar, M. AHRQ Quality Indicators [slides]. Rockville (MD): Agency for Healthcare Research and Quality; 2005. 20 slides colour. • General Questions about the AHRQ QIs [Internet]. Rockville (MD): Agency for Healthcare Research and Quality; July 2004 [cited 2007 Oct 31]. Available from: http://www.qualityindicators.ahrq.gov/general_faq.htm • AHRQ Prevention Quality Indicators Overview [Internet]. Rockville (MD): Agency for Healthcare Research and Quality; July 2004 [cited 2007 Oct 31]. Available from: http://www.qualityindicators.ahrq.gov/pqi_overview.htm • Agency for Healthcare Research and Quality. Prevention Quality Indicators: Technical Specifications. Version 3.2. Rockville (MD): AHRQ; March 2008.IntroMedI - class 9 - PQIs Related Articles • Ansari Z, Laditka JN, Laditka SB. Access to Healthcare and Hospitalization for Ambulatory Care Sensitive Conditions. Med Care Res Rev. 2006; 63:719-42 • Billings J, Zeitel L, Lukomnick J, Carey TS, Blank AE, Newman L. Impact of socioeconomic status on hospital use in New York City. Health Aff (Millwood). 1993; 2:162-9. • Starfield B. Primary care and health: a cross-national comparison. JAMA. 1991; 266:2268-71. • Sanderson C, Dixon J. Conditions for which onset or hospital admission is potentially preventable by timely and effective ambulatory care. J Health Serv Res Policy. 2000, 5:222-30. • Kozak LJ, Hall MJ, Owings MF. Trends in Avoidable Hospitalizations, 1980-1998. Health Aff. 2001; 2 (20): 225-32. • Casanova C, Starfield B. Hospitalizations of children and access to primary care: a crossnational comparison. Int J Health Serv. 1995; 25:283-94. • Ansari Z, Barbetti T, Carson NJ, Auckland MJ, Cicuttini F: The Victorian ambulatory care sensitive conditions study: rural and urban perspectives. Soz Praventivmed. 2003; 48:3343. IntroMedI - class 9 - PQIs • Sheerin I, Allen G, Henare M, Craig K. Avoidable hospitalizations: potential for primary and public health initiatives in Canterbury, New Zealand. N Z Med J. 2003; 119(1236). • Roos LL, Walld R, Uhanova J, Bond R: Physician visits, hospitalizations, and socioeconomic status: ambulatory care sensitive conditions in a Canadian setting. Health Serv Res. 2005, 40:1167-85. • Porter J, Herring J, Lacroix J, Levinton C. Avoidable Admissions and Repeat Admissions: What Do They Tell Us? Healthc Q. 2007, 10:26-28. • Niti M, Ng TP. Avoidable hospitalization rates in Singapore, 1991-1998: assessing trends and inequities of quality primary care, J Epidemiol Community Health. 2003; 57: 17-22. • Rizza P, Bianco A, Pavia M, Angelillo IF. Preventable hospitalization and access to primary healthcare in an area of Southern Italy. BMC Health Serv Res. 2007; 7:134. • Sanchez JLA, Vilalta JS, Perepérez SB, Martínez IM. Characteristics of avoidable hospitalization in Spain. Med Clin (Barc). 2004; 122(17):653-8. • Weissman JS, Gatsonis C, Epstein AM. Rates of avoidable hospitalization by insurance status in Massachusetts and Maryland. JAMA. 1992; 268:2388-94. IntroMedI - class 9 - PQIs • Pappas G, Hadden WC, Kozak LJ, Fisher GF. Potentially Avoidable Hospitalization inequalities in rates between US socioeconomic groups. Am J Public Health. 1997; 87:811-6. • Booth GL, Hux JE. Relationship Between Avoidable Hospitalizations for Diabetes Mellitus and Income Level. Arch Intern Med. 2003; 163:101-6. Data Sources • Administração Central do Sistema de Saúde, IP (ACSS). www.acss.min-saude.pt • Statistics Portugal [Internet]. Lisbon: INE. 1864- [cited 2008 Mar 30]. http://www.ine.pt • Regulation (EC) No 1059/2003 of the European Parliament and of the Council of 26 May 2003 on the establishment of a common classification of territorial units for statistics (NUTS) (Official Journal L 154, 21/06/2003) • Departamento de Gestão Financeira. Serviço Nacional de Saúde – Contas Globais 2000 [Internet]. IGIF; 2002 Sep [cited 2008 Apr 19]. 192p. Available from: http://www.acss.minsaude.pt/Downloads_ACSS/relatorios_contas/Relatorio_Contas_2000.pdf IntroMedI - class 9 - PQIs • Departamento de Gestão Financeira. Serviço Nacional de Saúde – Contas Globais 2001 [Internet]. IGIF; 2003 Nov [cited 2008 Apr 19]. 171p. Available from: http://www.acss.minsaude.pt/Downloads_ACSS/relatorios_contas/Relatorio_Contas_2001.pdf • Departamento de Consolidação e Controlo de Gestão do SNS. Serviço Nacional de Saúde – Contas Globais 2002 [Internet]. IGIF; 2004 Apr [cited 2008 Apr 19]. 237p. Available from: http://www.acss.minsaude.pt/Downloads_ACSS/relatorios_contas/Relatorio_Contas_2002.pdf • Departamento de Consolidação e Controlo de Gestão do SNS. Serviço Nacional de Saúde – Contas Globais 2003 [Internet]. Lisbon: Instituto de Gestão Informática e Financeira da Saúde; 2005 Apr [cited 2008 Apr 19]. 223p. Available from: http://www.acss.minsaude.pt/Downloads_ACSS/relatorios_contas/Relatorio_Contas_2003.pdf • Departamento de Consolidação e Controlo de Gestão do SNS. Serviço Nacional de Saúde – Contas Globais 2004 [Internet]. Lisbon: Instituto de Gestão Informática e Financeira da Saúde; 2006 Mar [cited 2008 Apr 19]. 187p. Available from: http://www.acss.minsaude.pt/Downloads_ACSS/relatorios_contas/Relatorio_Contas_2004.pdf IntroMedI - class 9 - PQIs Software • SPSS for Windows, Rel. 15.0.0 2006. Chicago (IL): SPSS Inc. • Microsoft Frontpage 2003, Rel. 11.5516.8202. USA: Microsoft Corporation. International Data •Health, United States, 2007 ;U.S. Department of Health and Human Services; Centers for Disease Control and Prevention; National Center for Health Statistics •World Health Organization. Available from:www.who.int/en •M. C. Peel, B. L. Finlayson, and T. A. McMahon. Updated world map of the Koppen-Geiger climate classification •National Diabetes Statistics. Available from: diabetes.niddk.nih.gov/dm/pubs/statistics/ •U.S. Census Bureau. Available from:www.census.gov/ IntroMedII - class 9 - PQIs Protocol developed by: Ana Catarina Moura, [email protected] Ana Margarida Oliveira, [email protected] Bárbara Mendonça, [email protected] Cláudia Pereira, [email protected] Hélio Alves, [email protected] João Miguel Rego, [email protected] José Pedro Pinto, [email protected] Maria Francisca Costa, [email protected] Maria Guiomar Pinheiro, [email protected] Nelson Couto, [email protected] Ricardo Reis, [email protected] José Alberto Silva Freitas, [email protected] IntroMedI - class 9 - PQIs Thank you for your time IntroMedI - class 9 - PQIs
Download